CLINICAL CASE





THE SITUATION
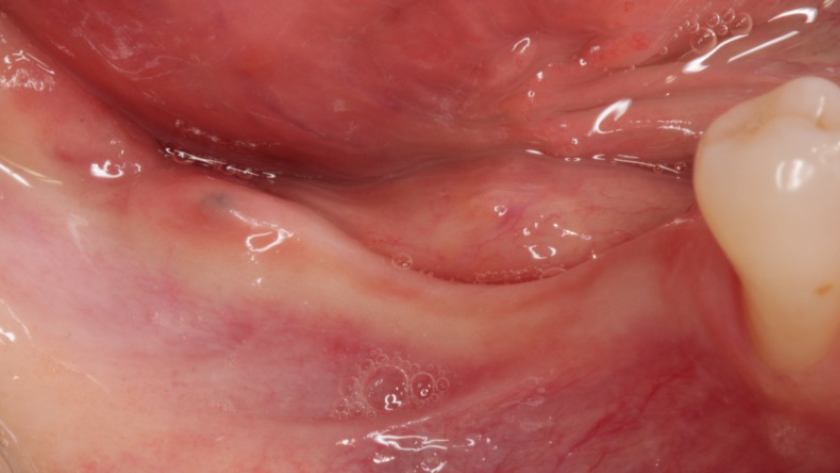
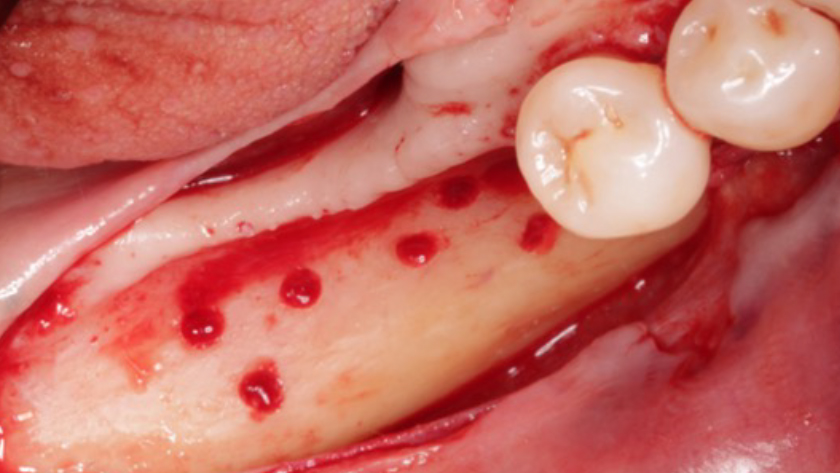
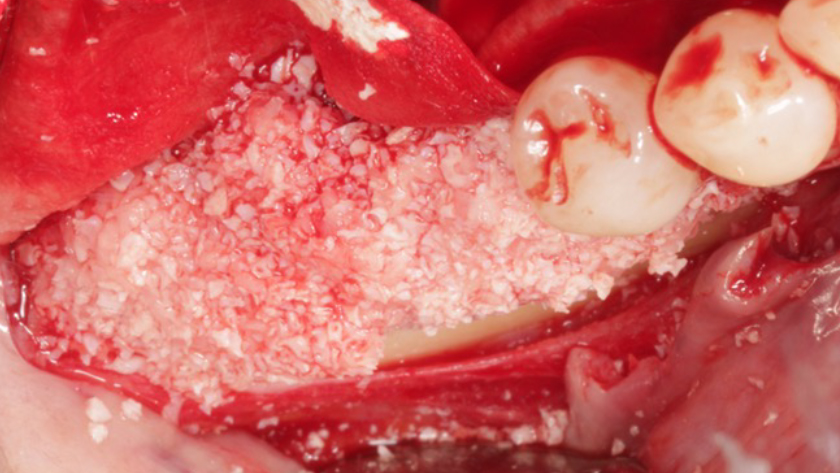
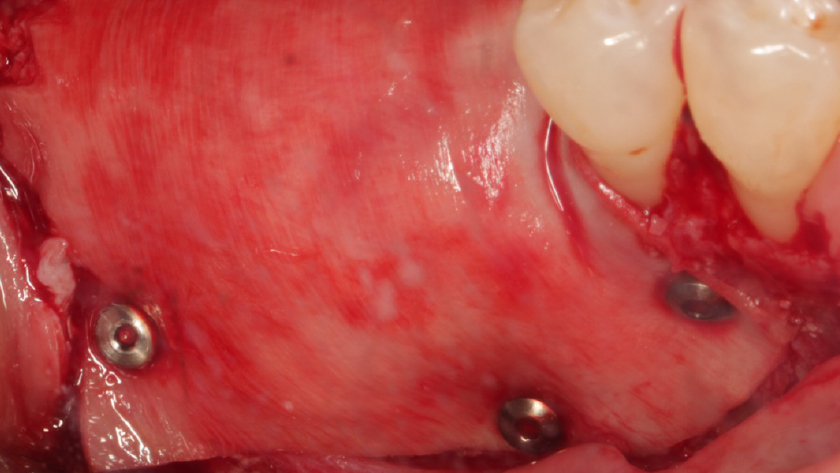
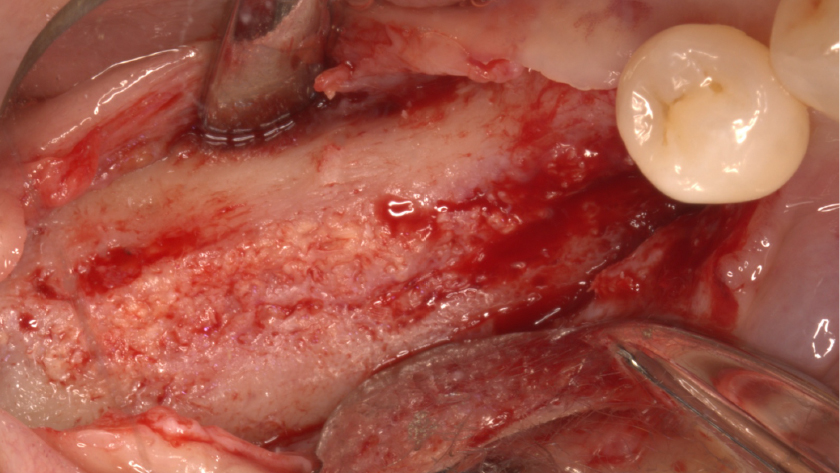
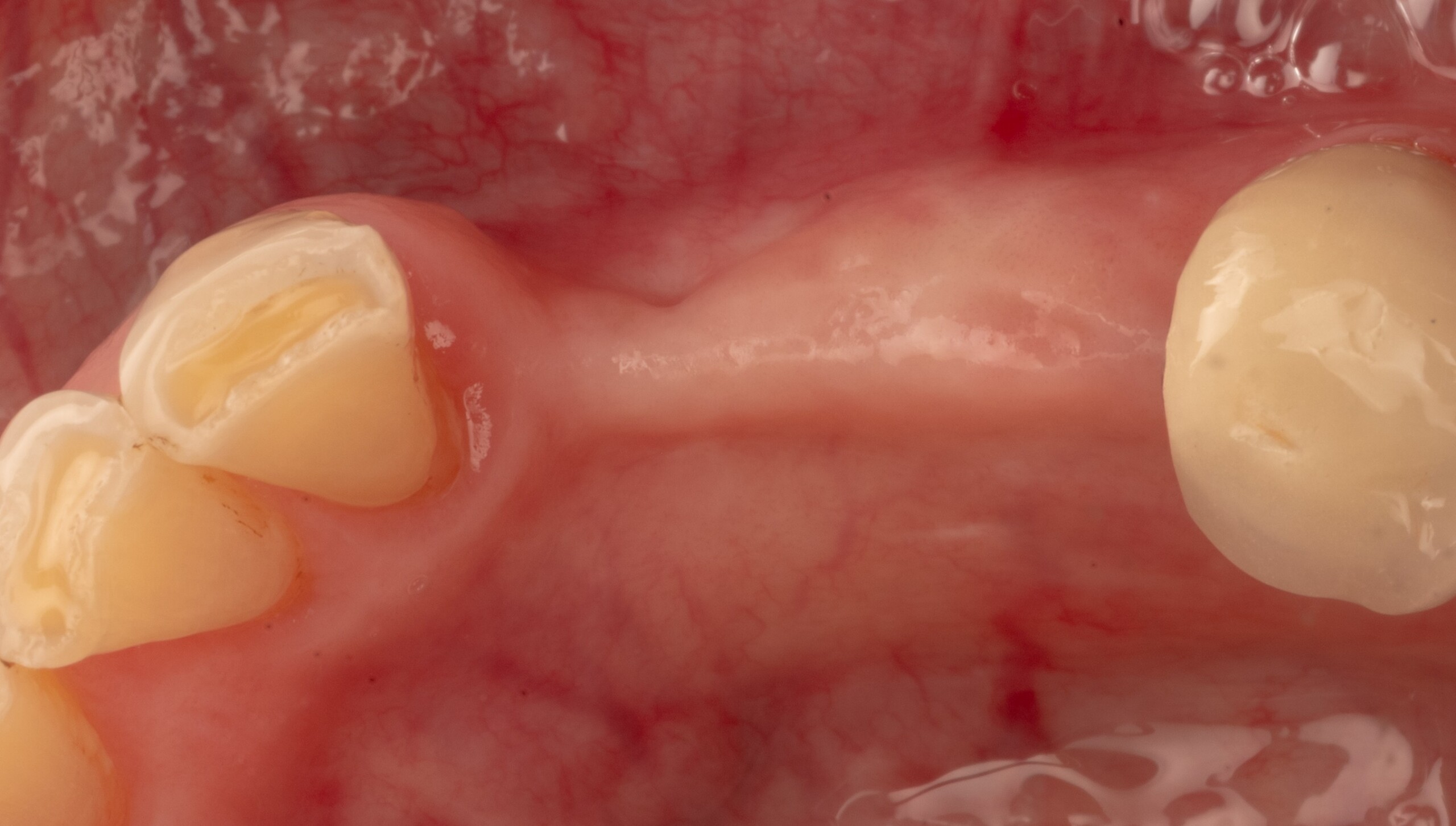
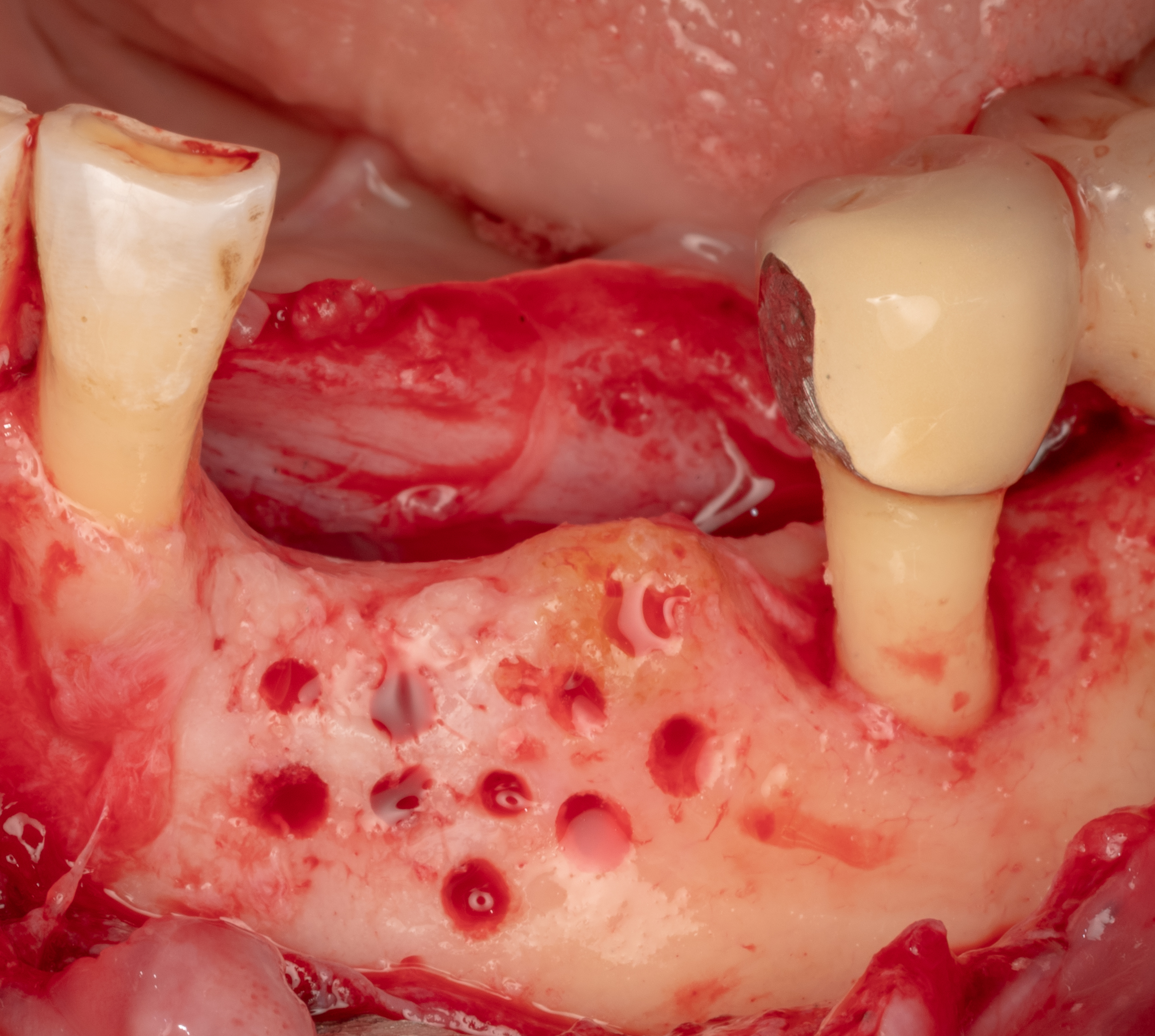
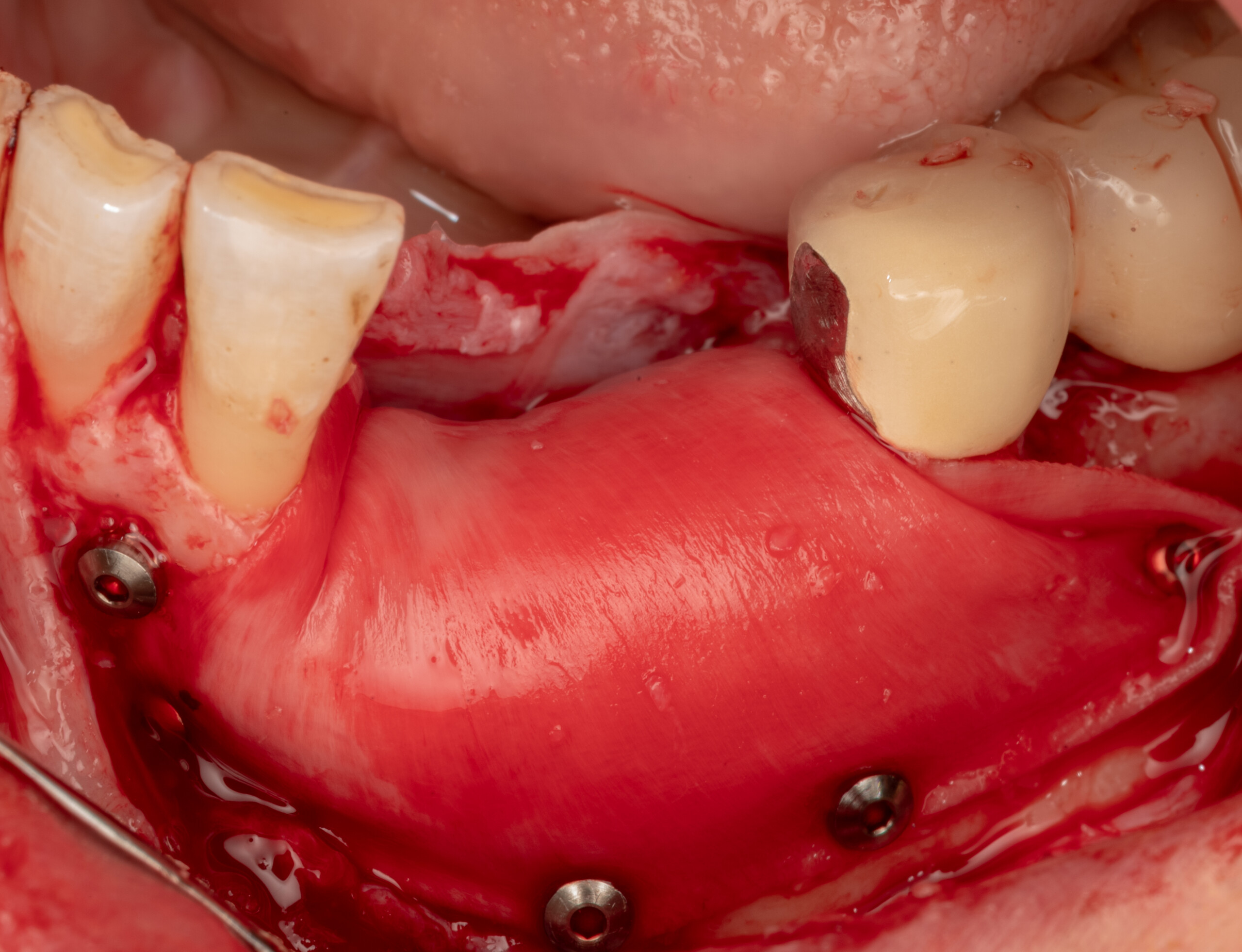
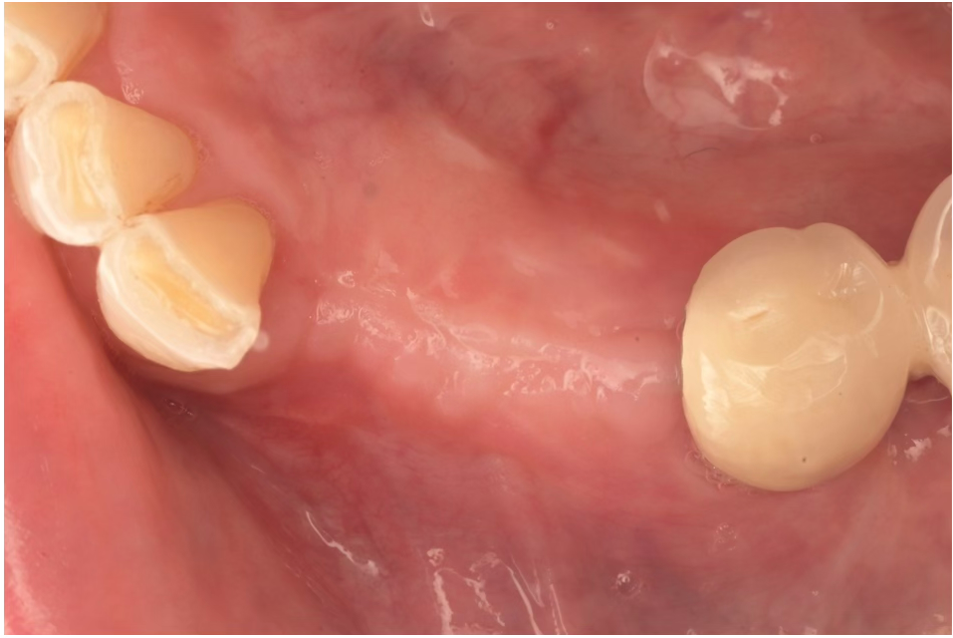
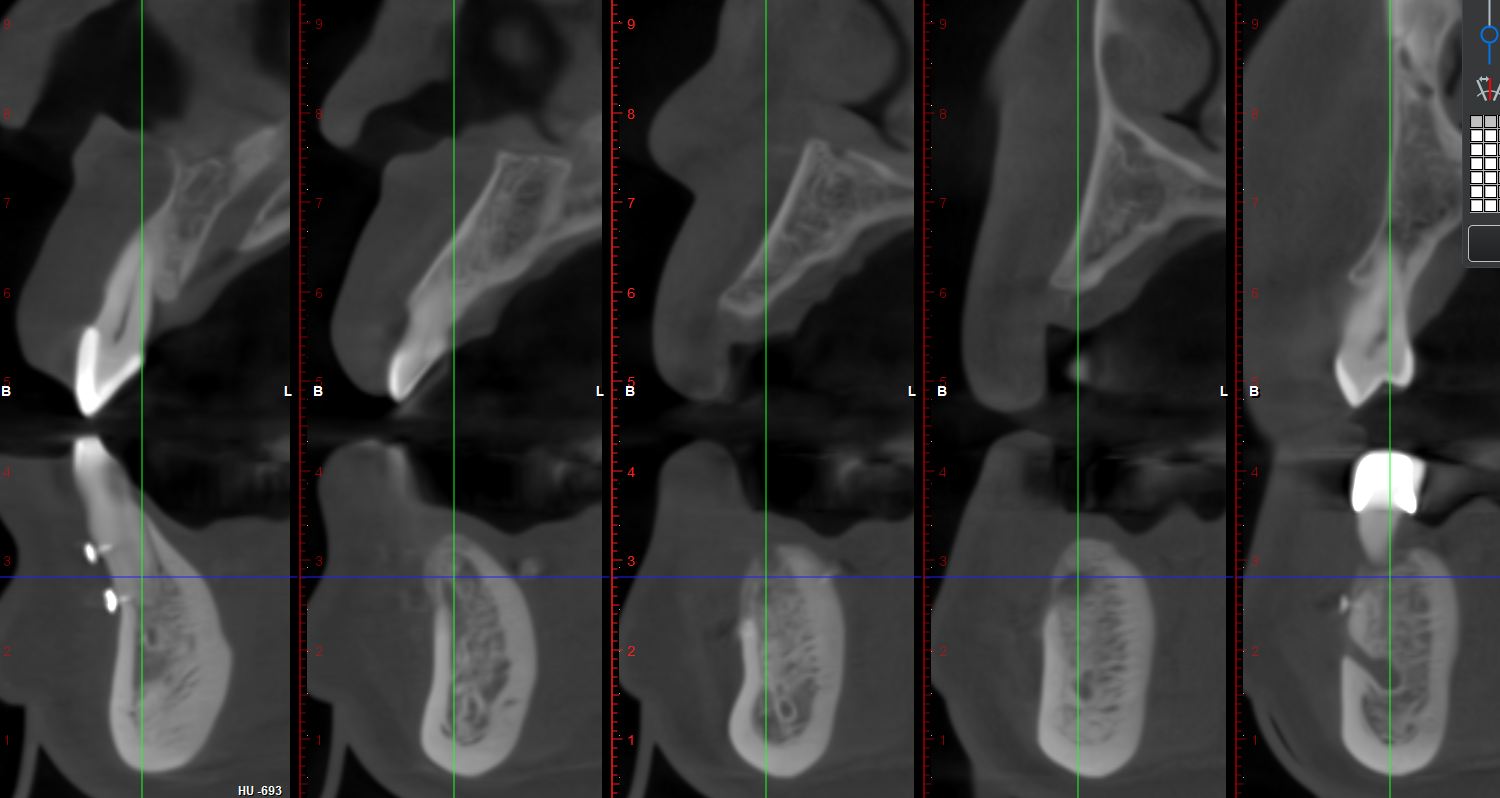
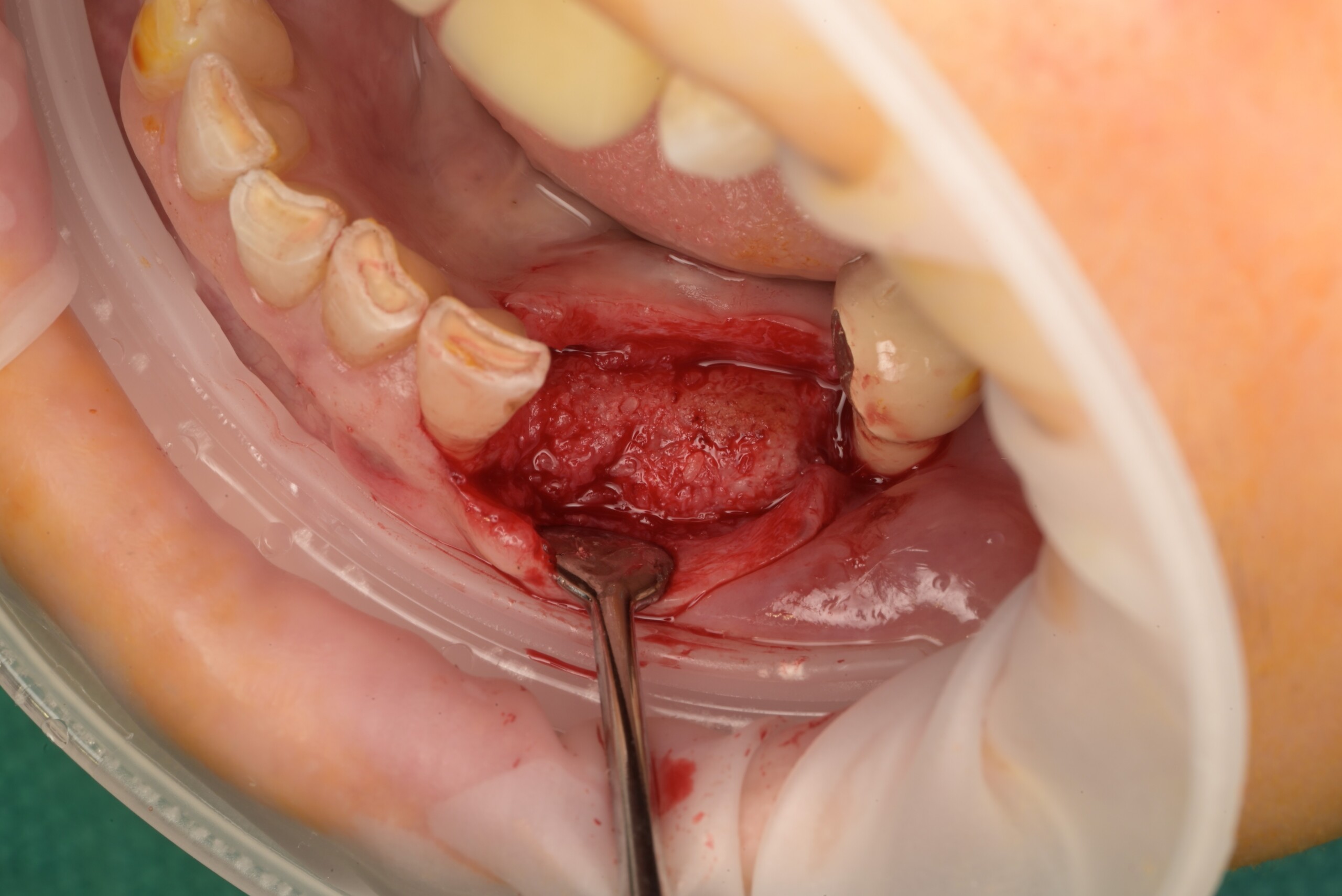
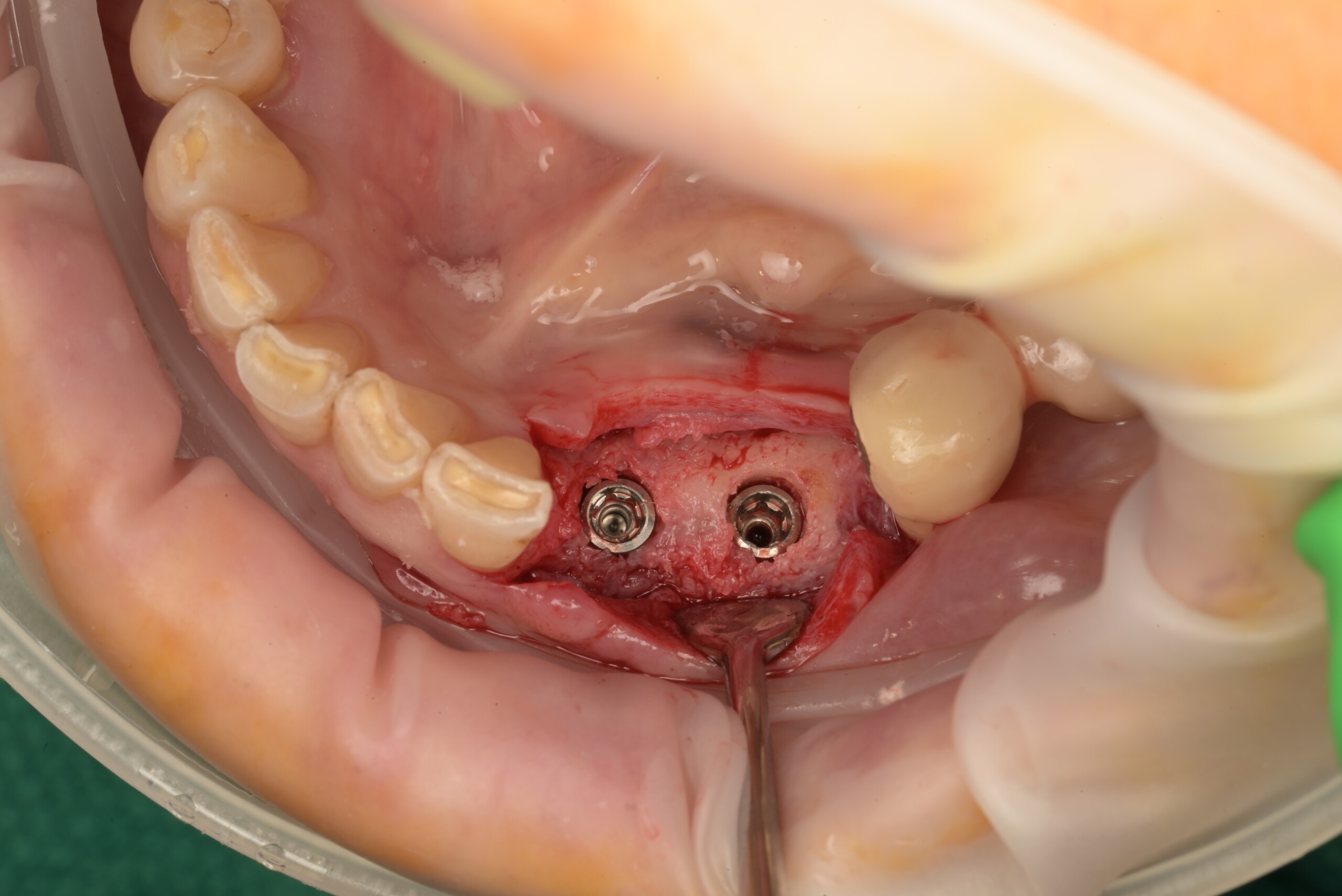
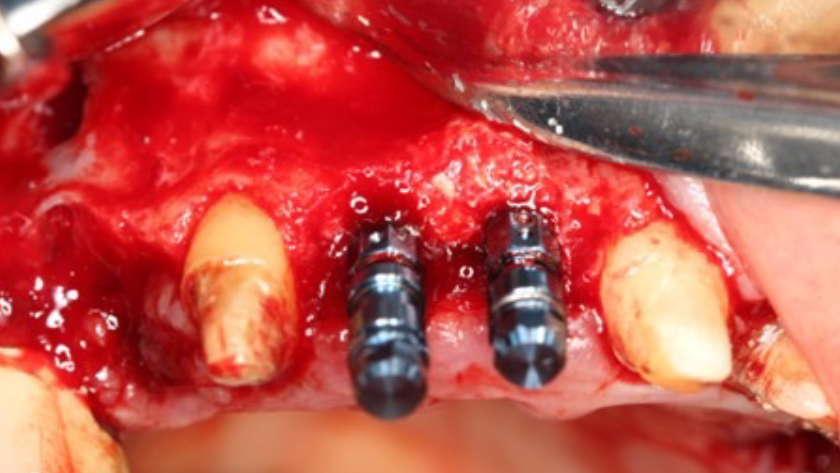
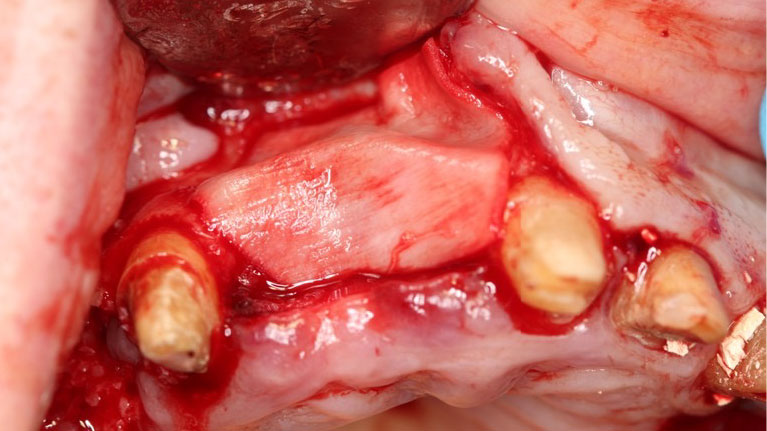
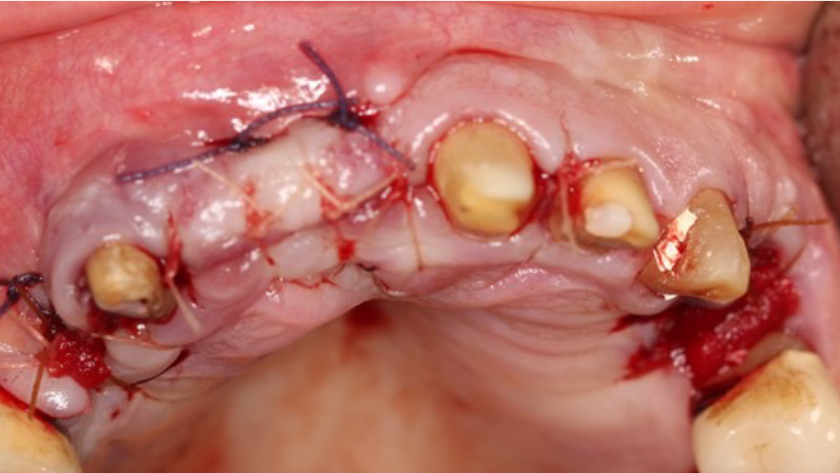
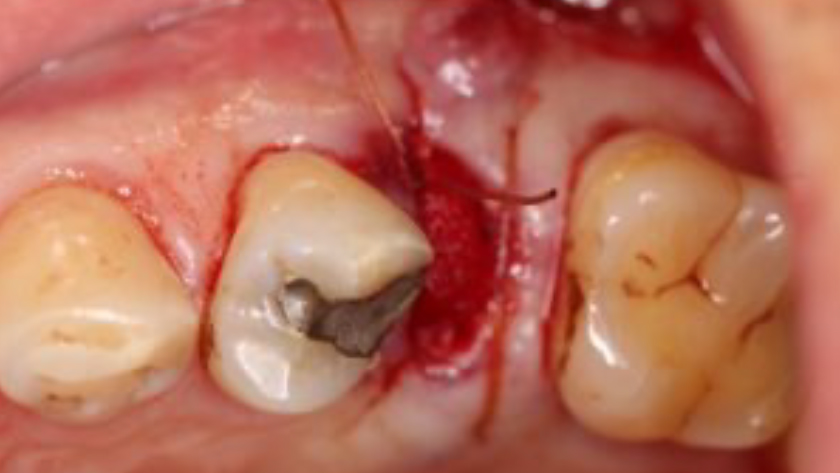
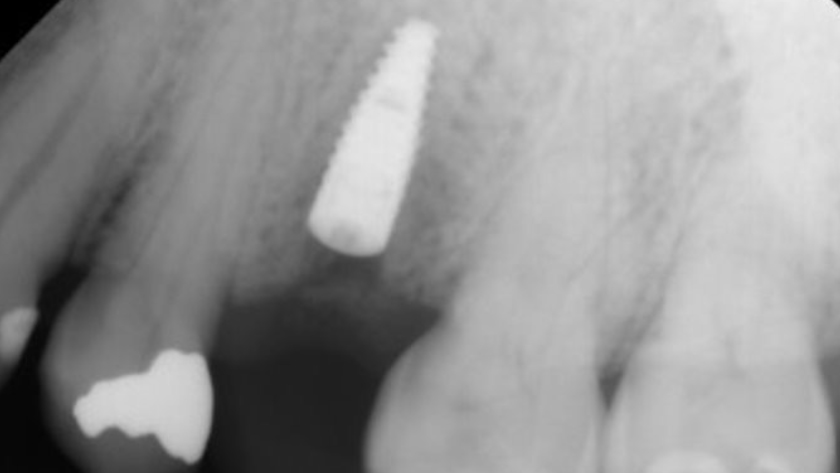
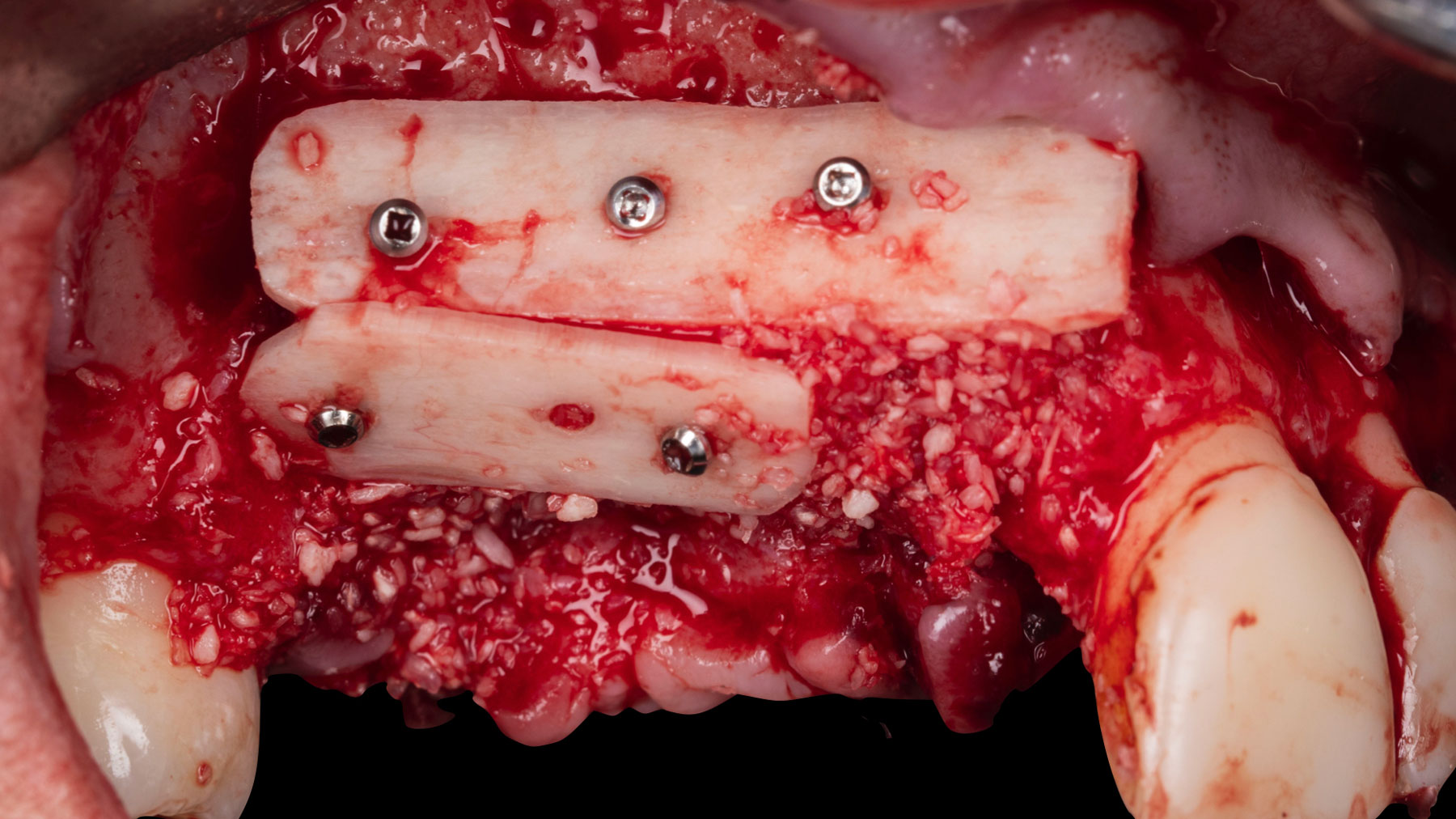
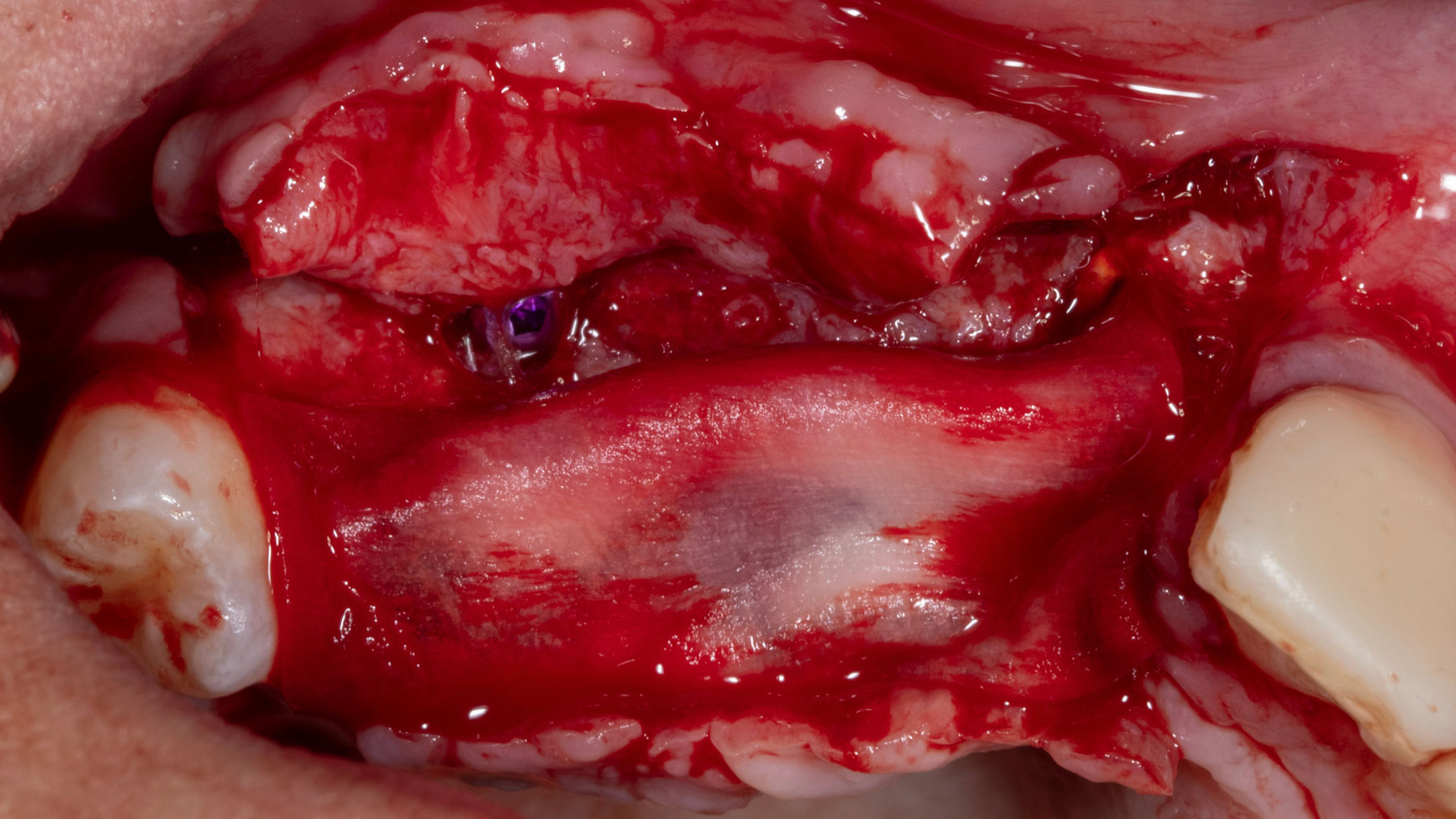
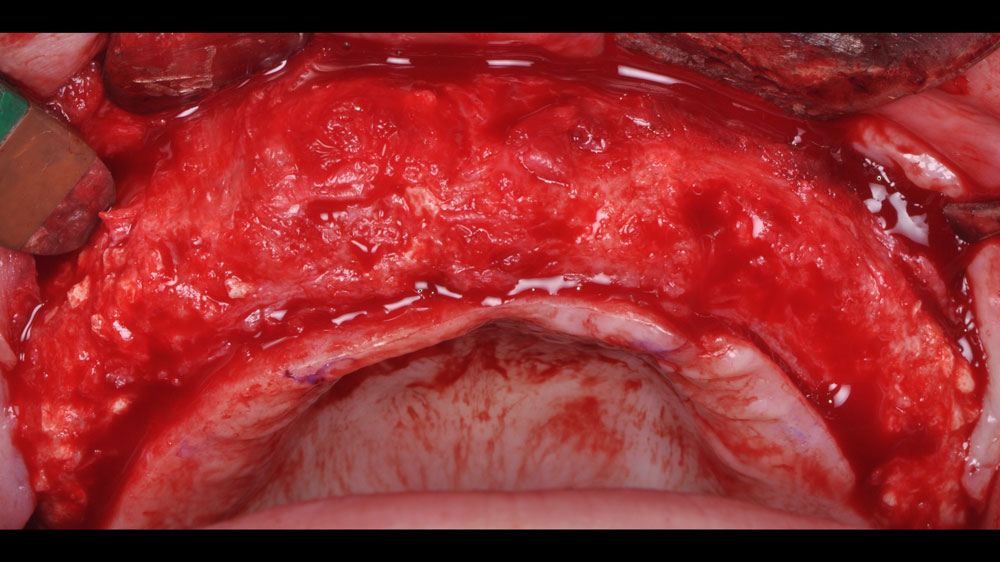
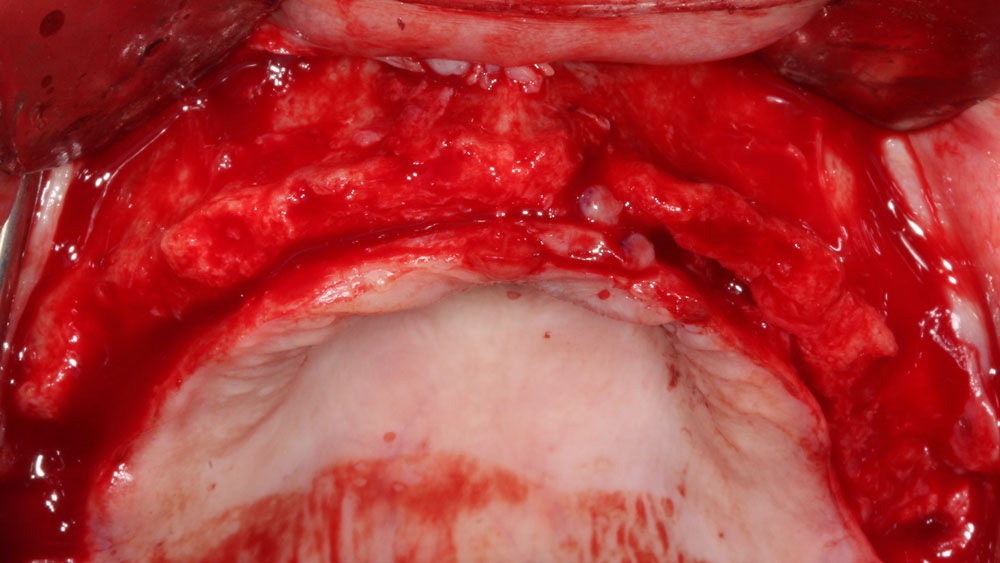
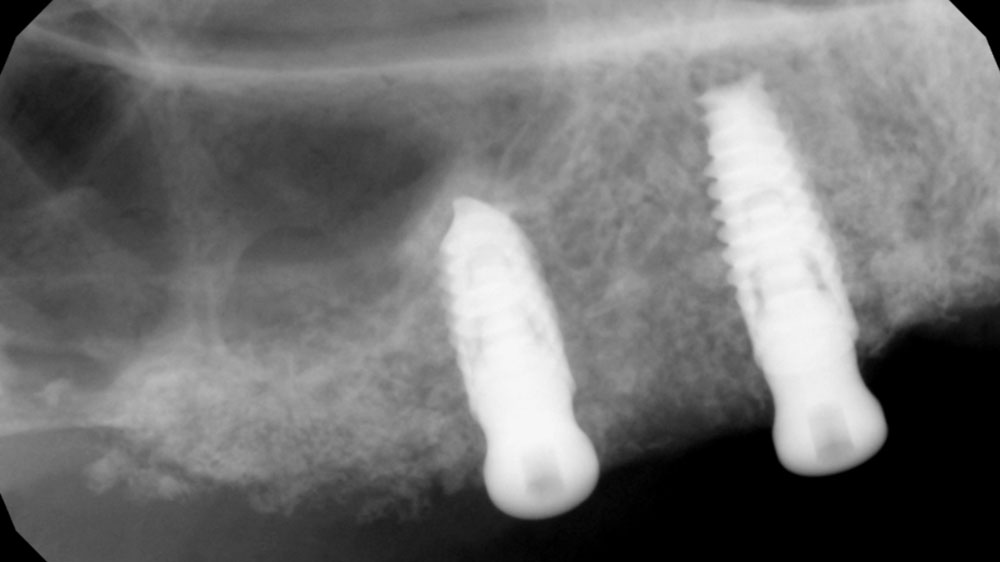
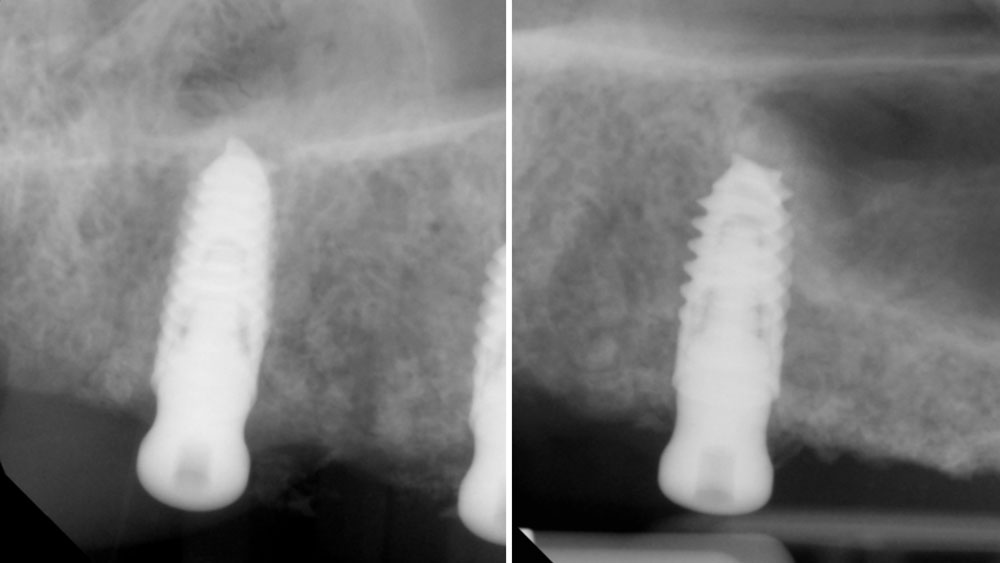
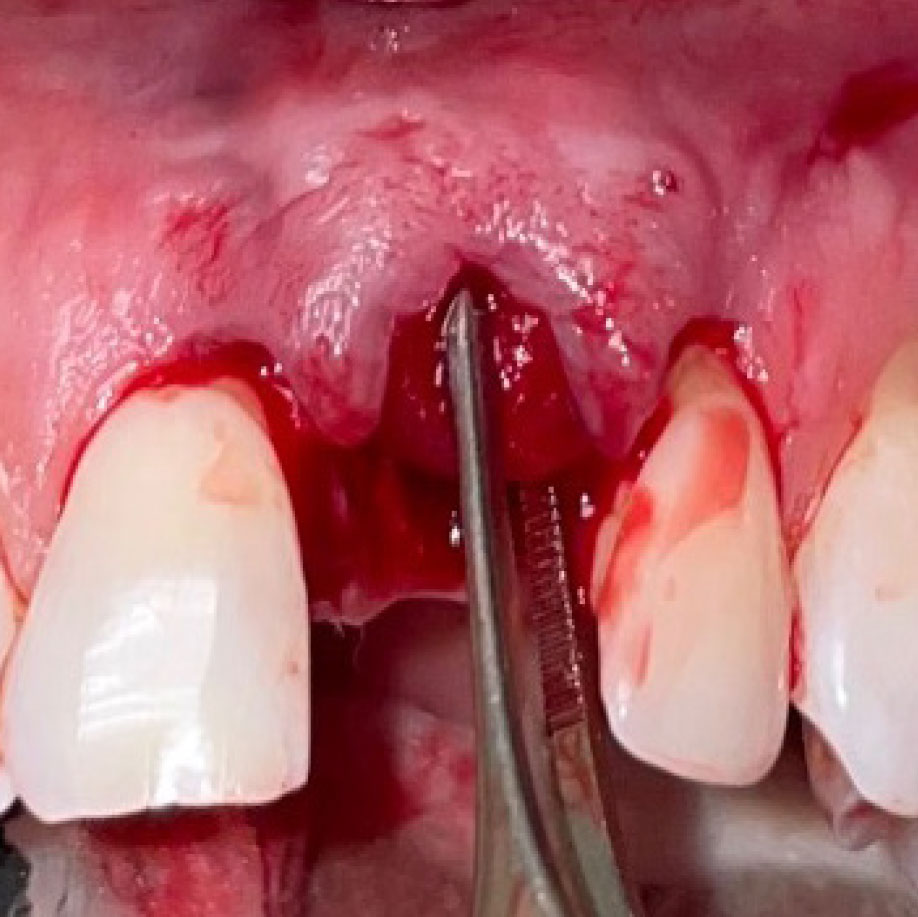
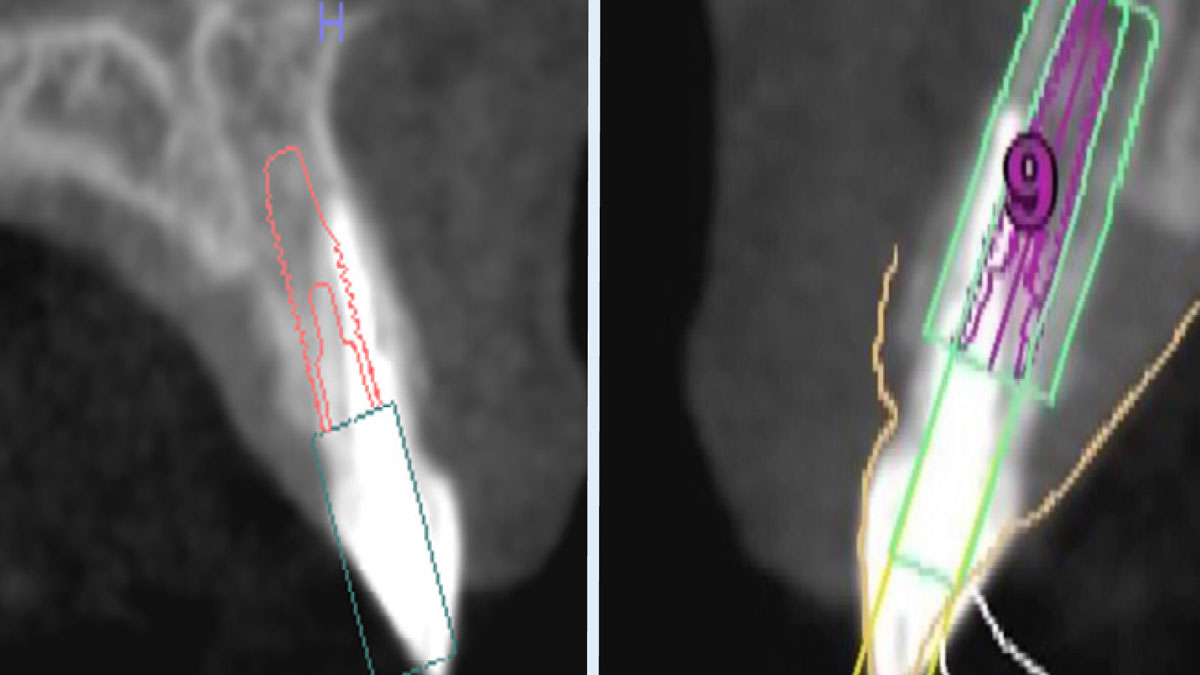
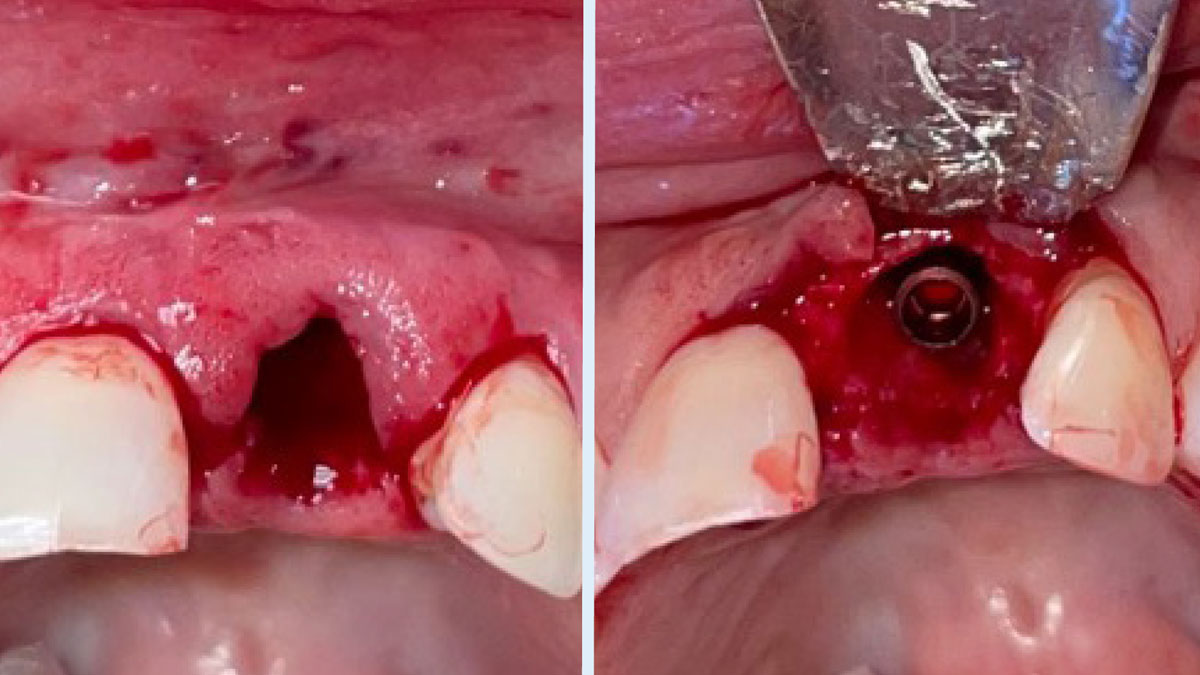
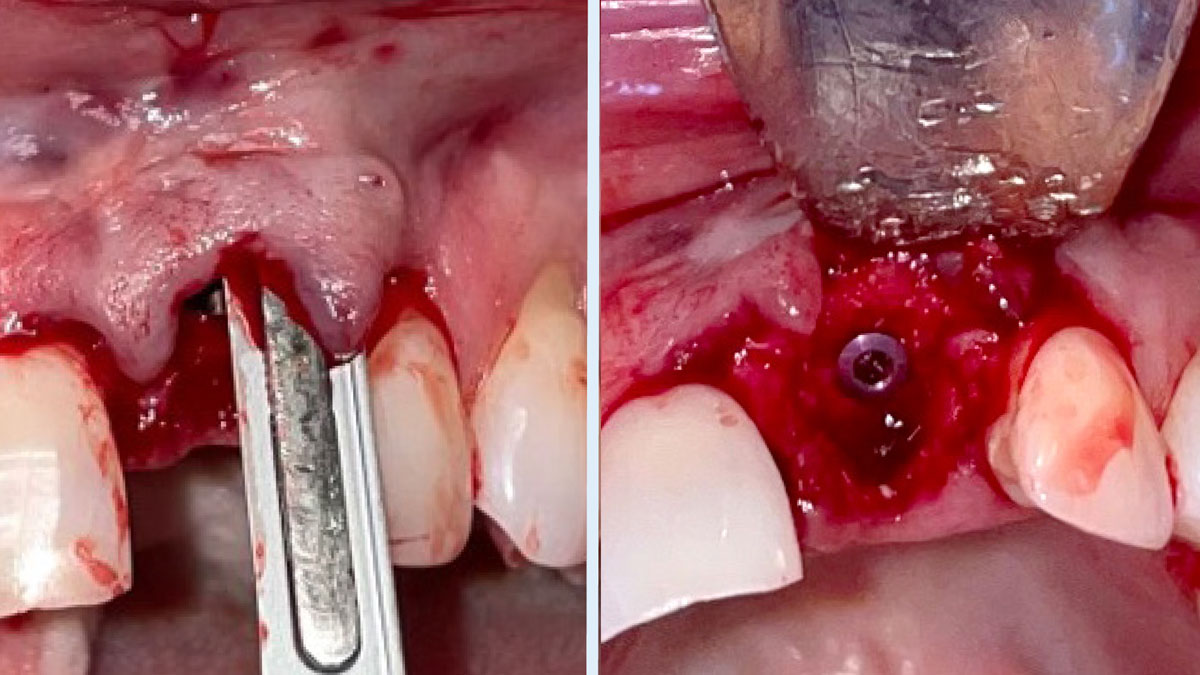
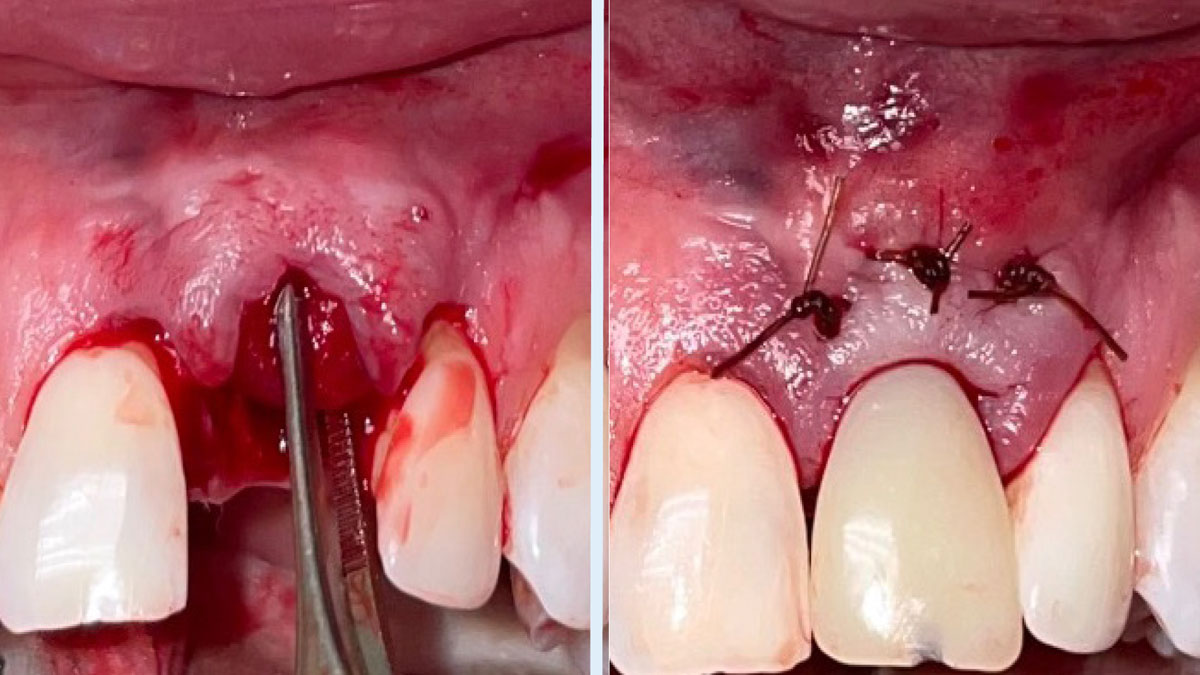
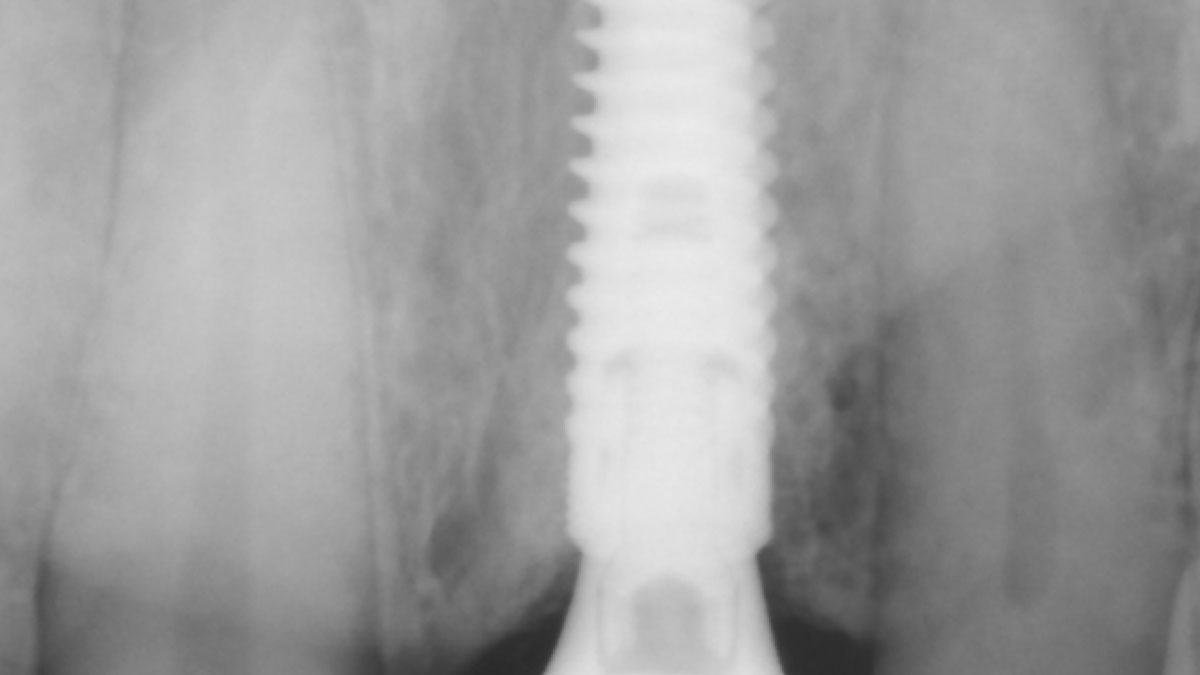
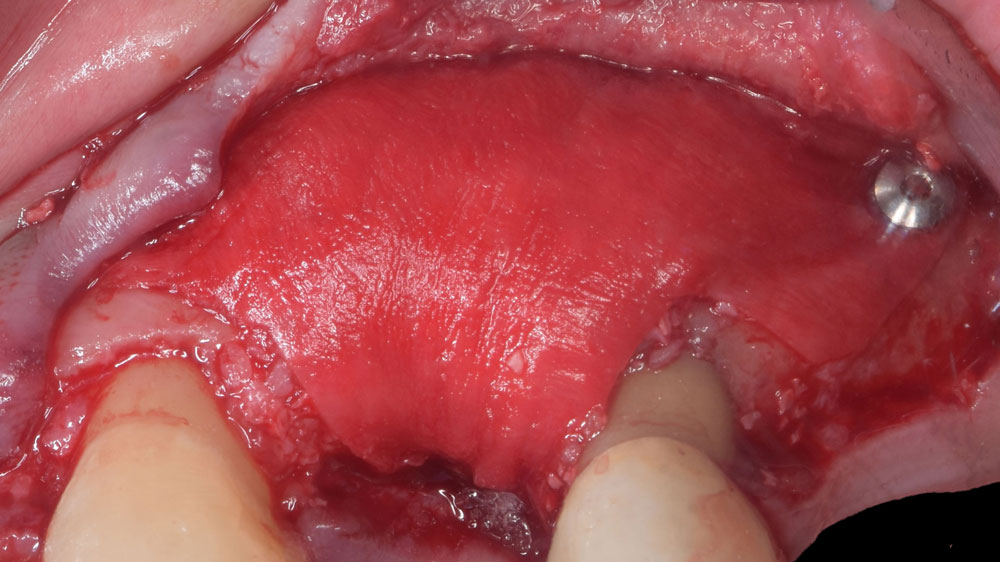
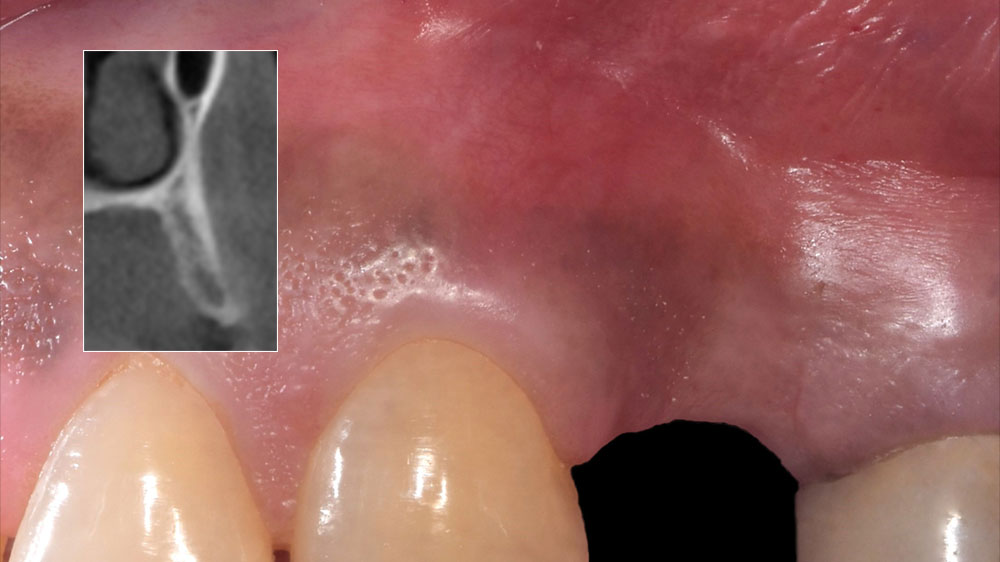
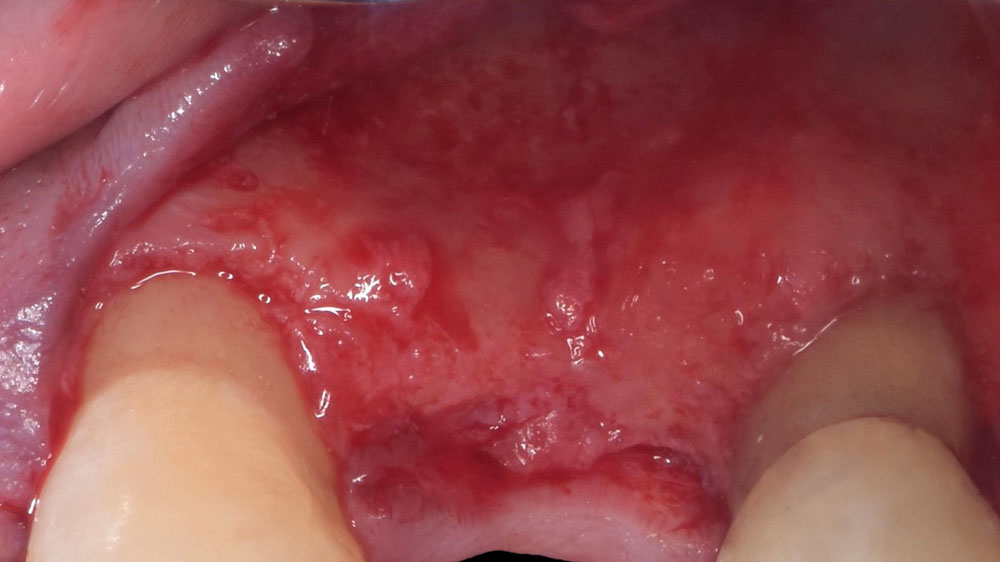
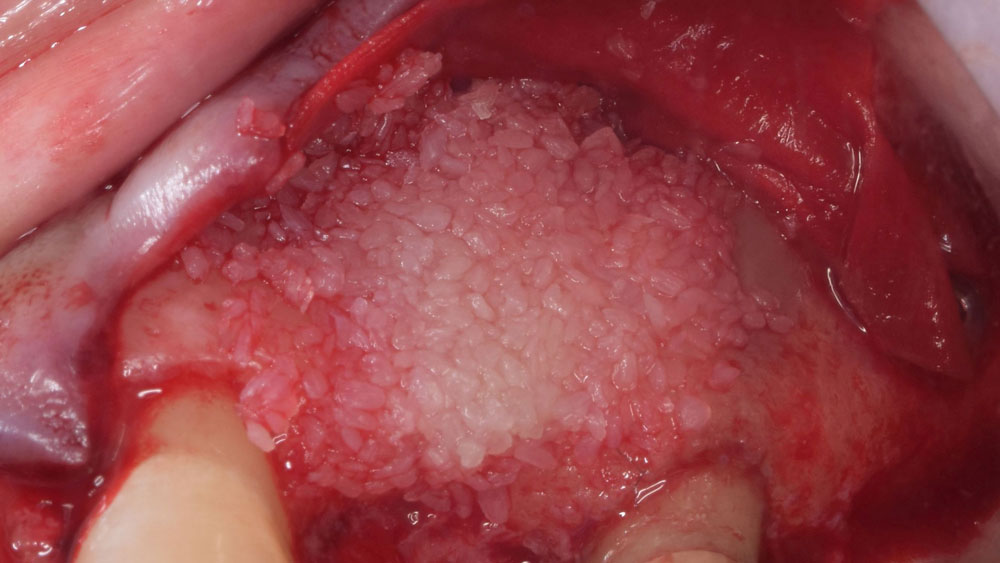
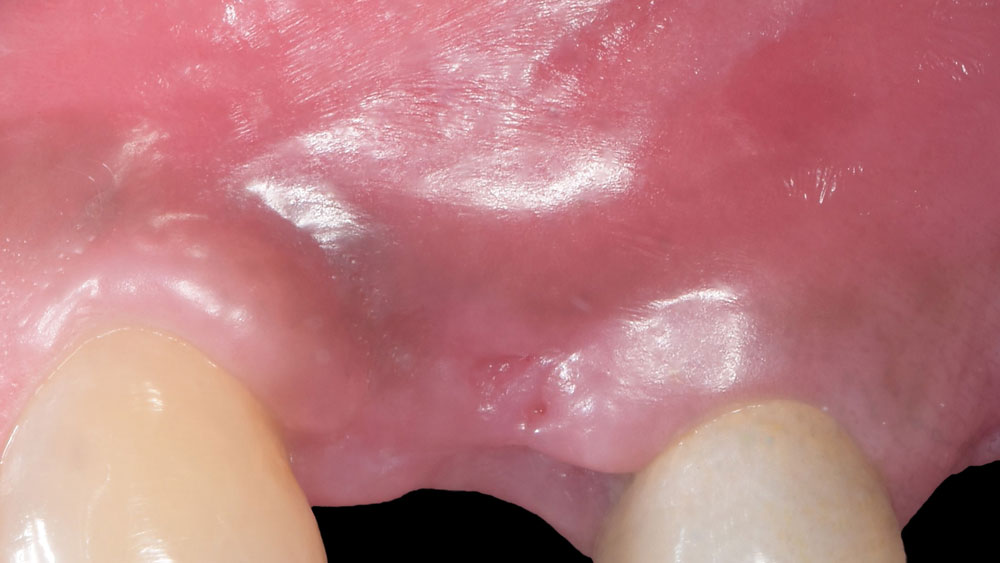
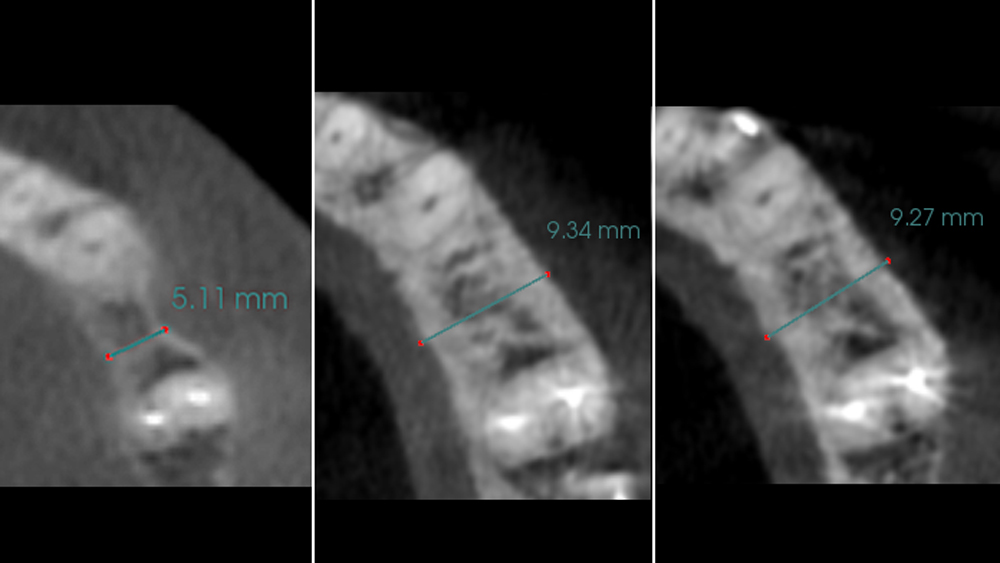
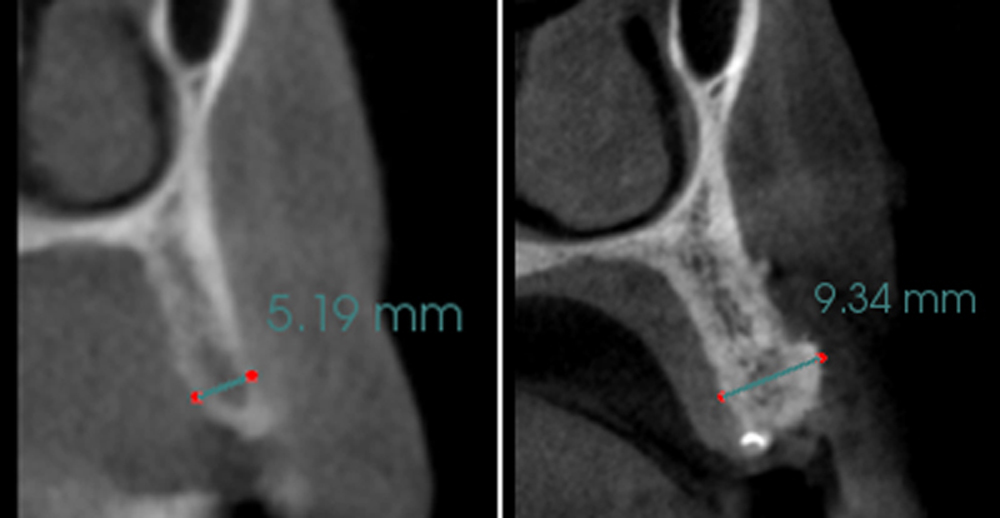
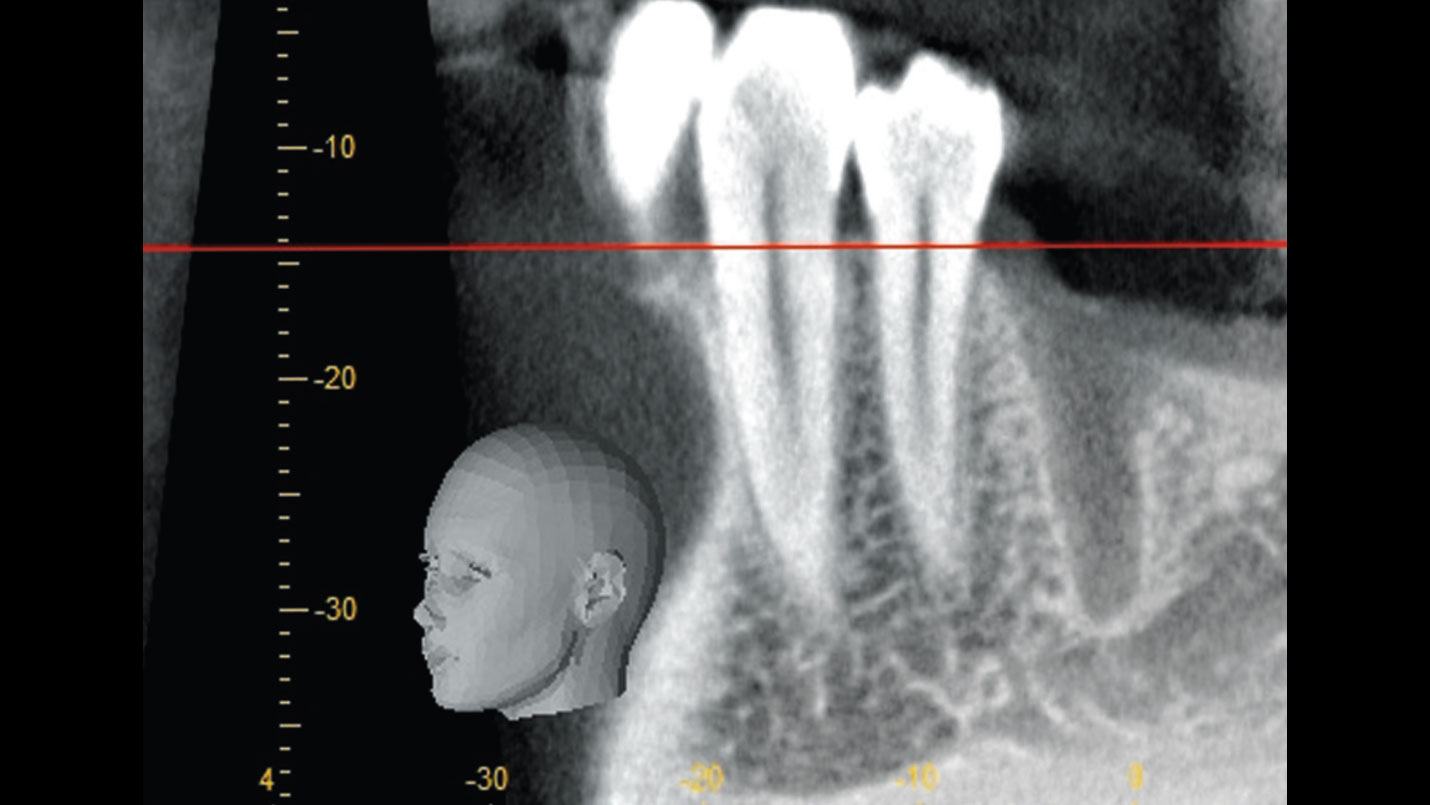
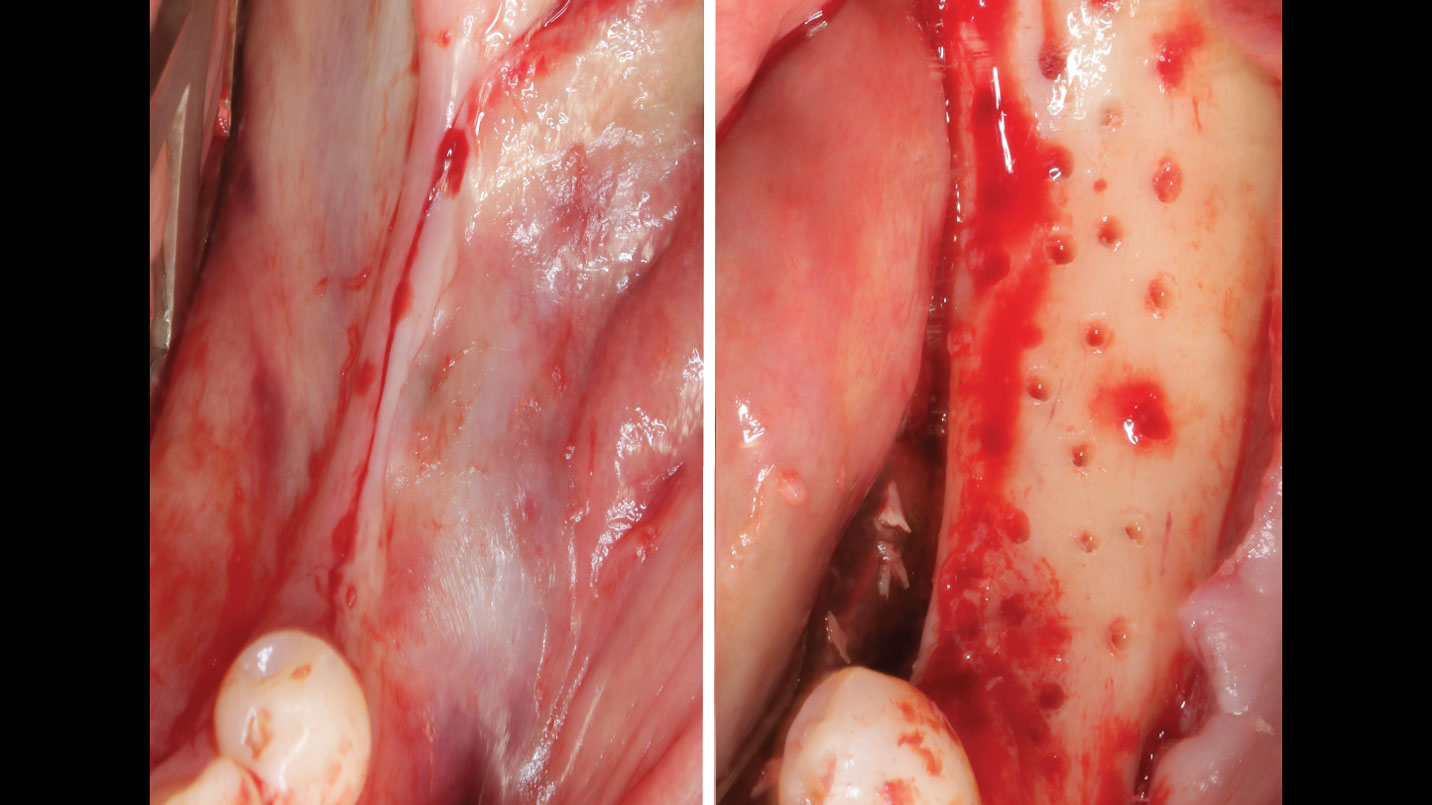
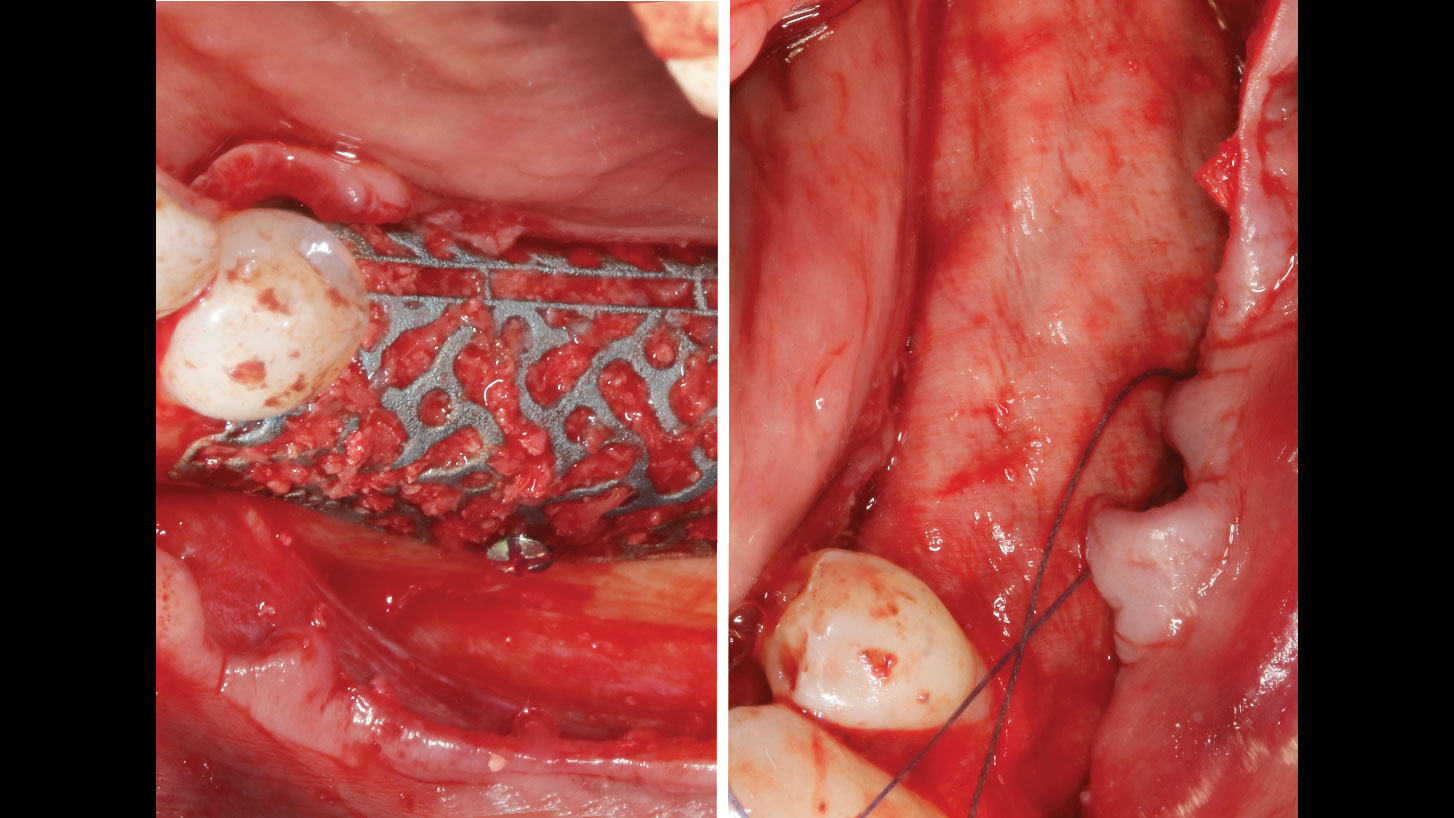
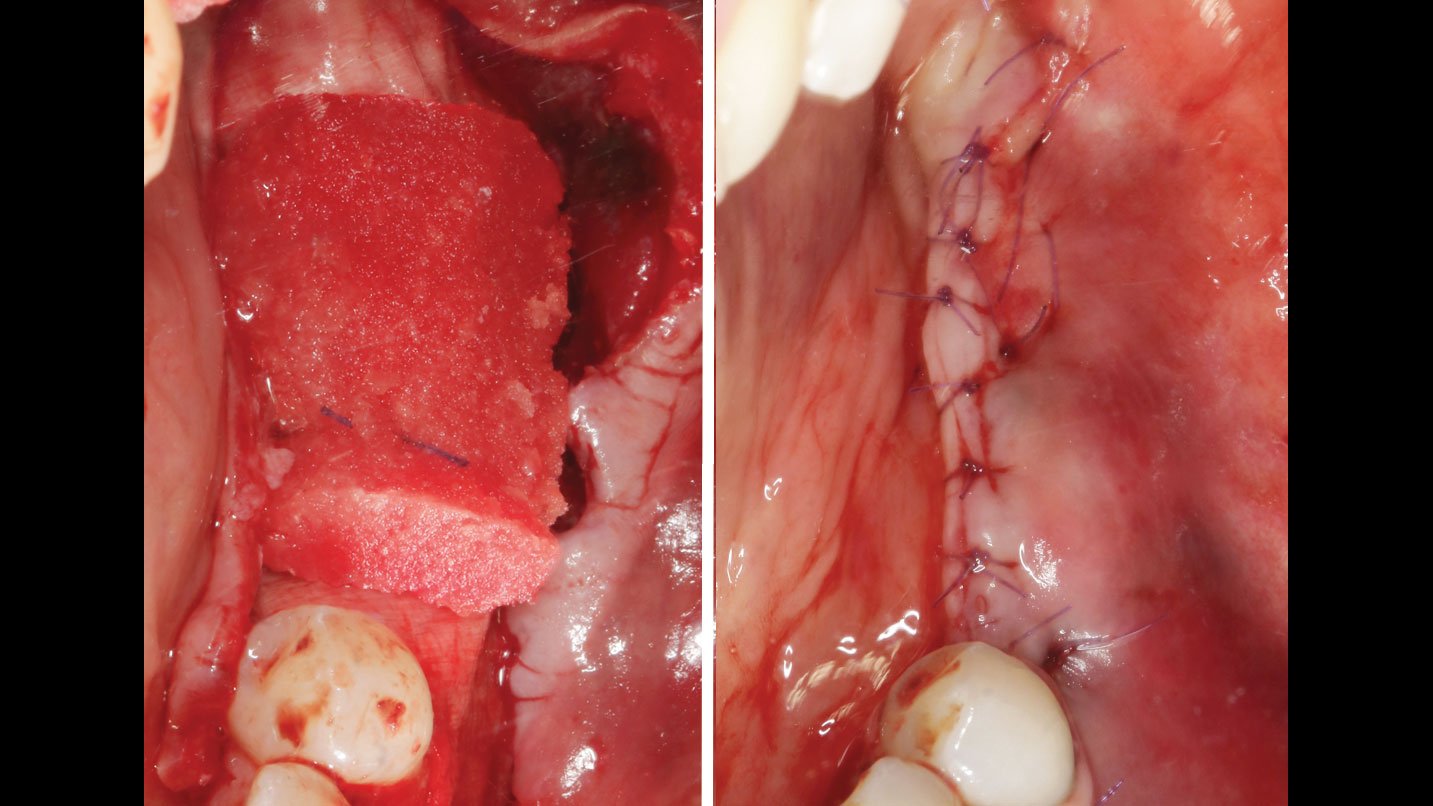
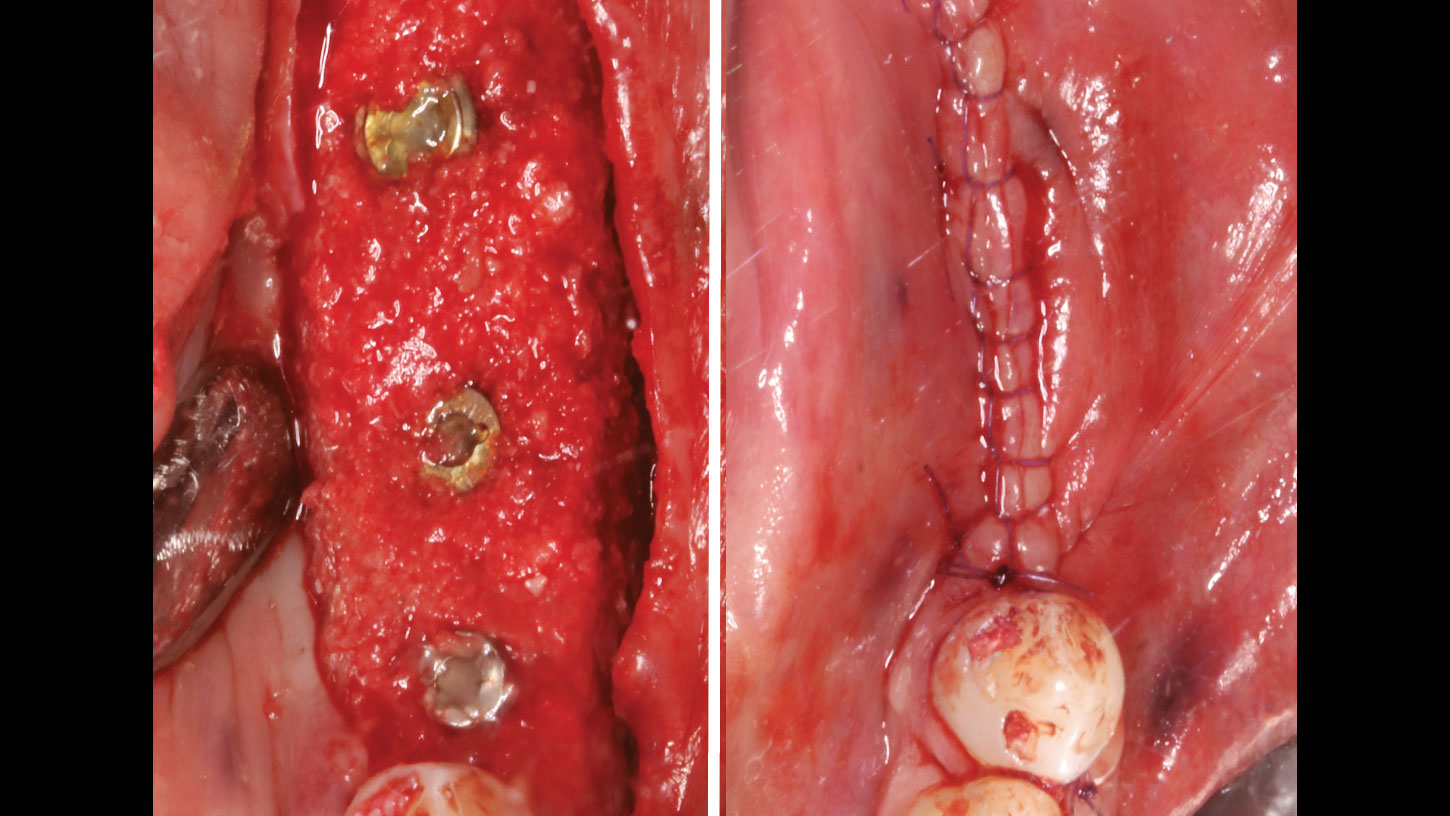
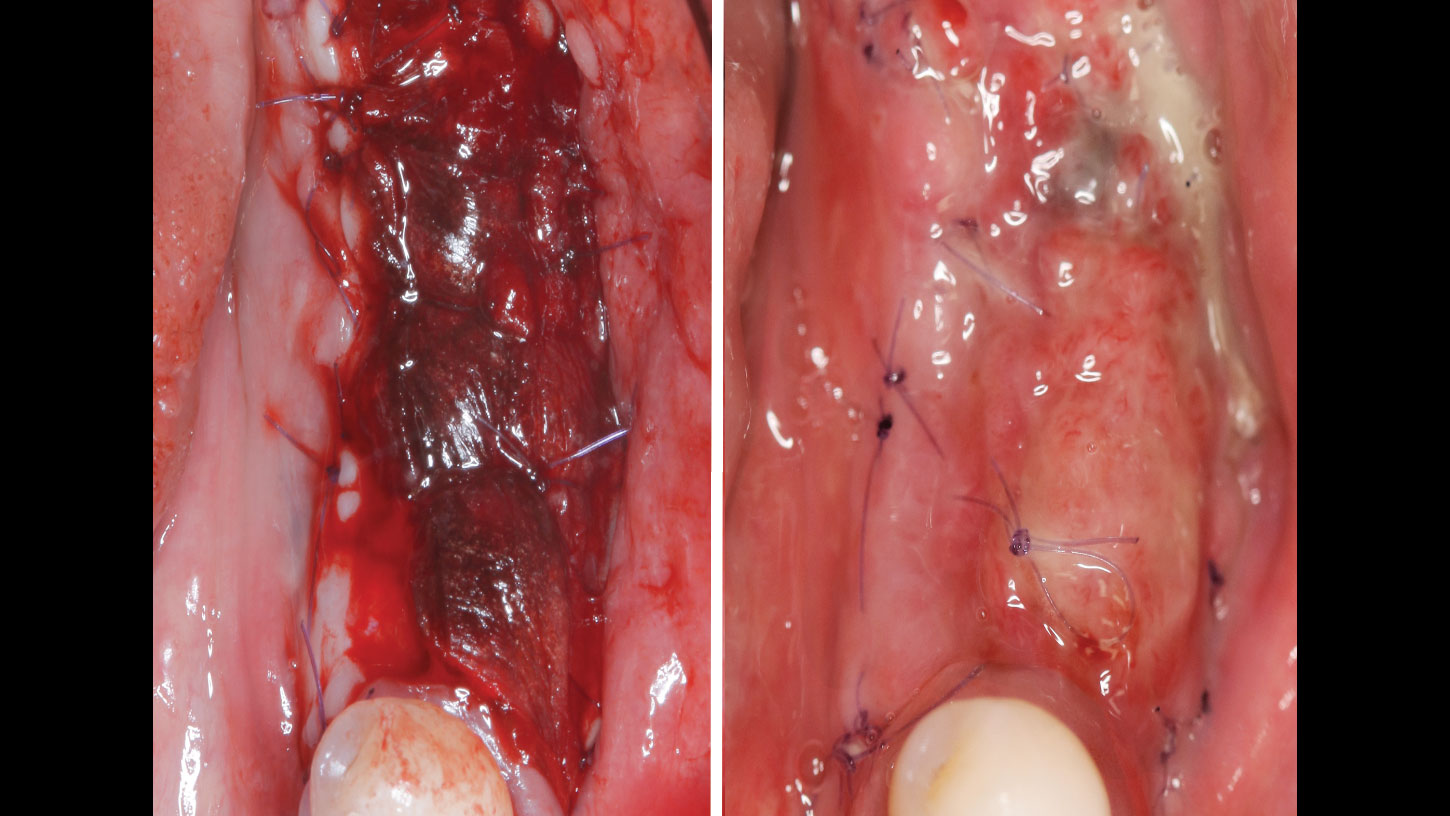
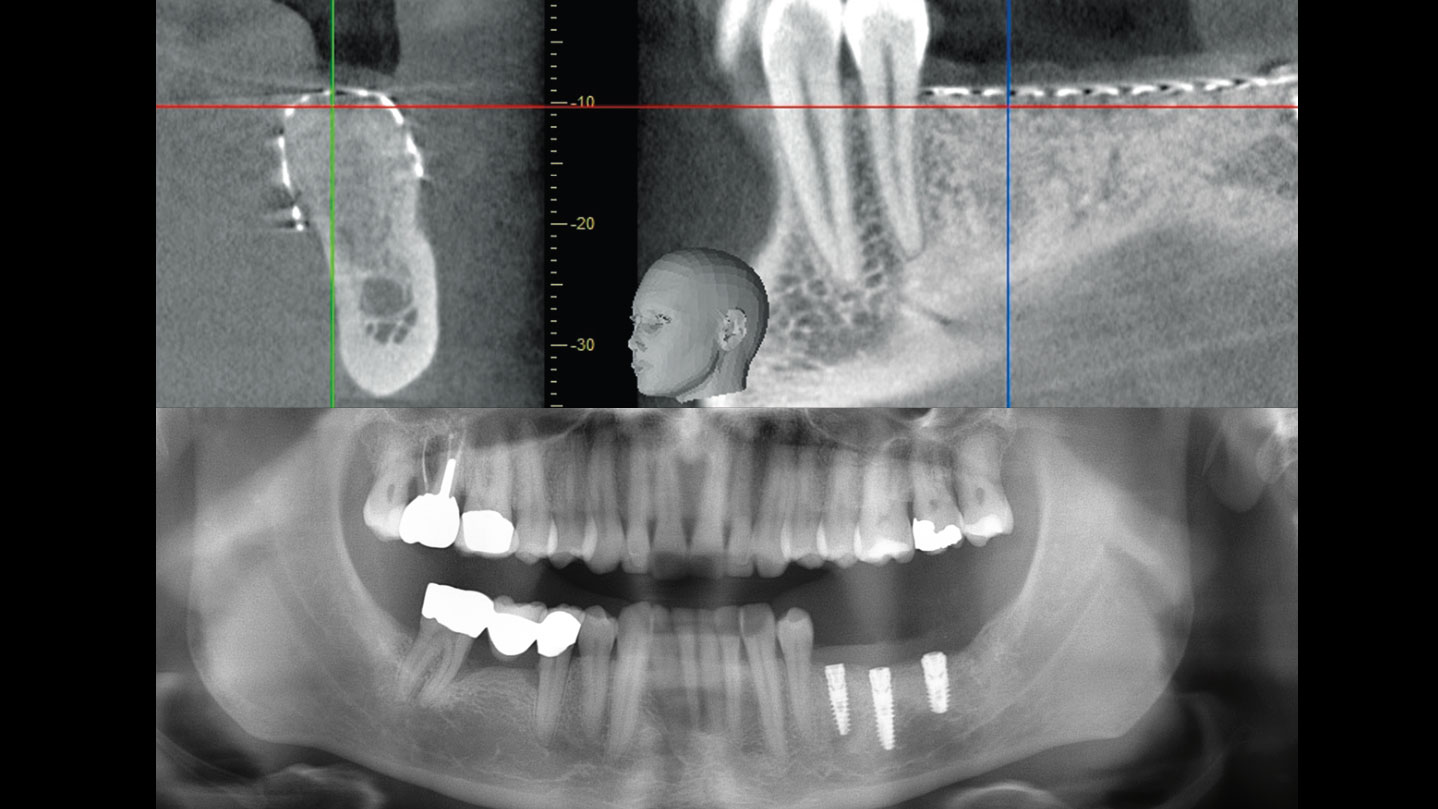
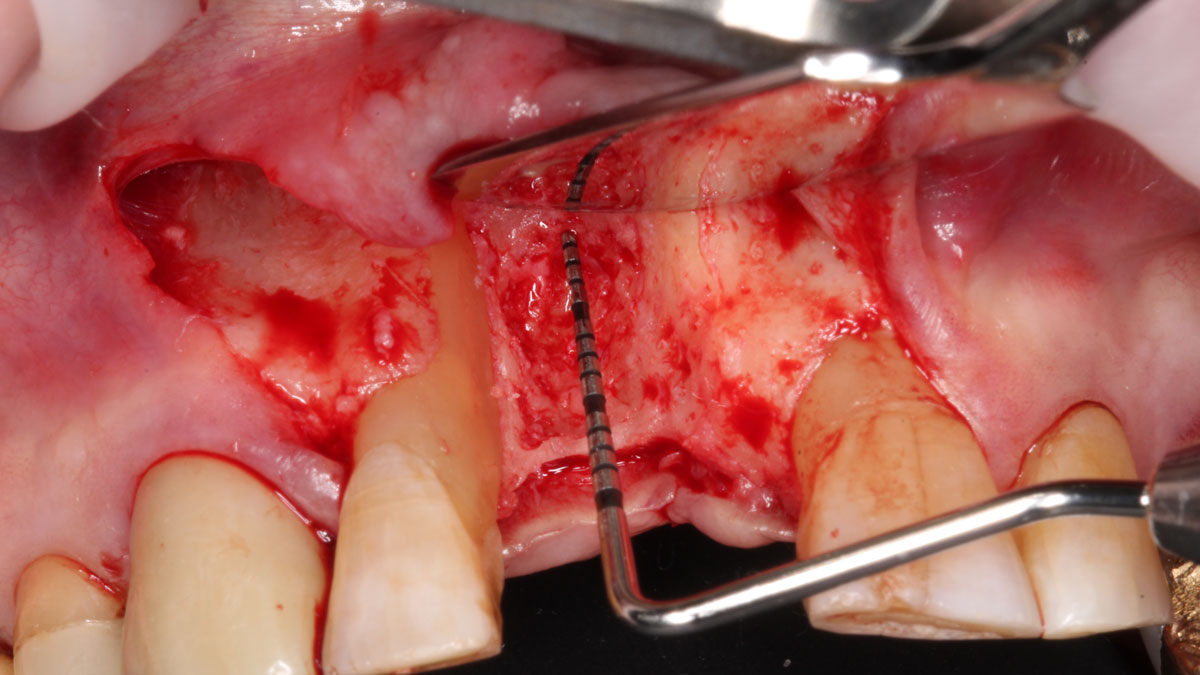
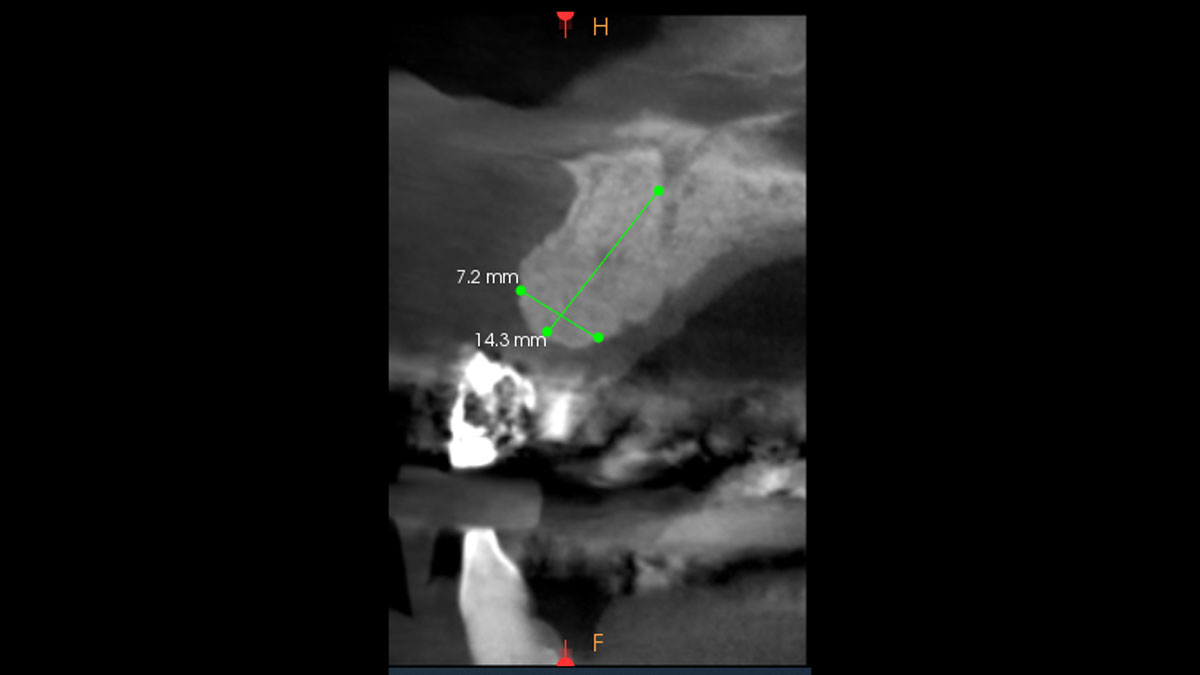
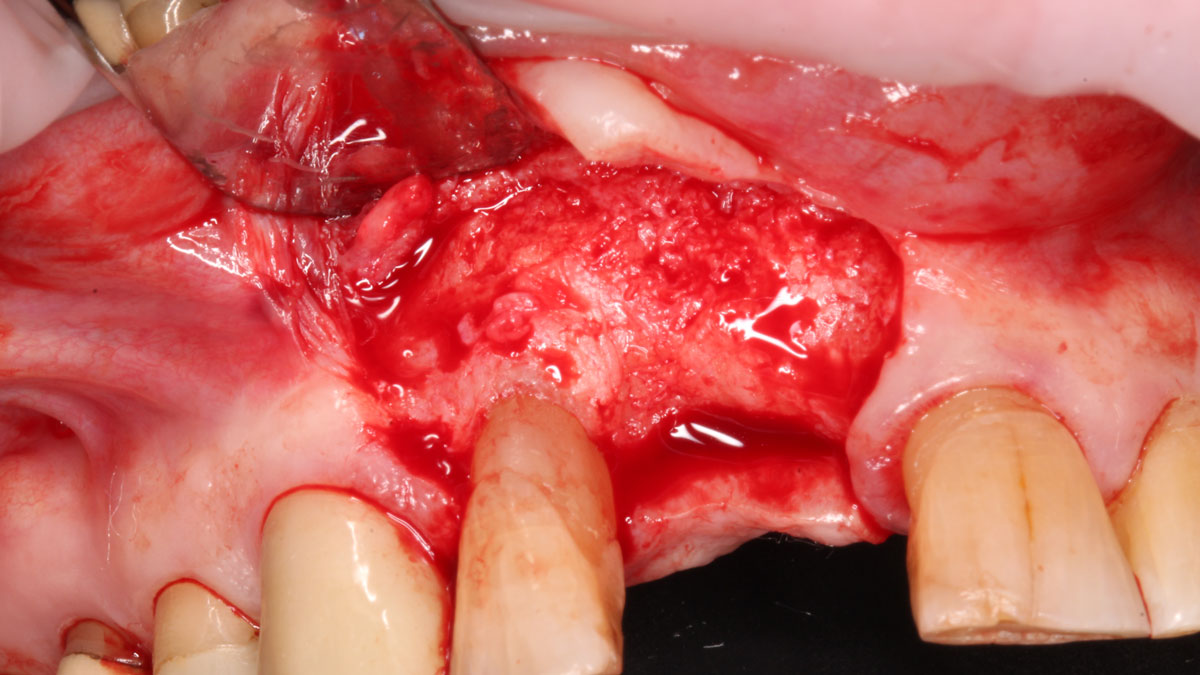
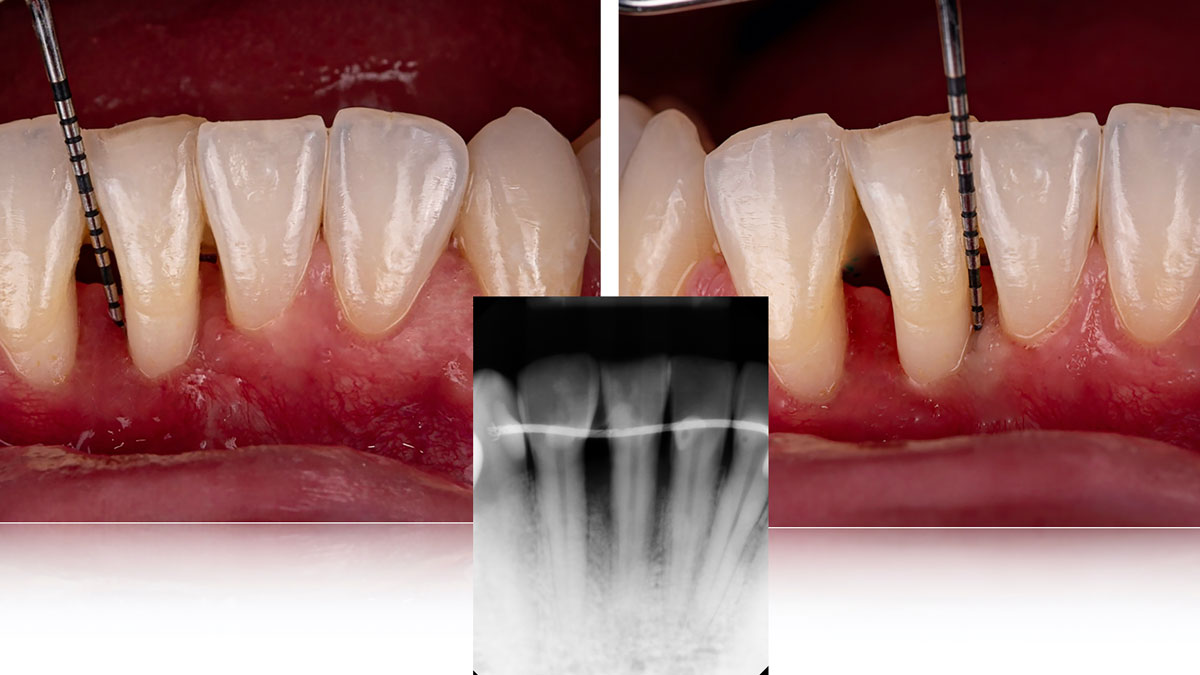
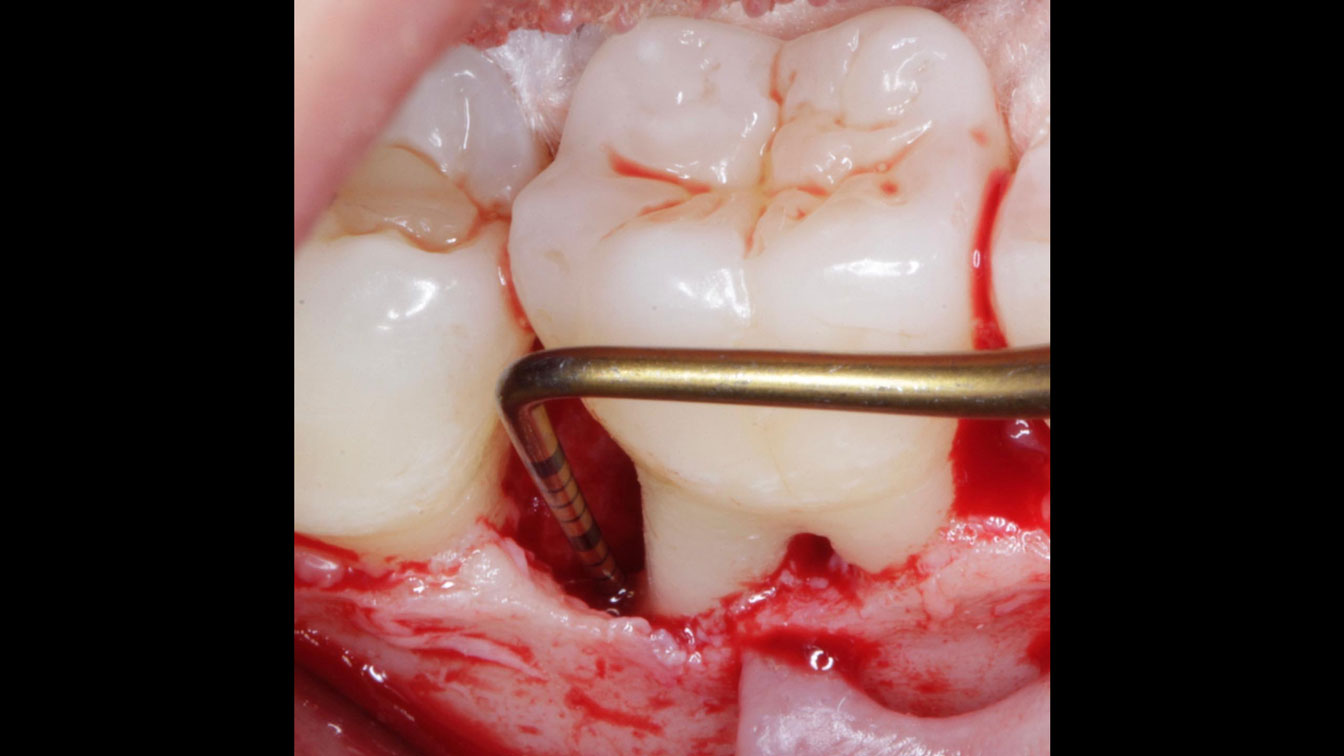
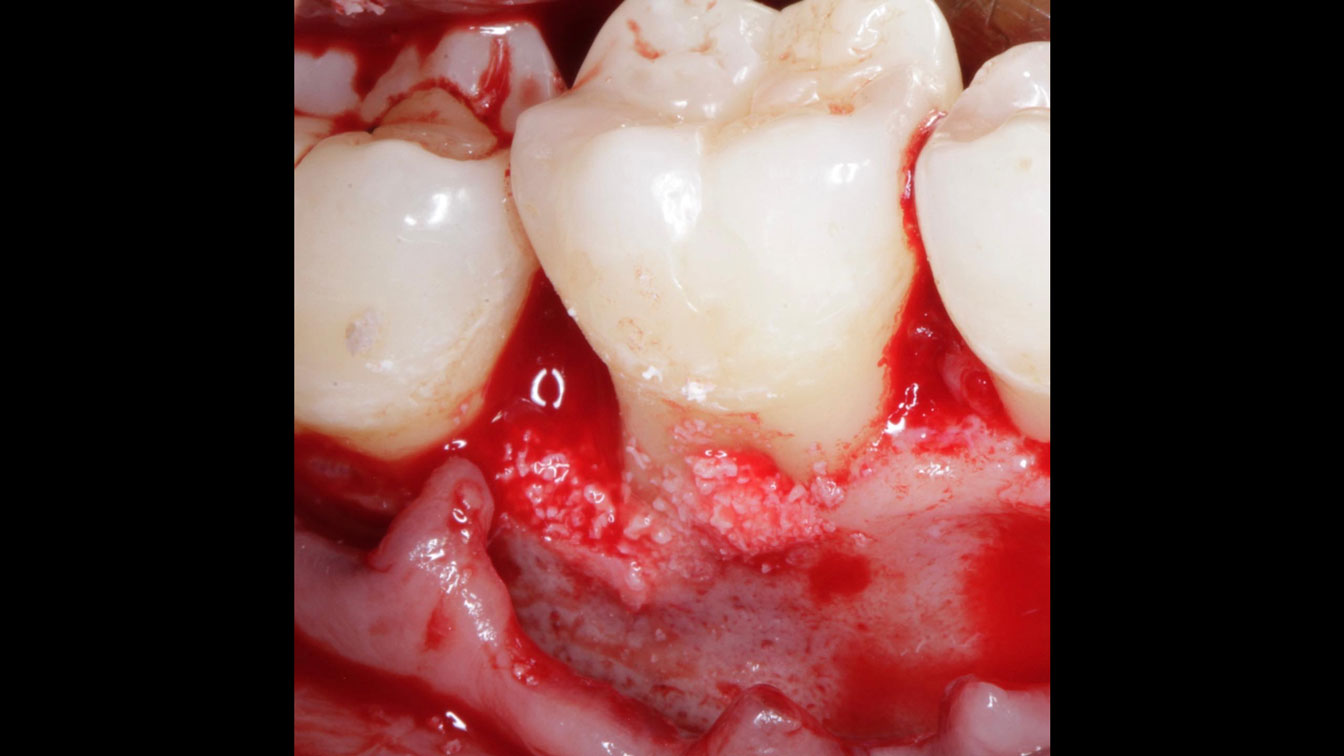
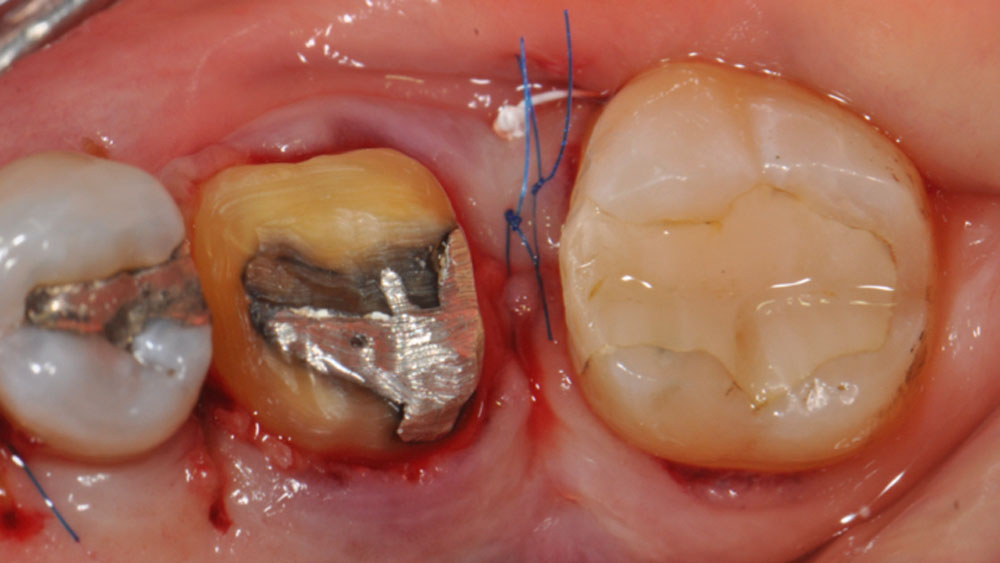
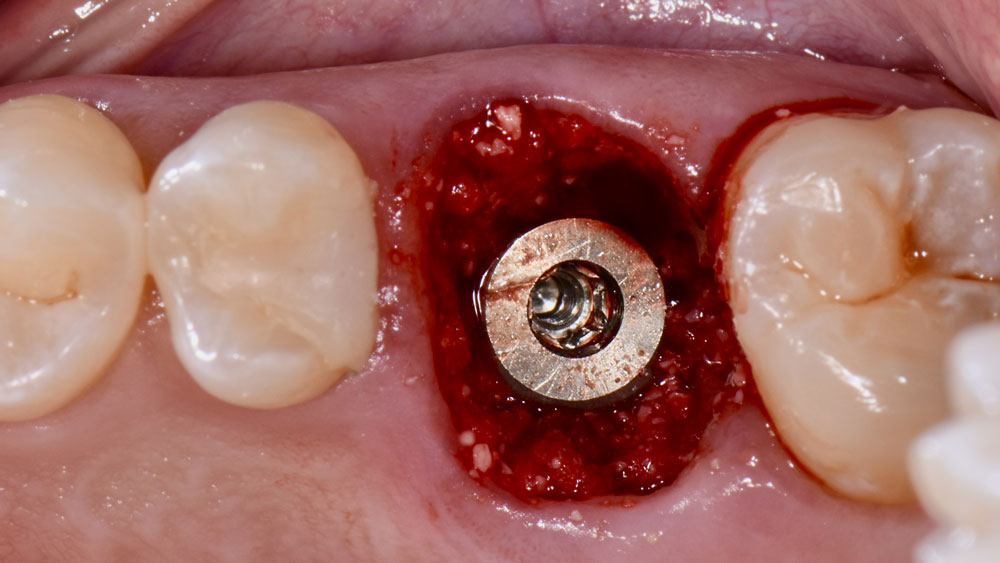
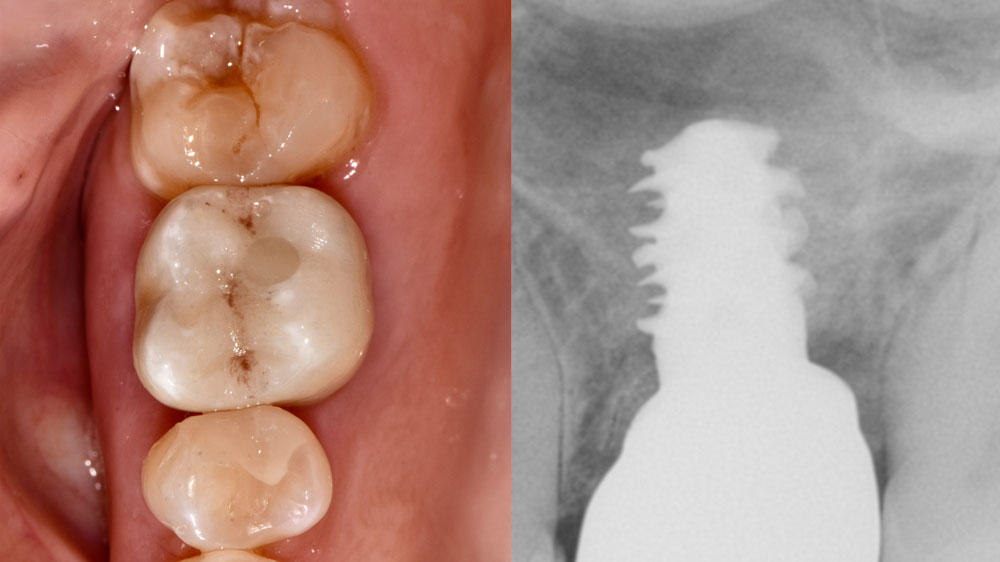
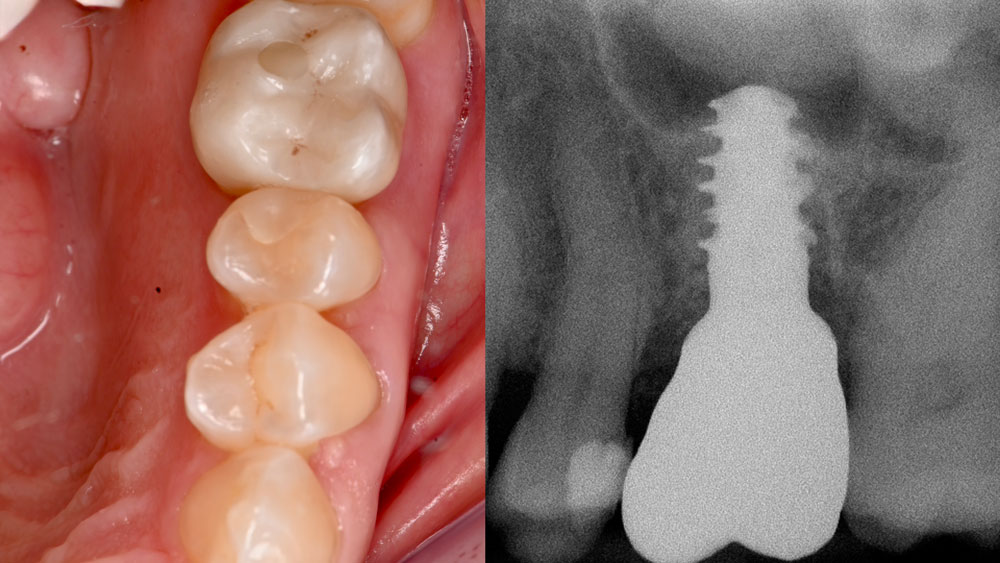
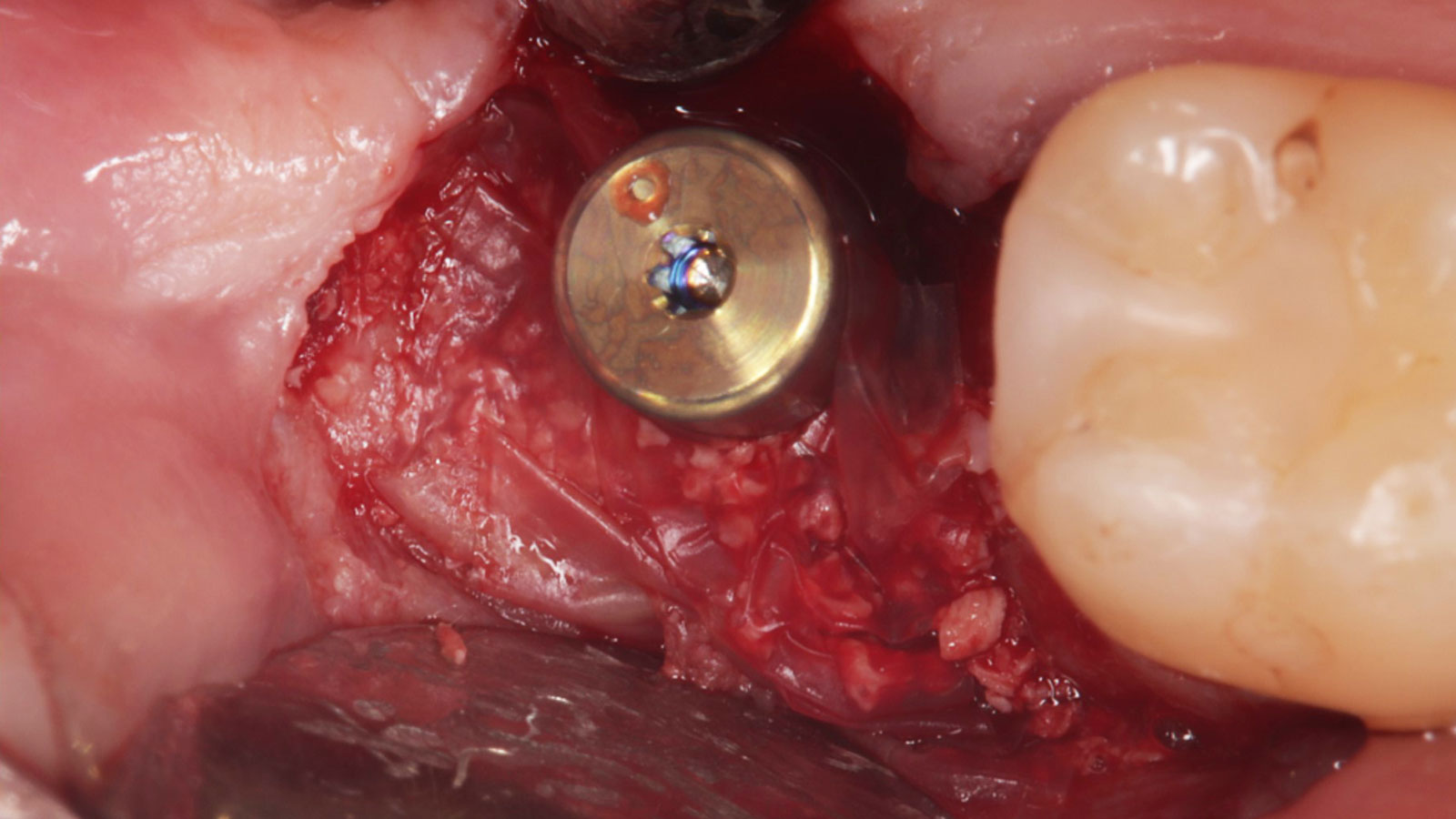
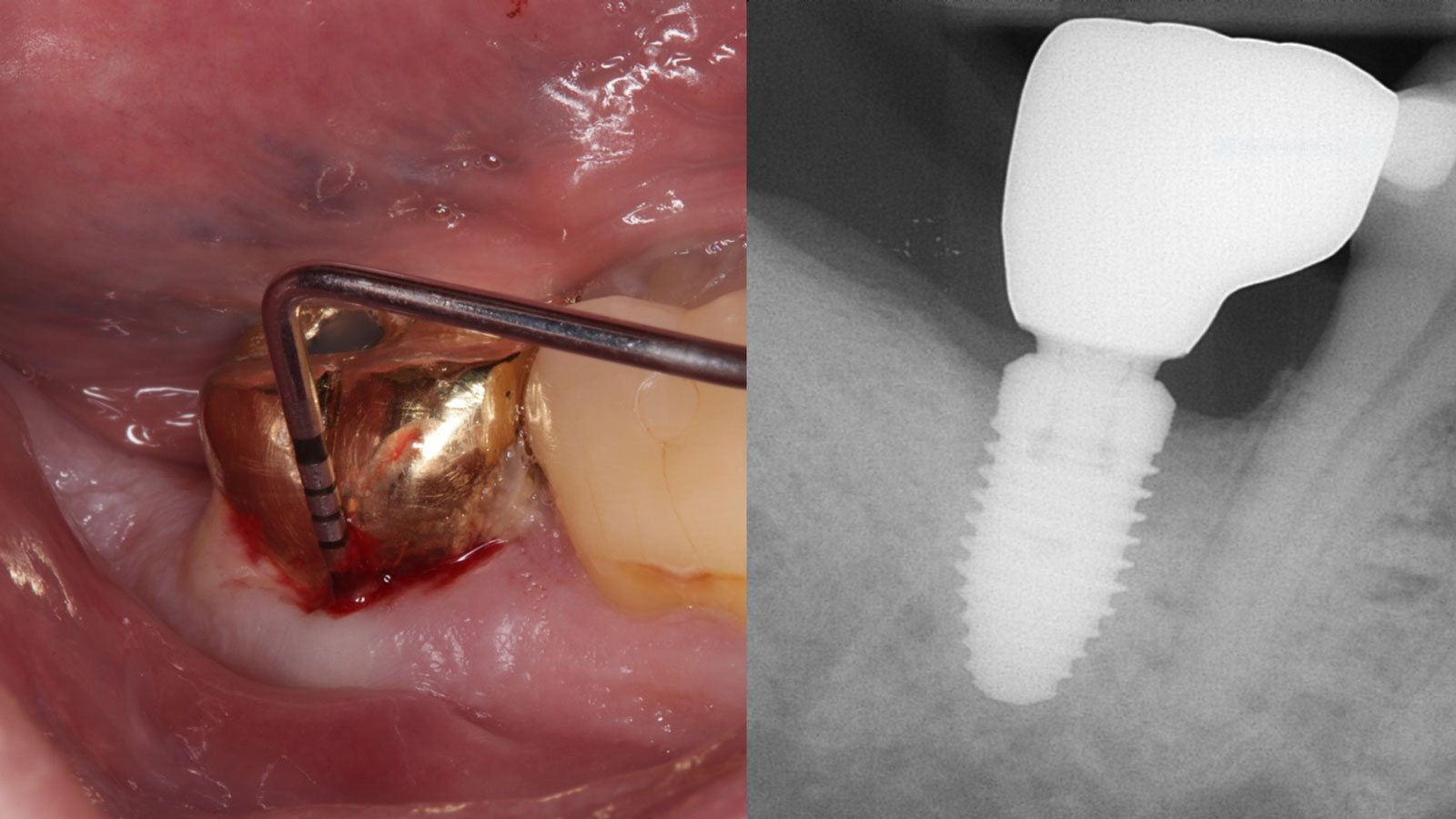
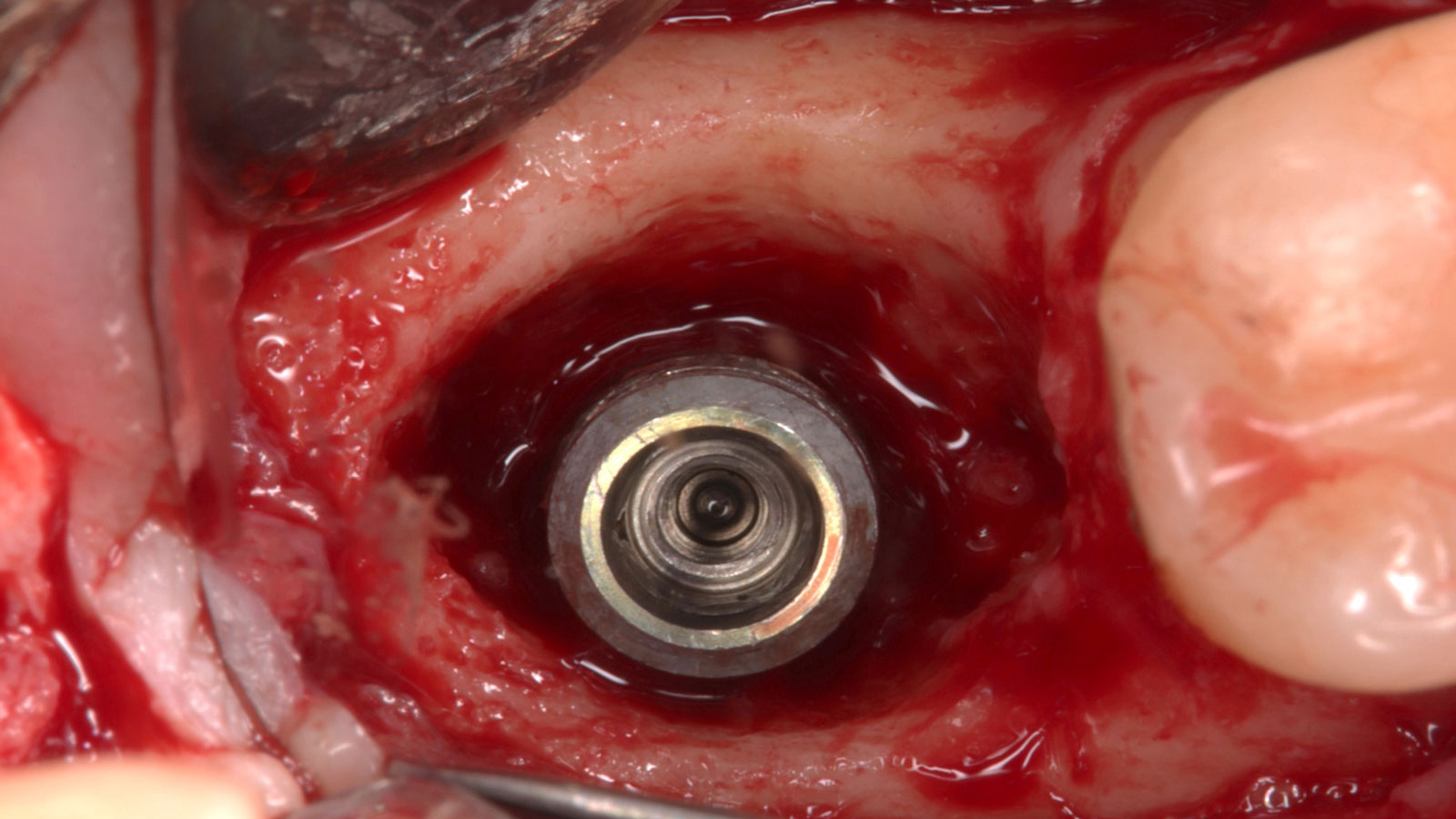
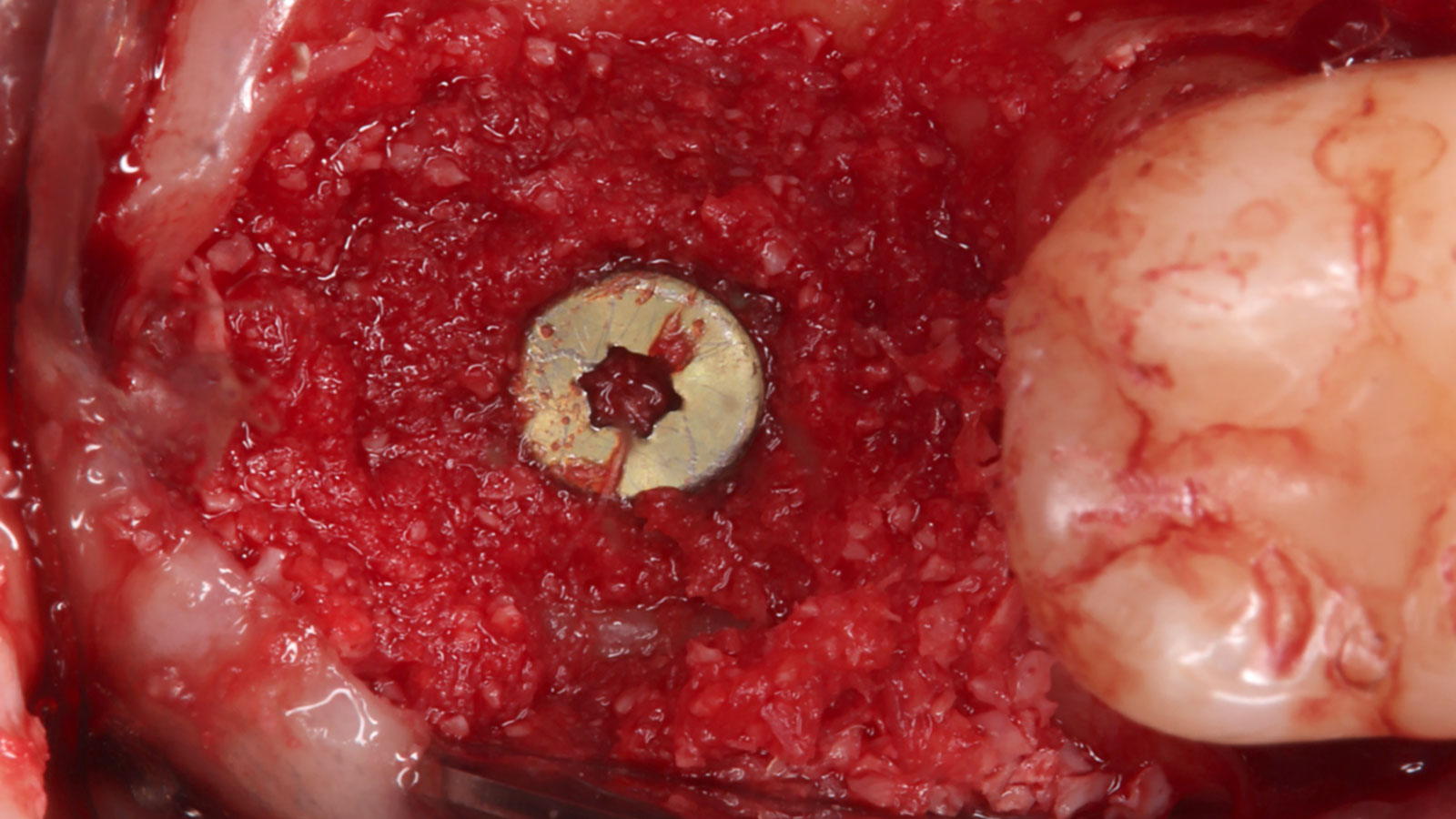
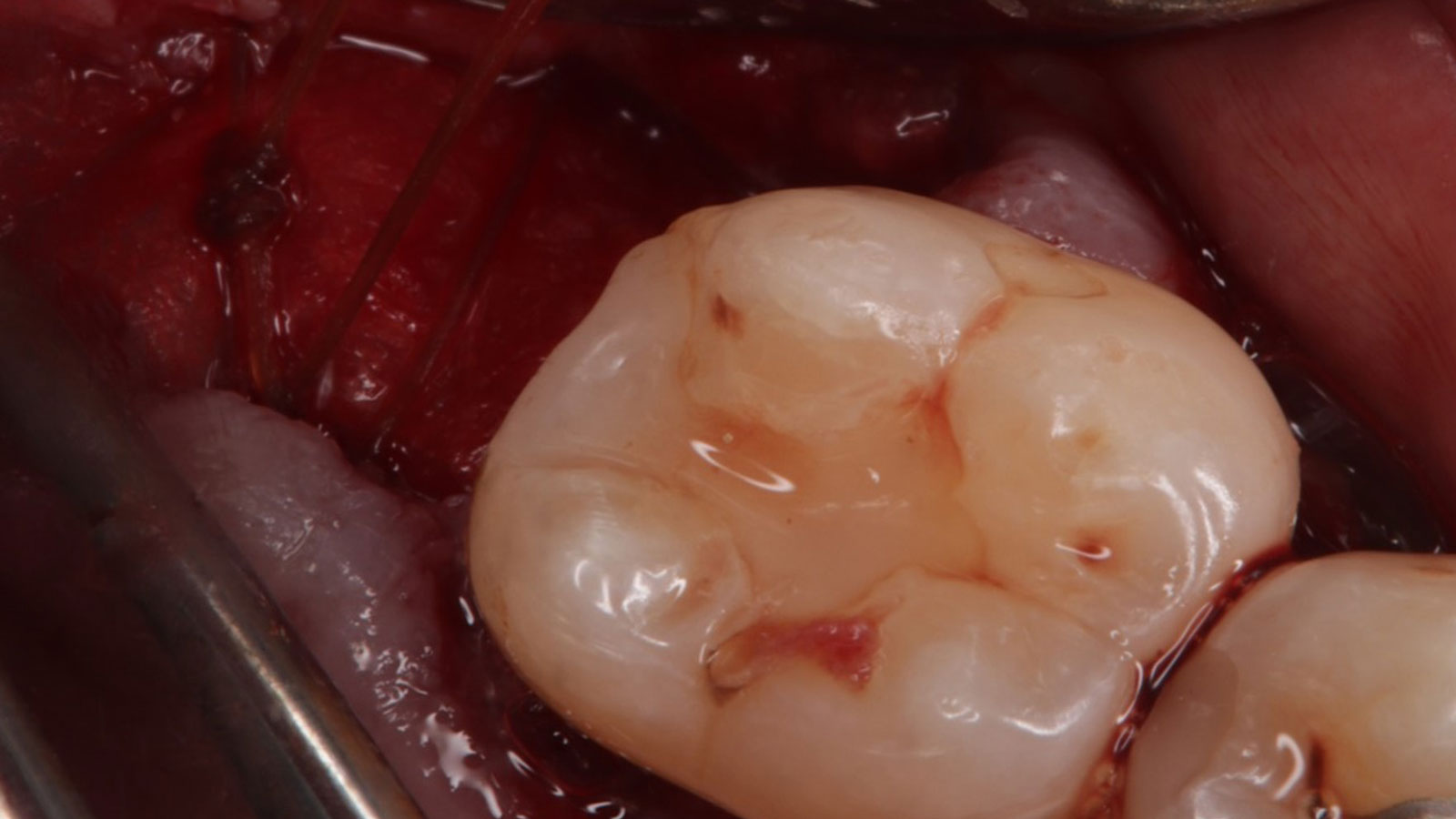
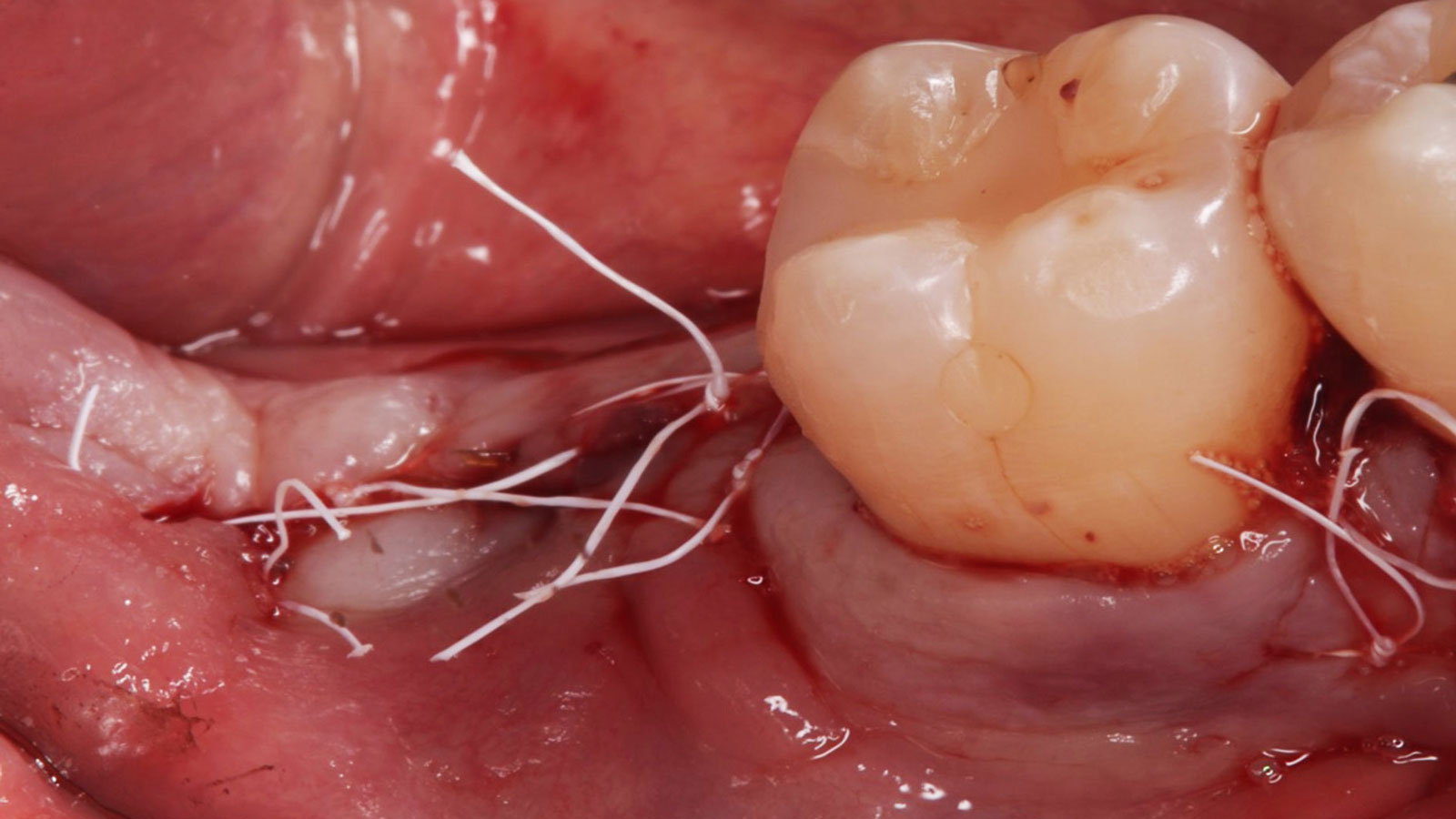
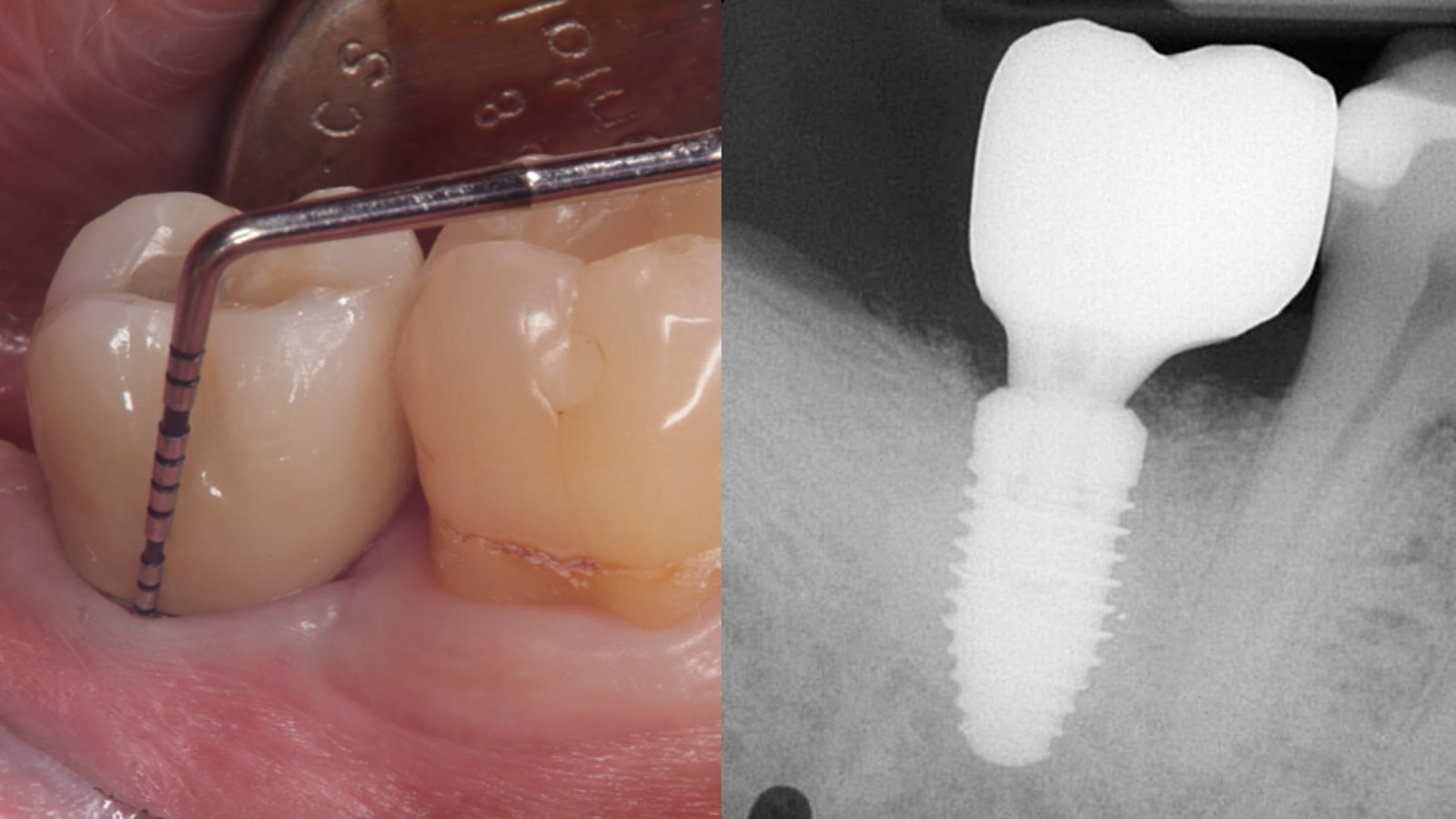
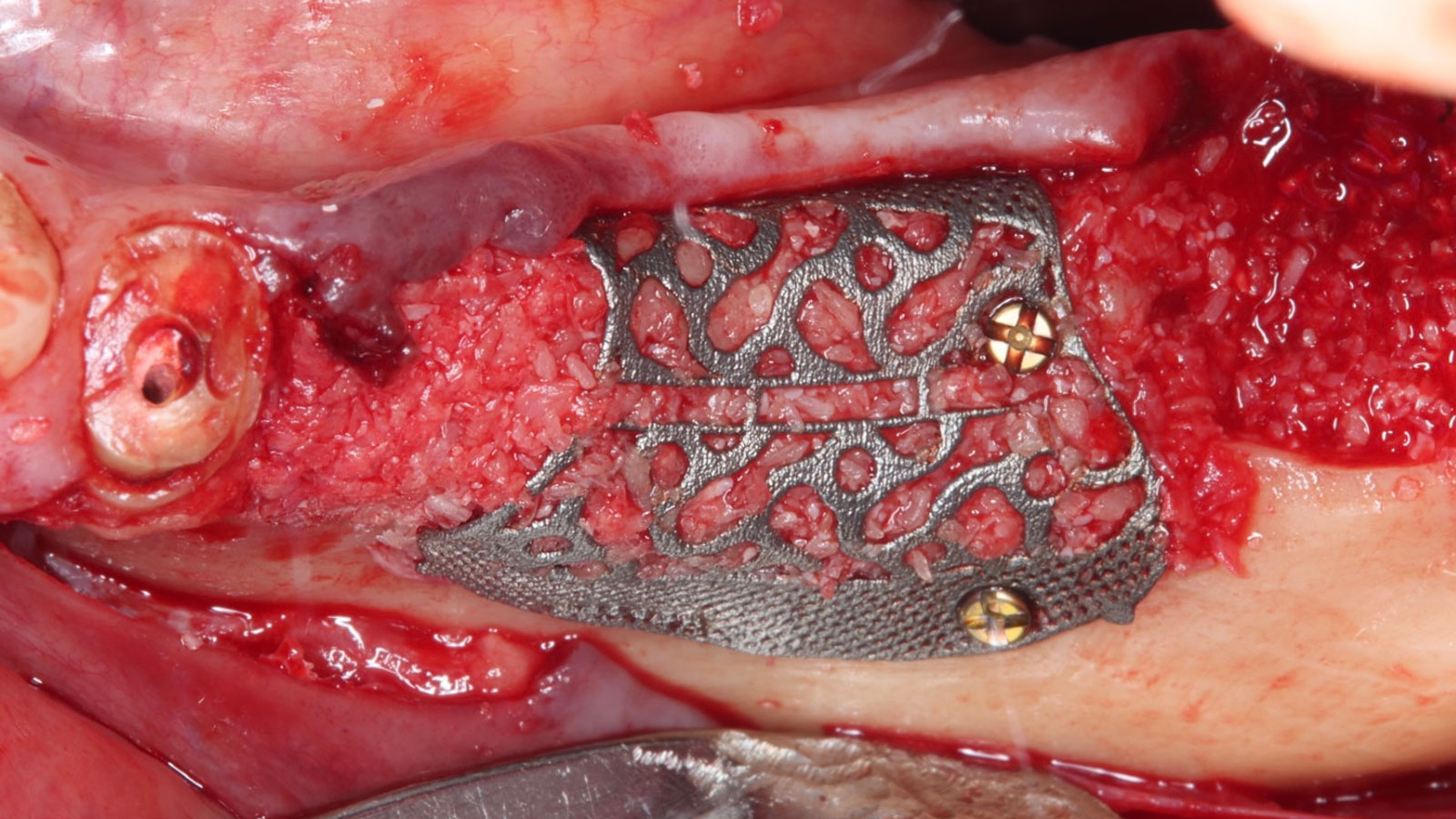
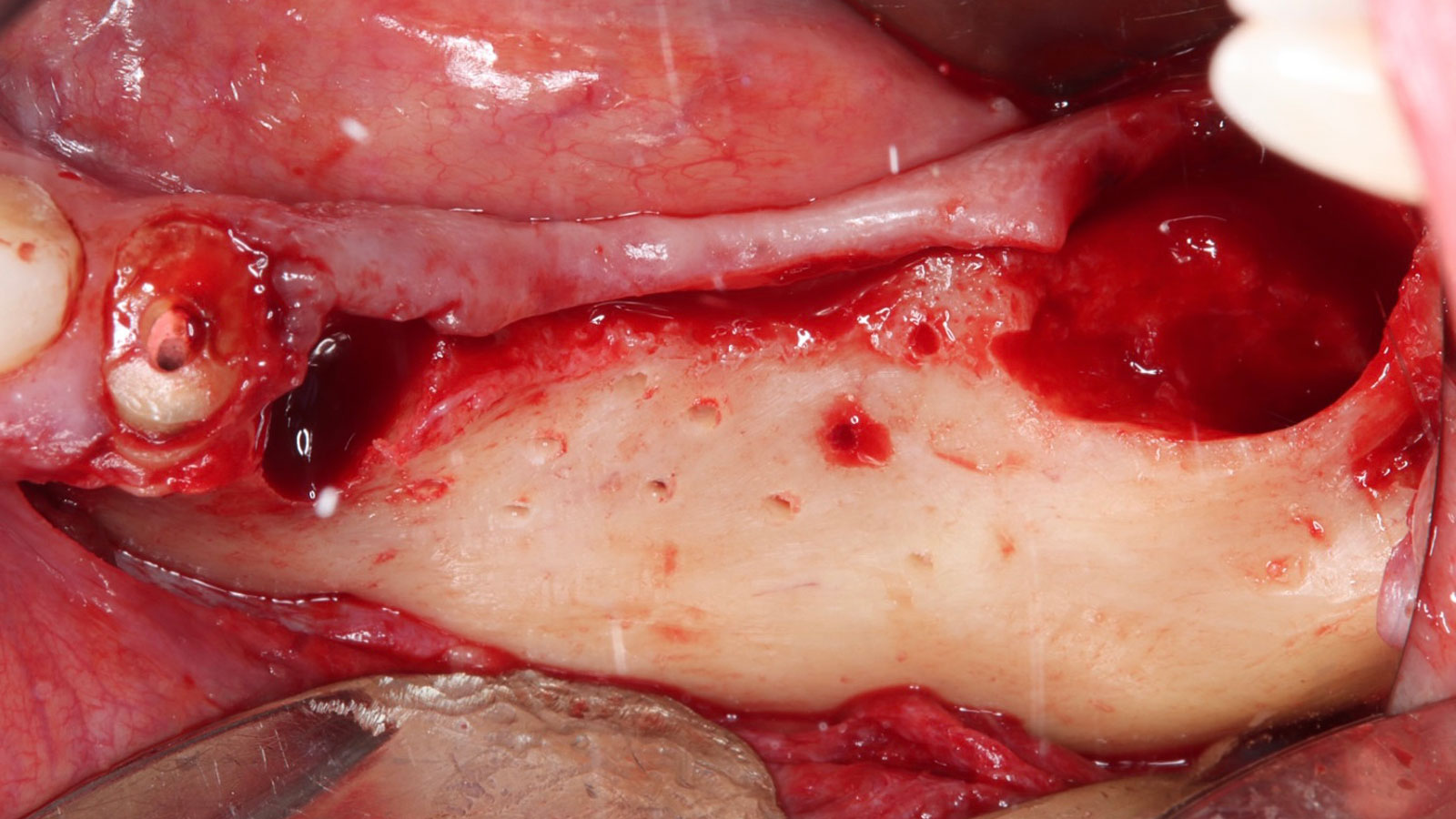
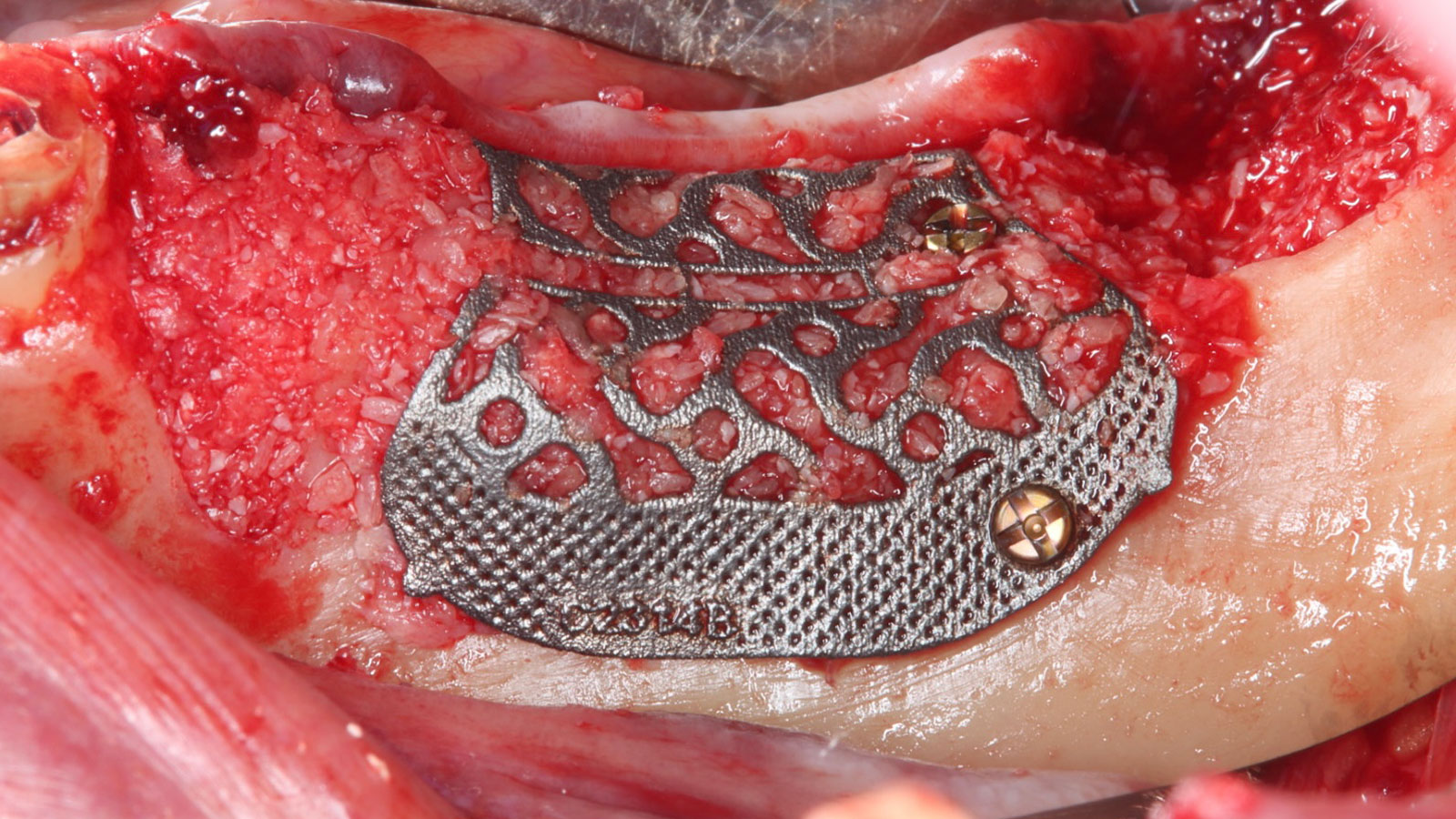
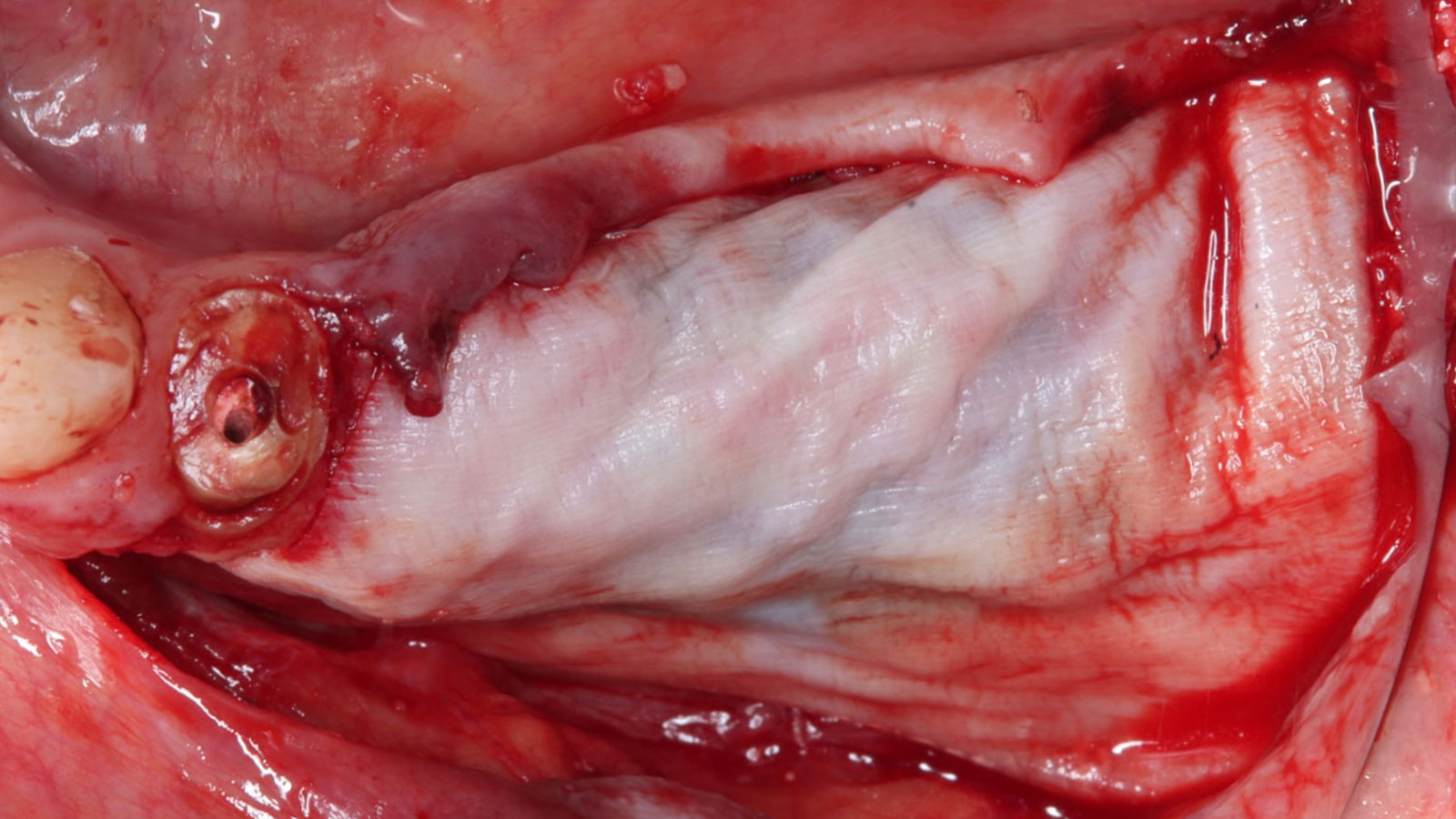
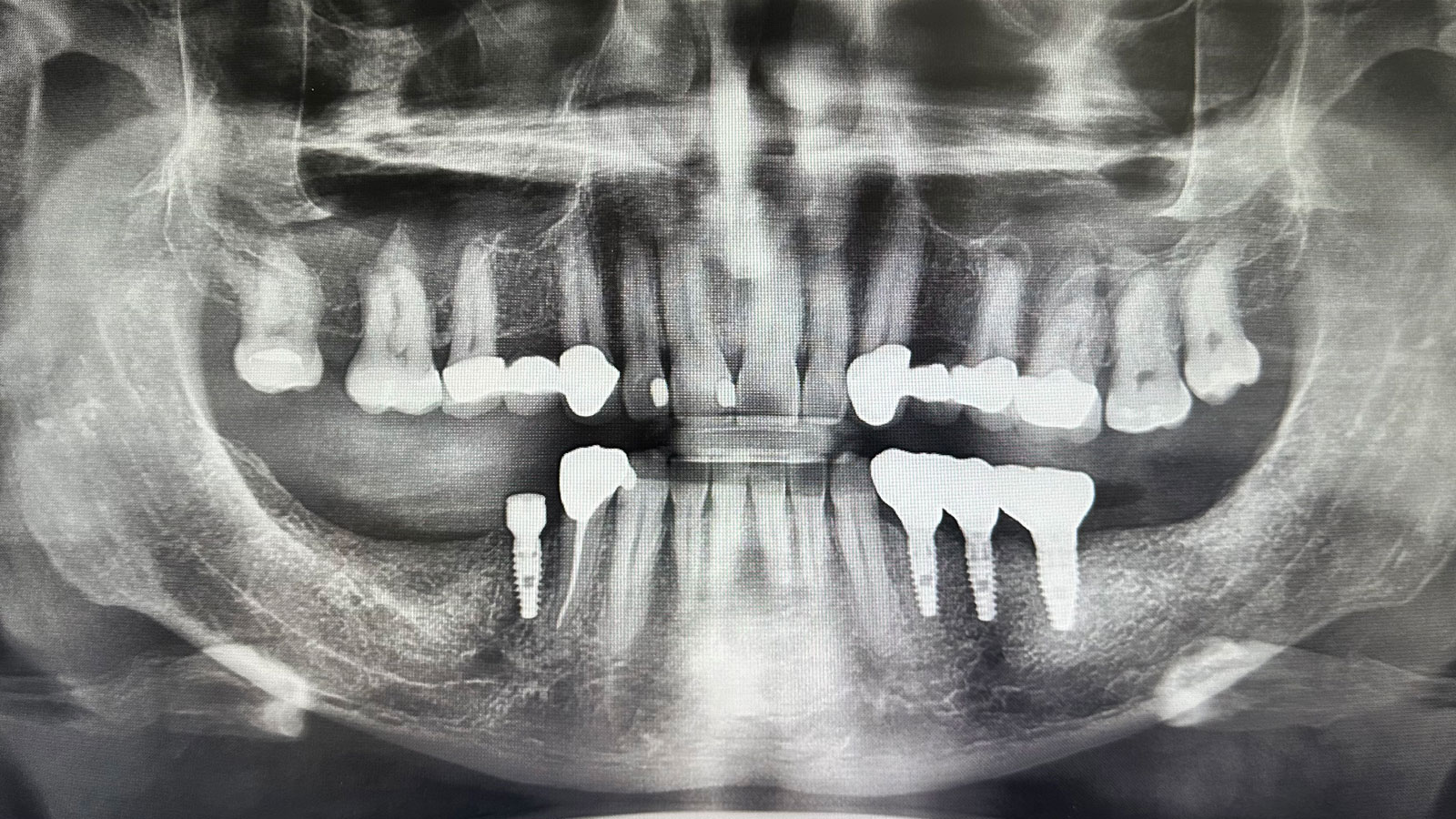
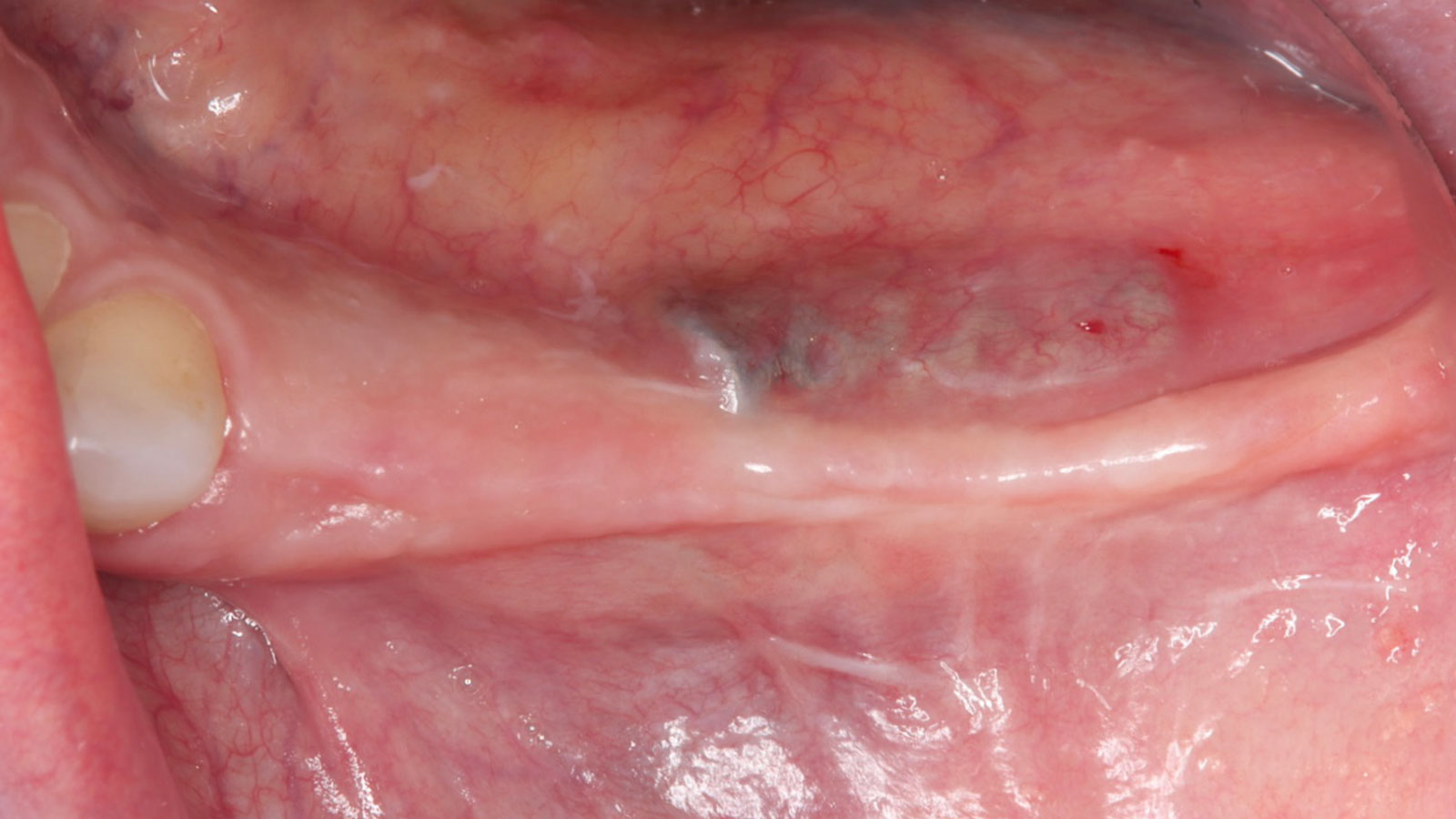
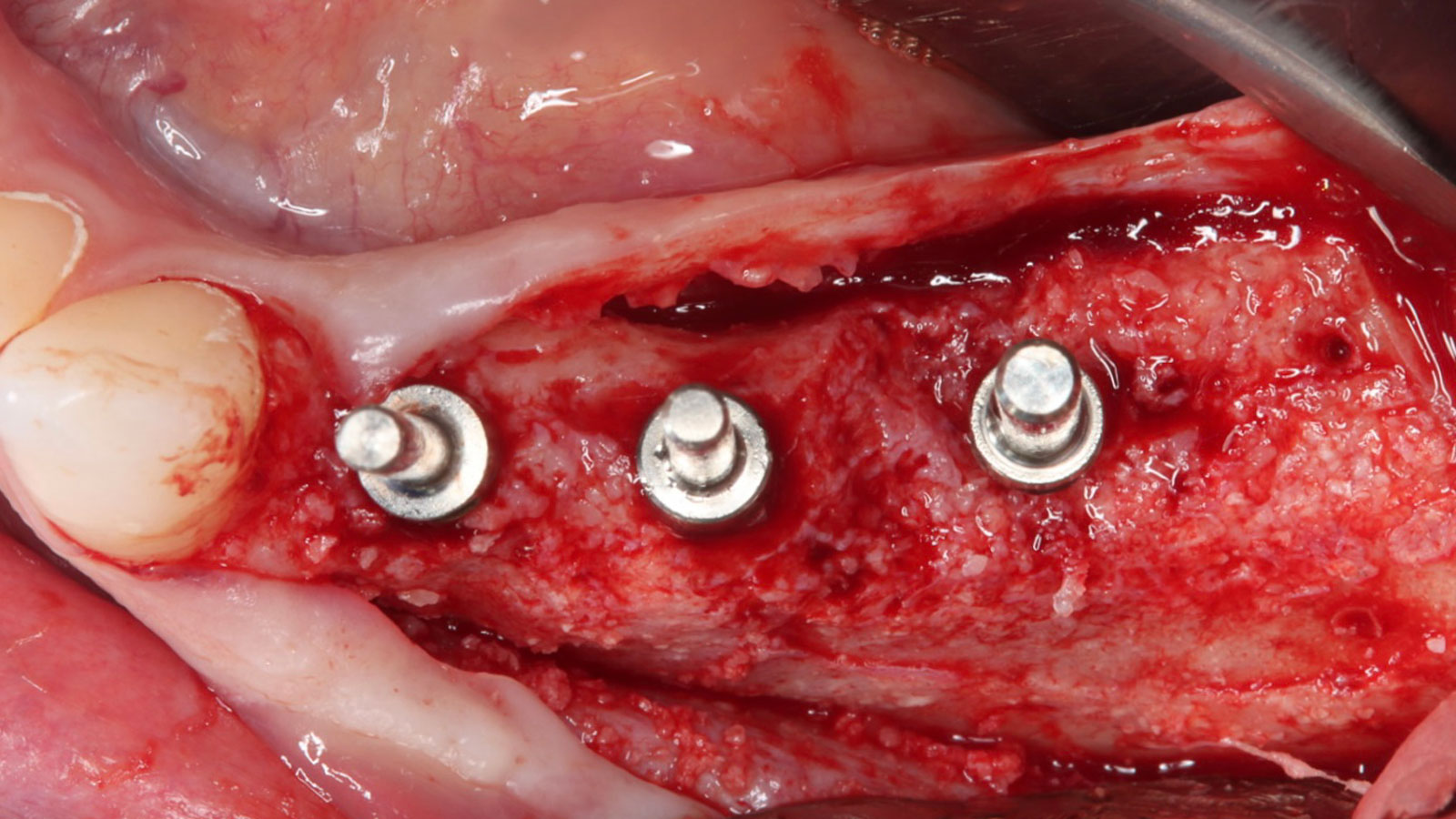
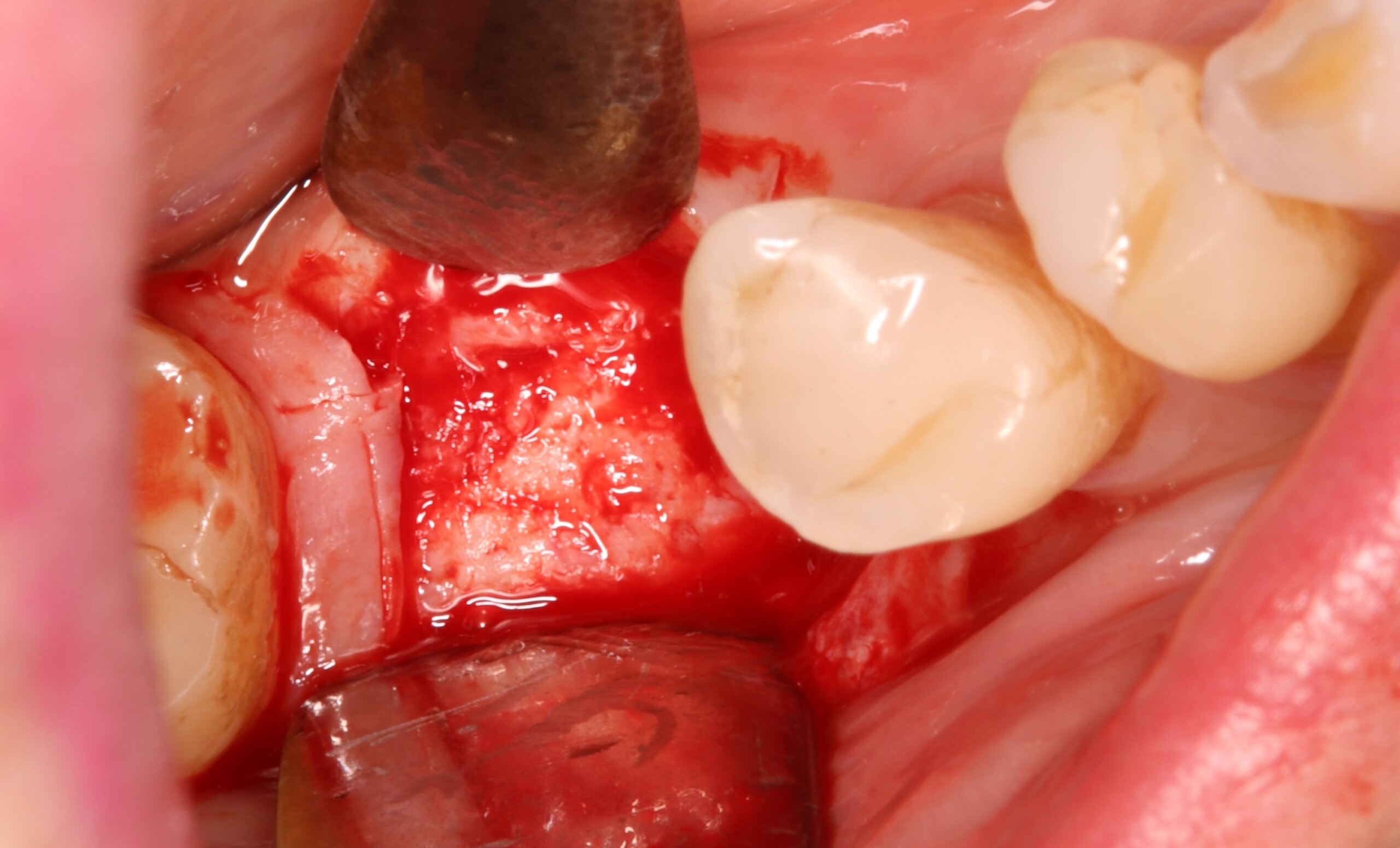
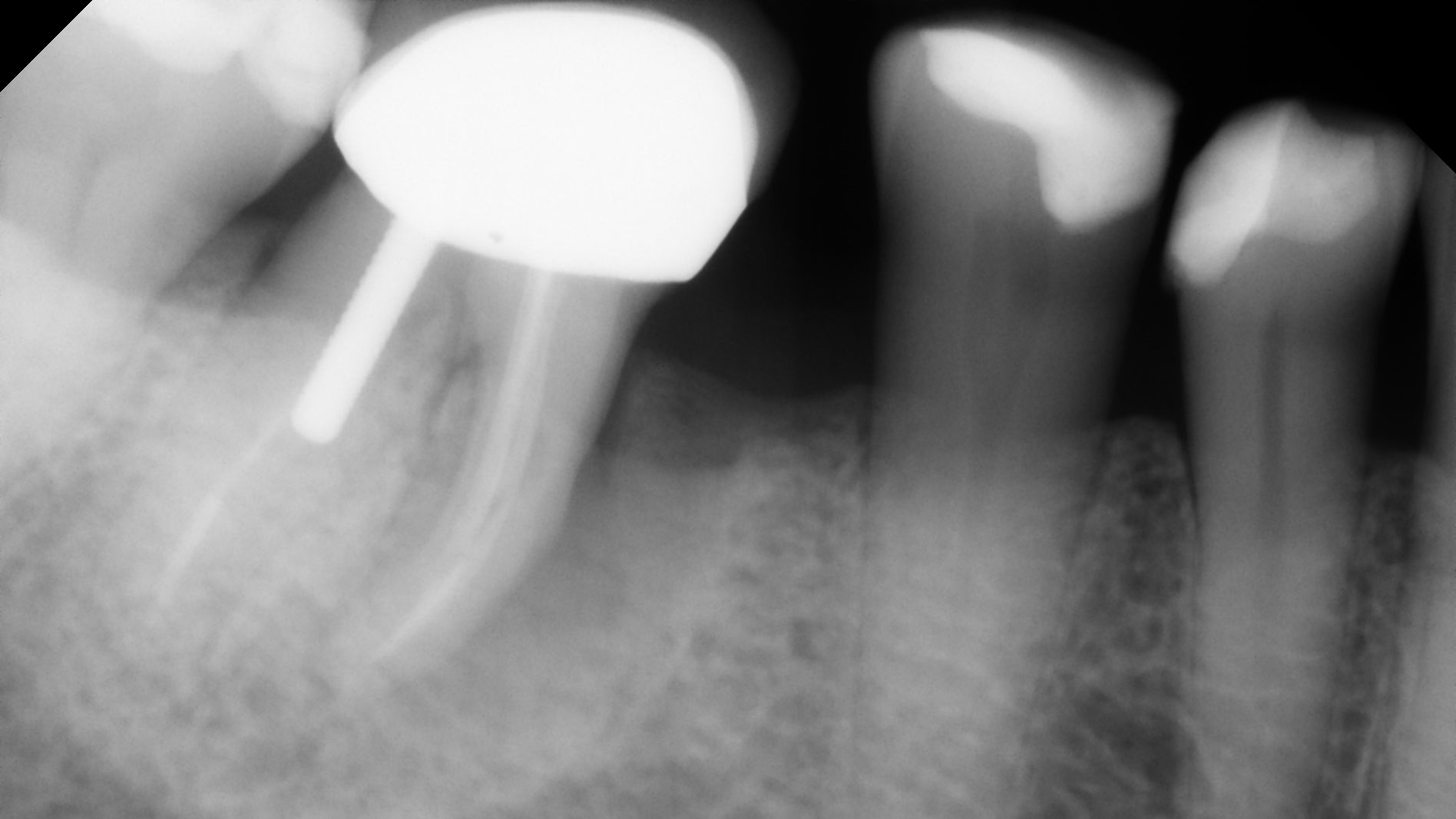
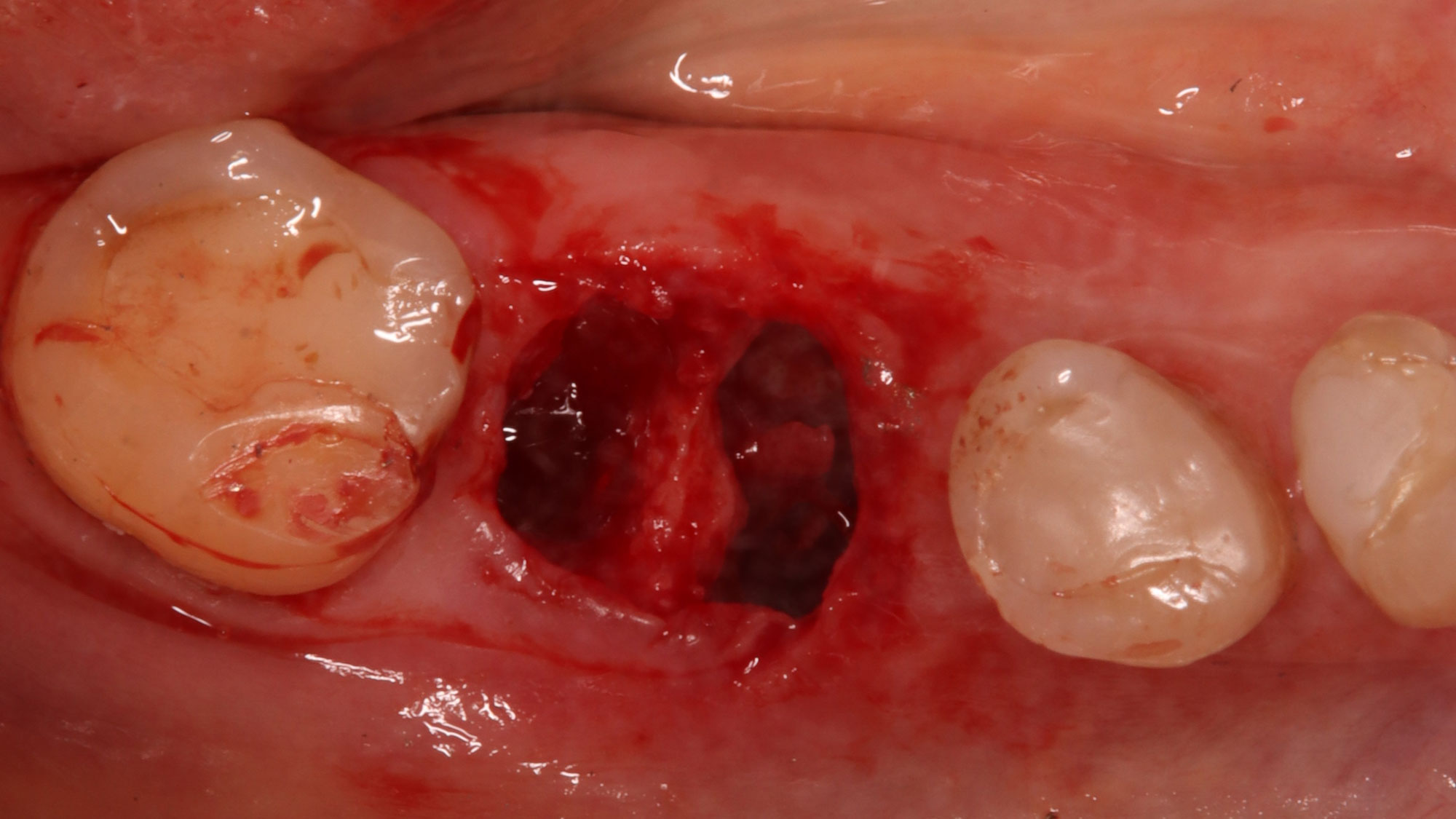
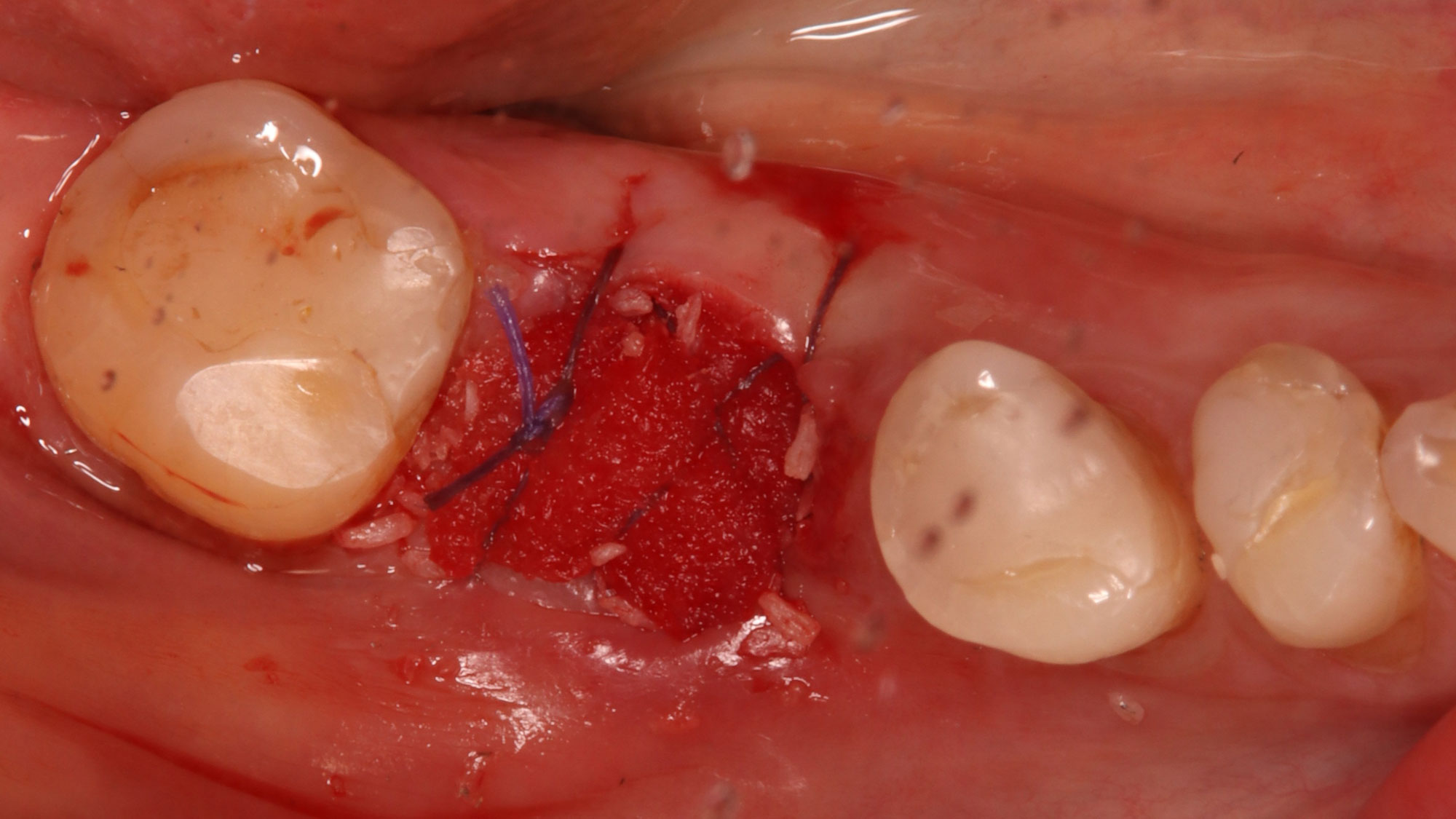
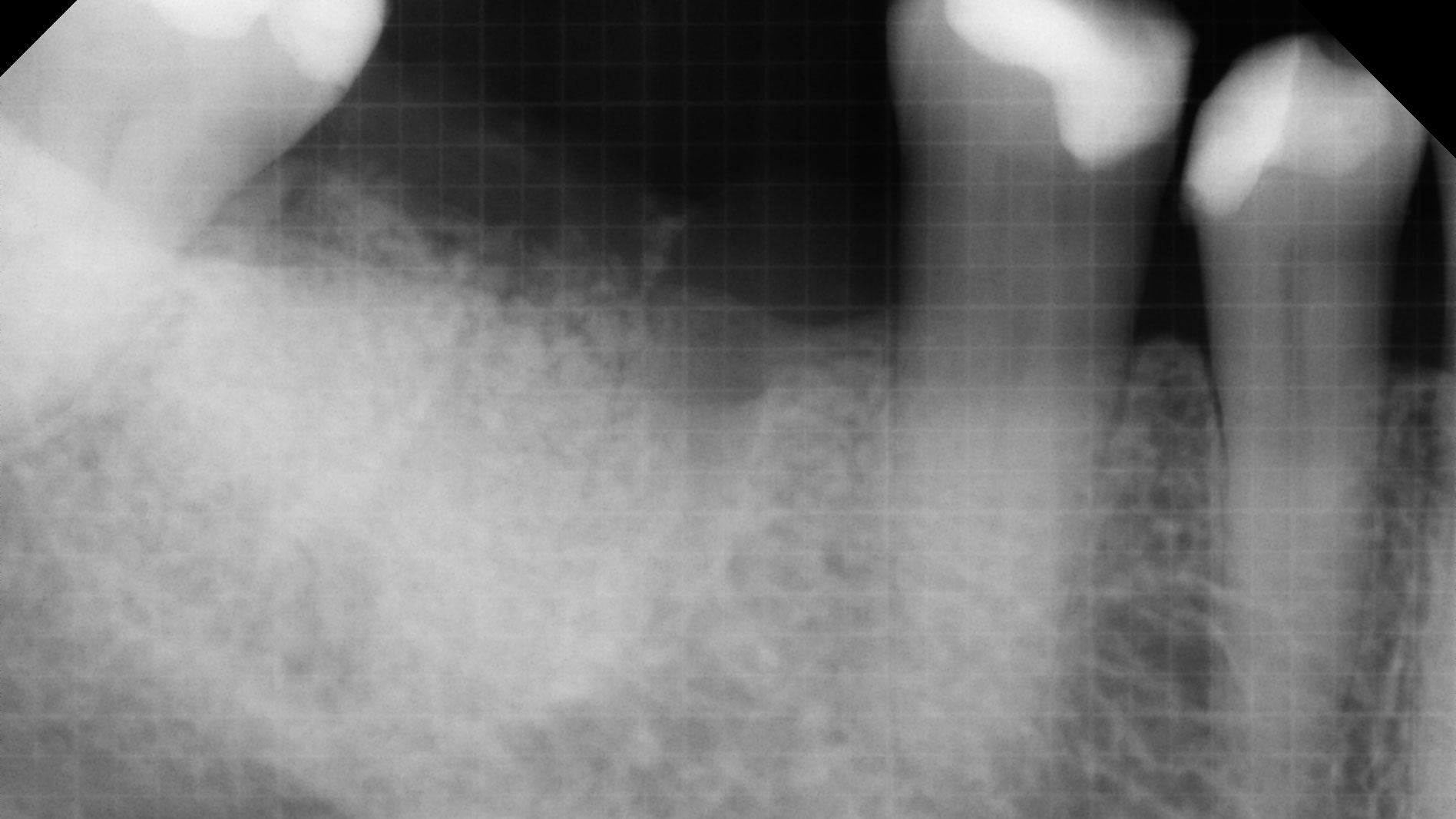
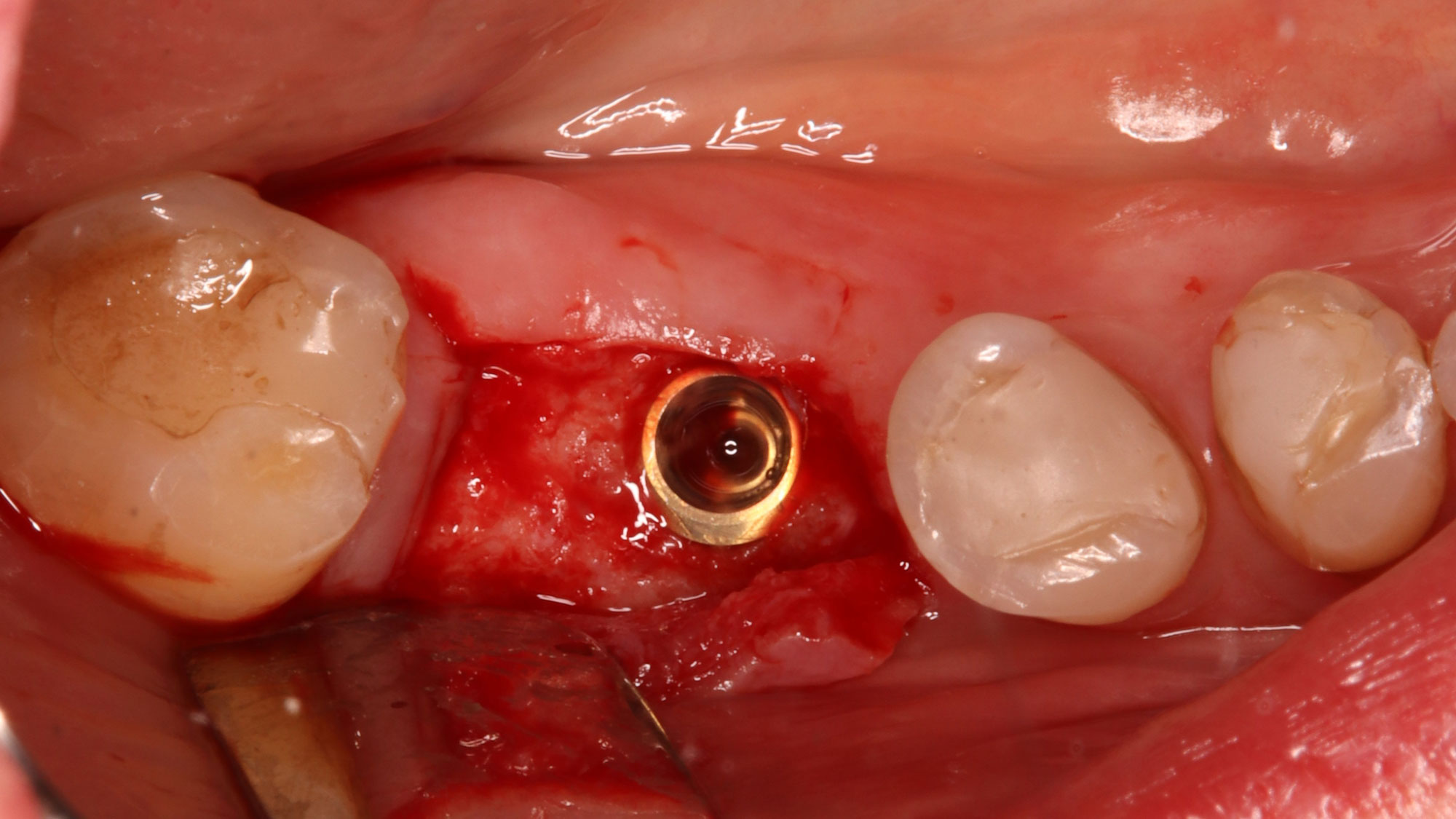
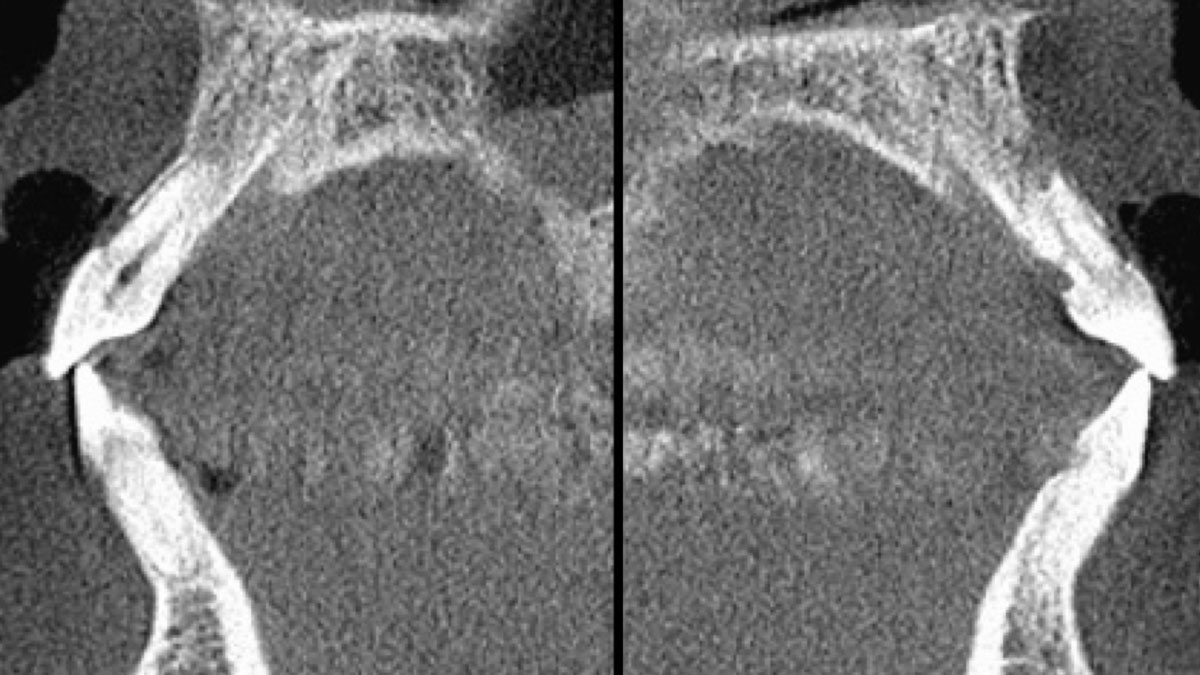
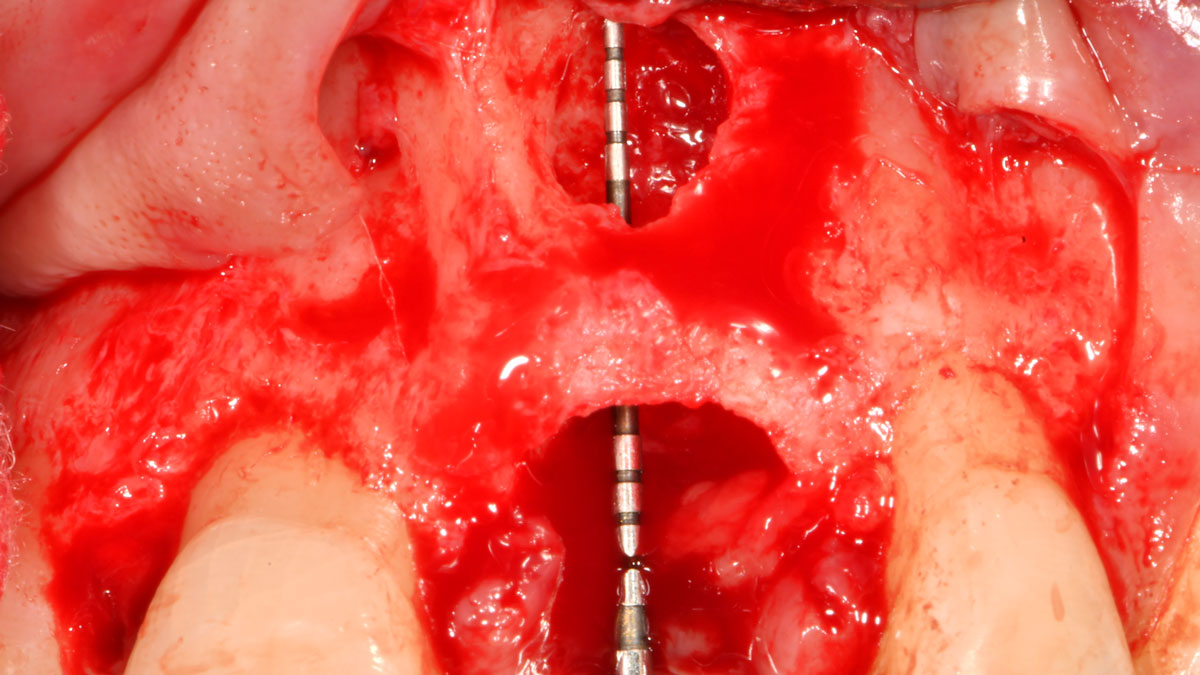
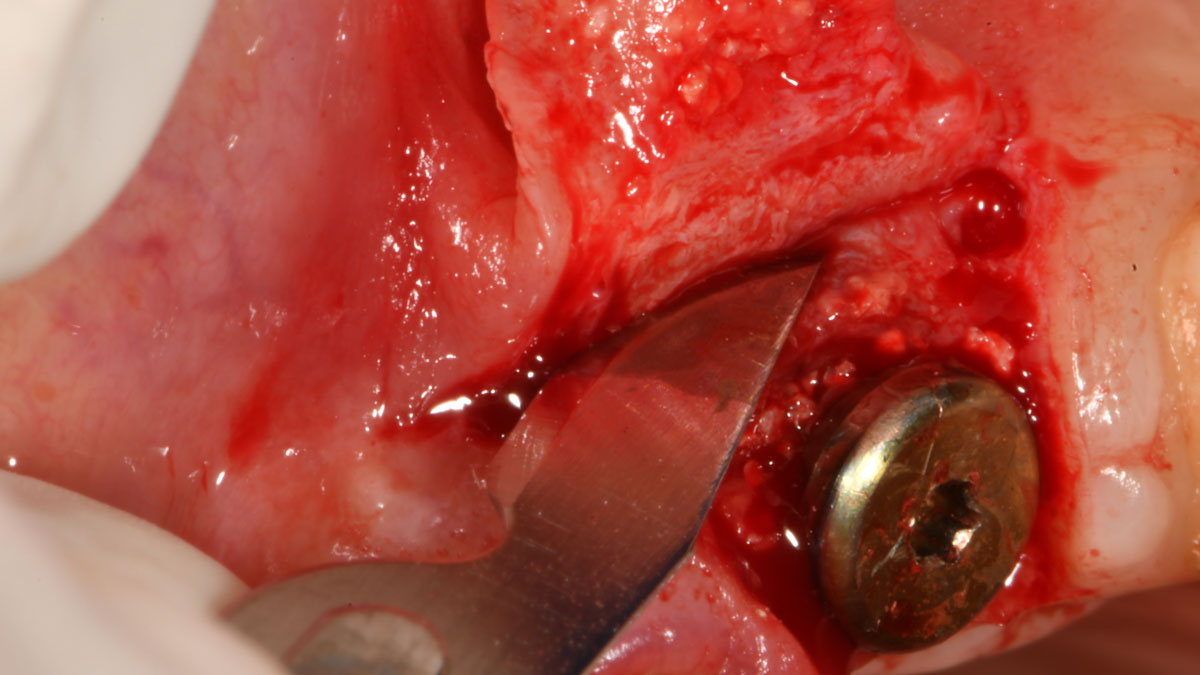
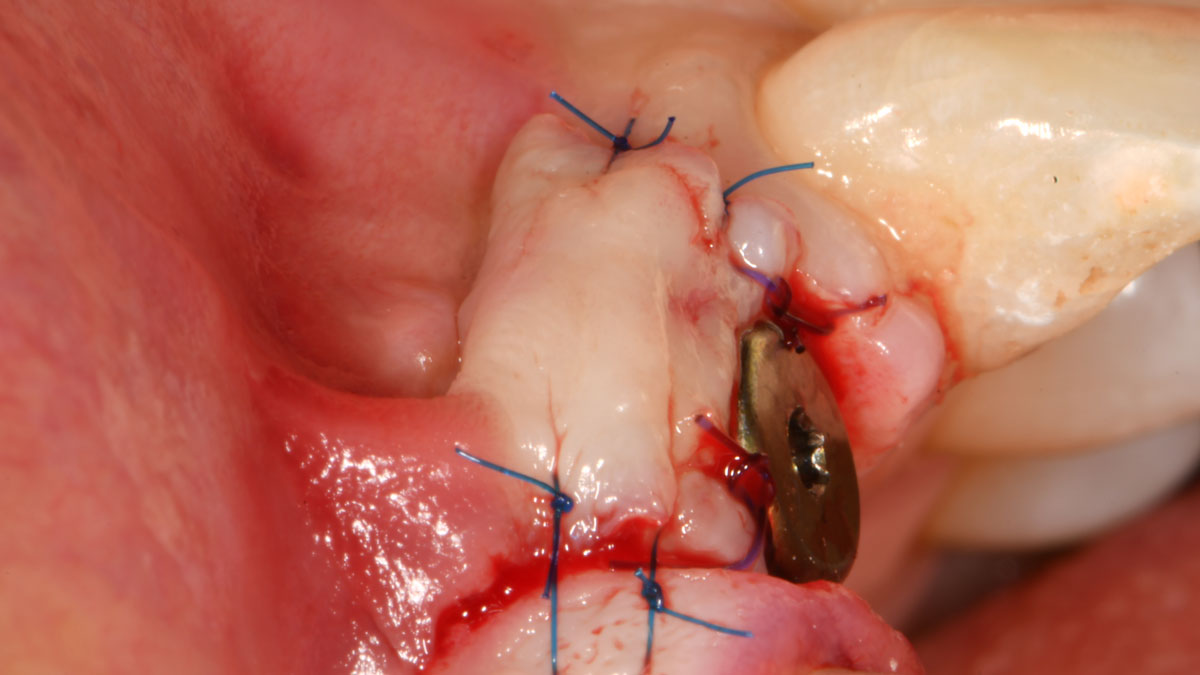
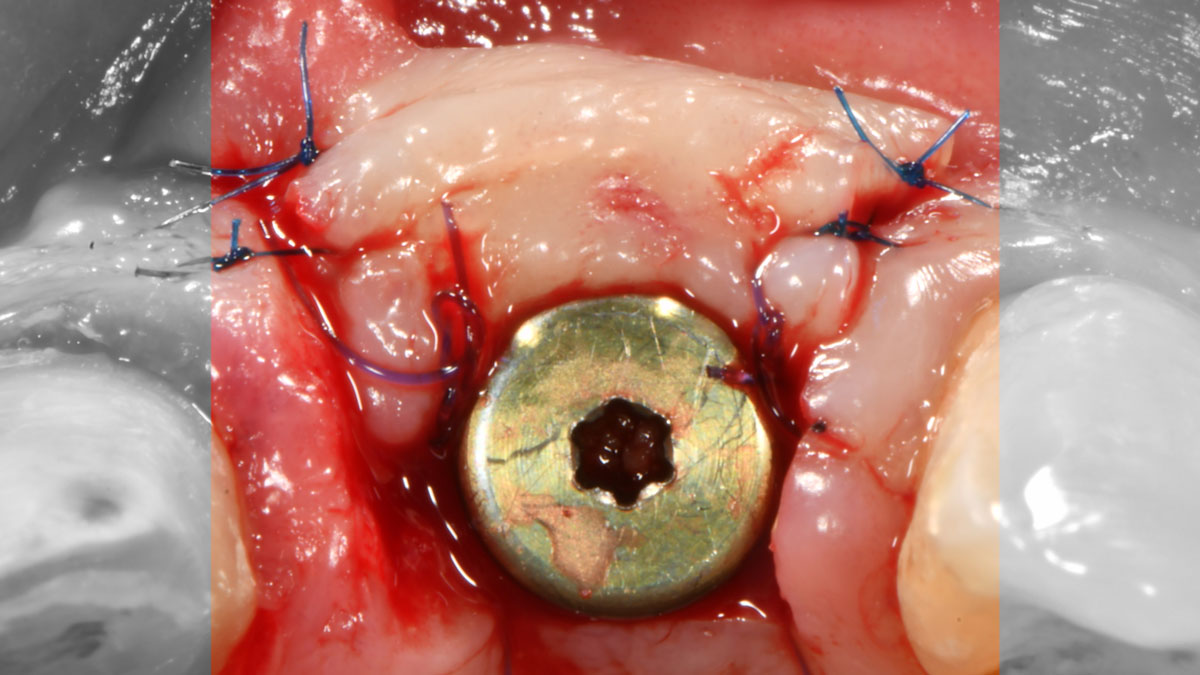
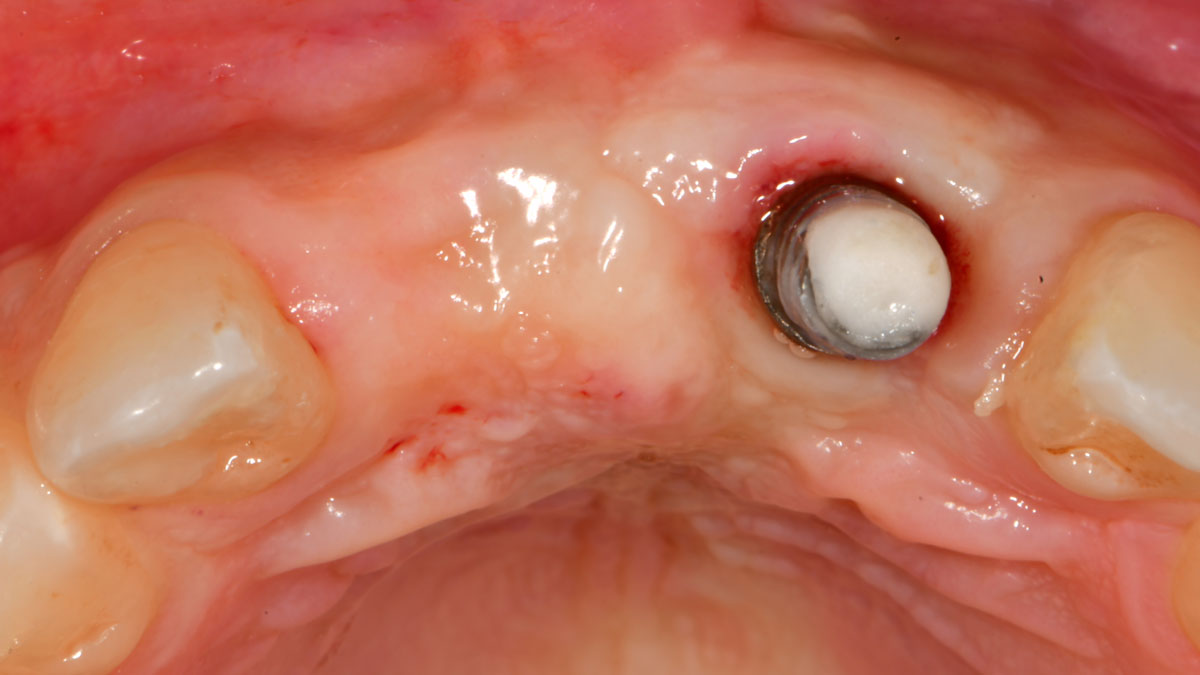
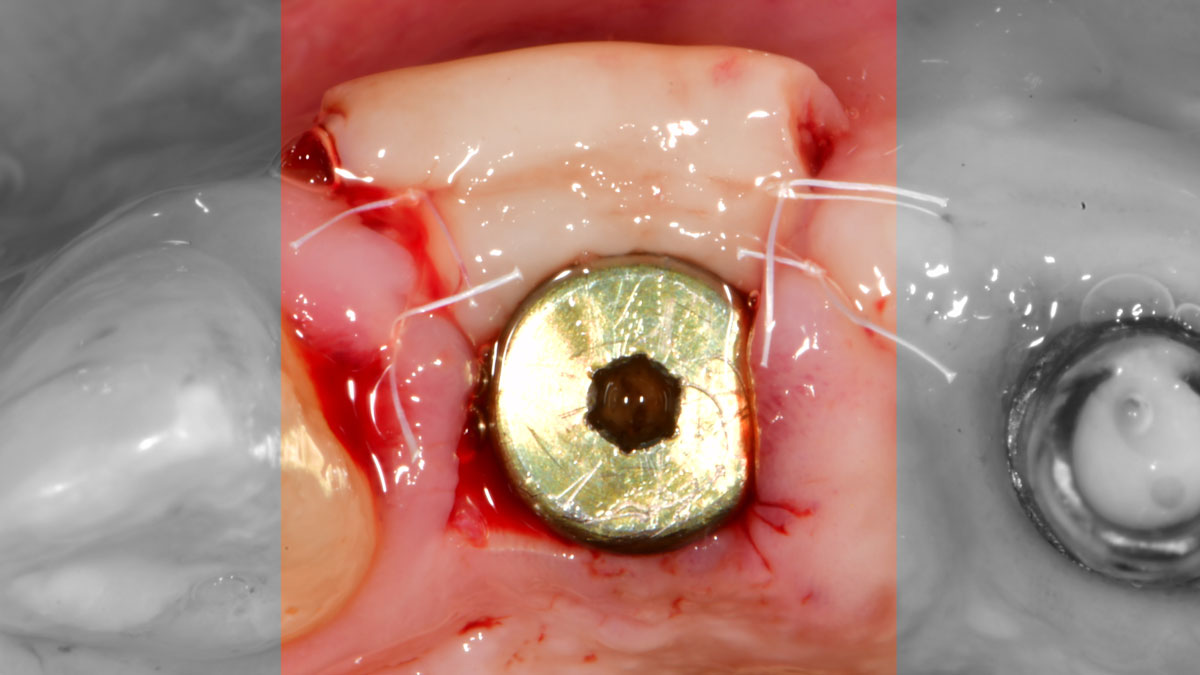
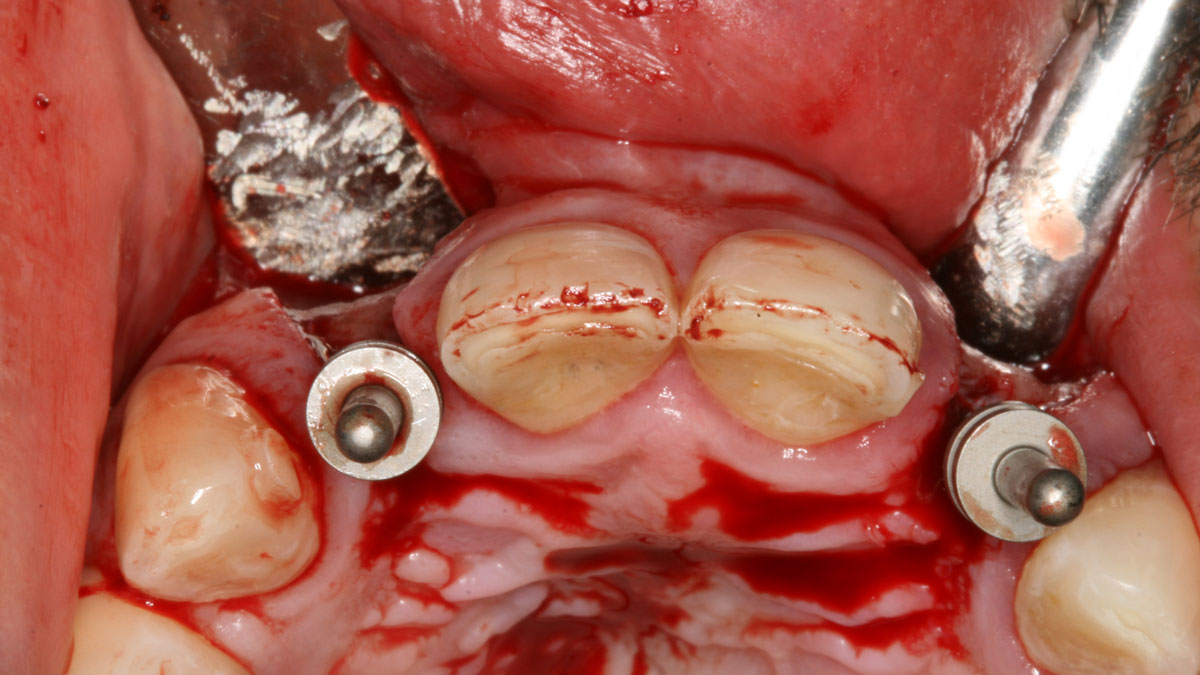
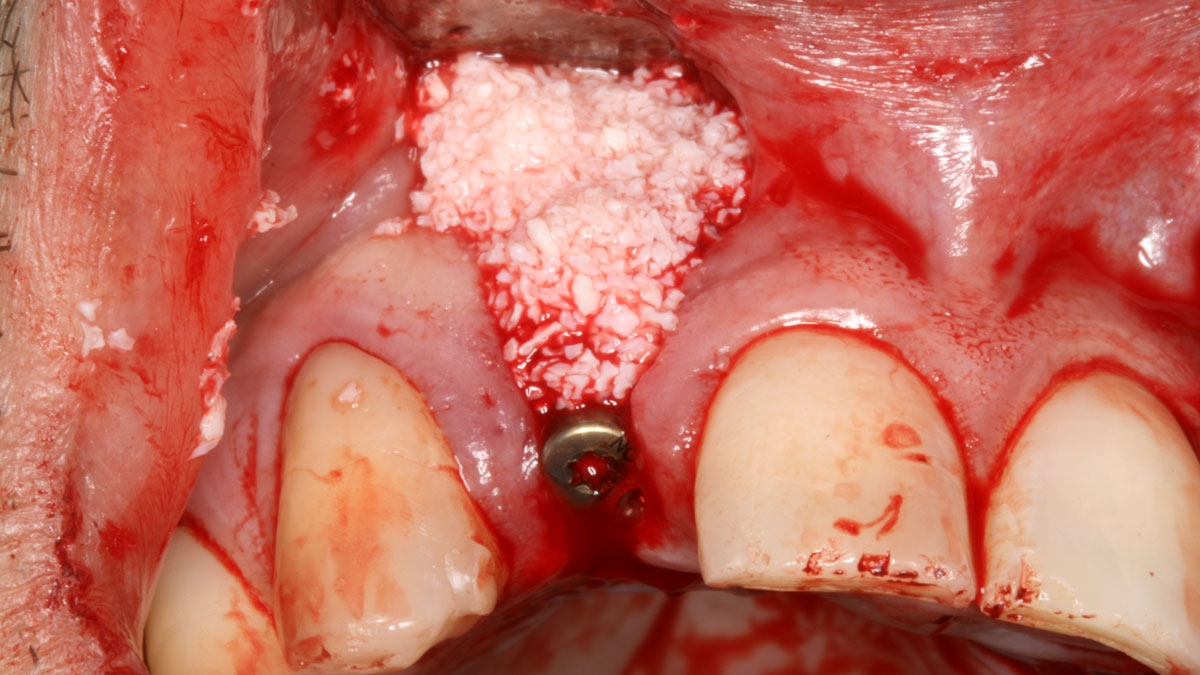
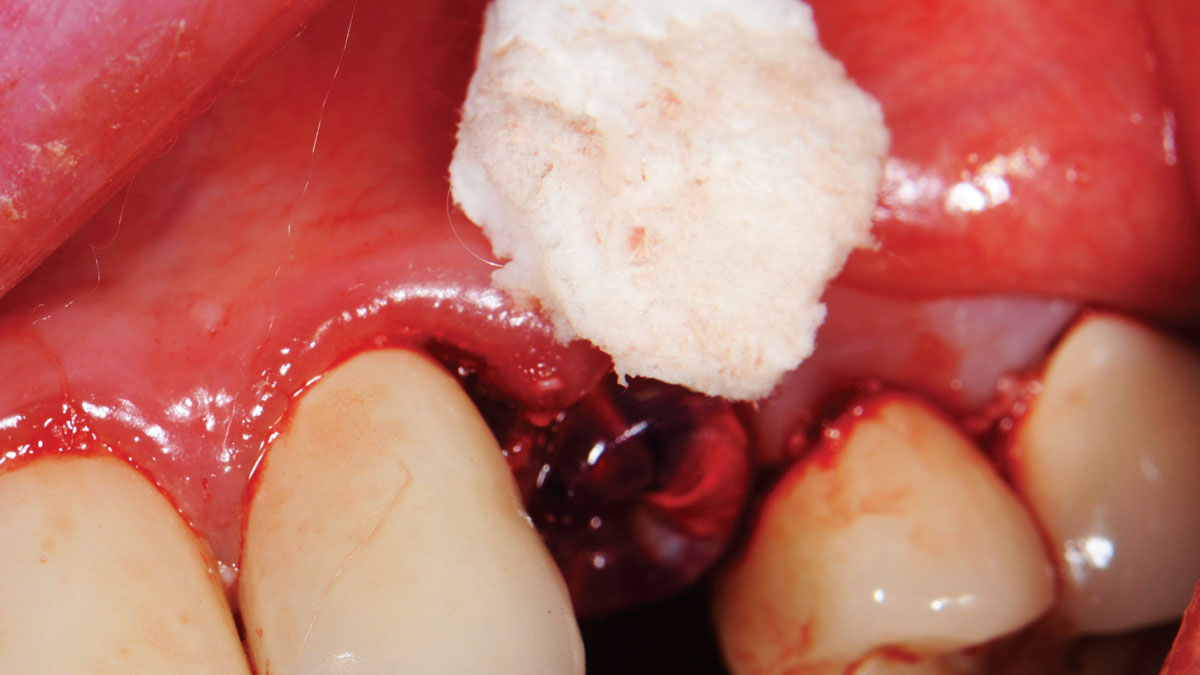
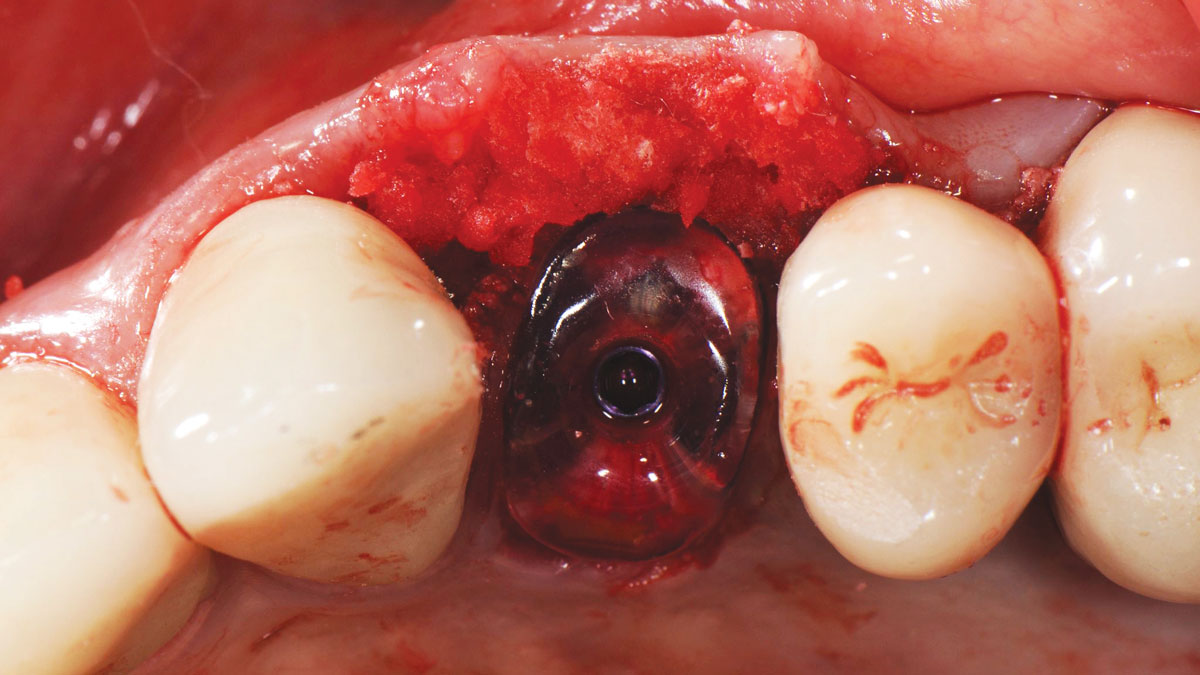
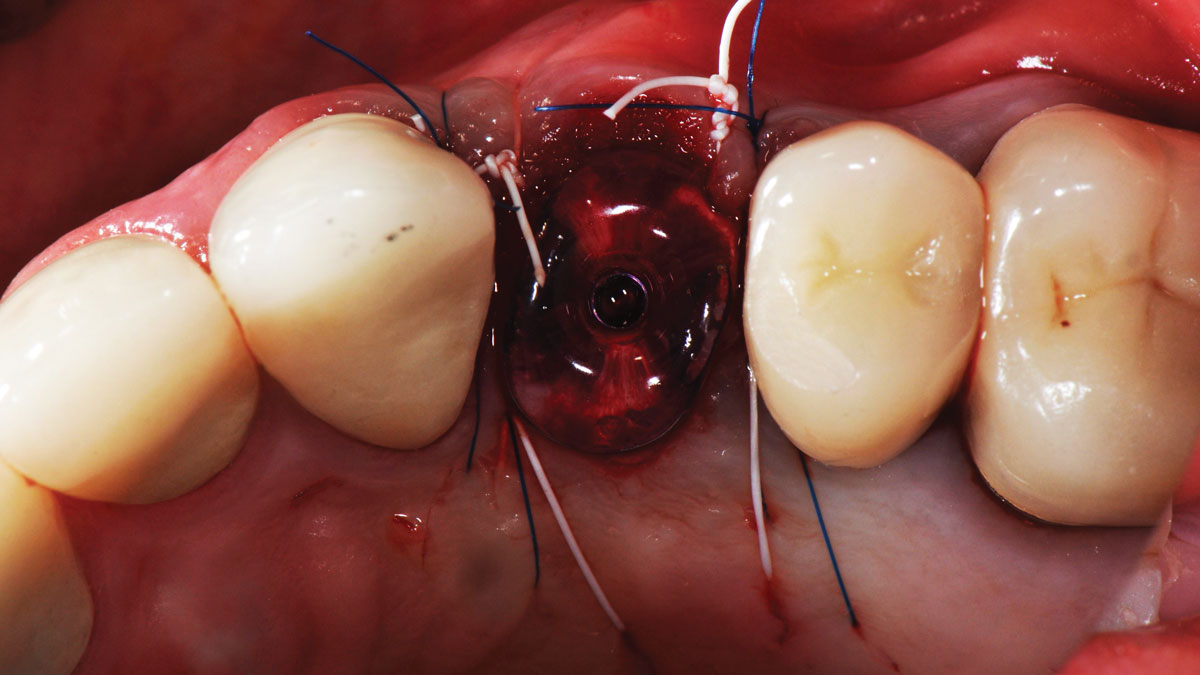
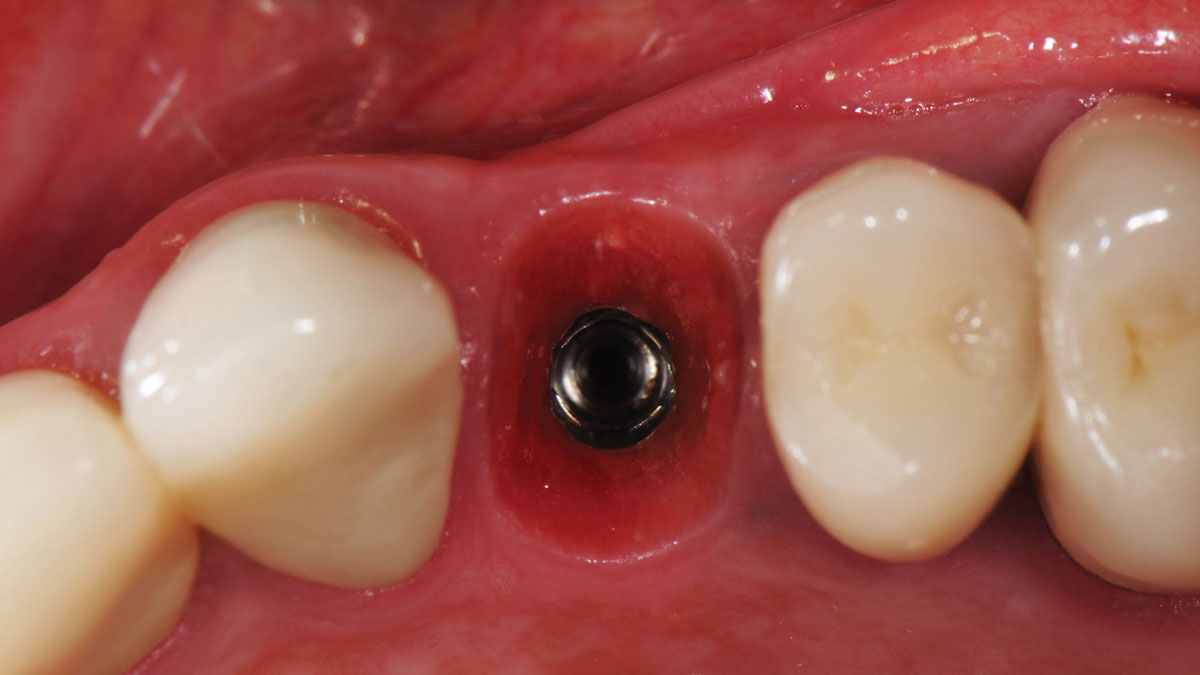
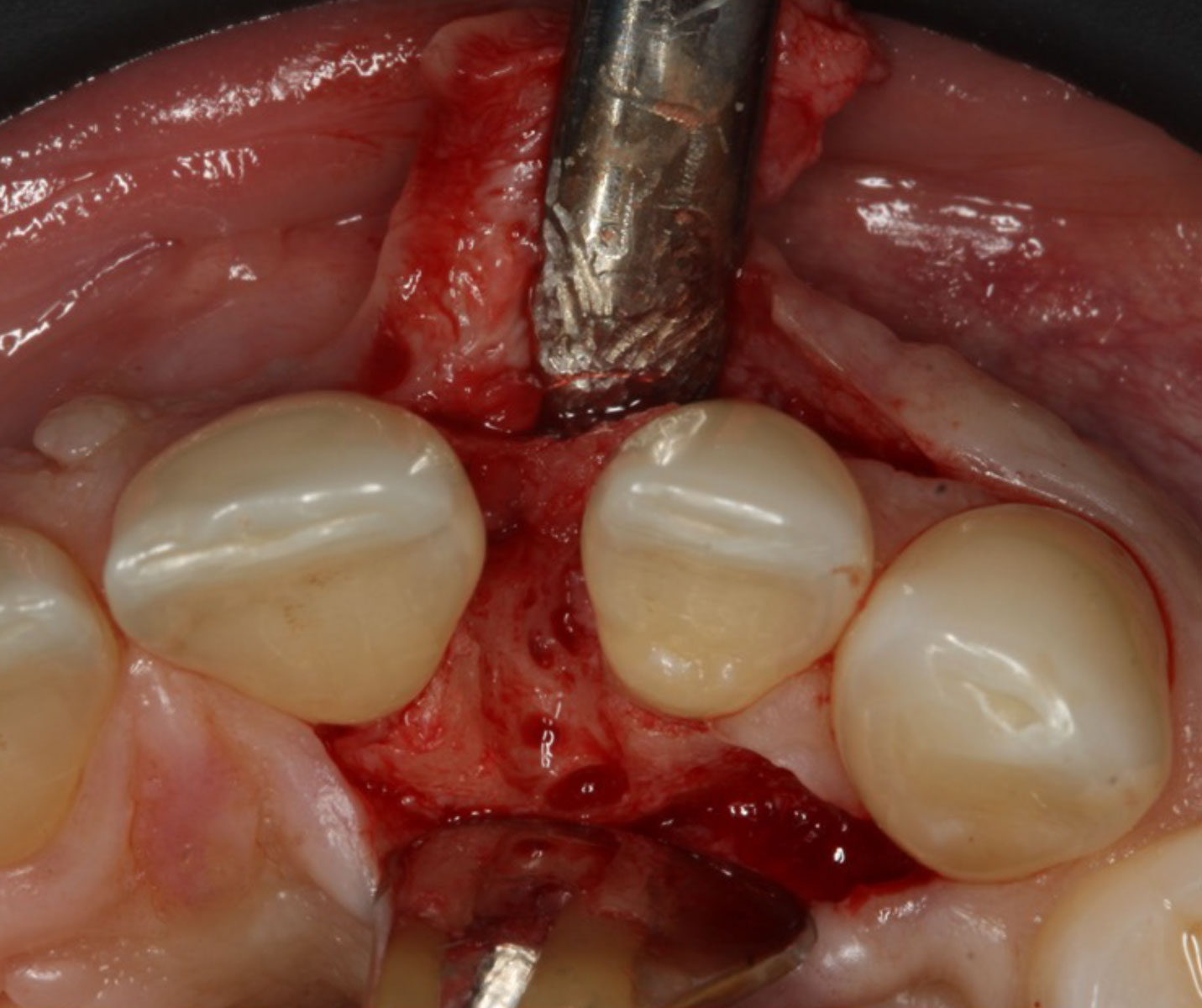
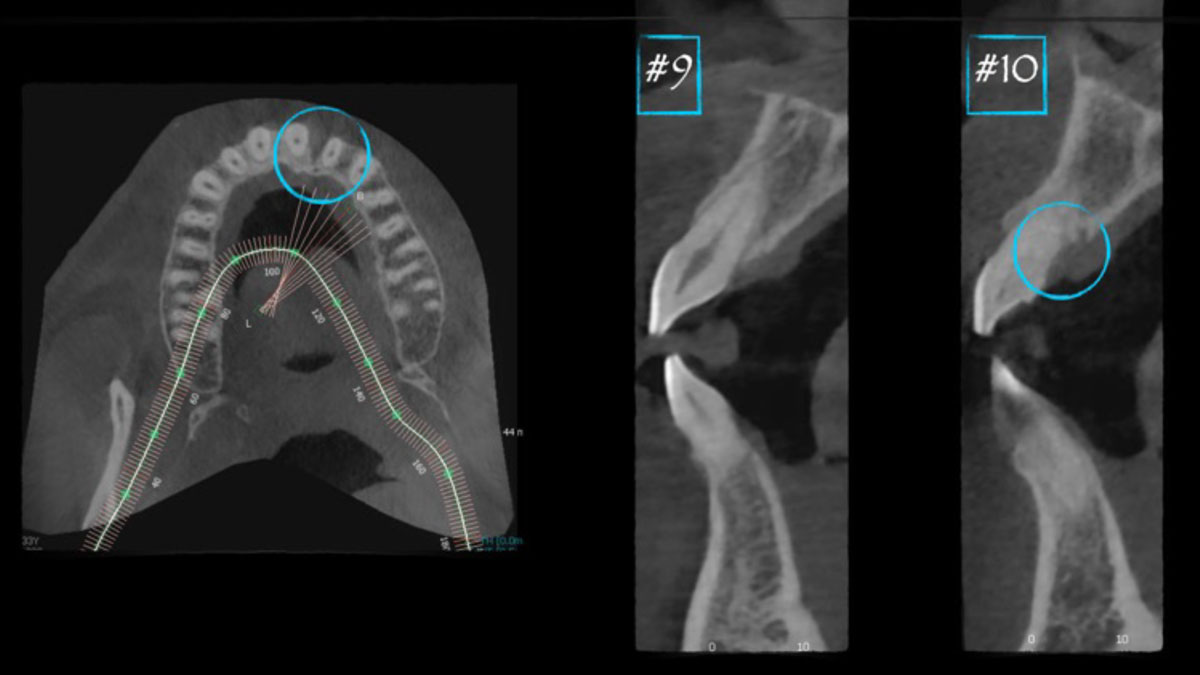
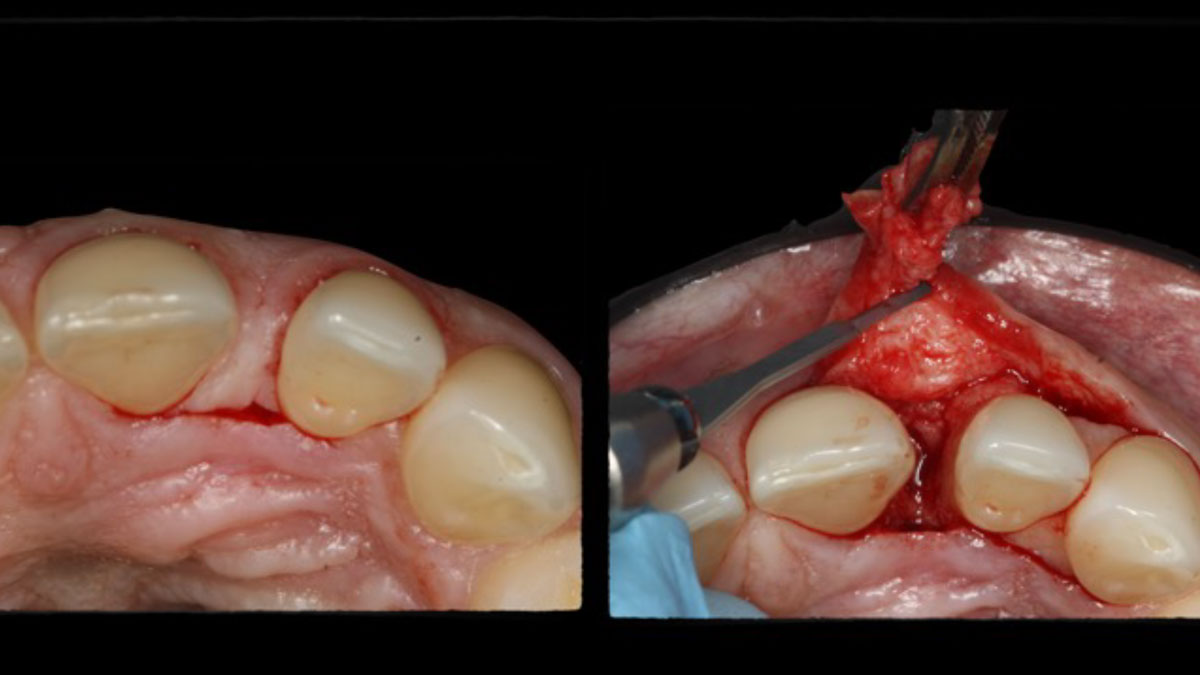
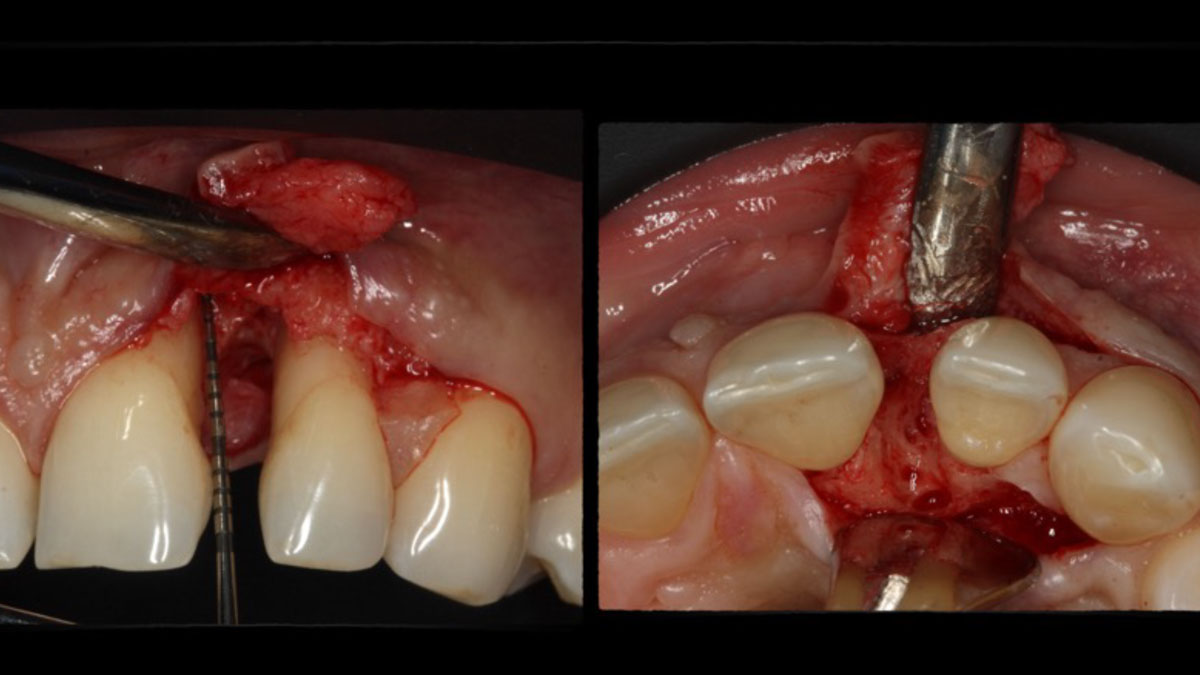
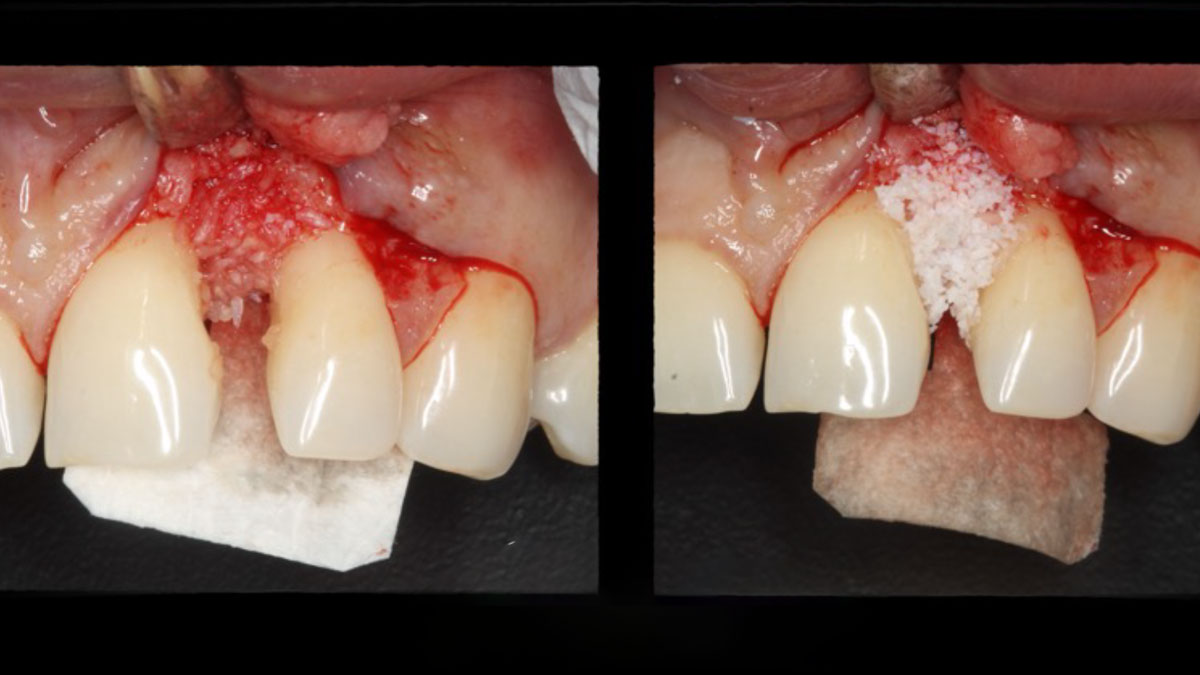
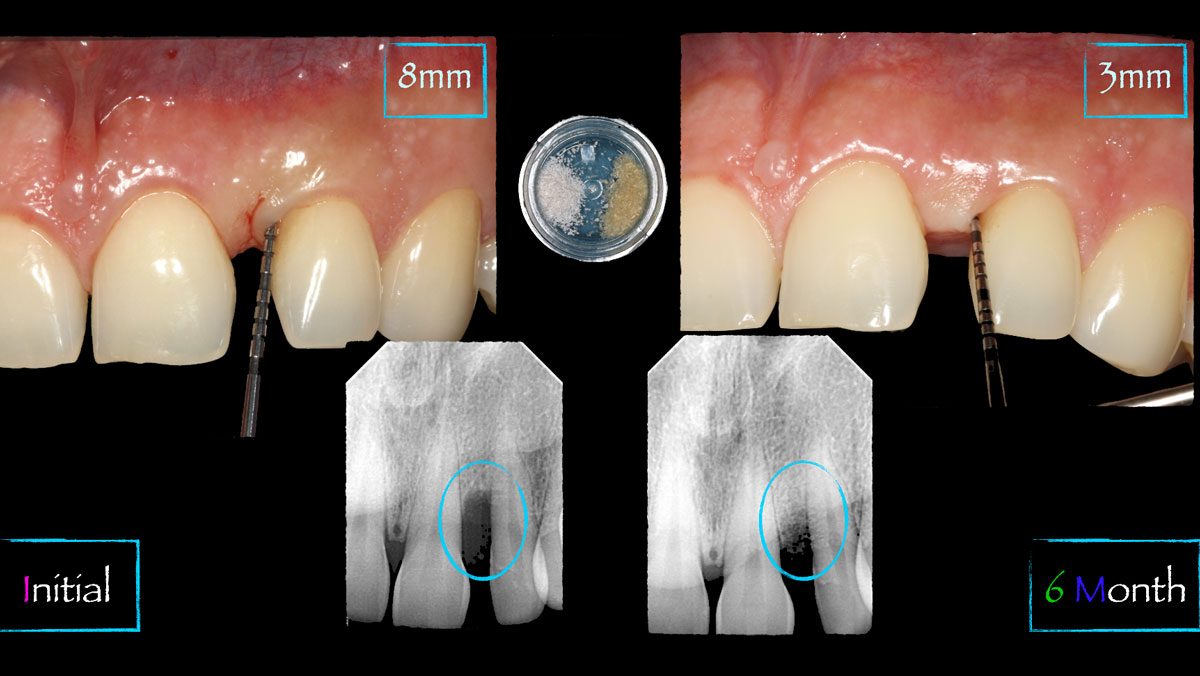
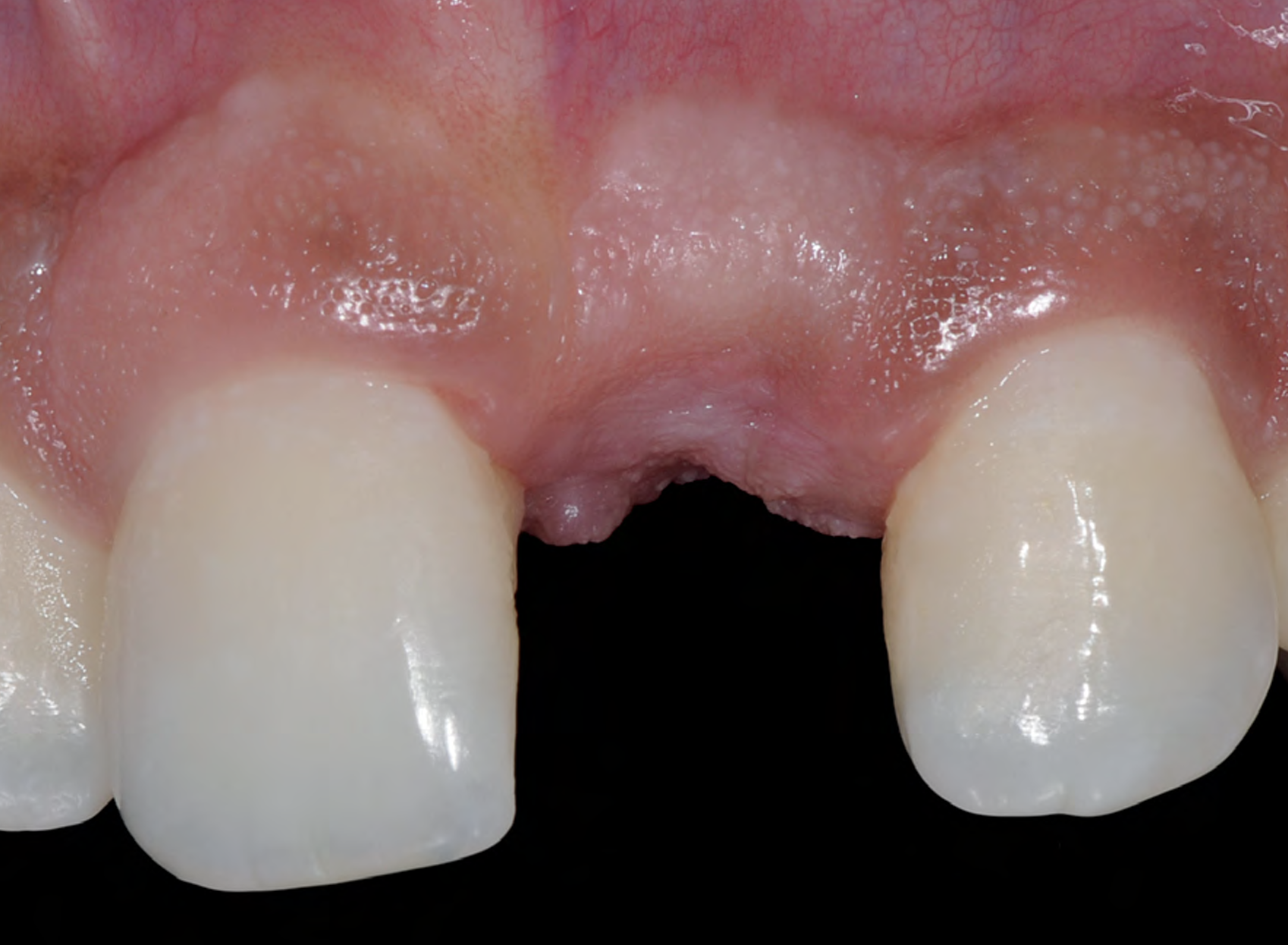
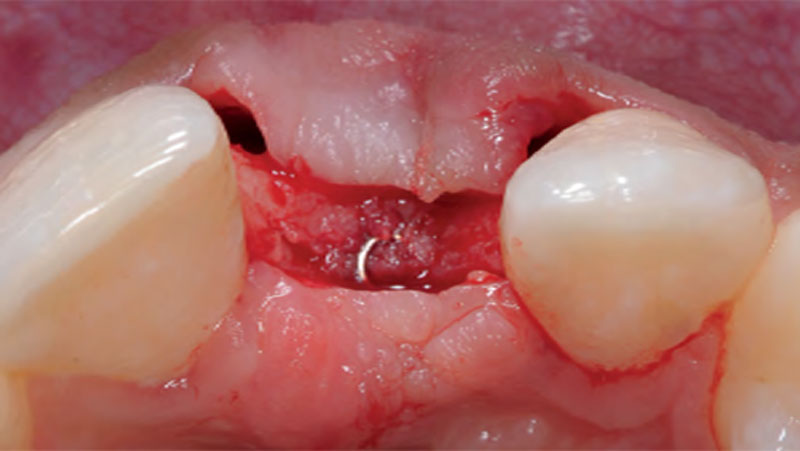
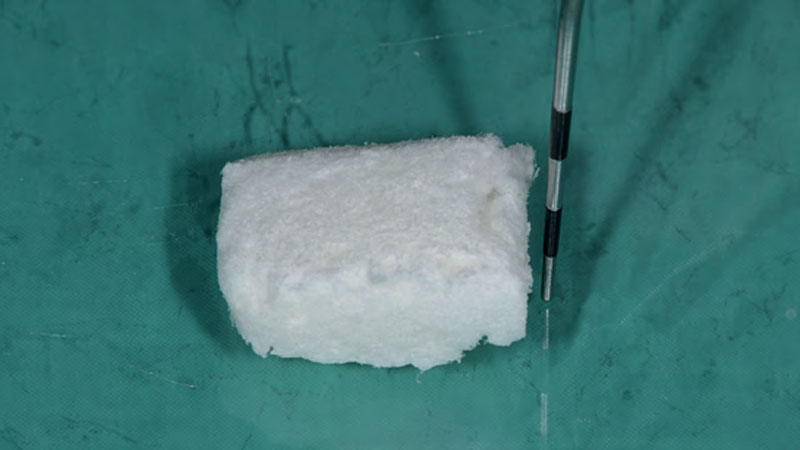
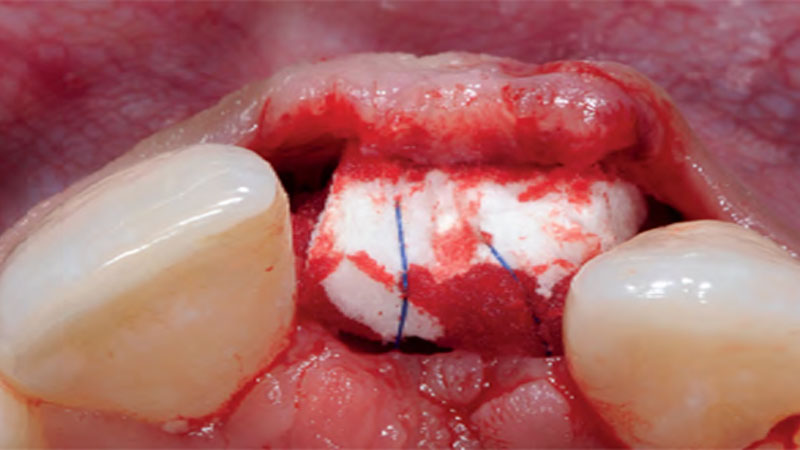
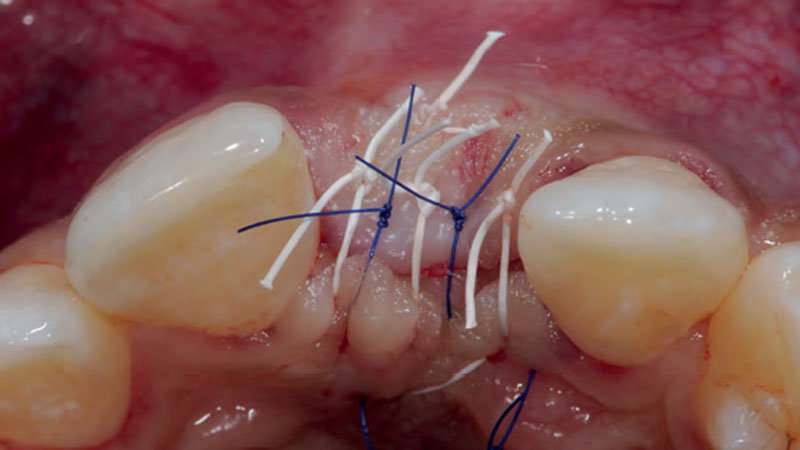
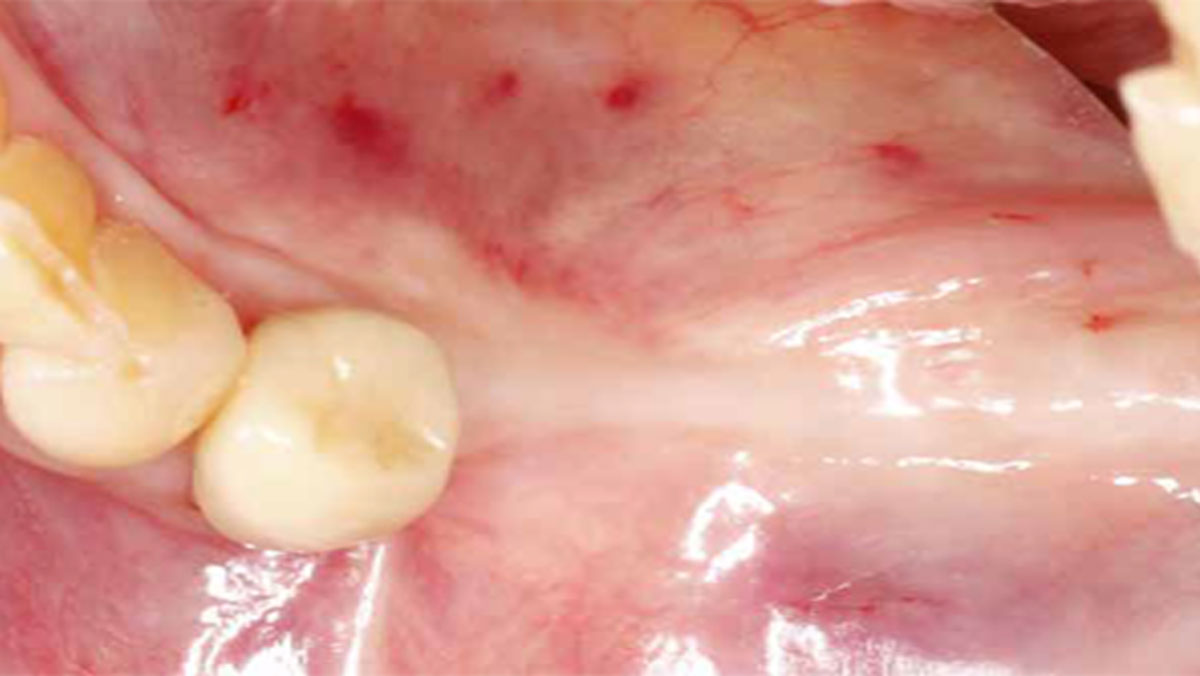
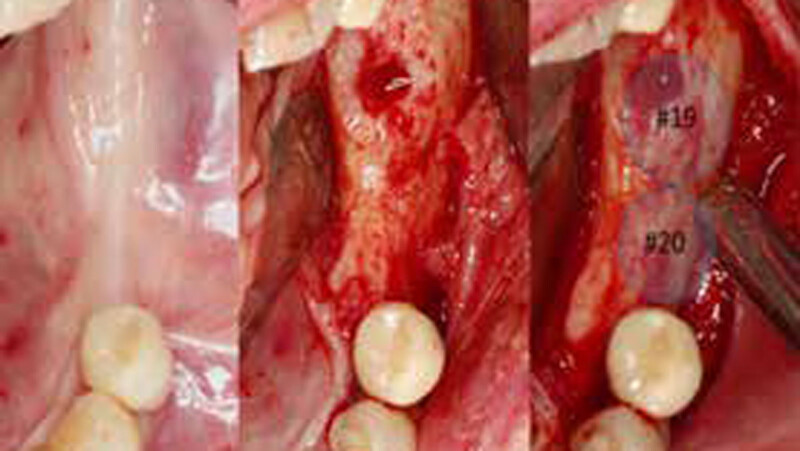
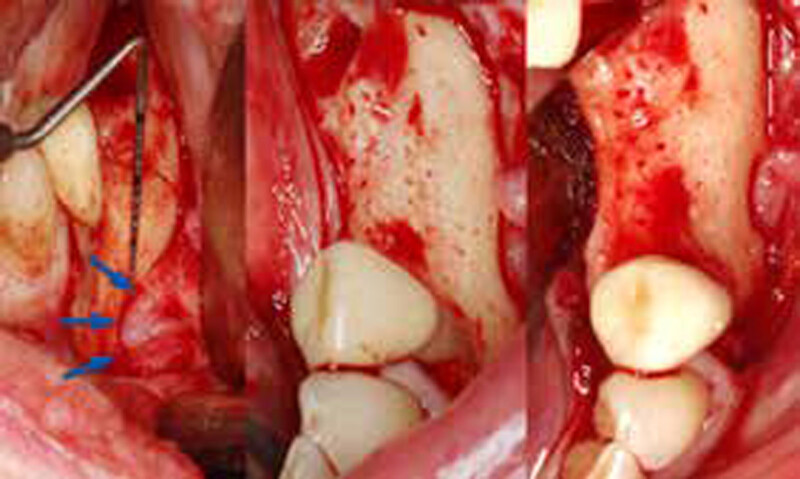
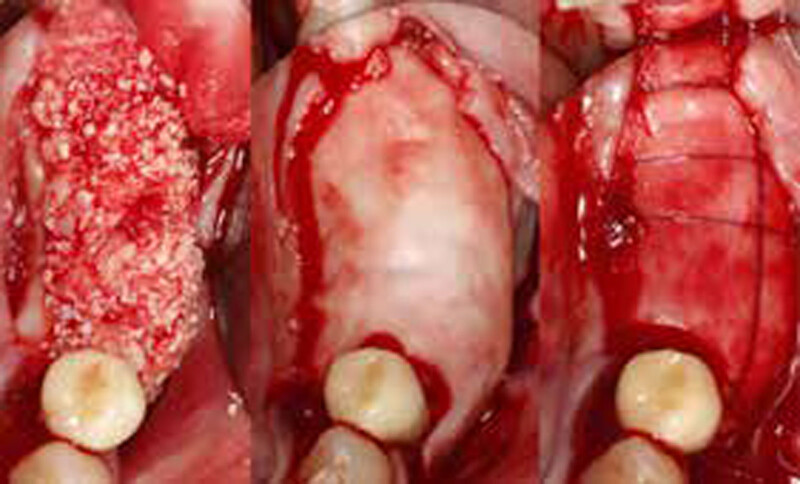
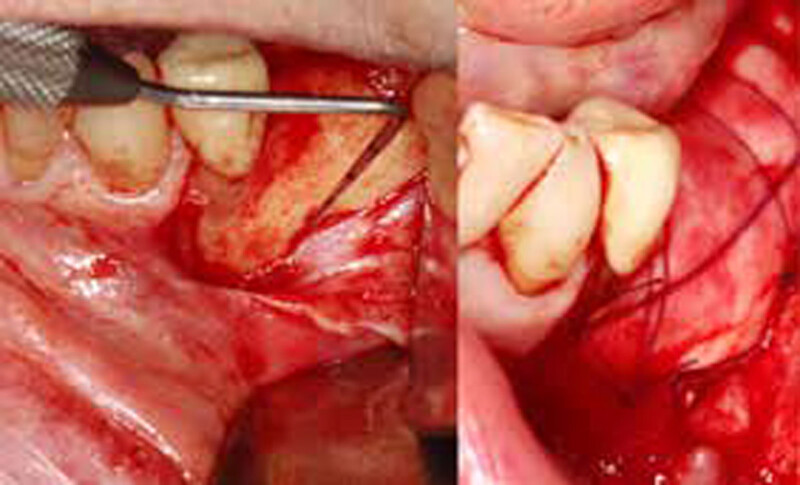
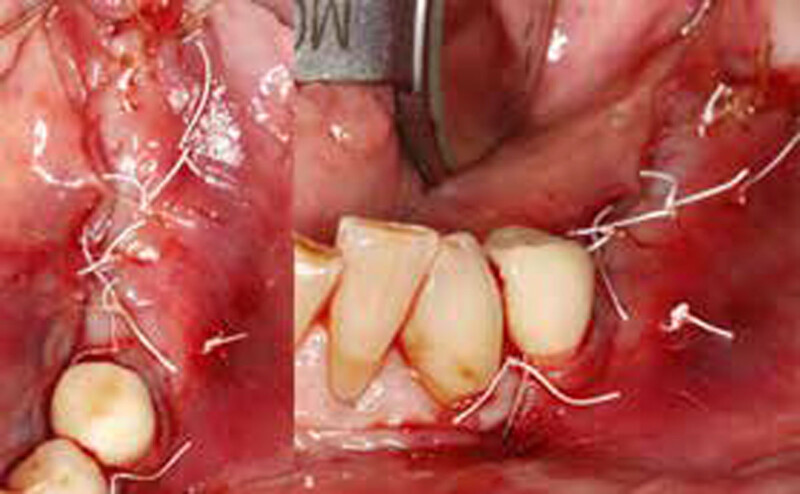
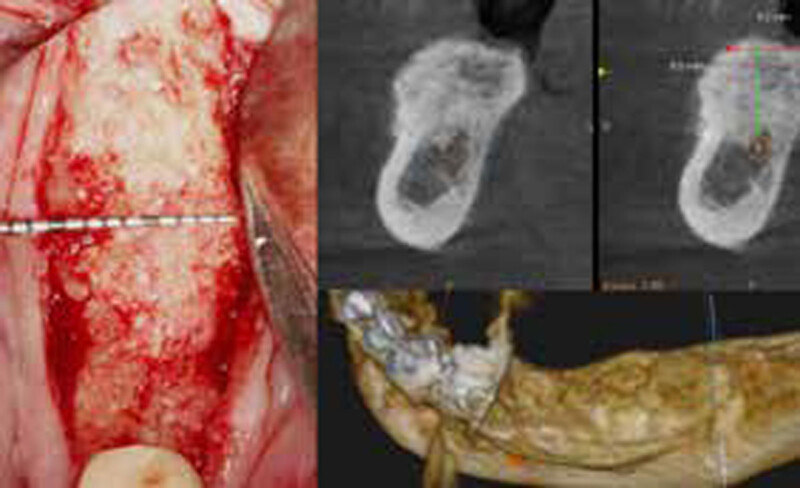
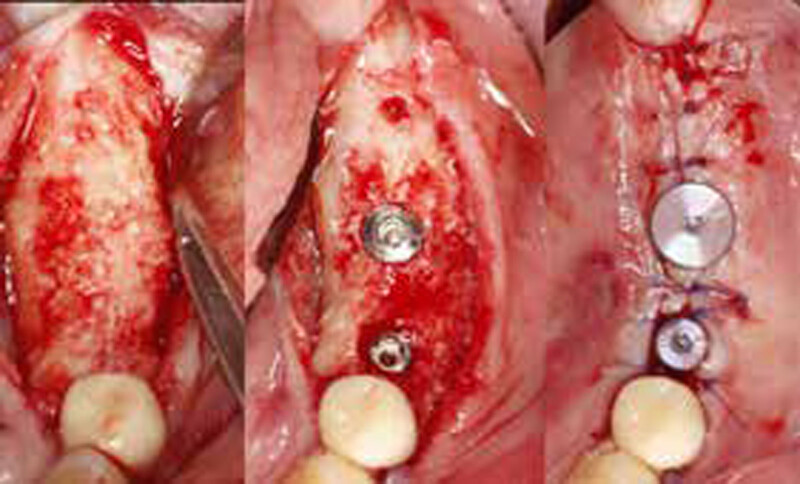
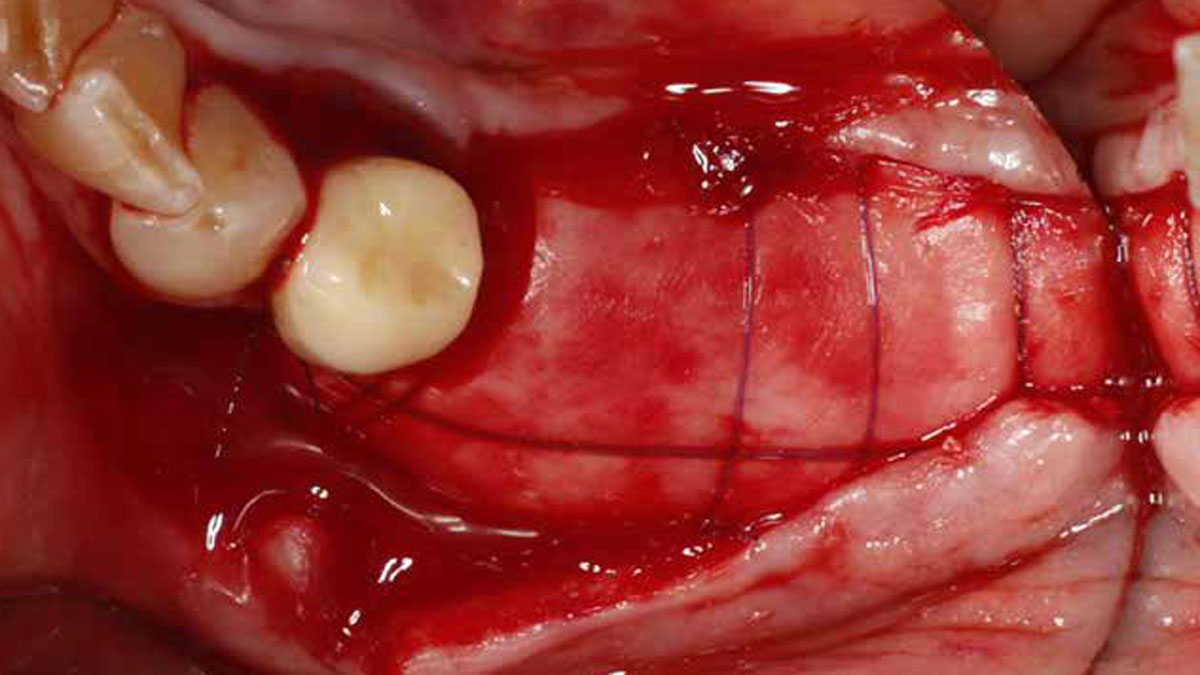
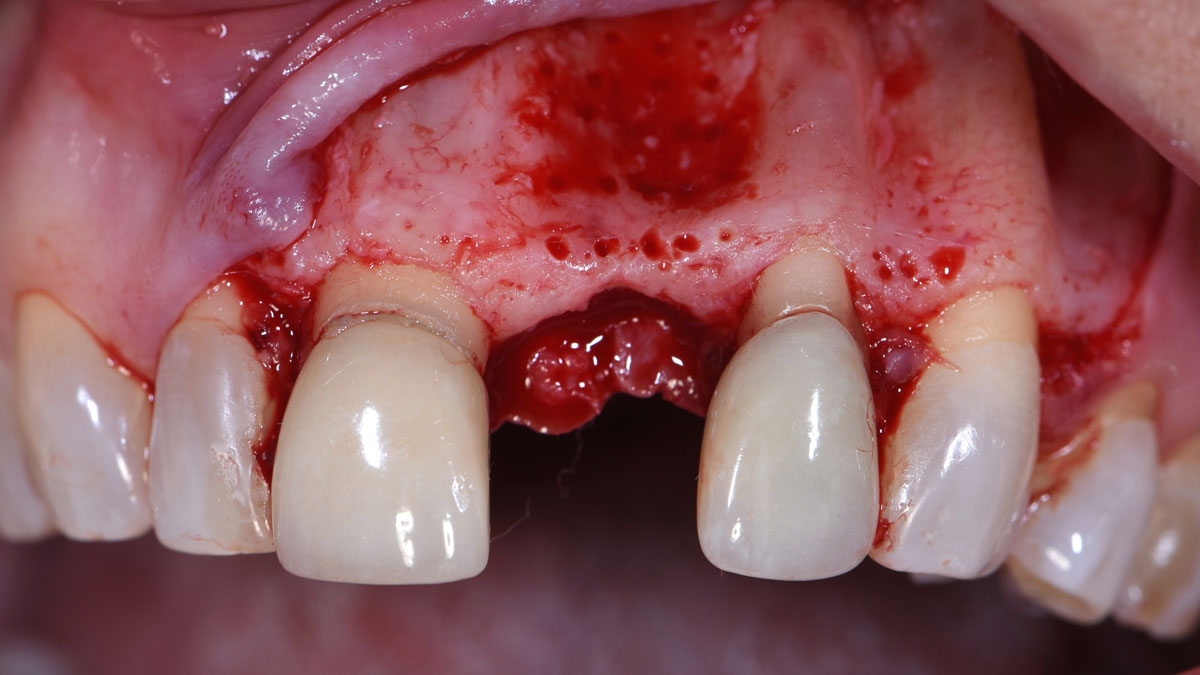
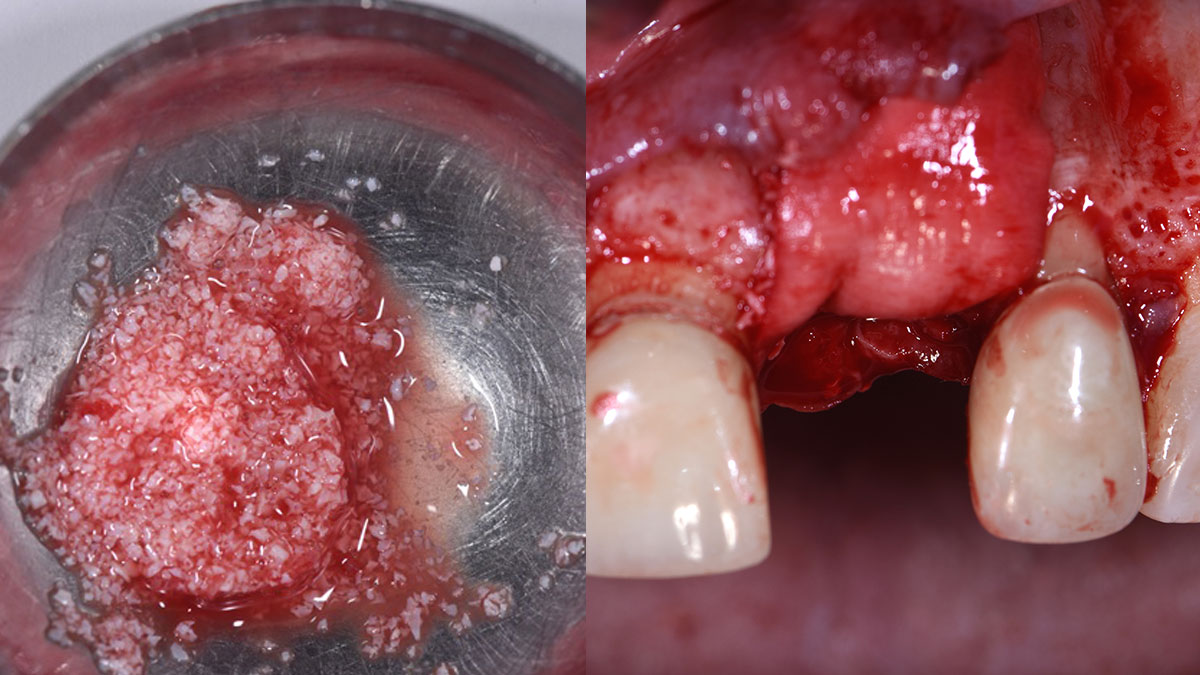
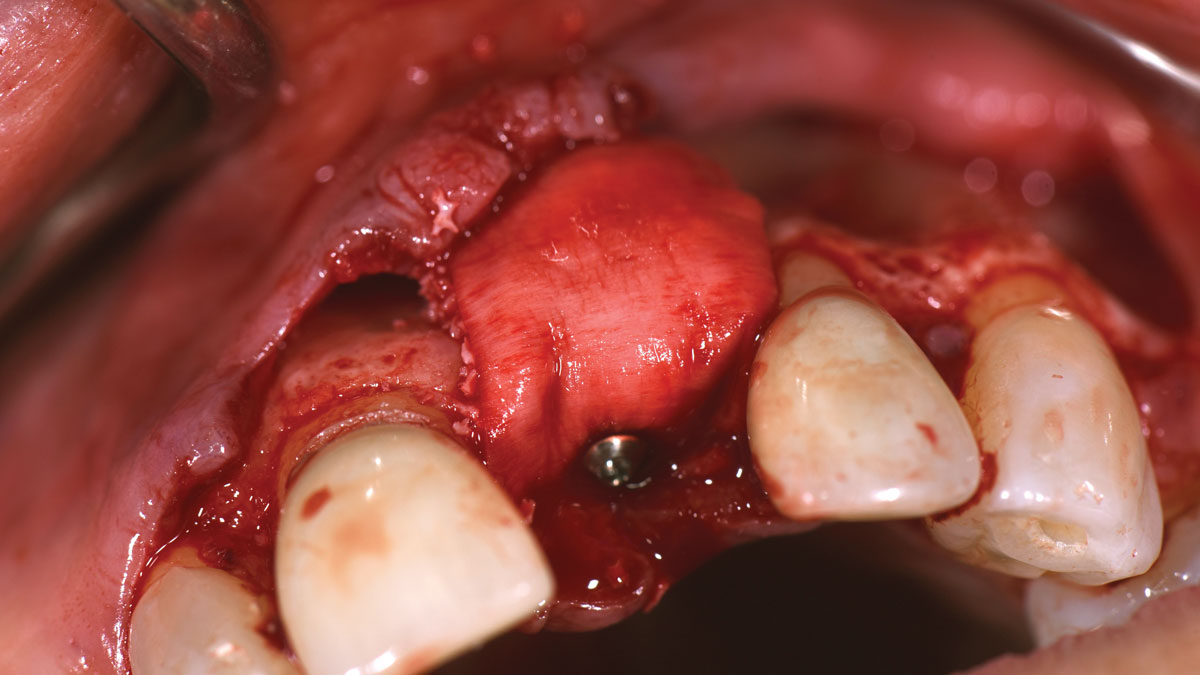
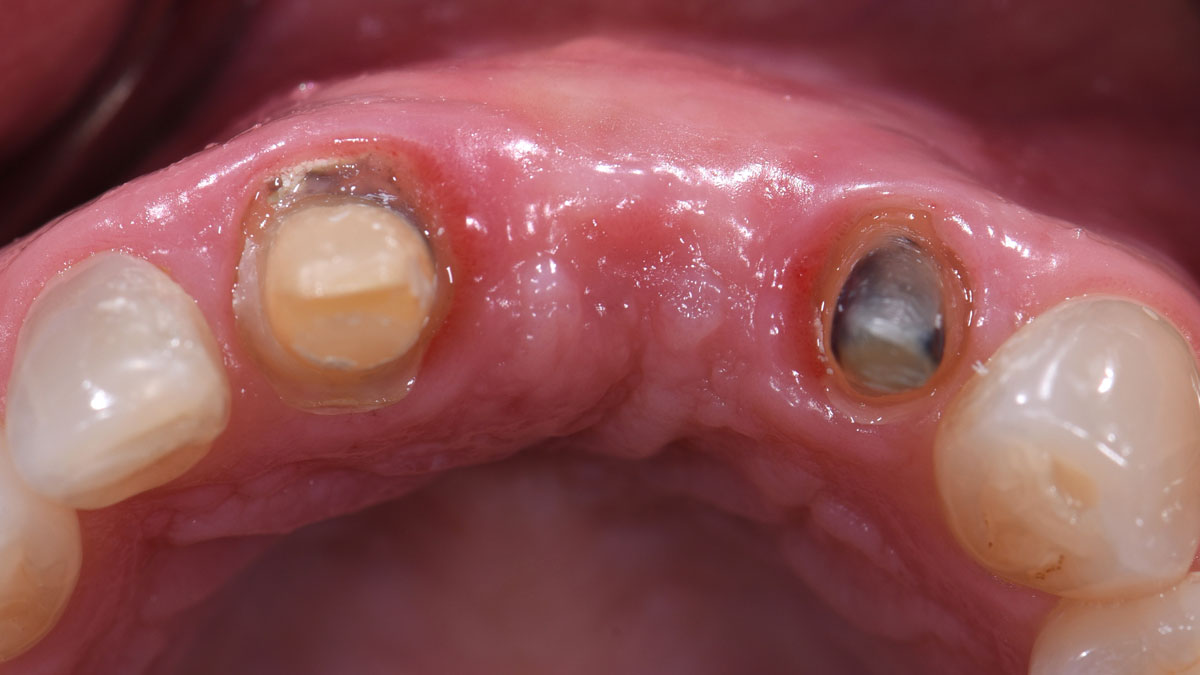
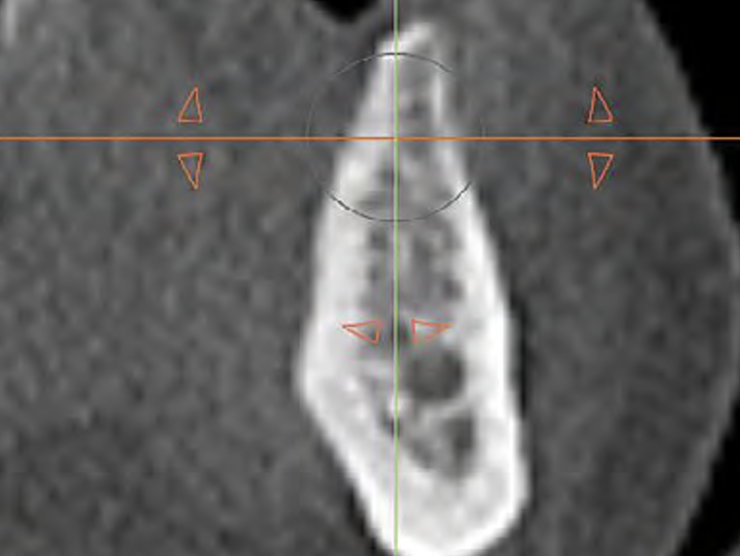
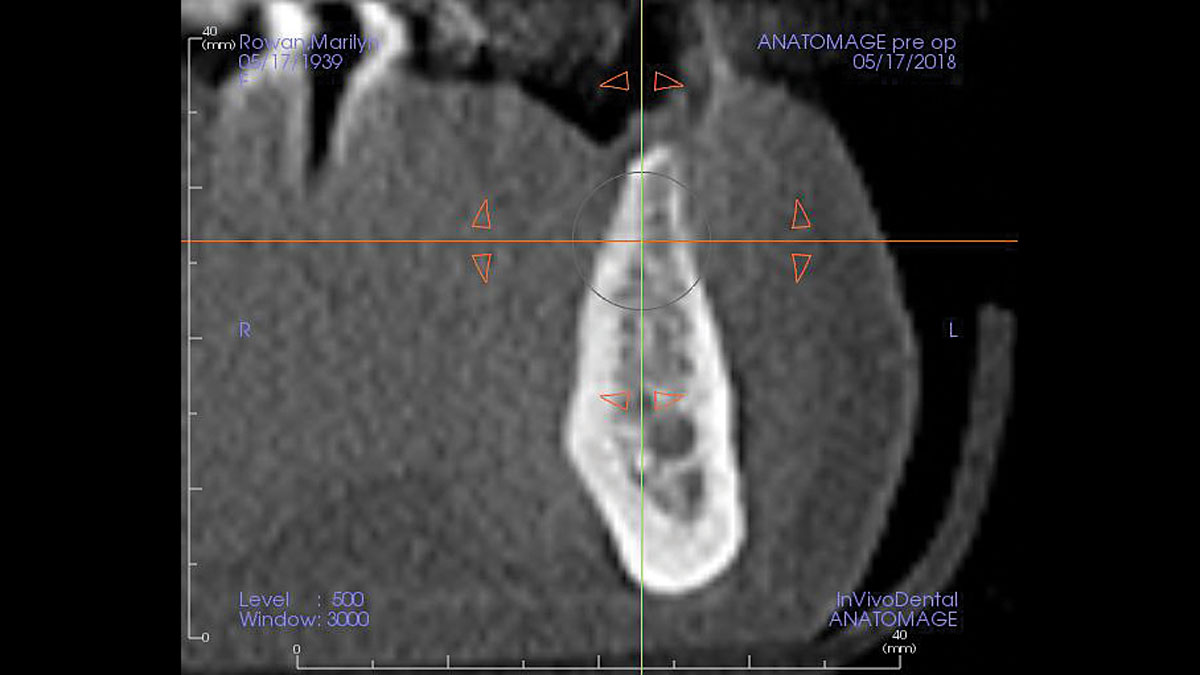
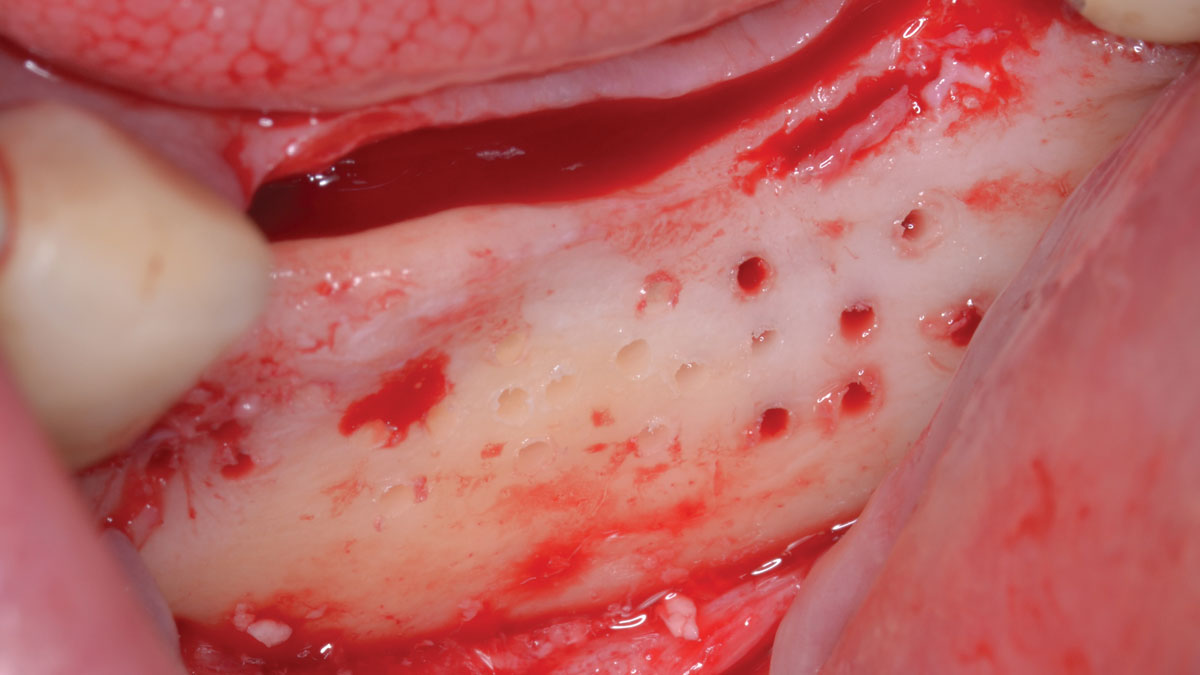
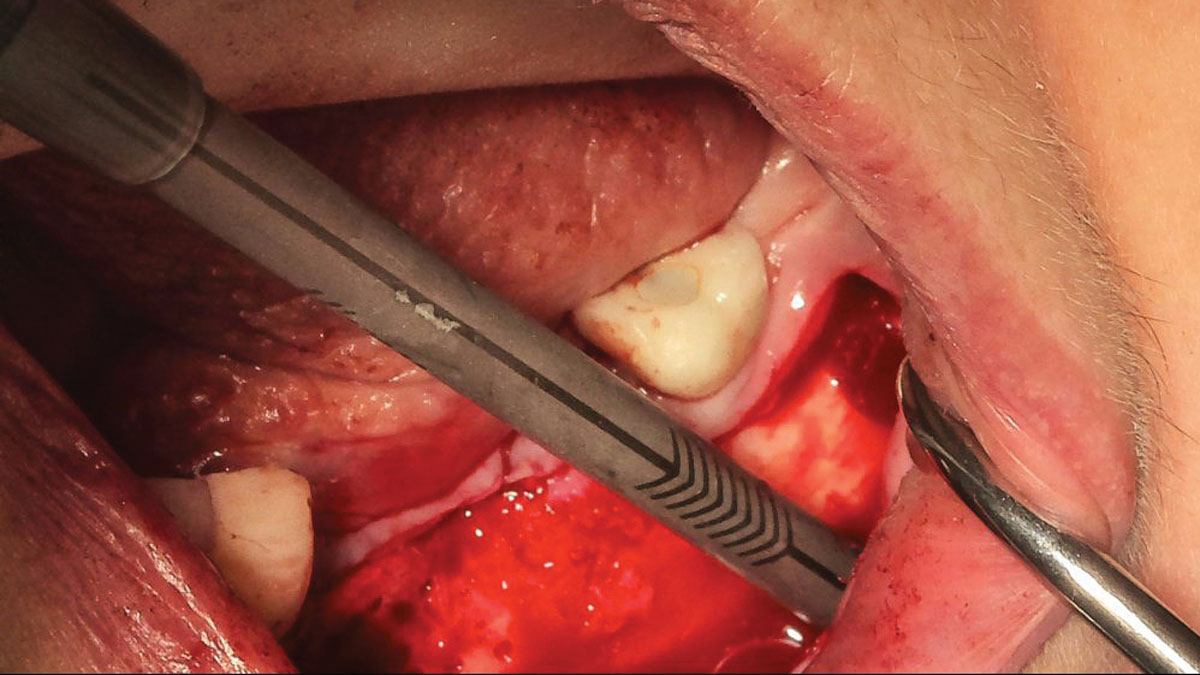
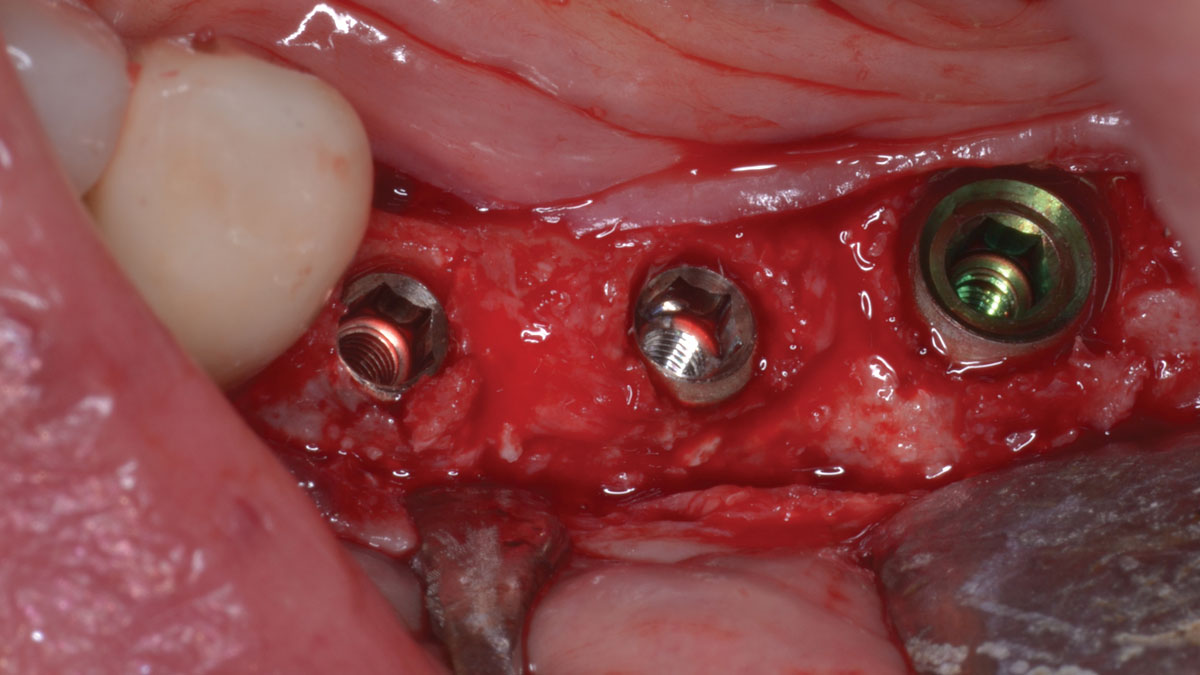
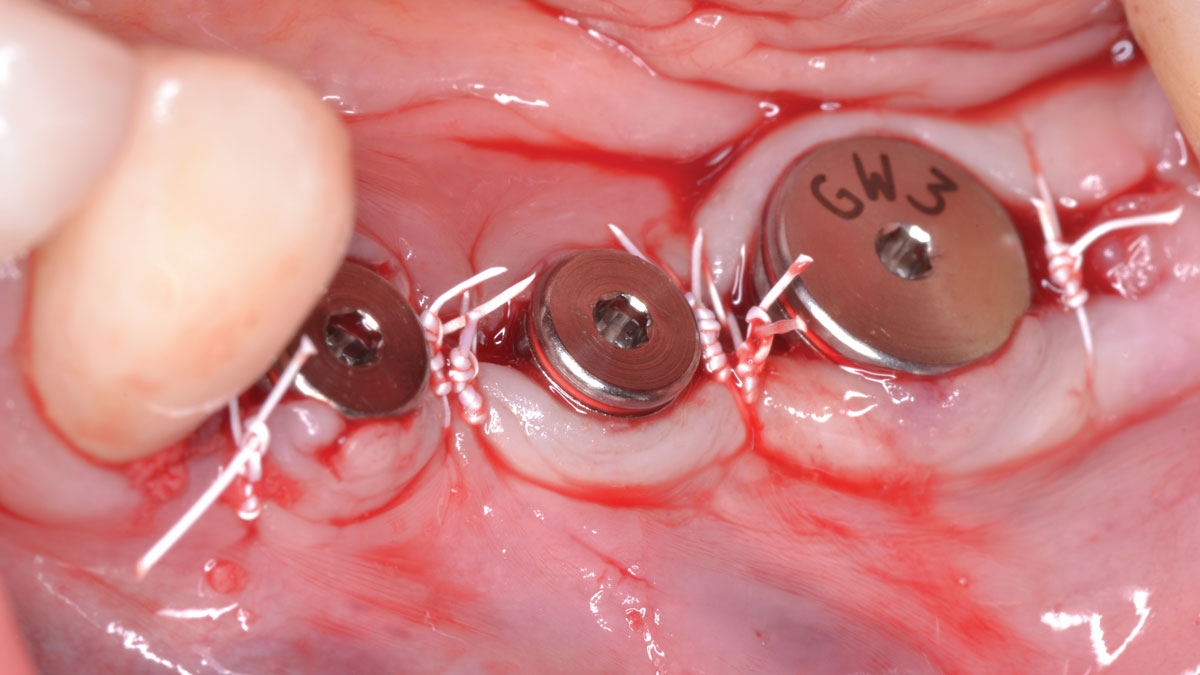
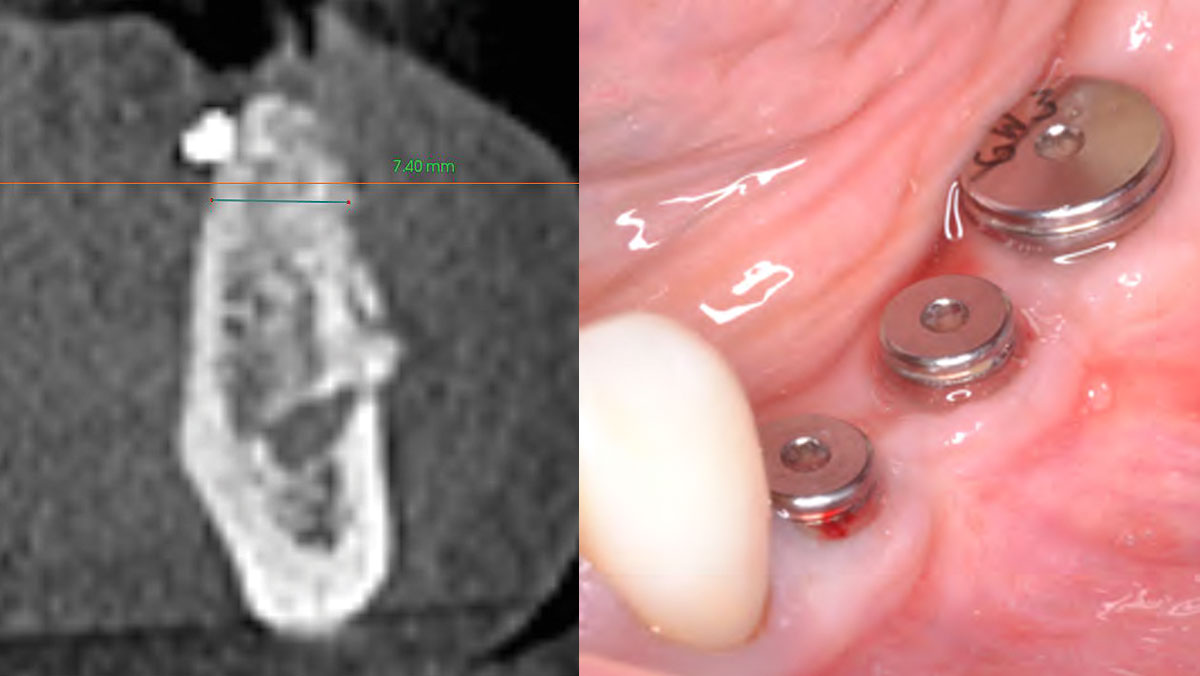
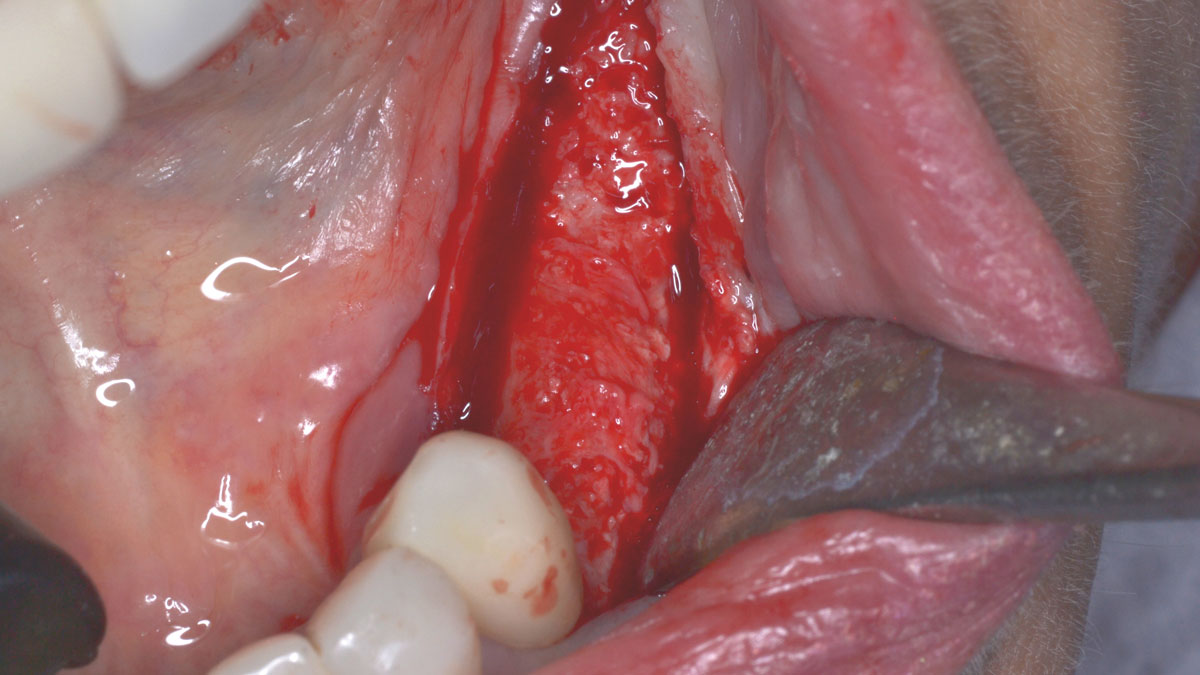
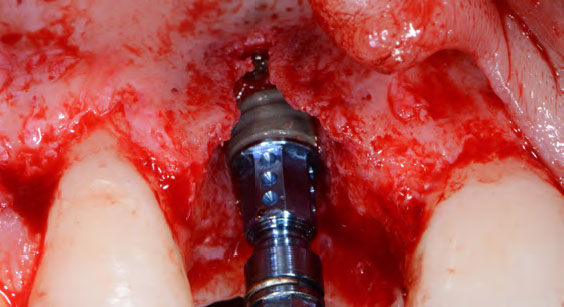
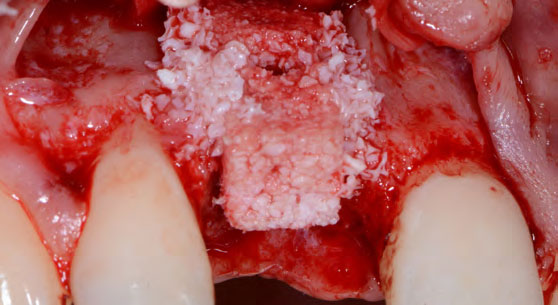
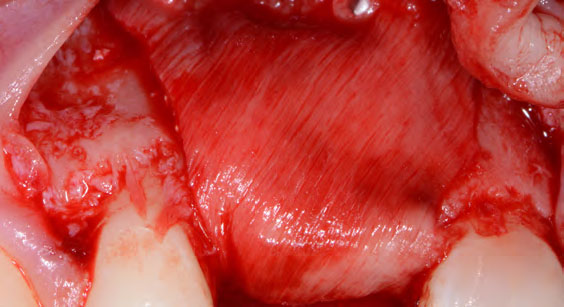
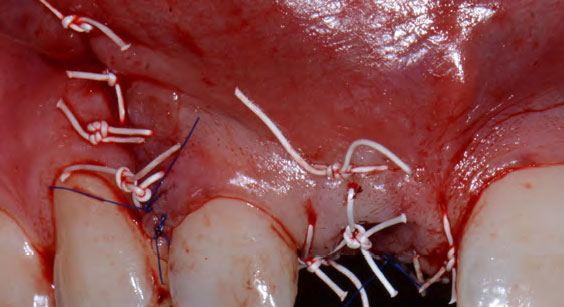
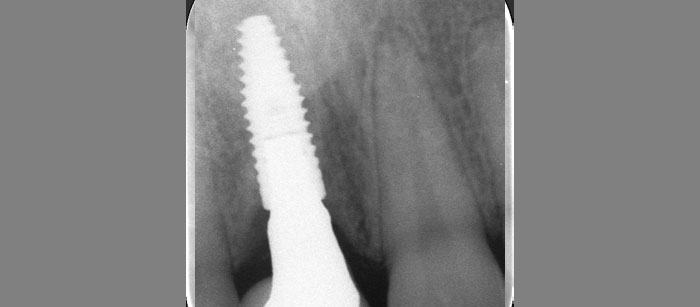
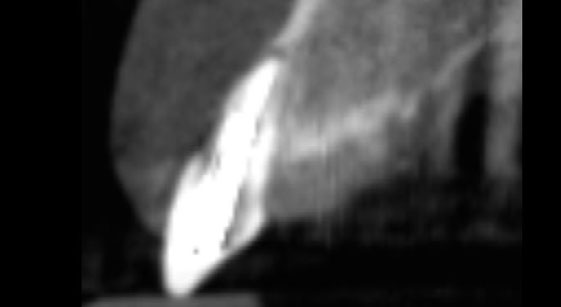
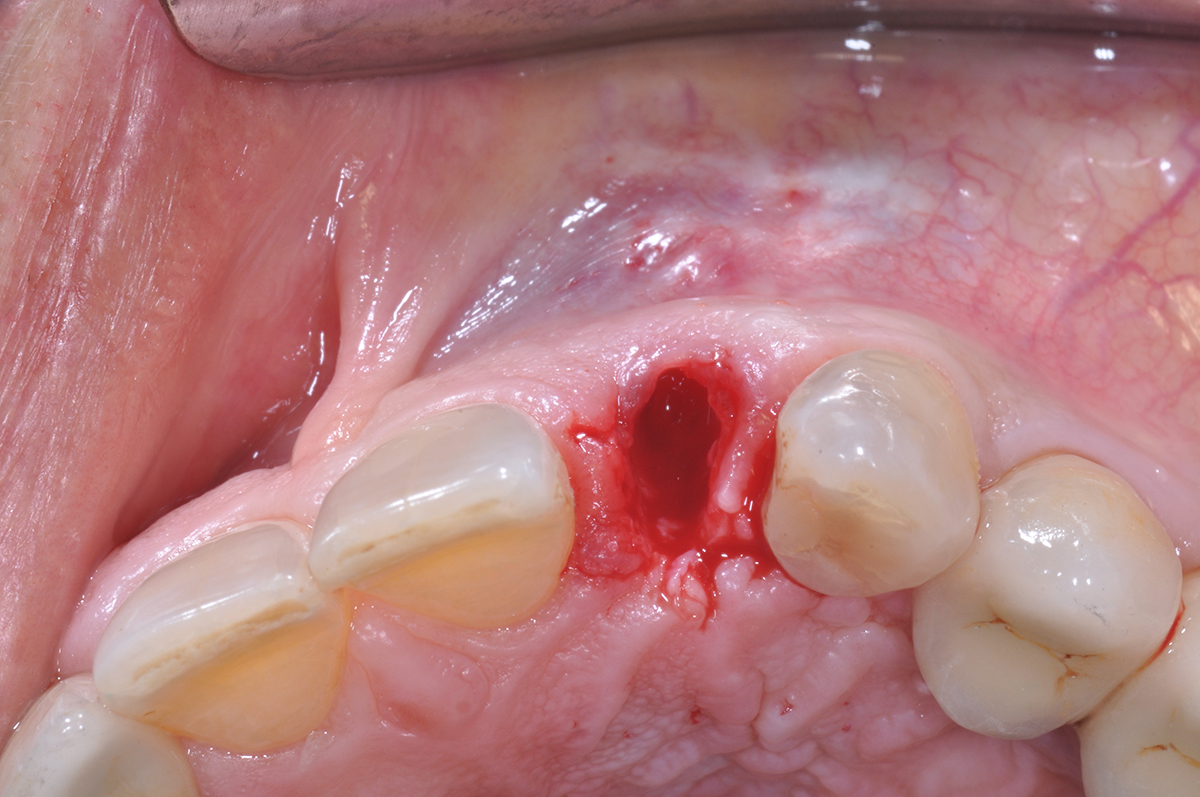
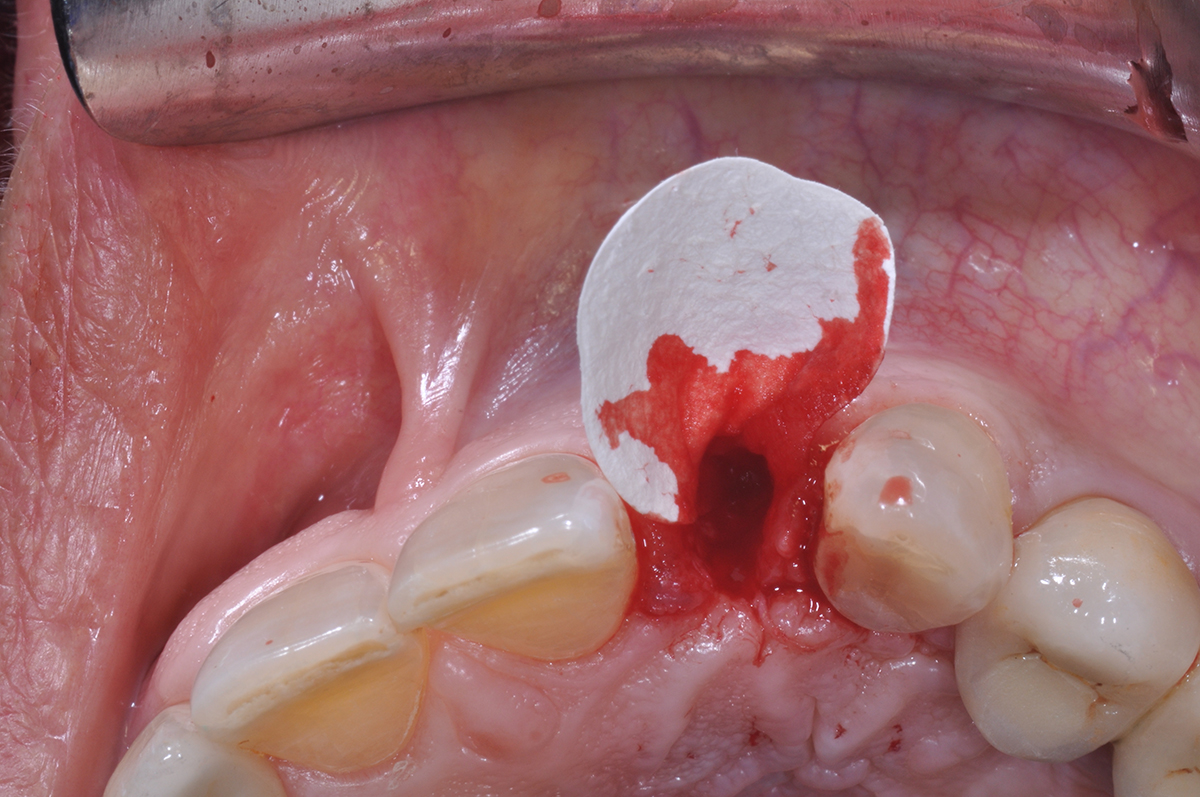
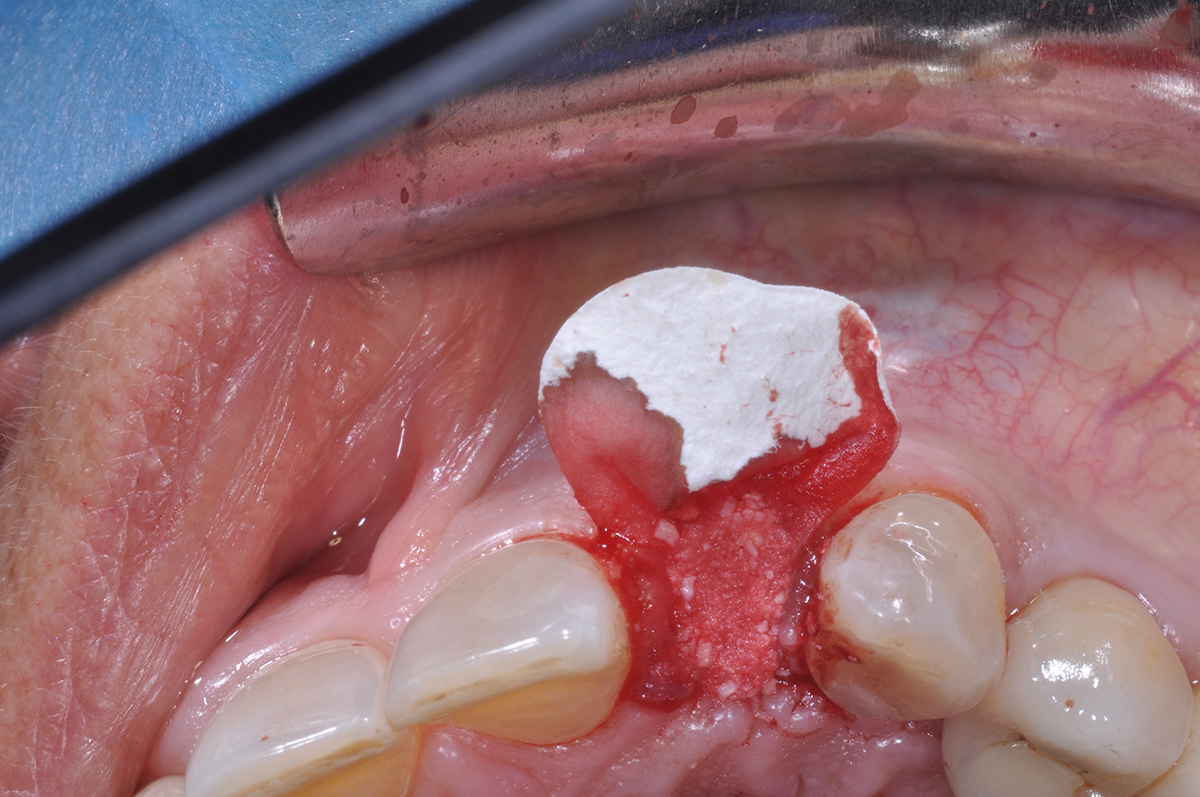
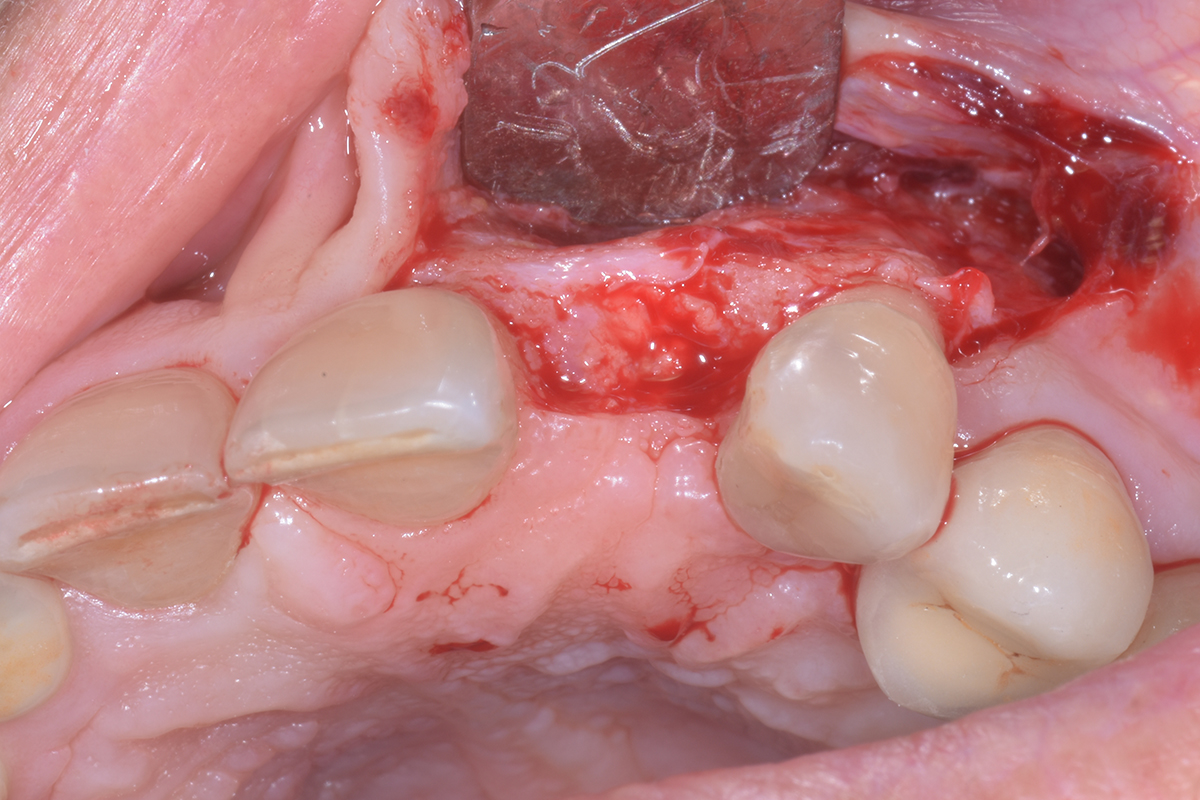
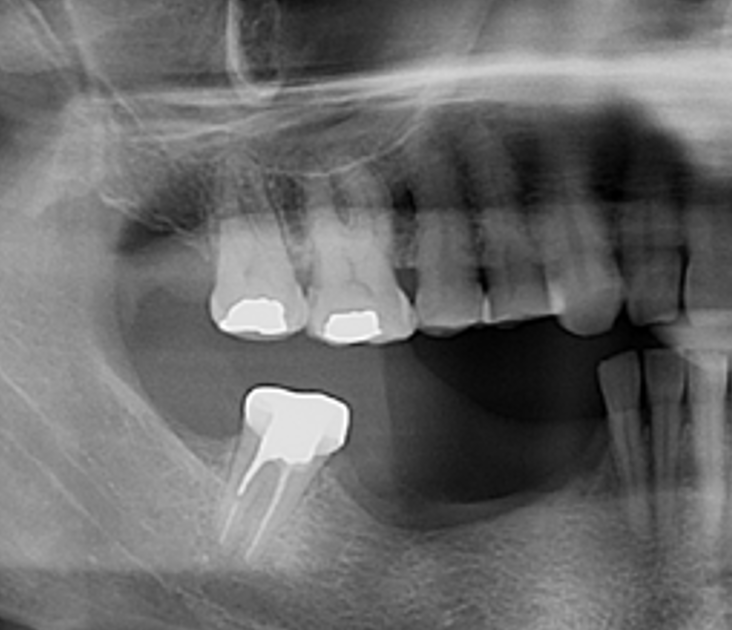
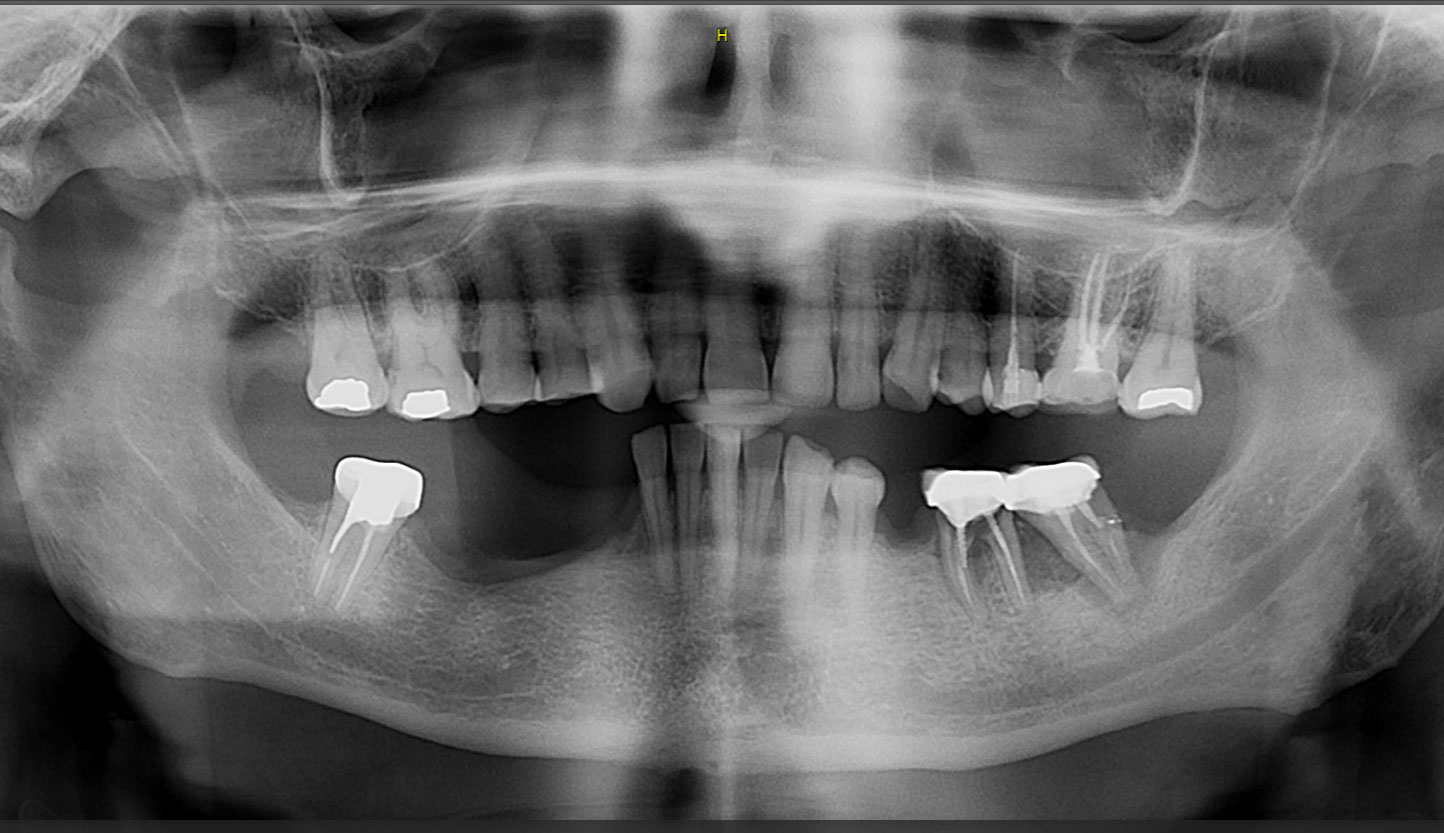
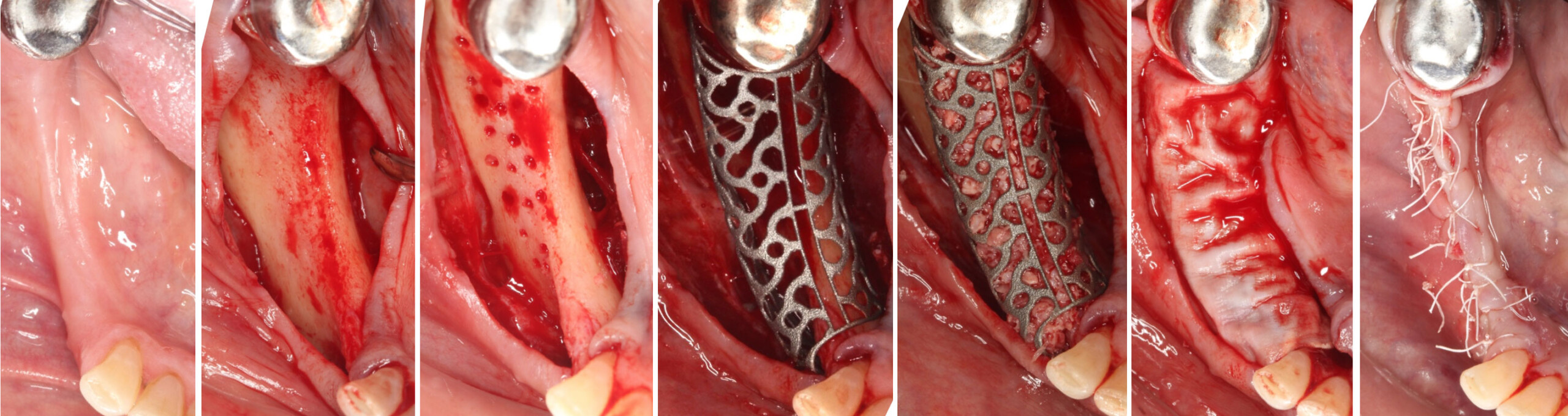
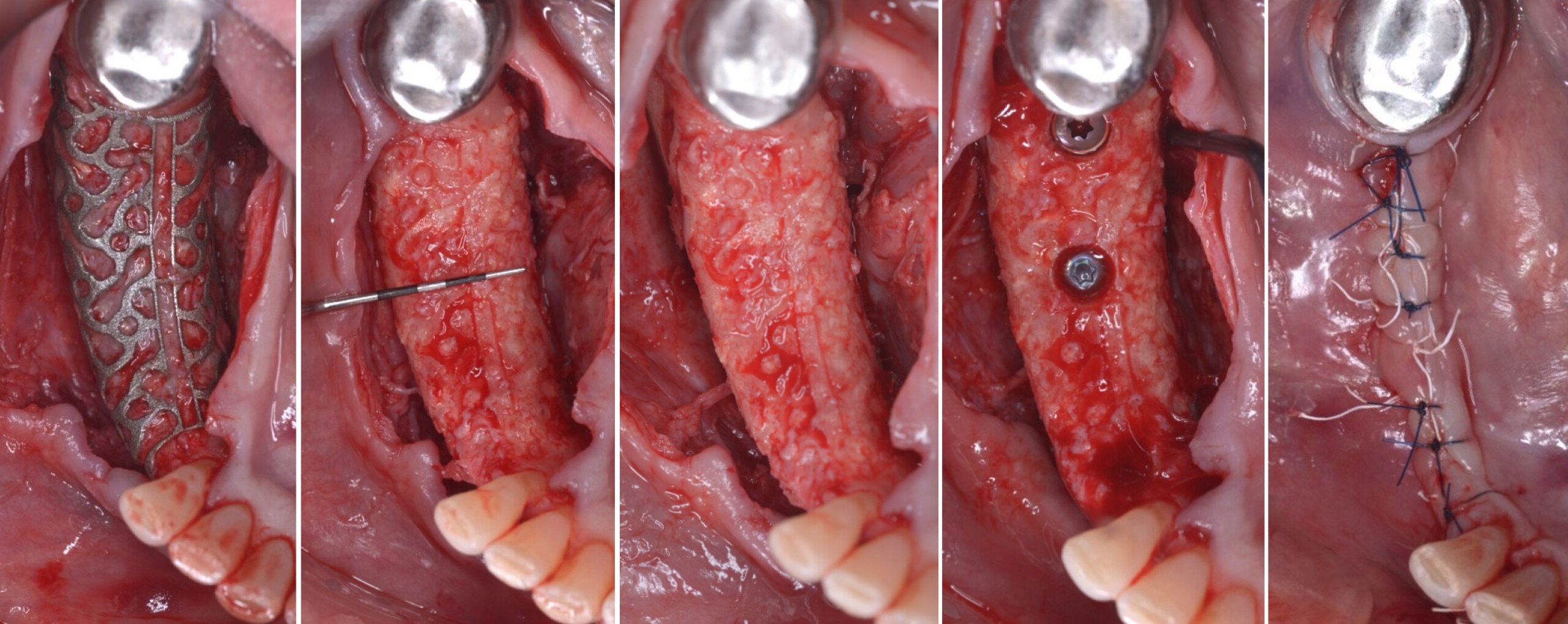
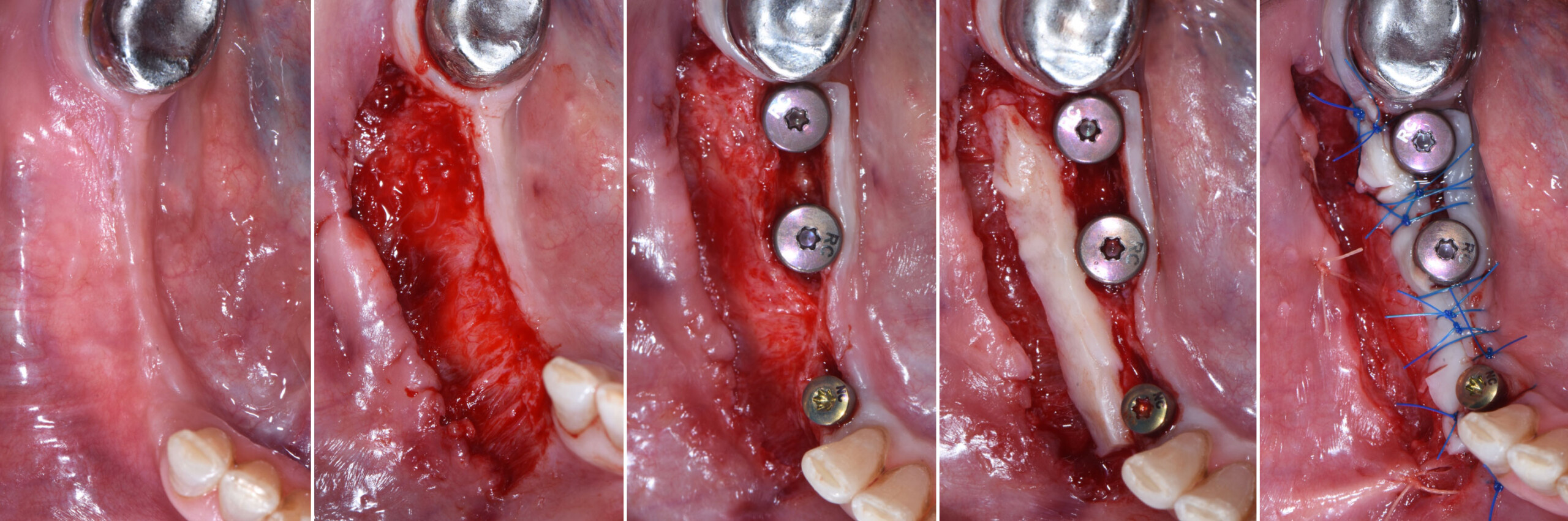
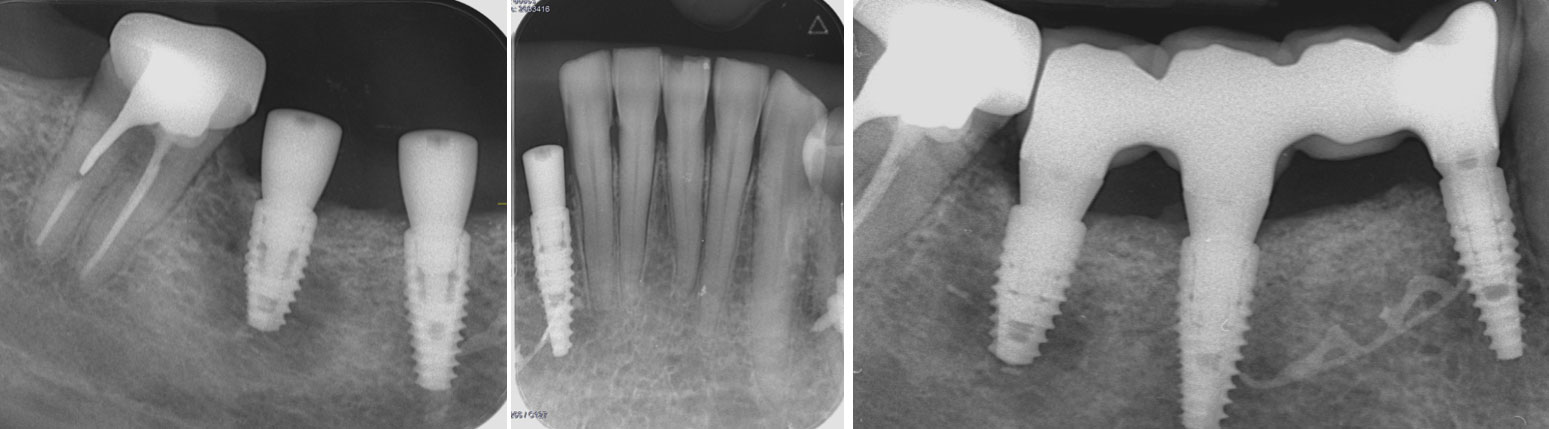
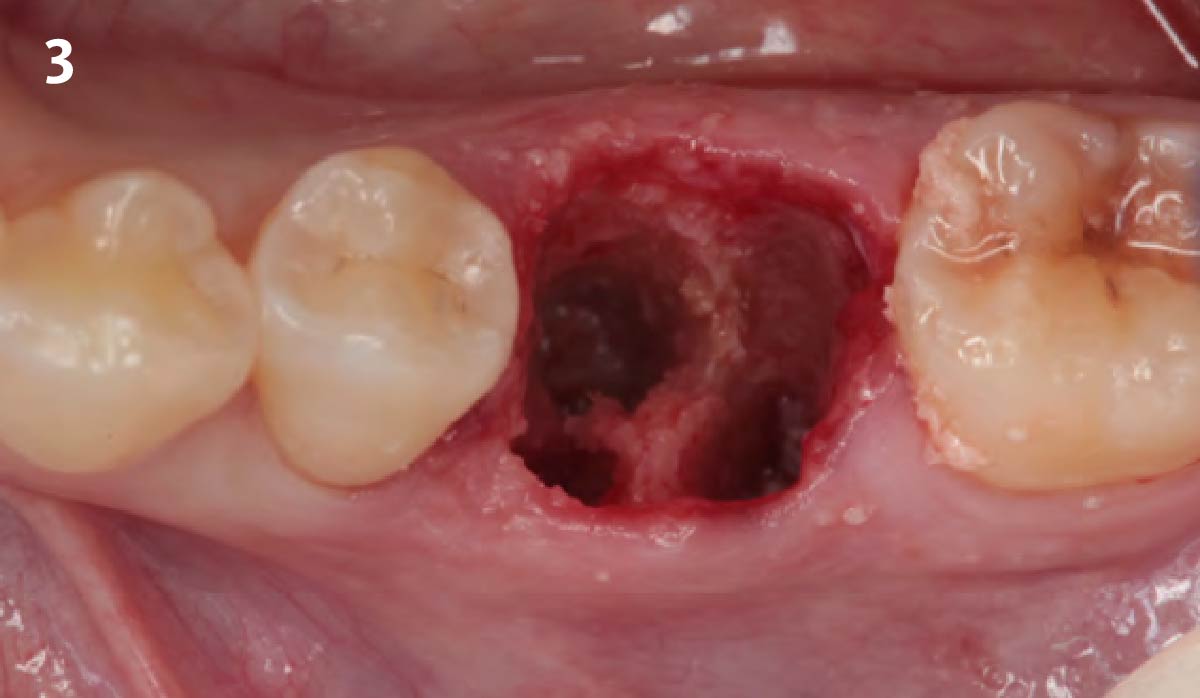
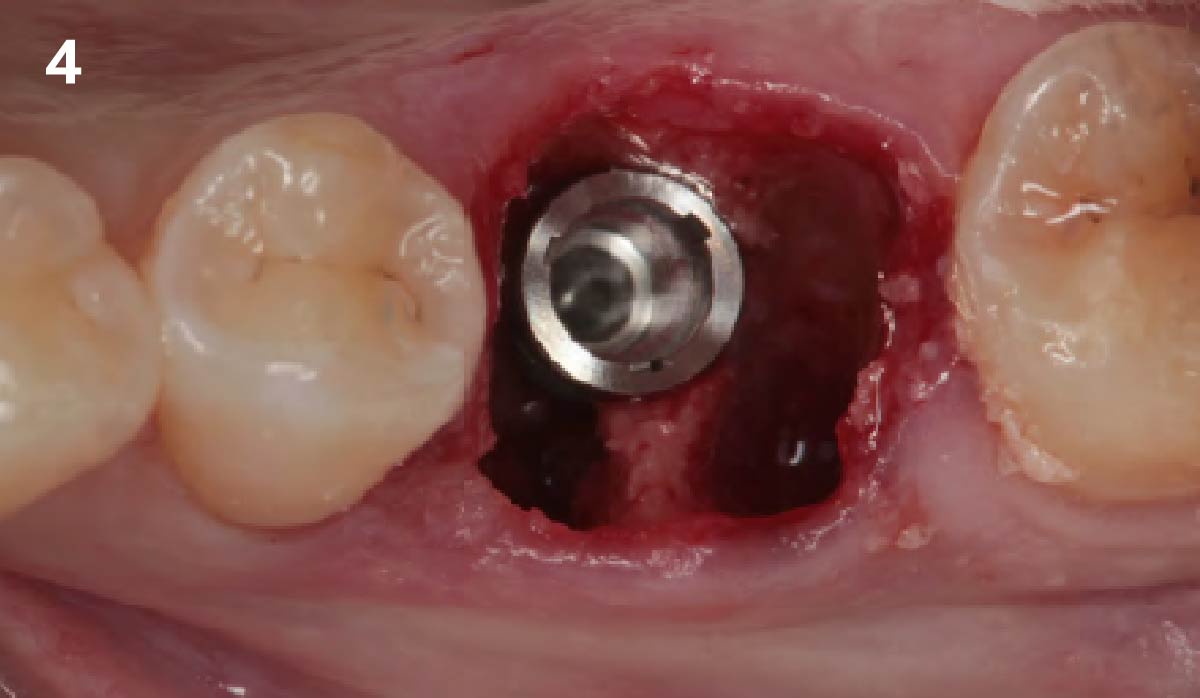
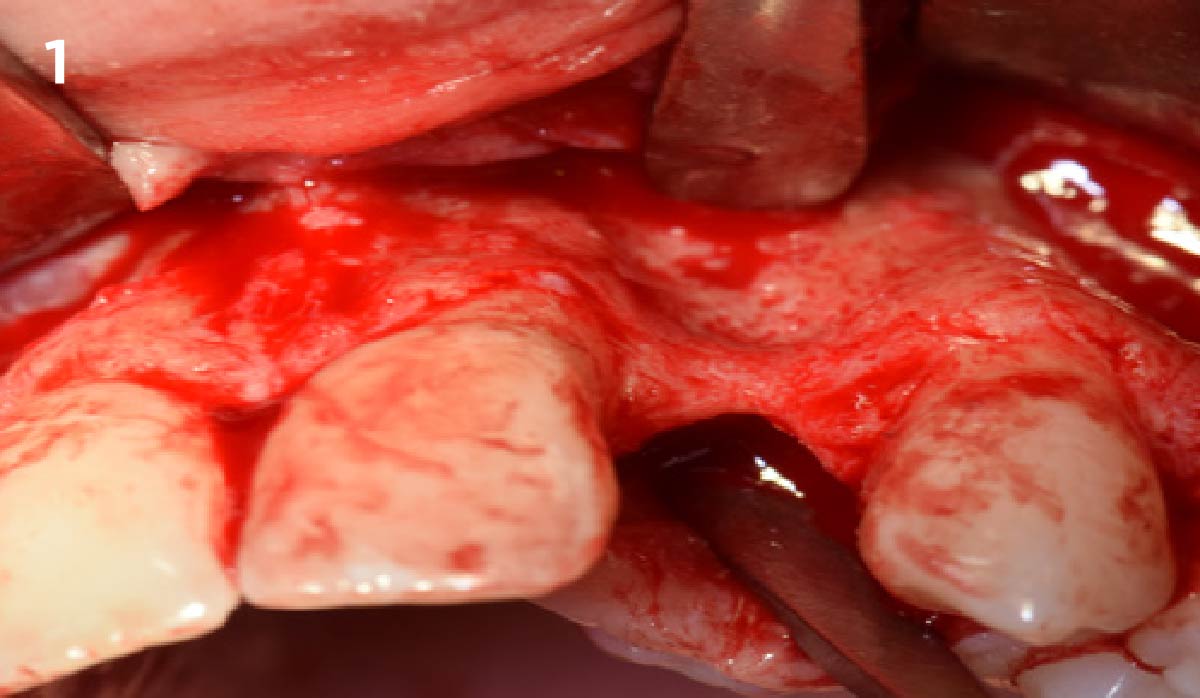
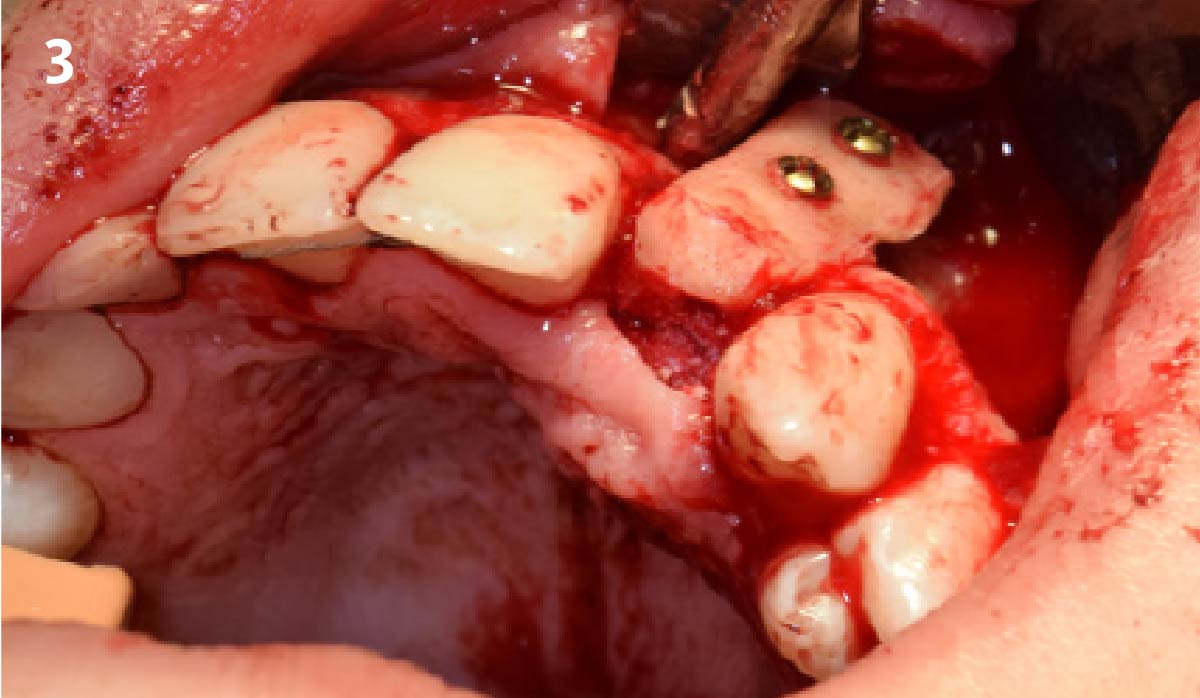
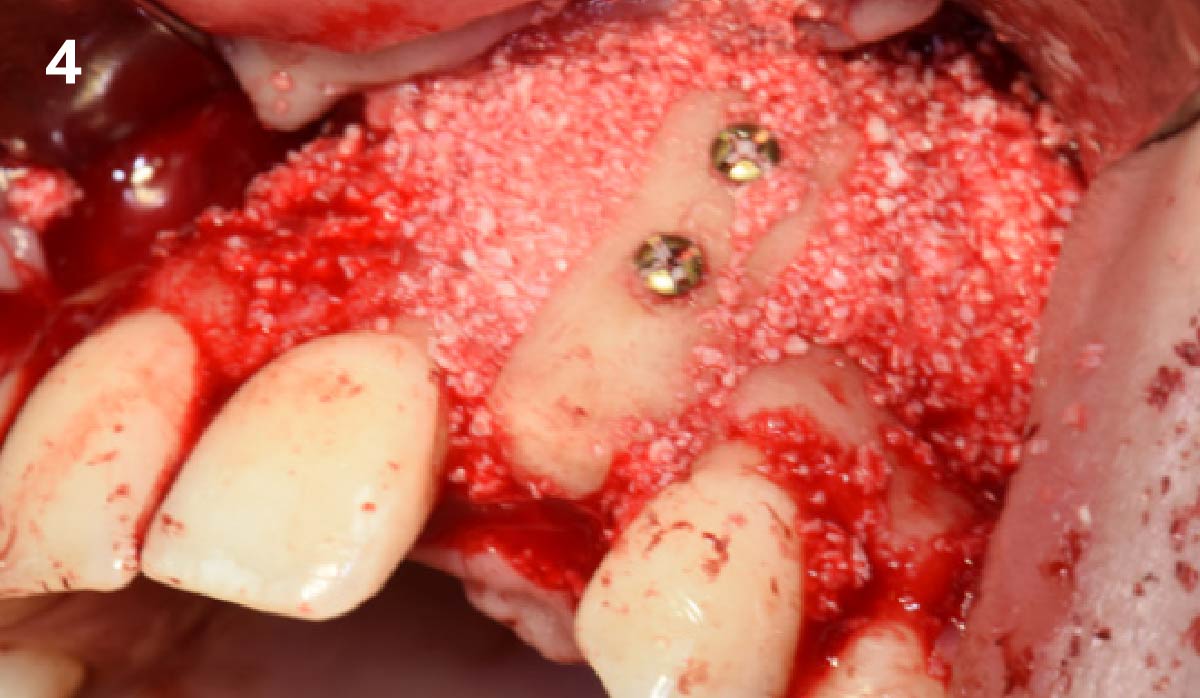
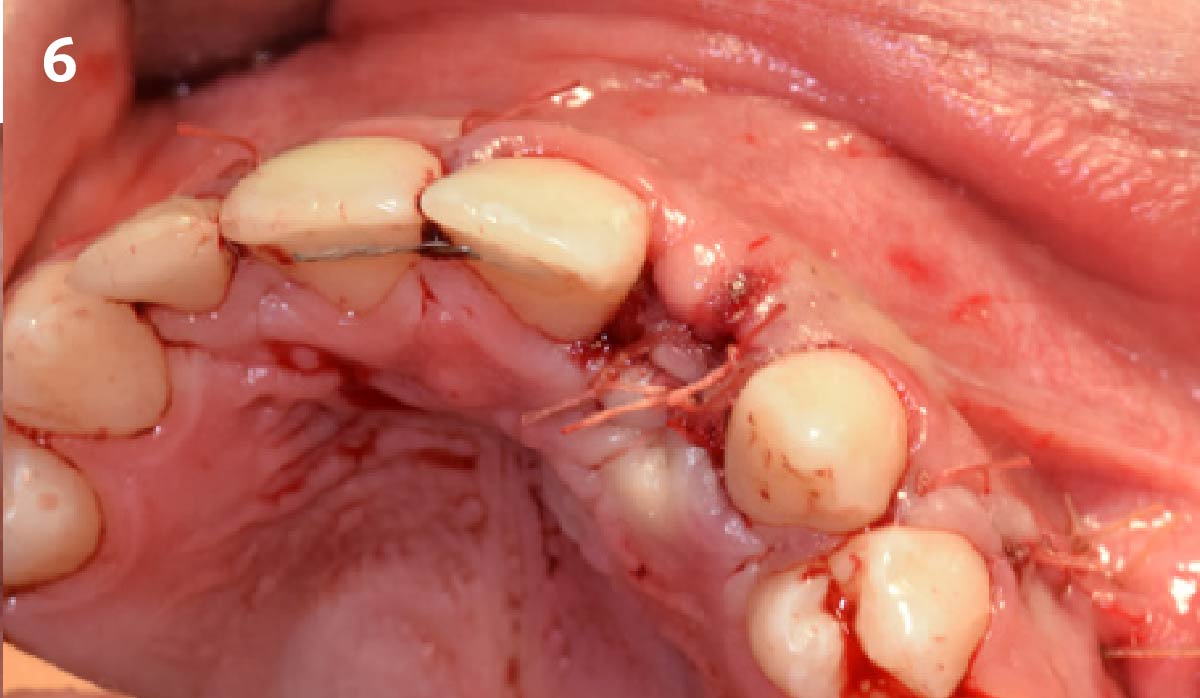
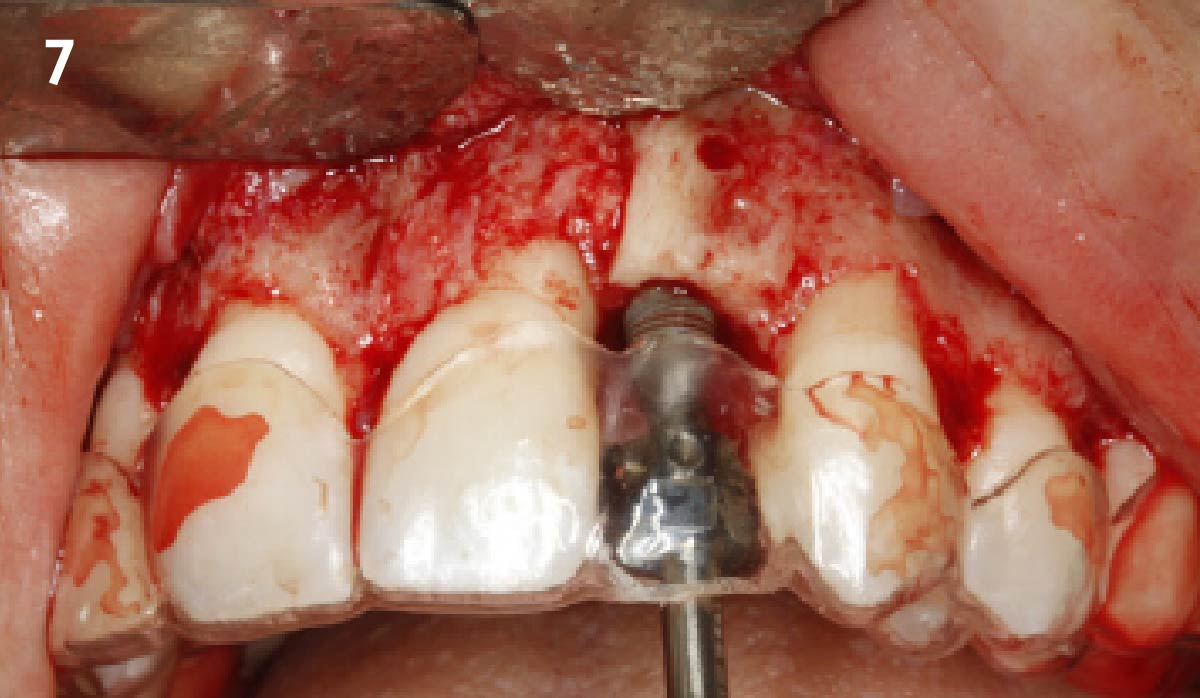
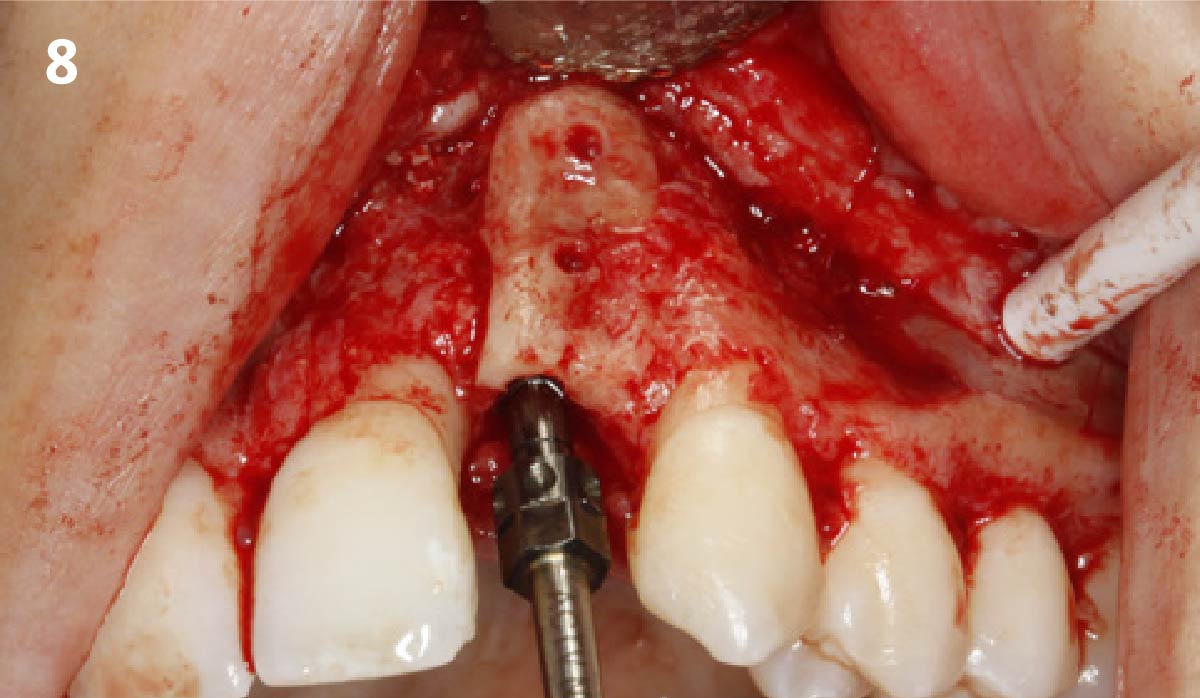
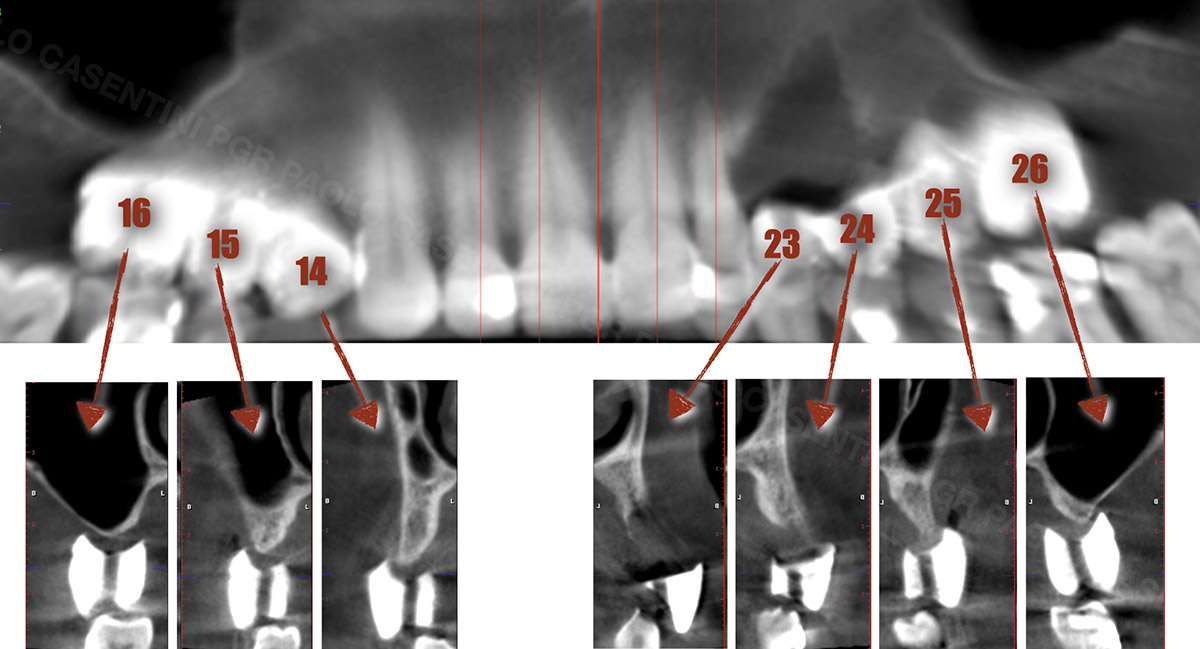
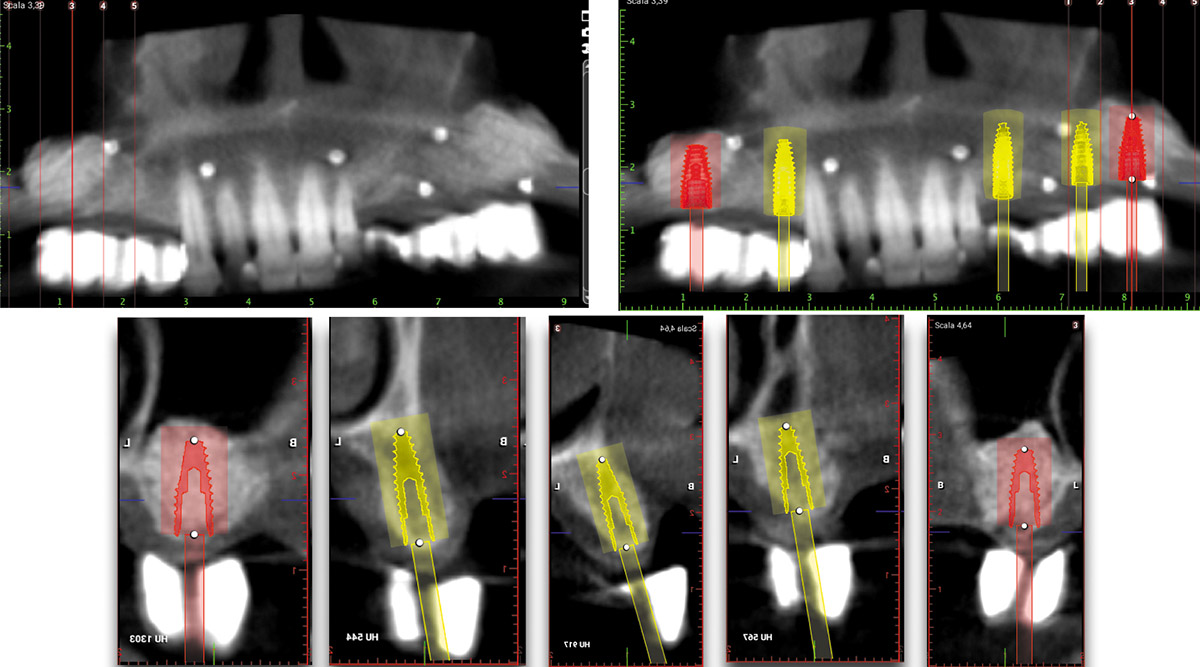
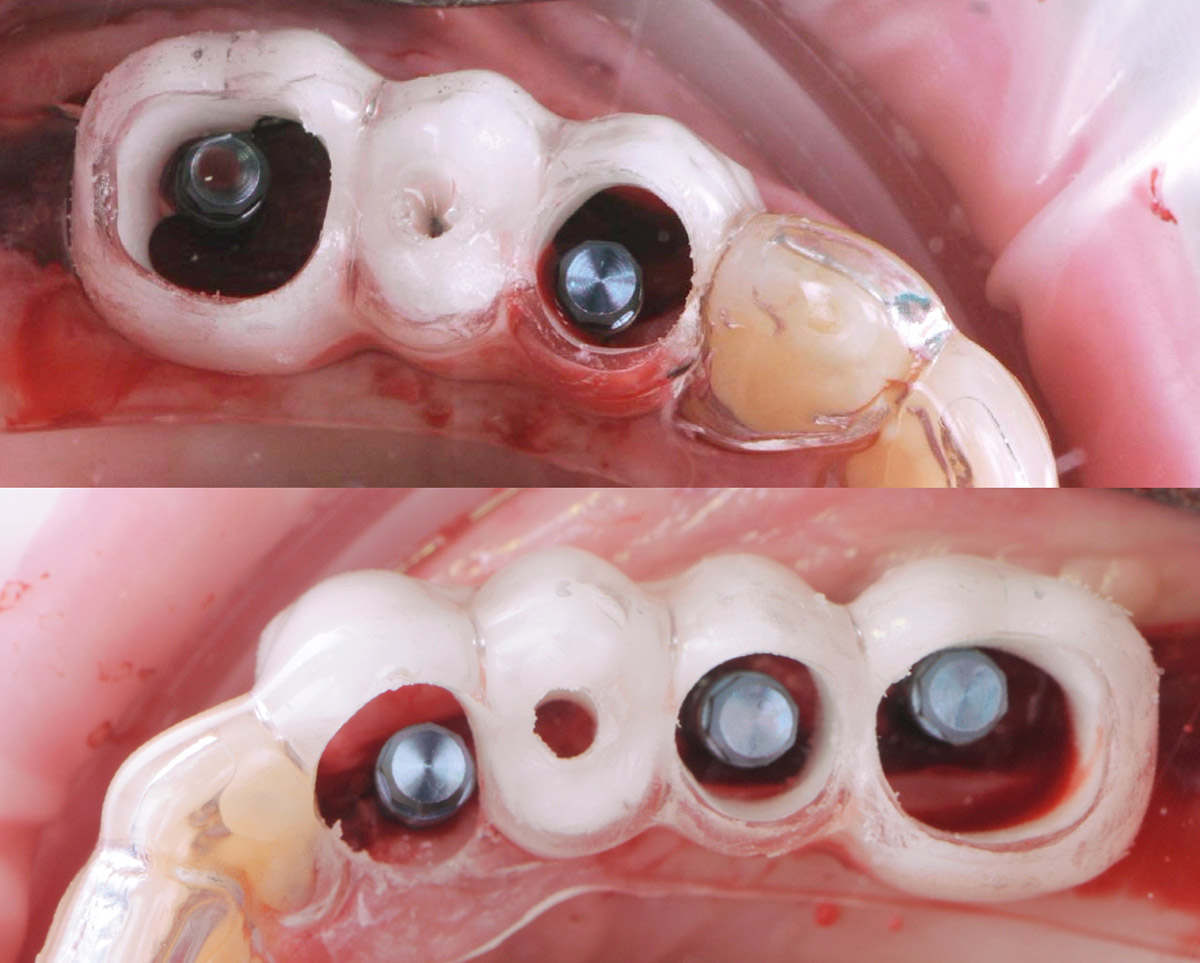
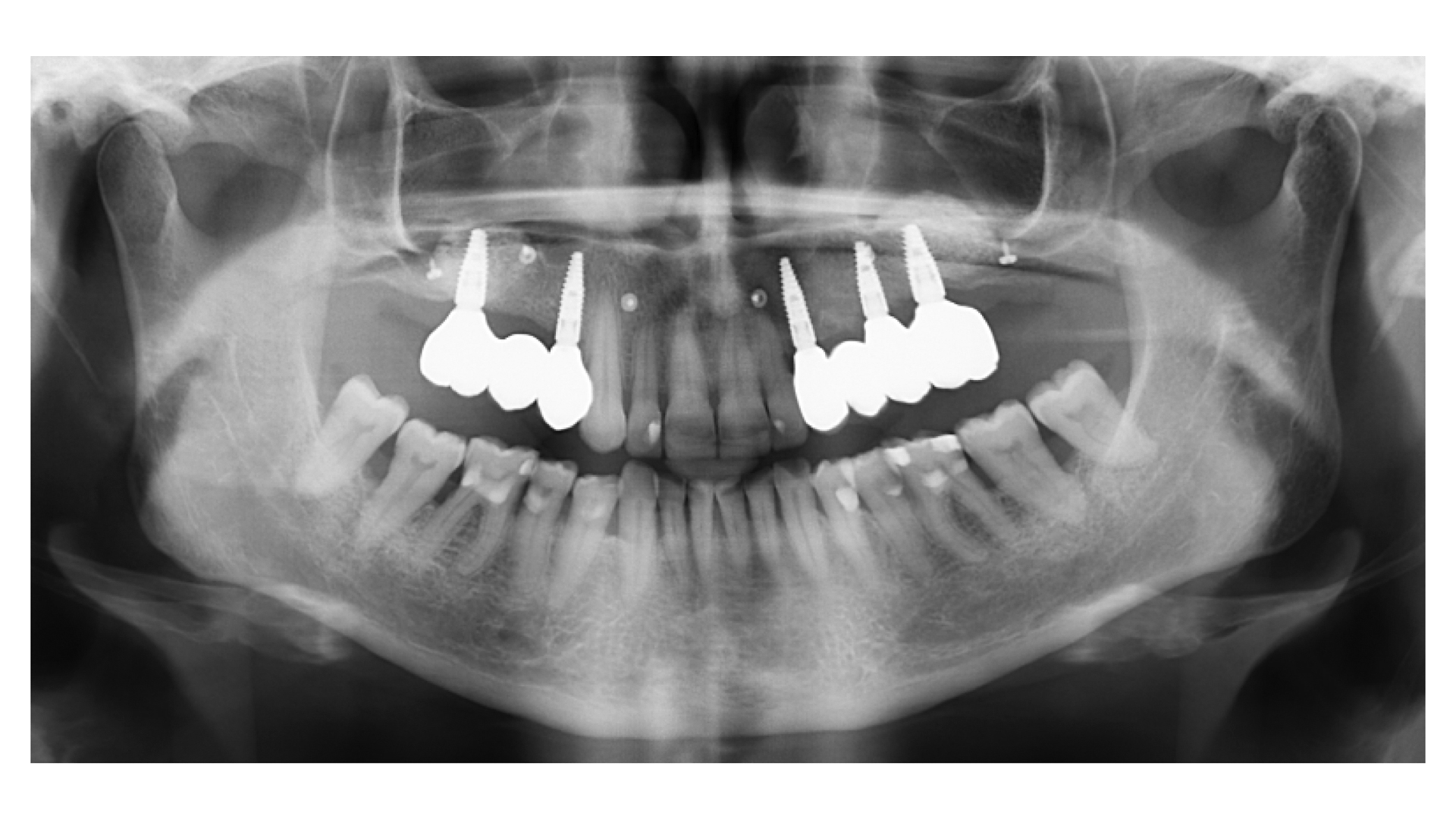
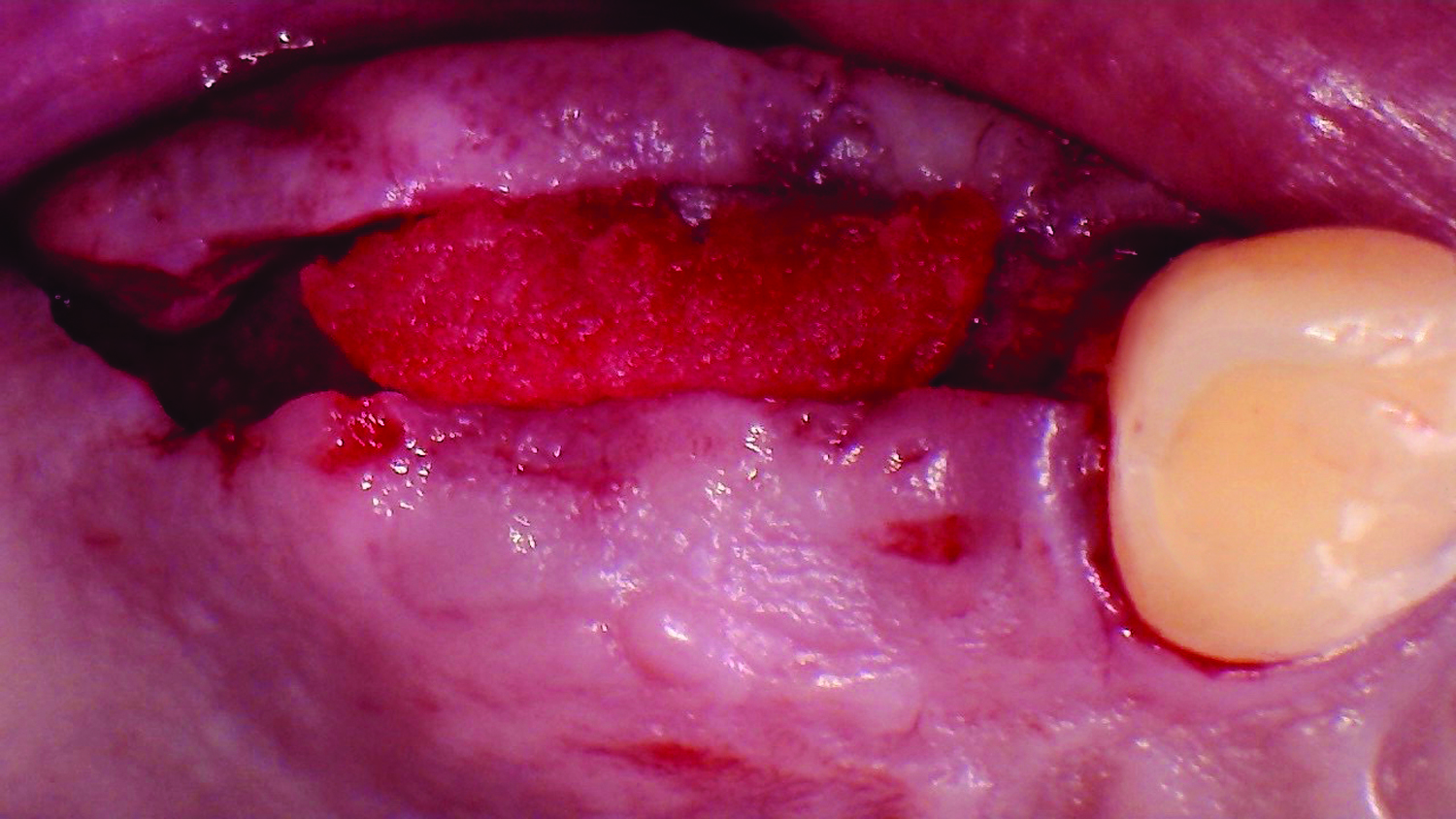
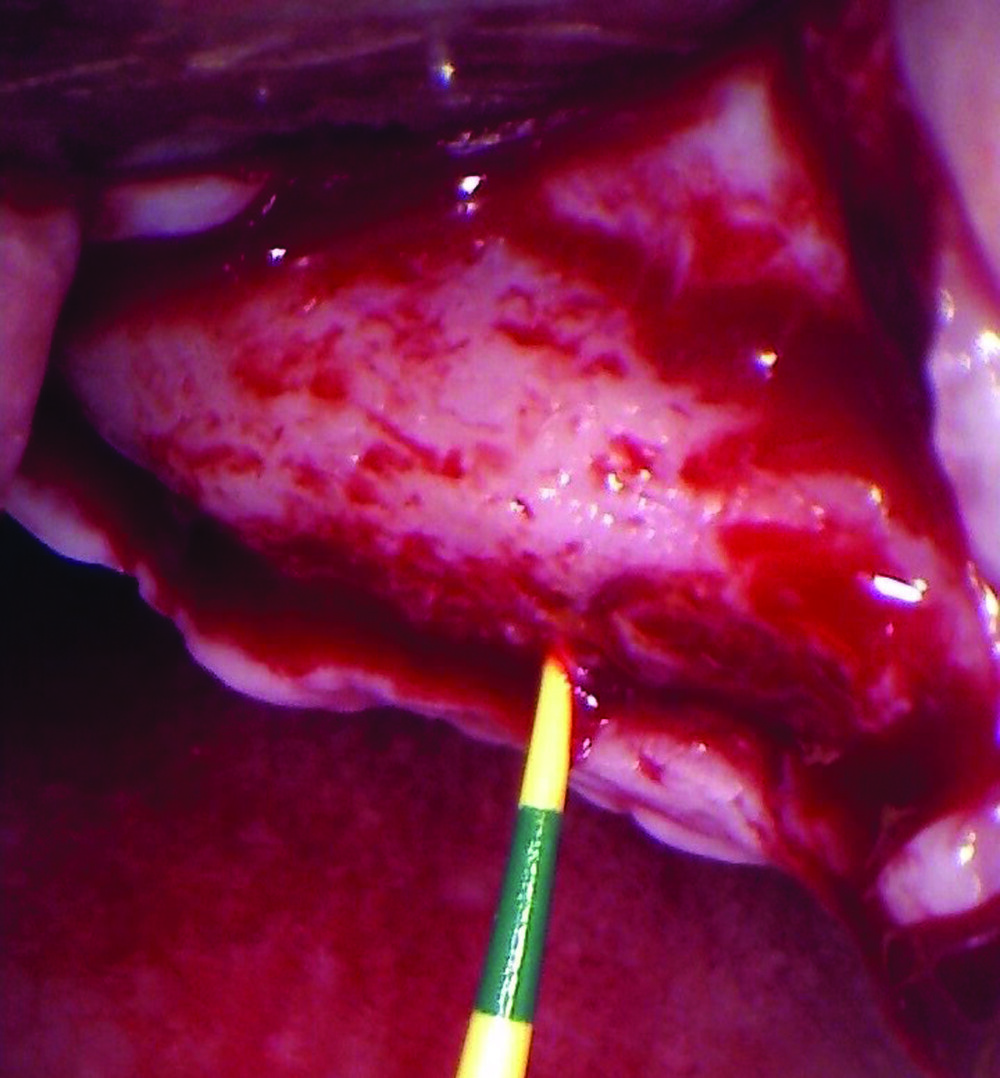
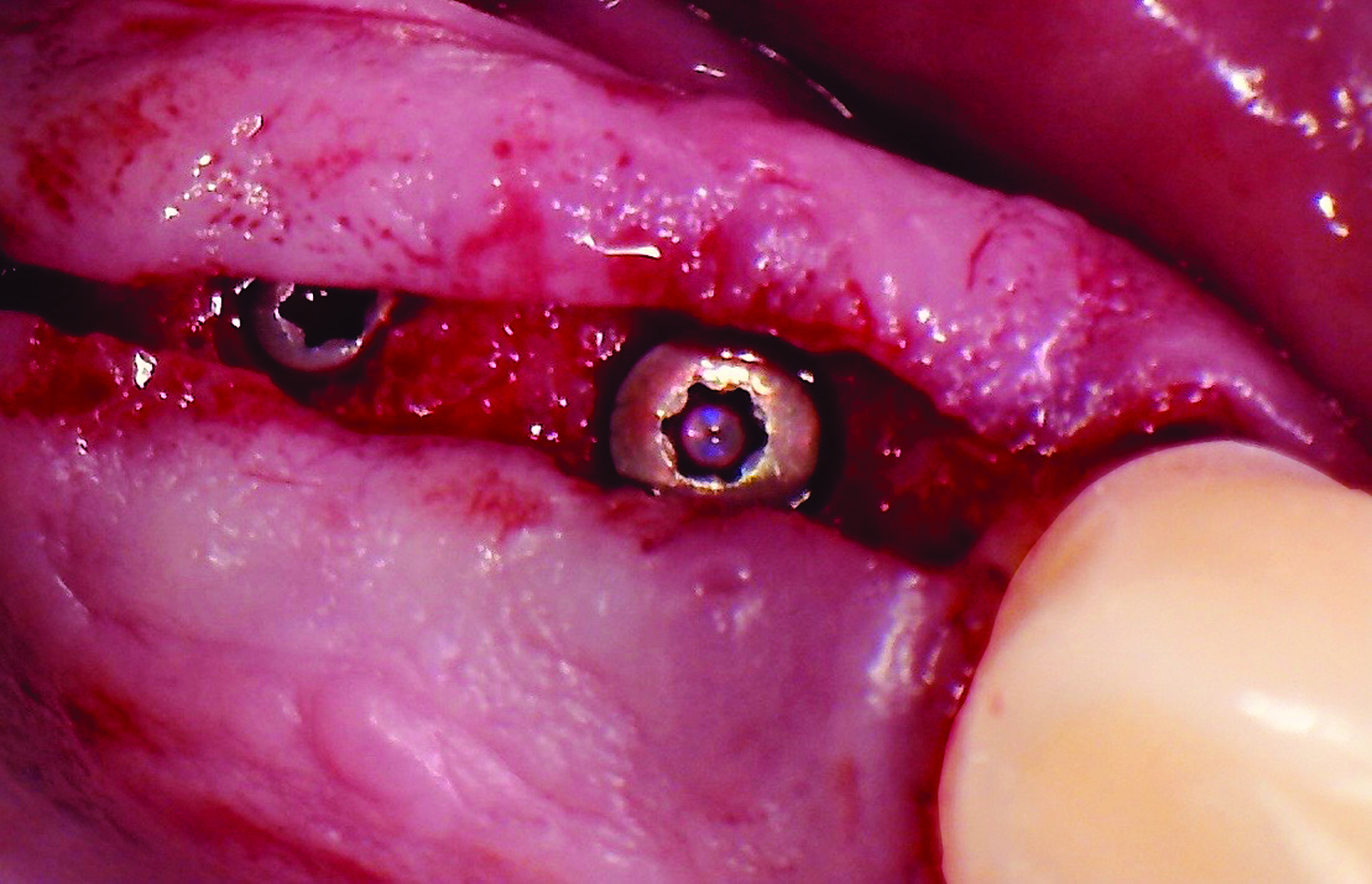
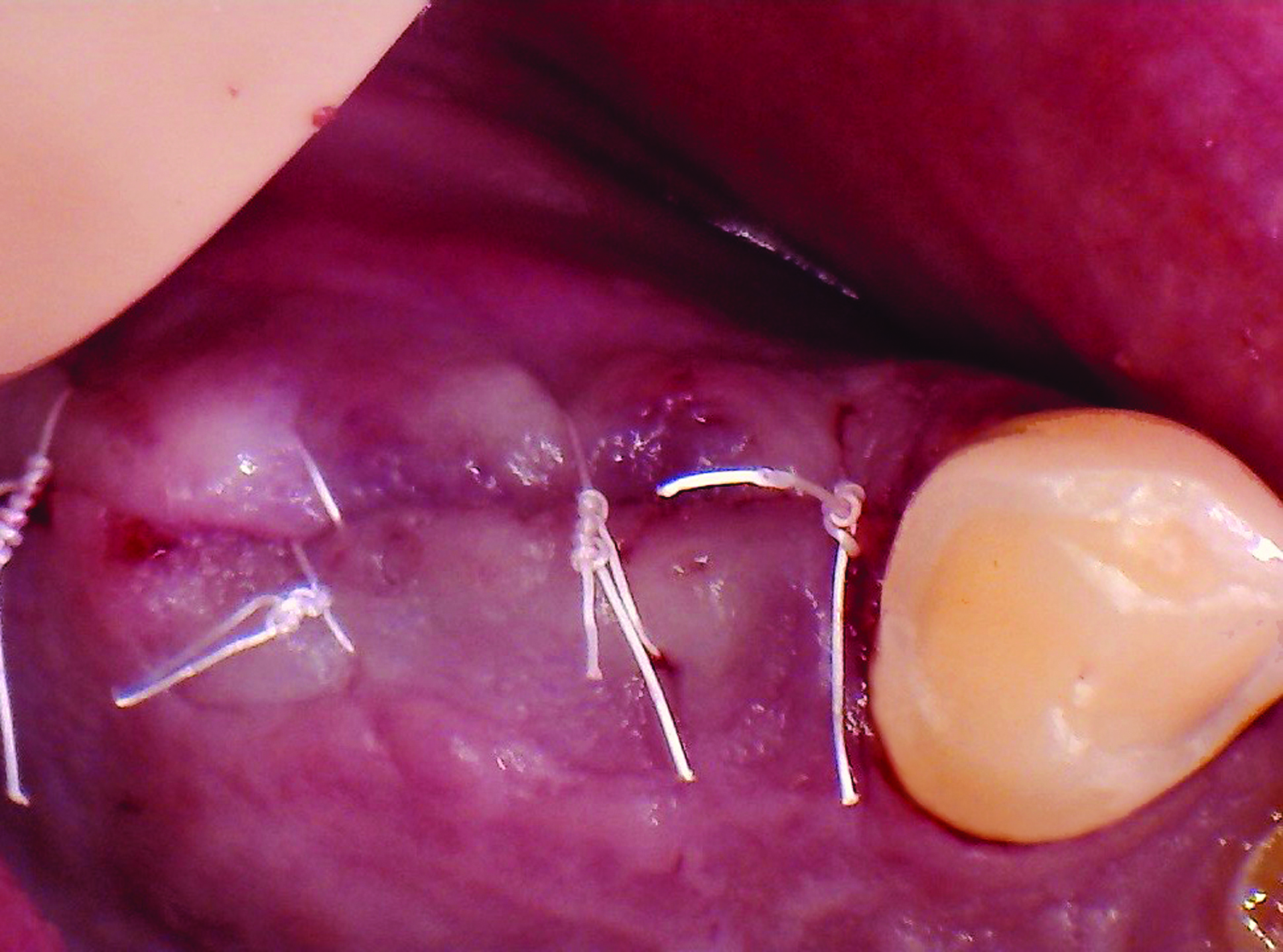
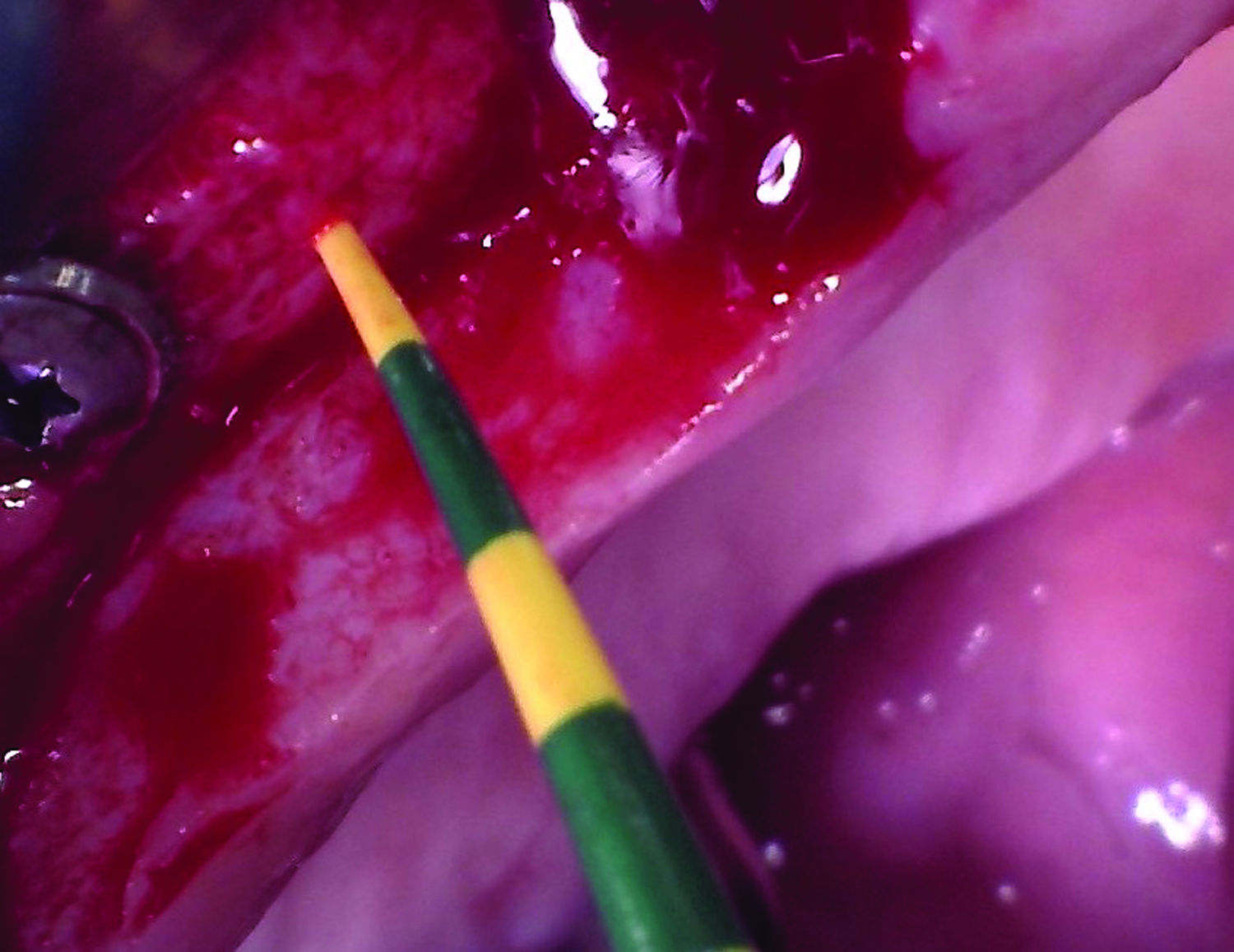
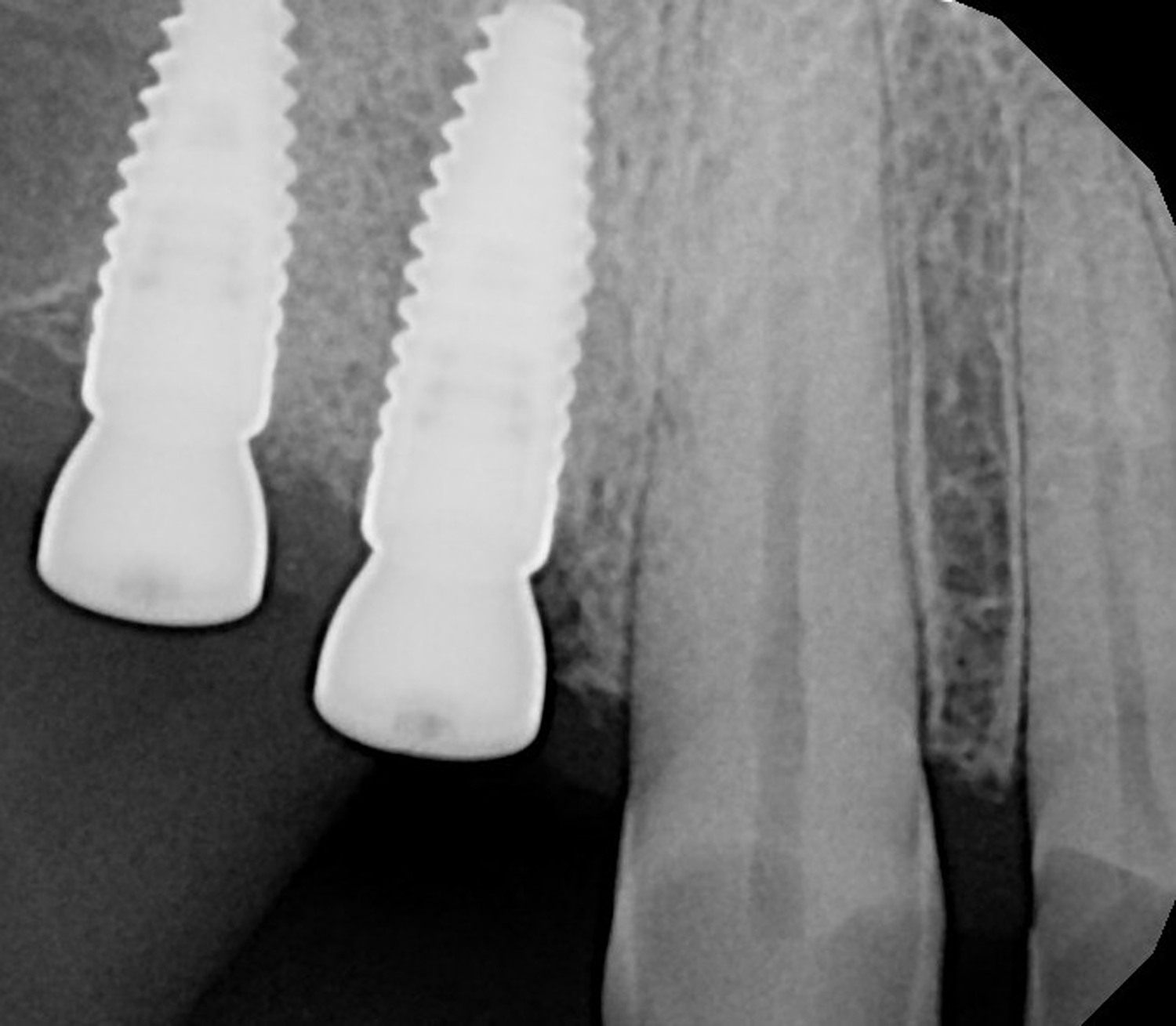
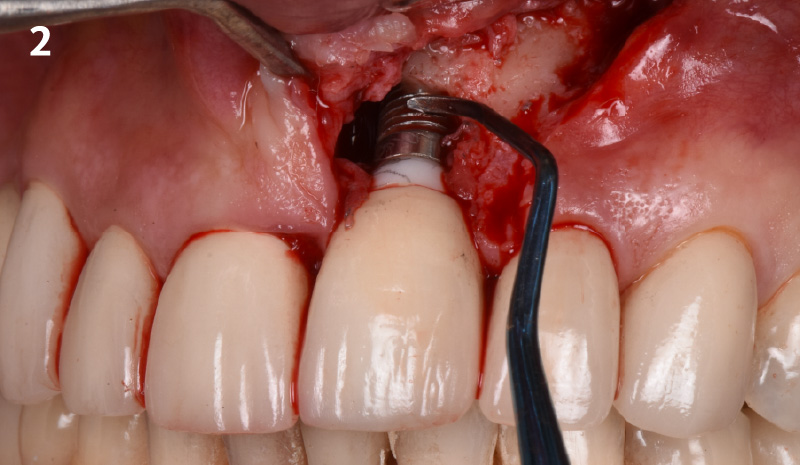
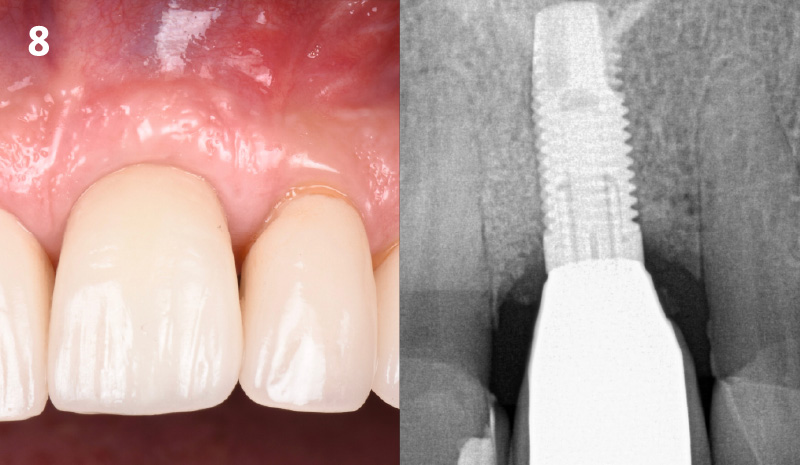
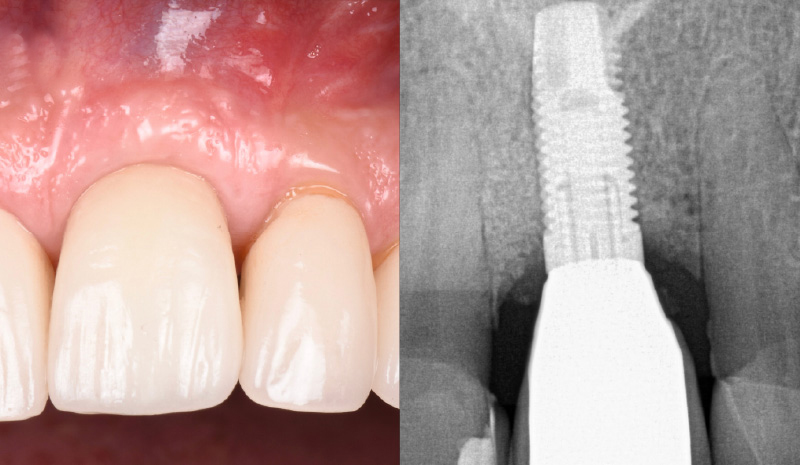
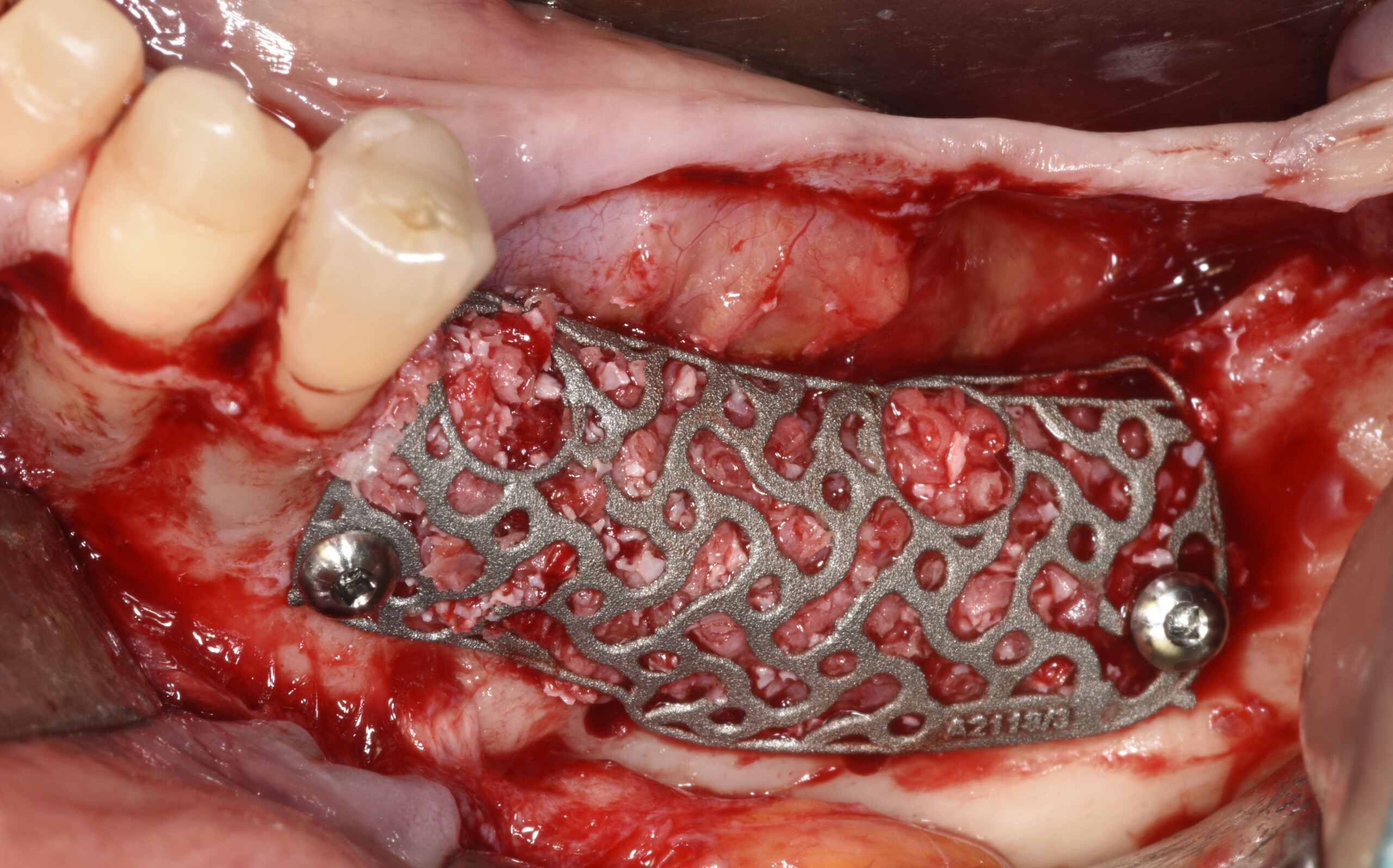
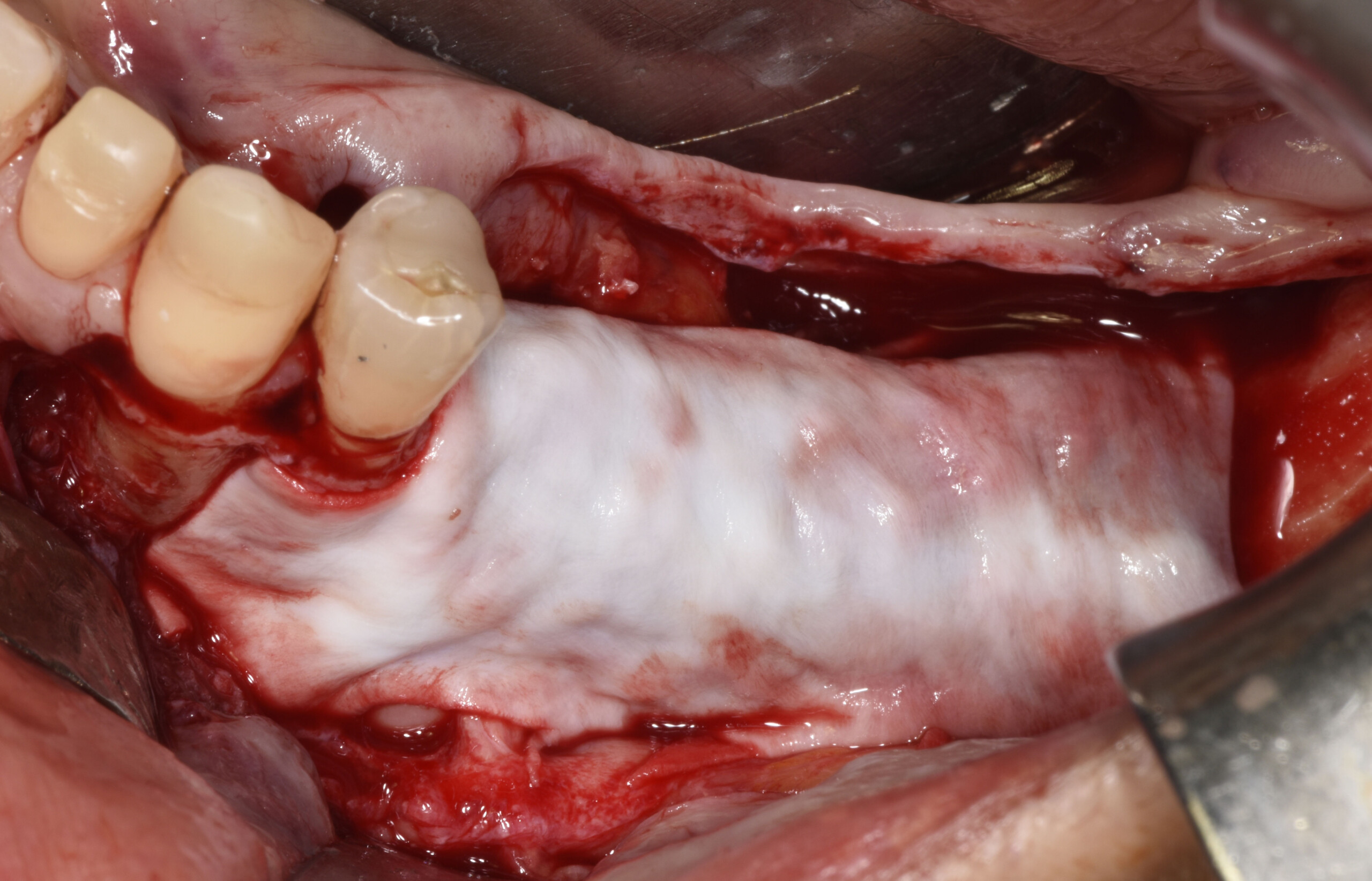
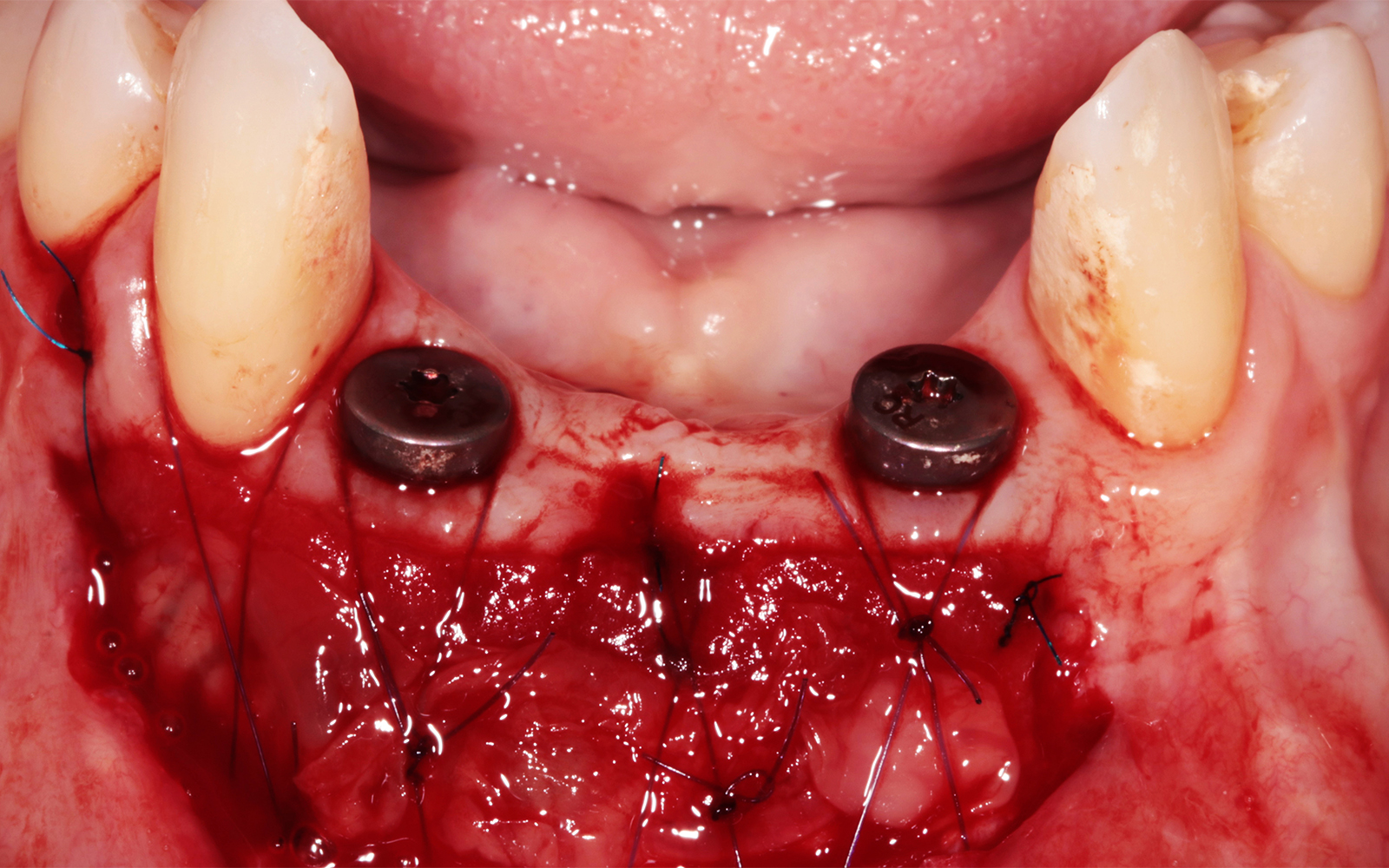
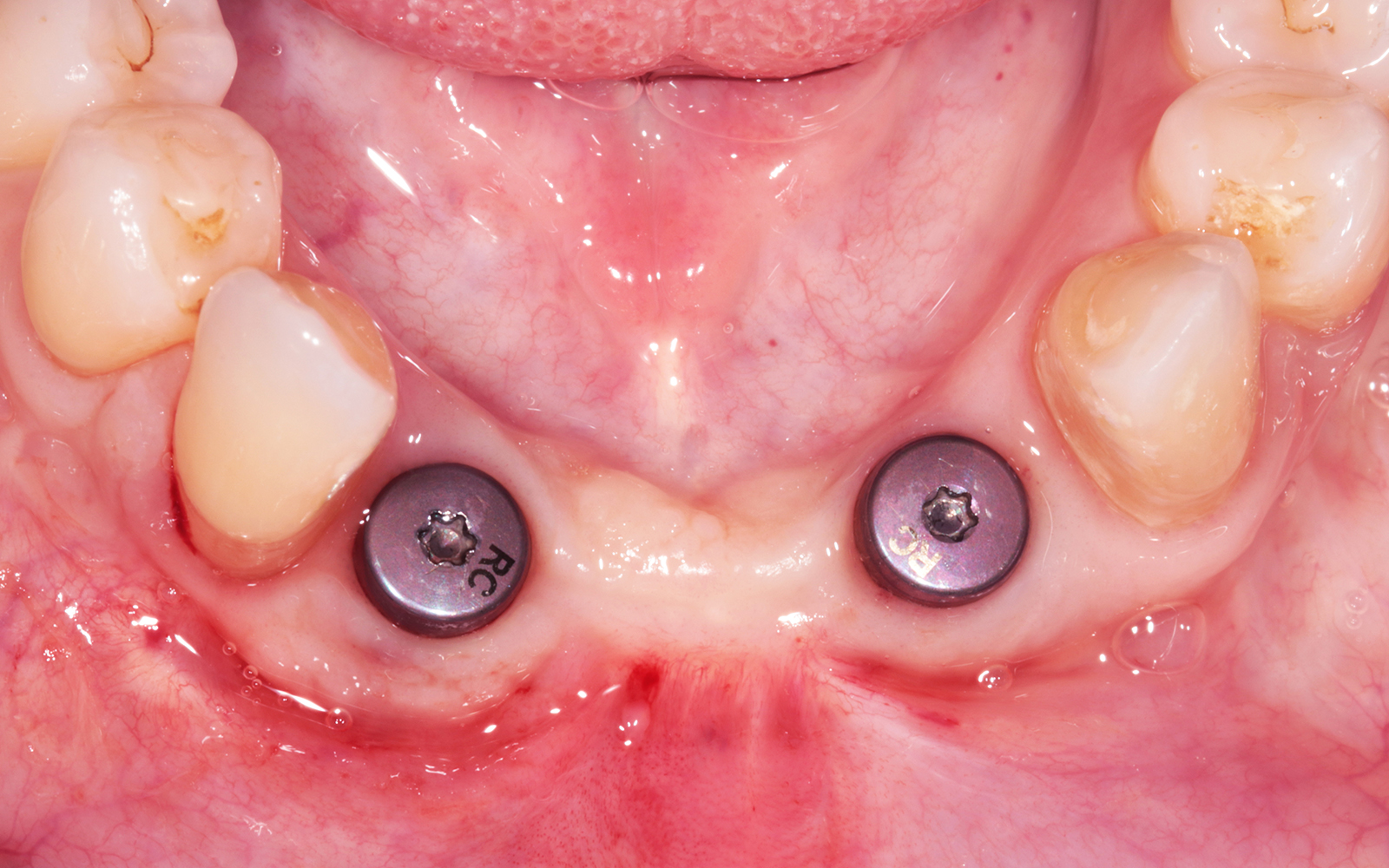
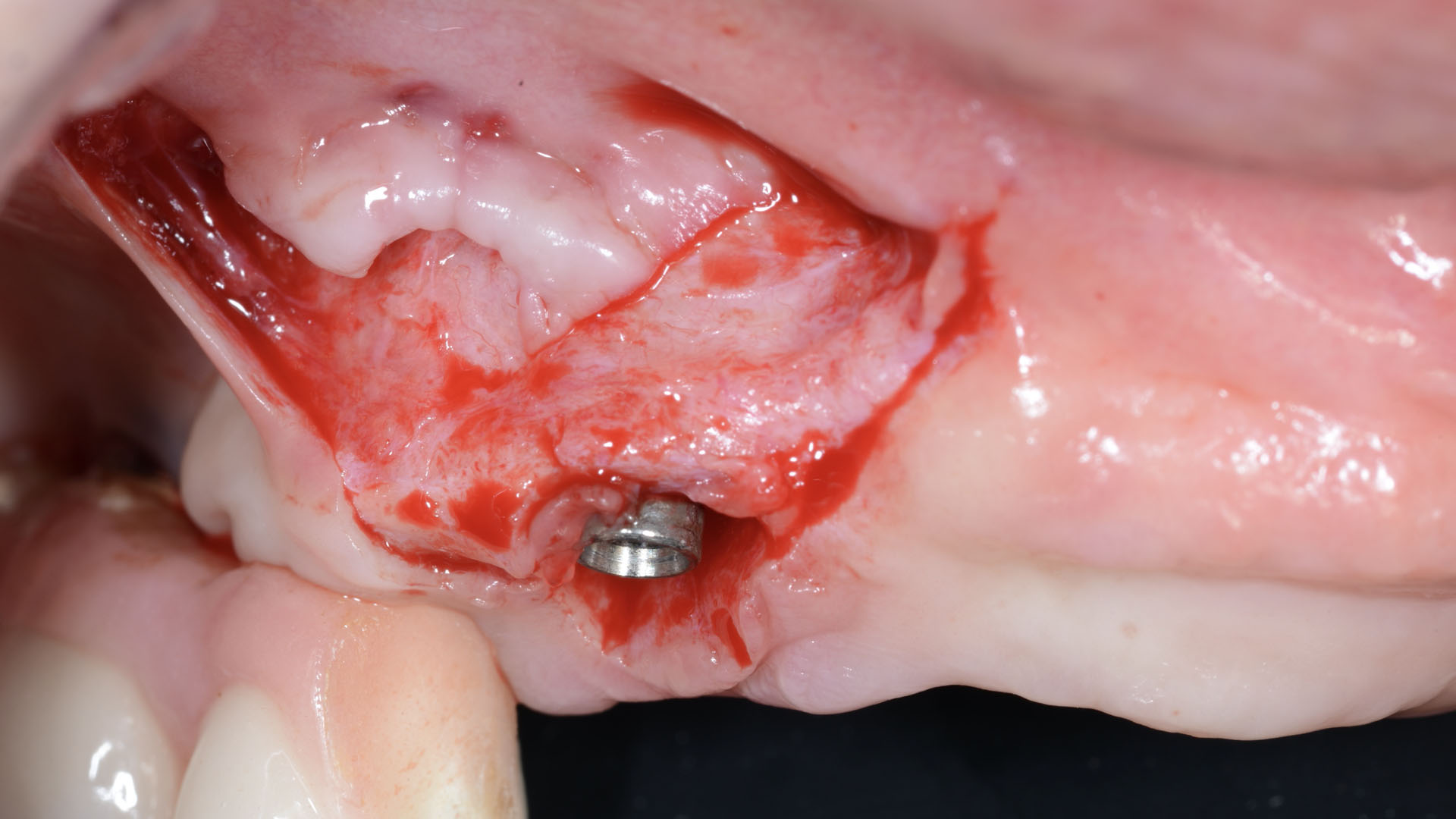
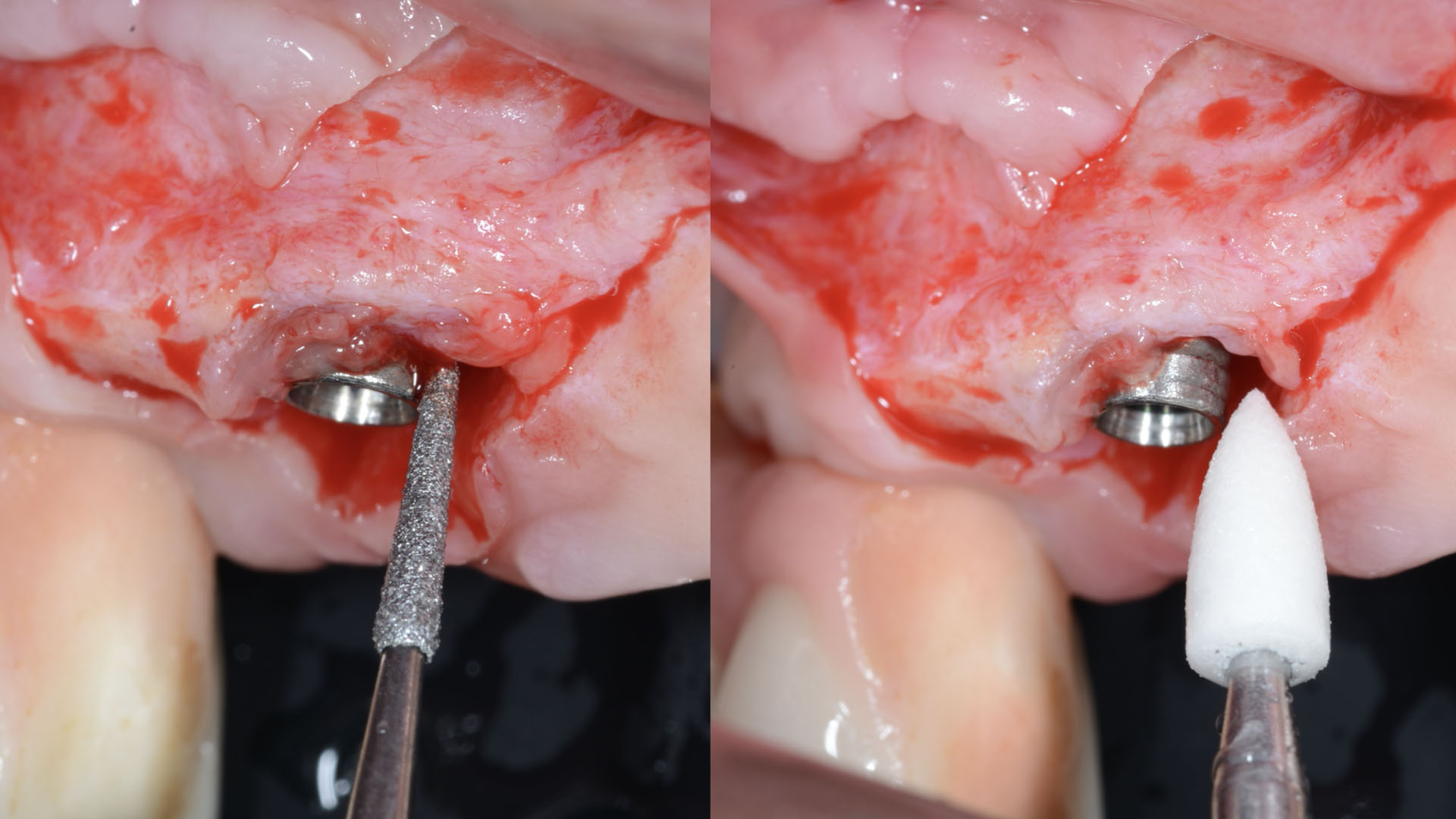
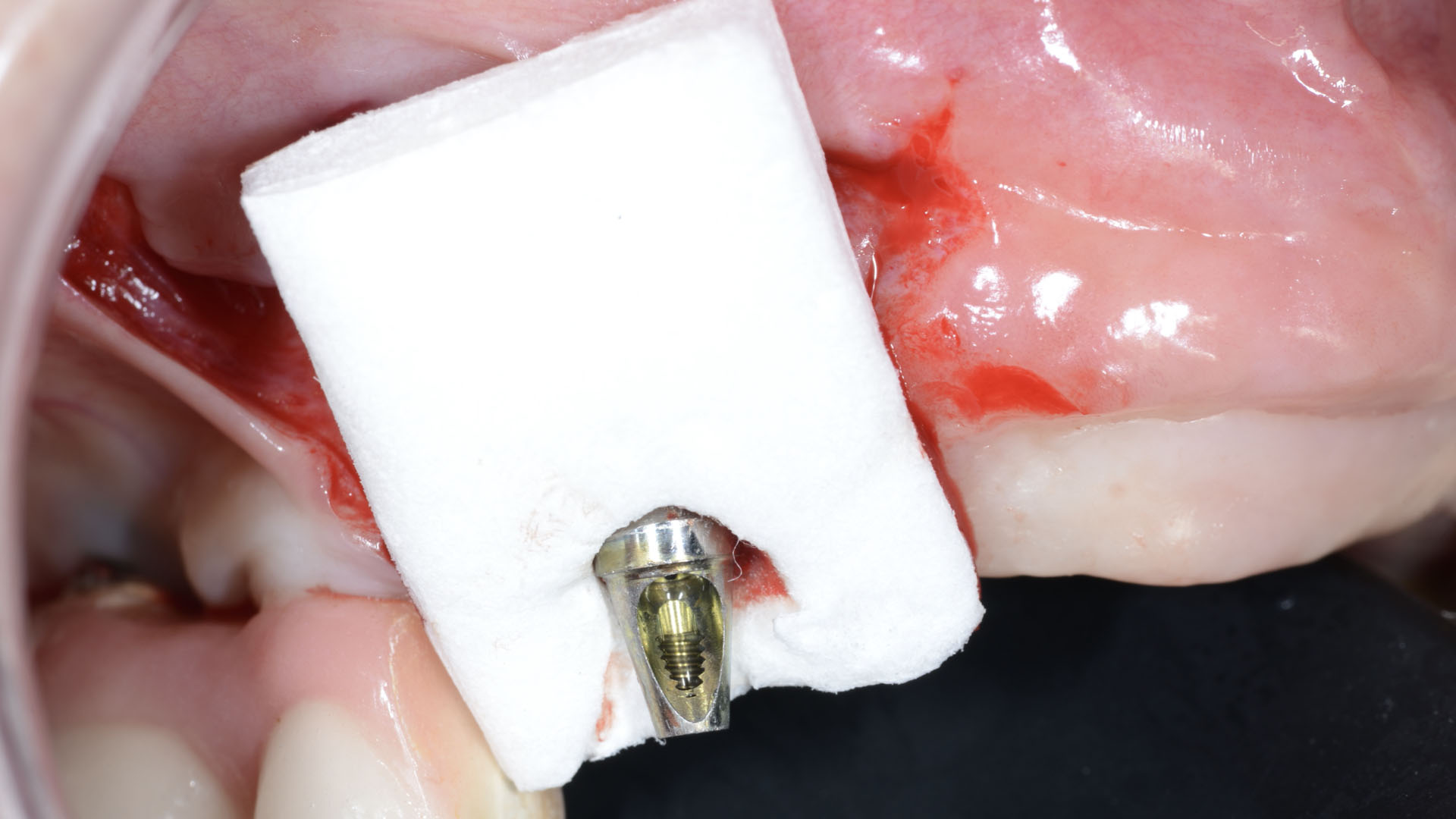
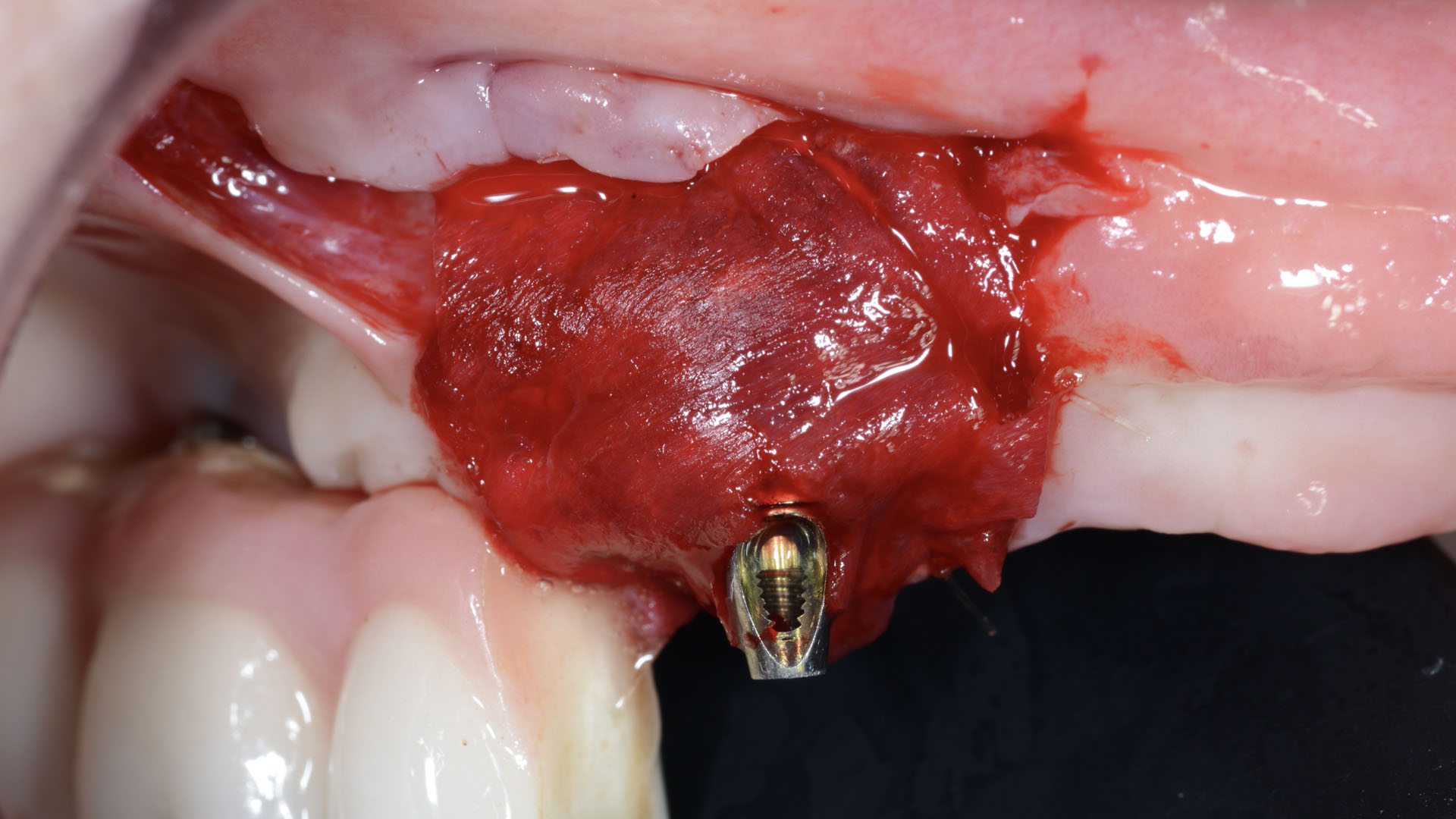
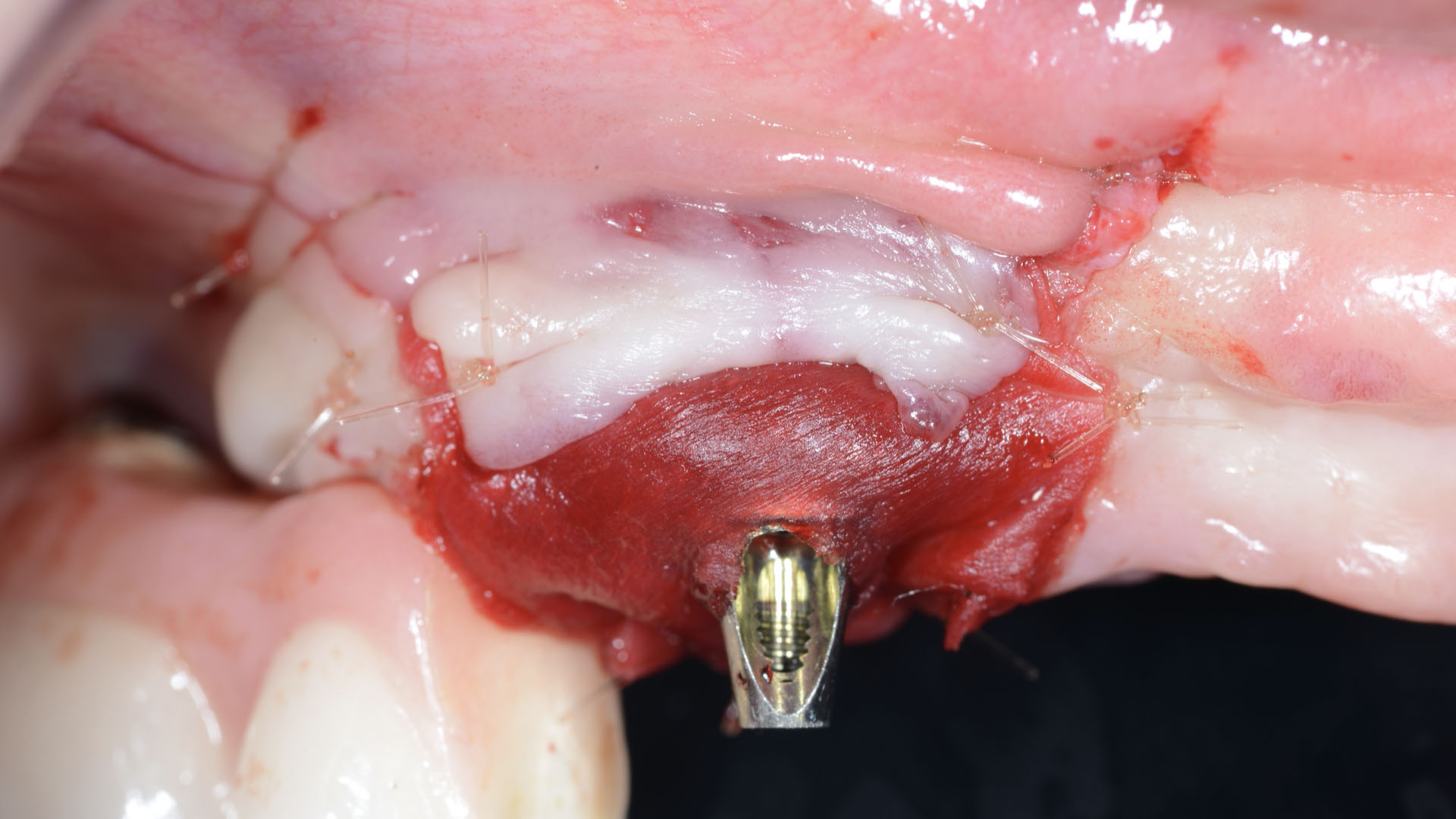
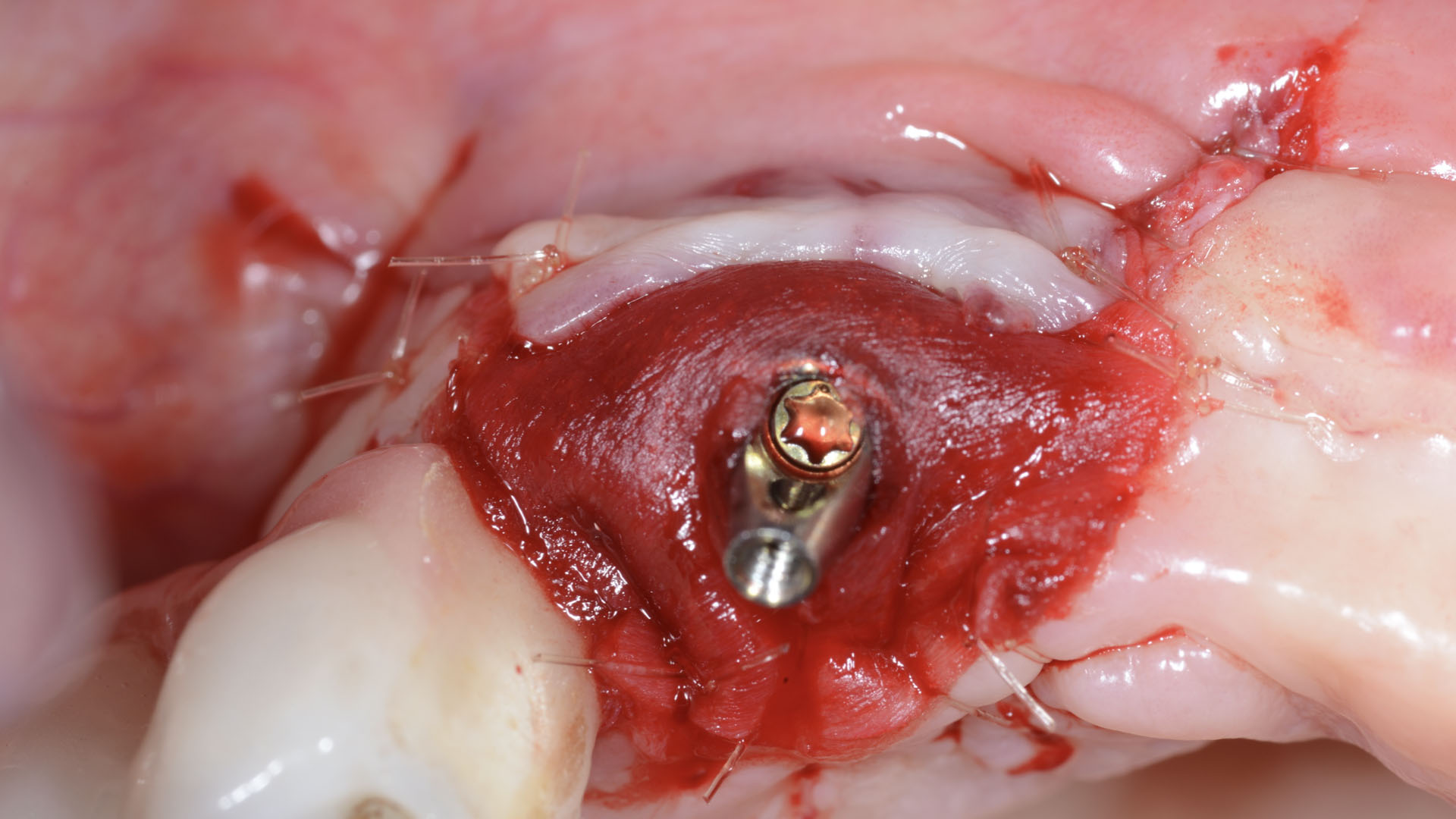
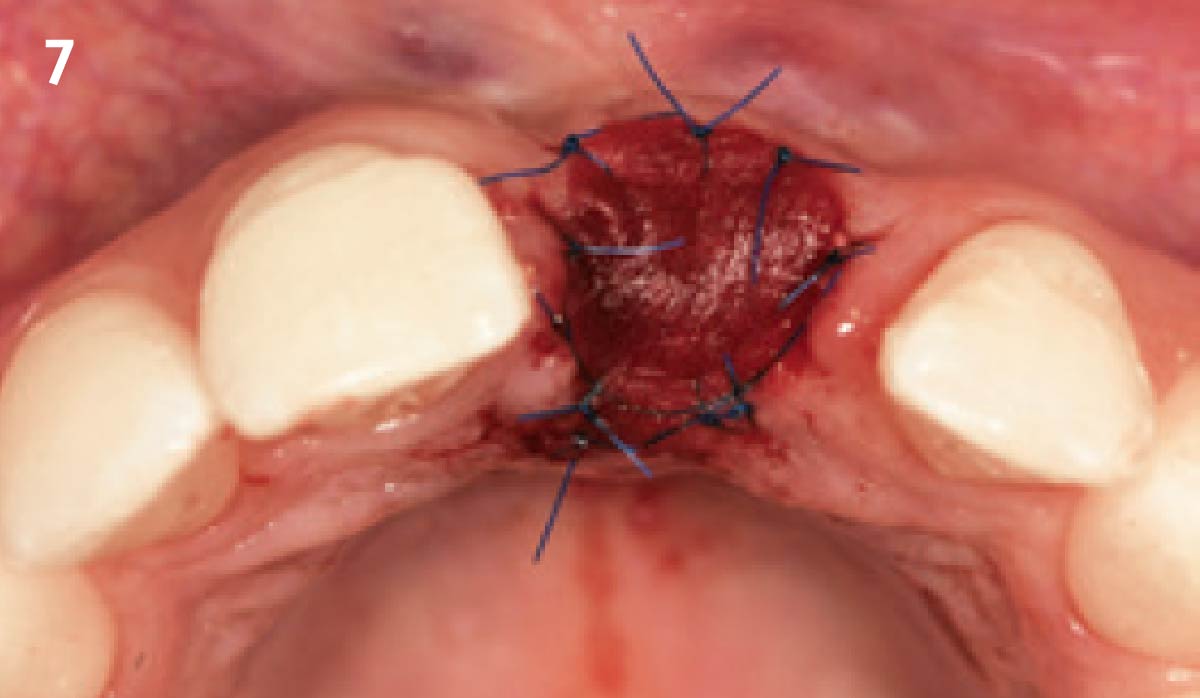
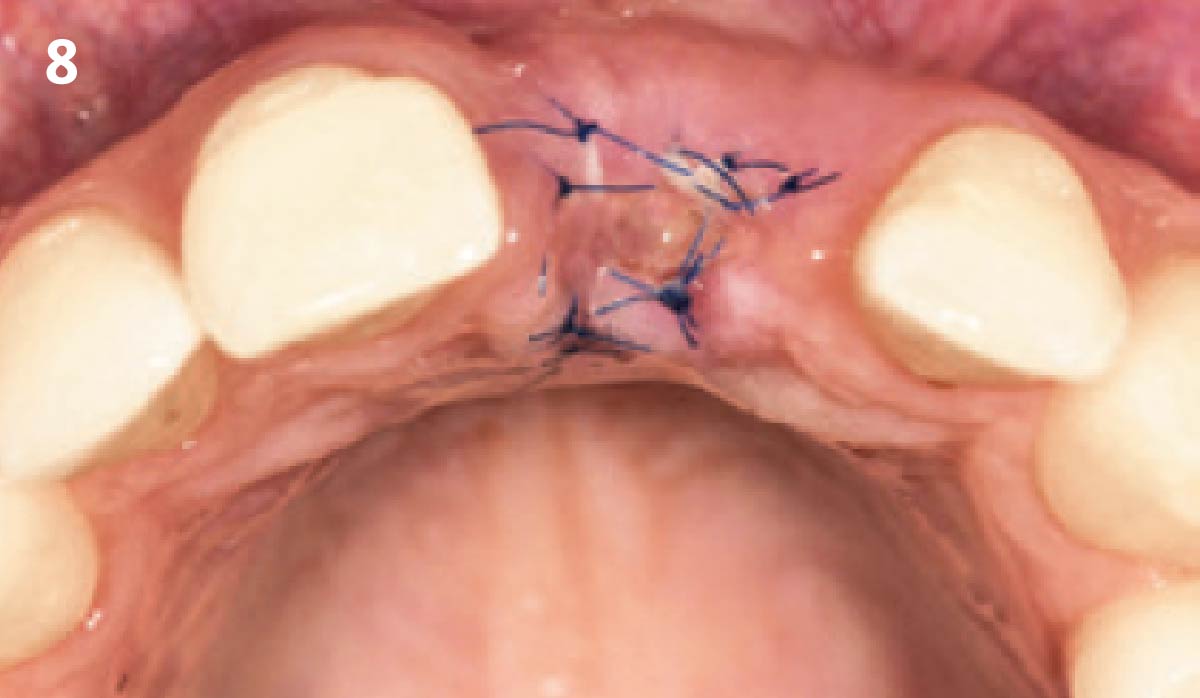
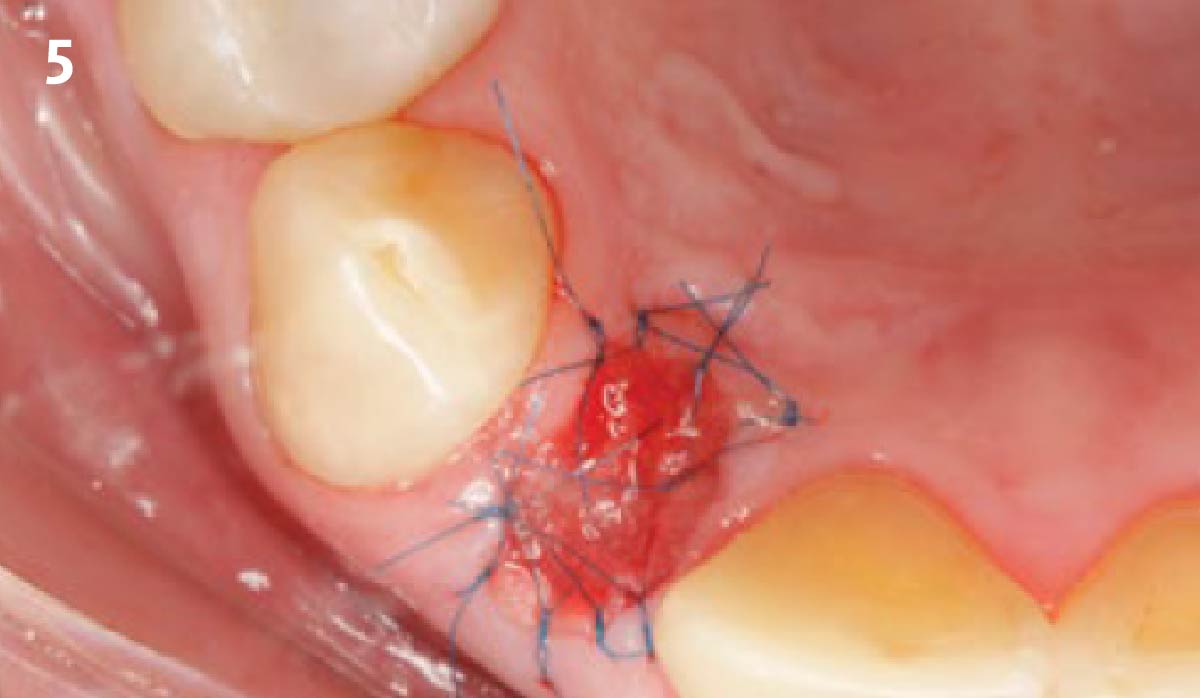
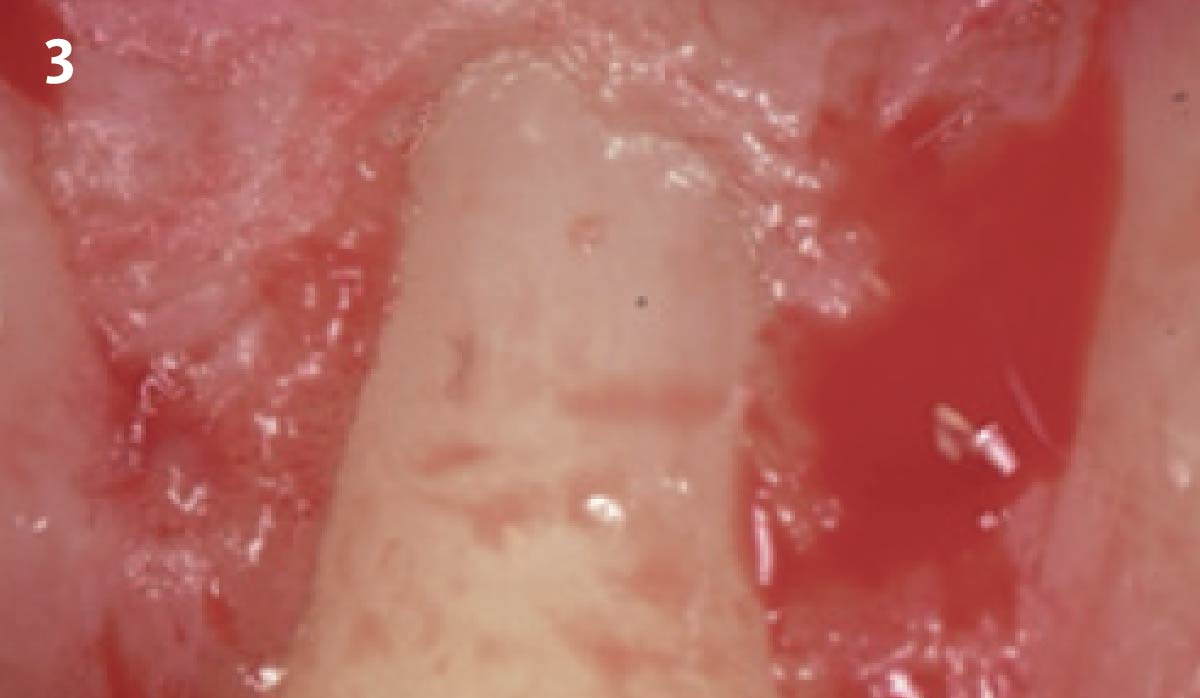
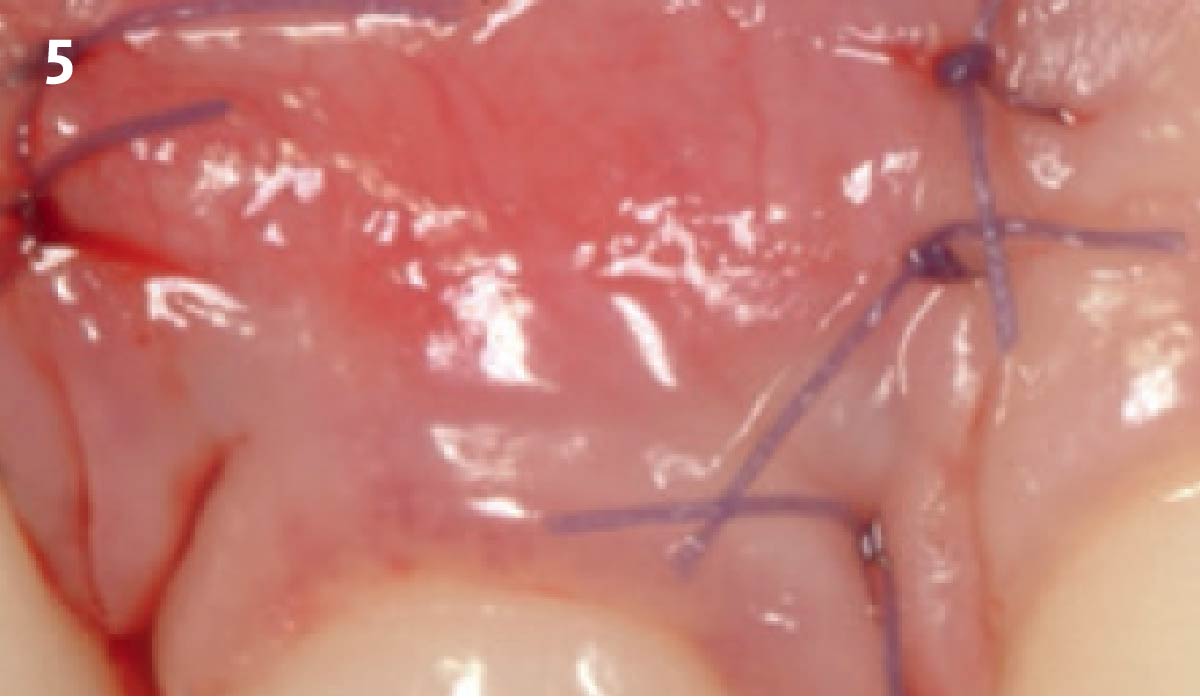
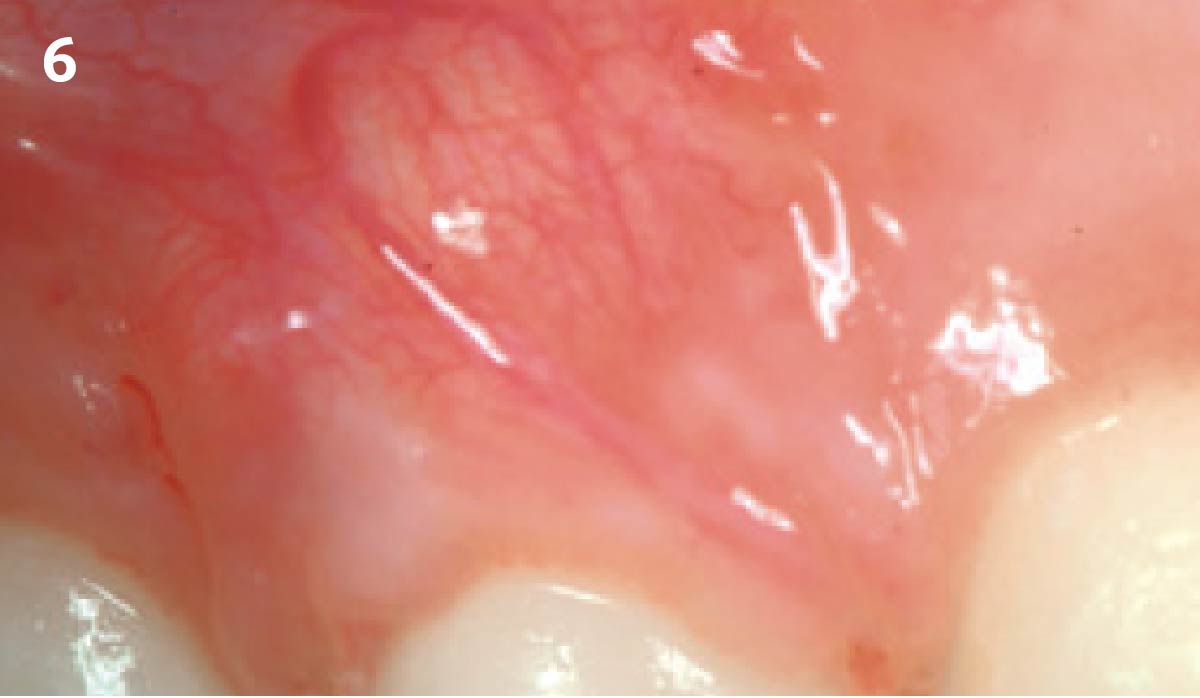
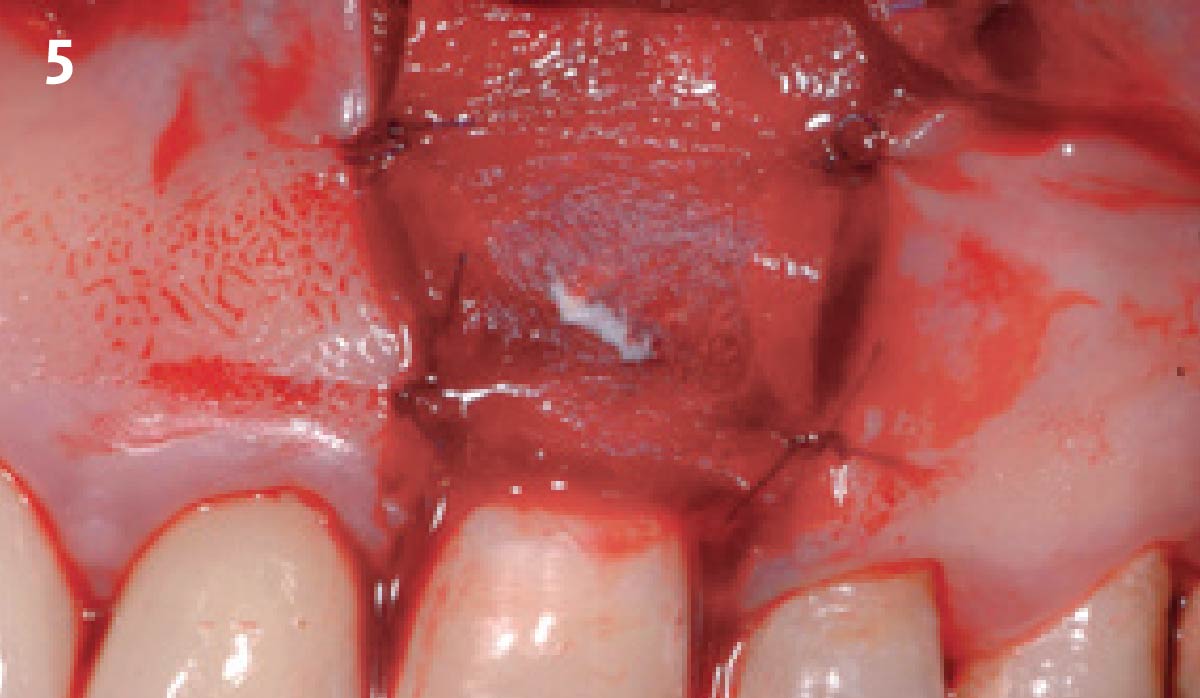
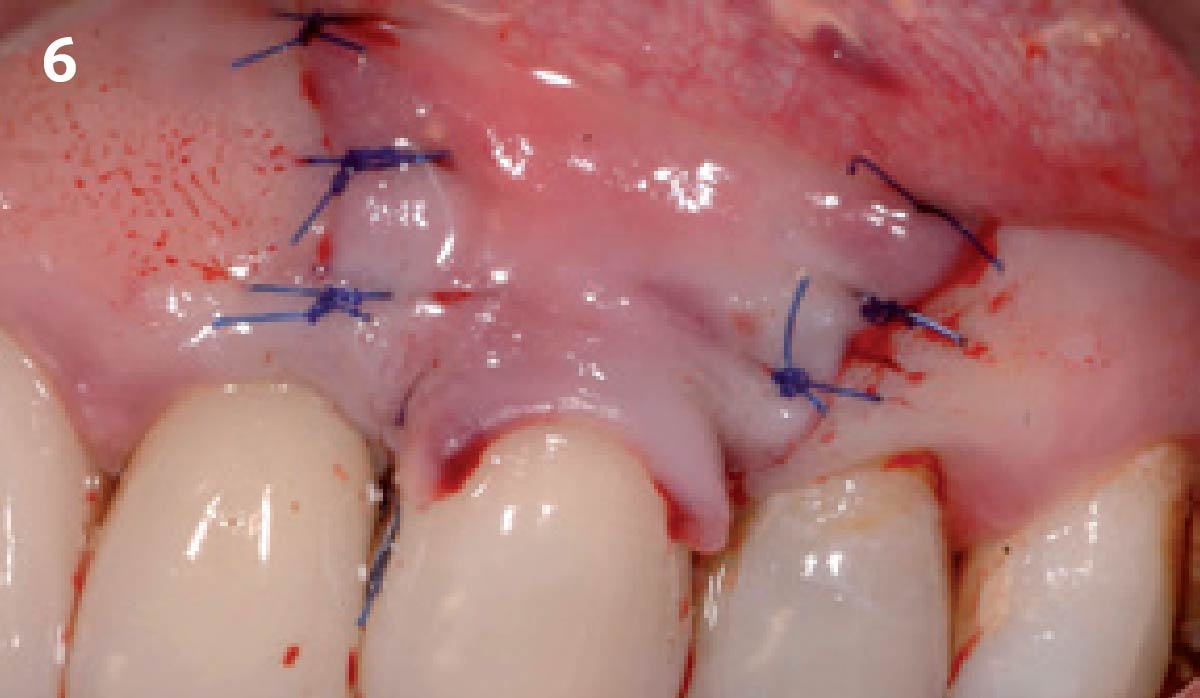
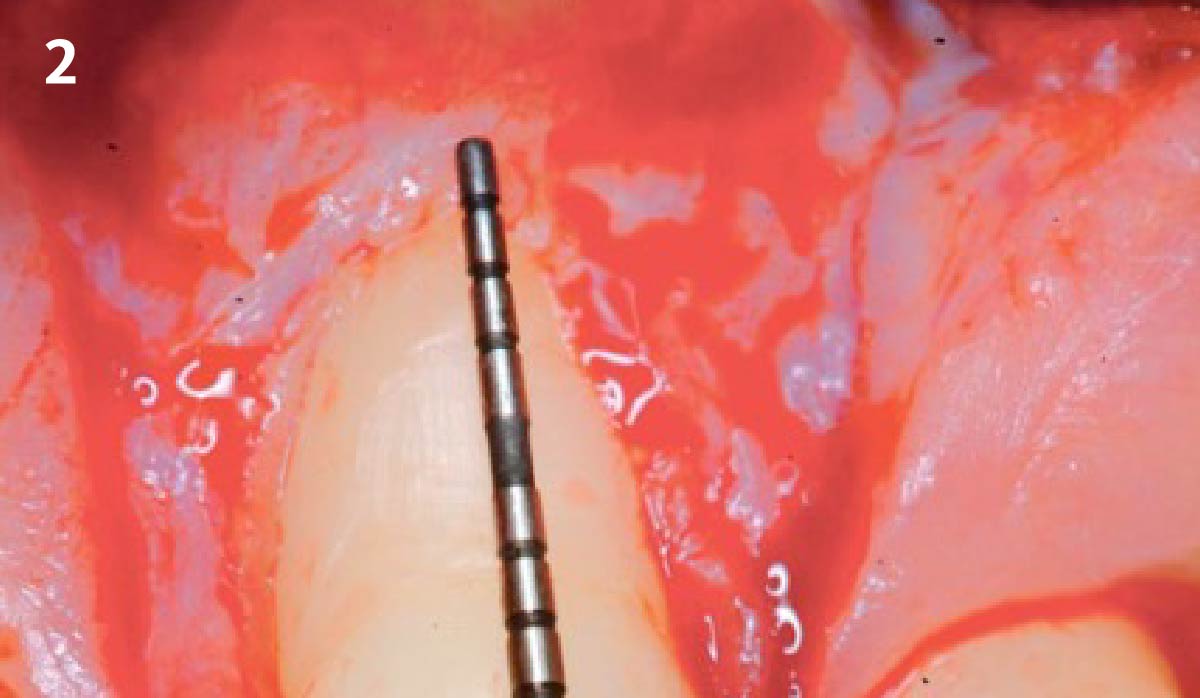
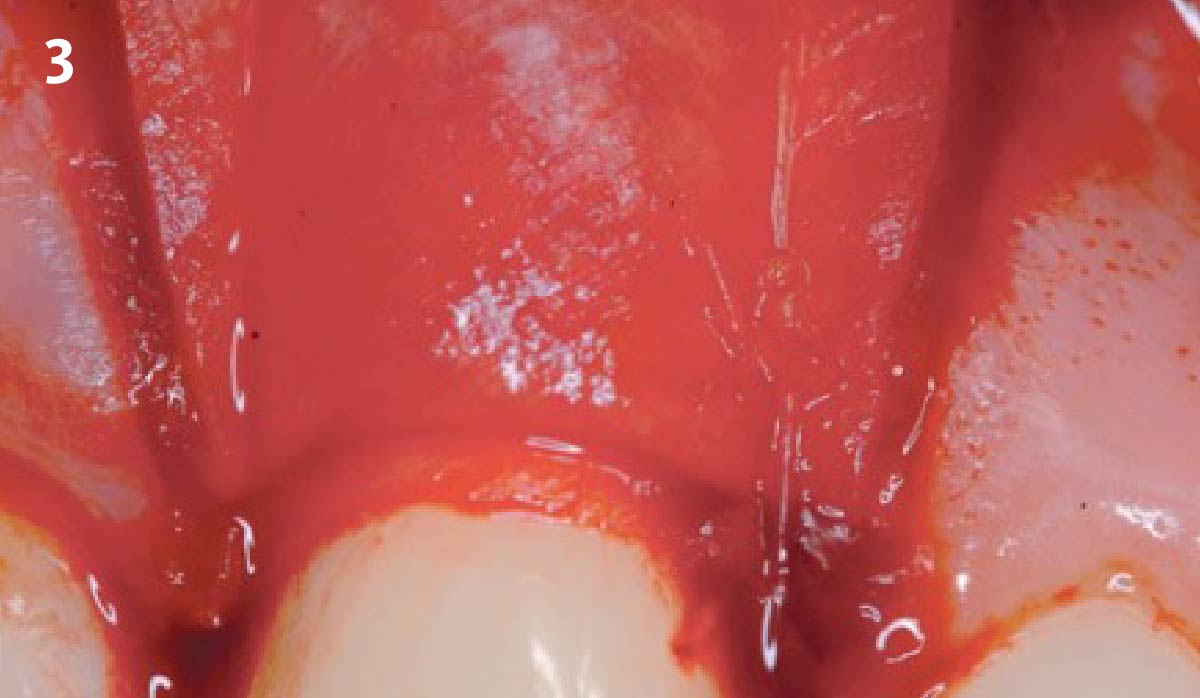
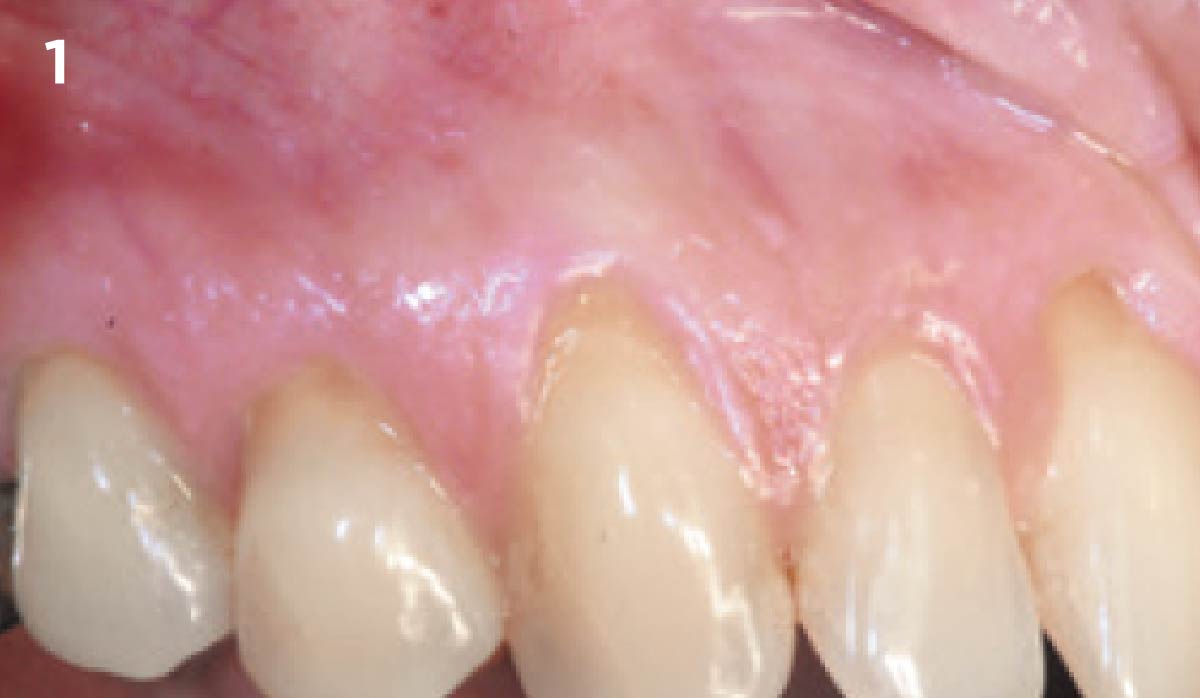
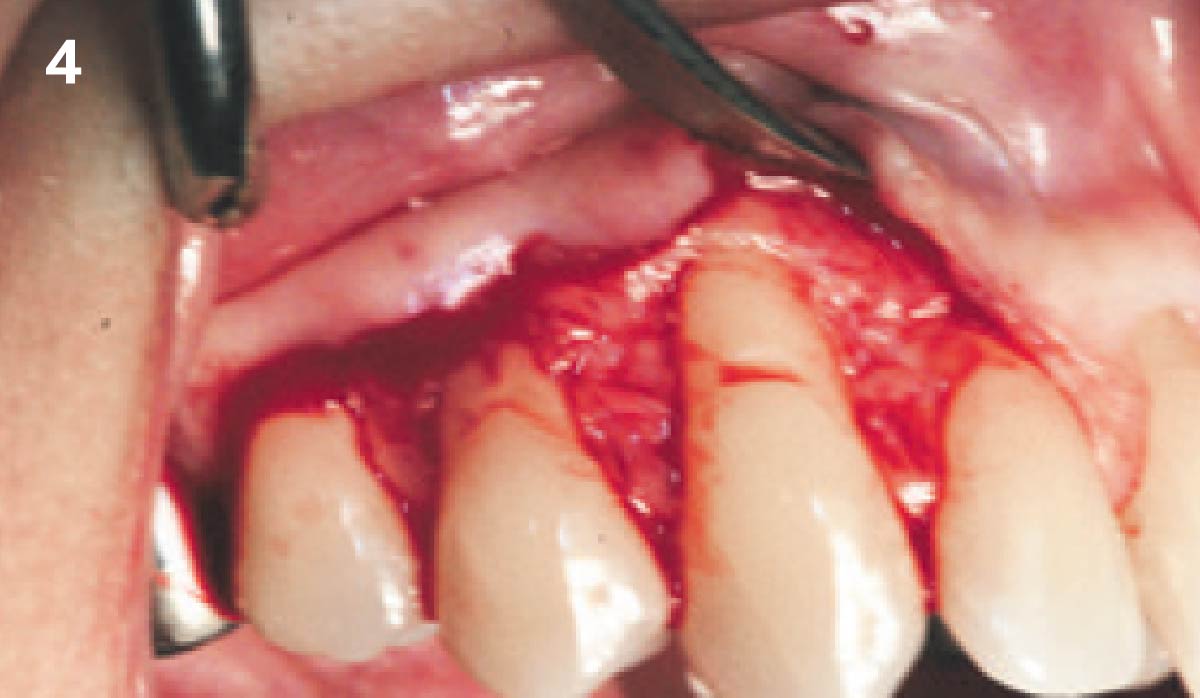
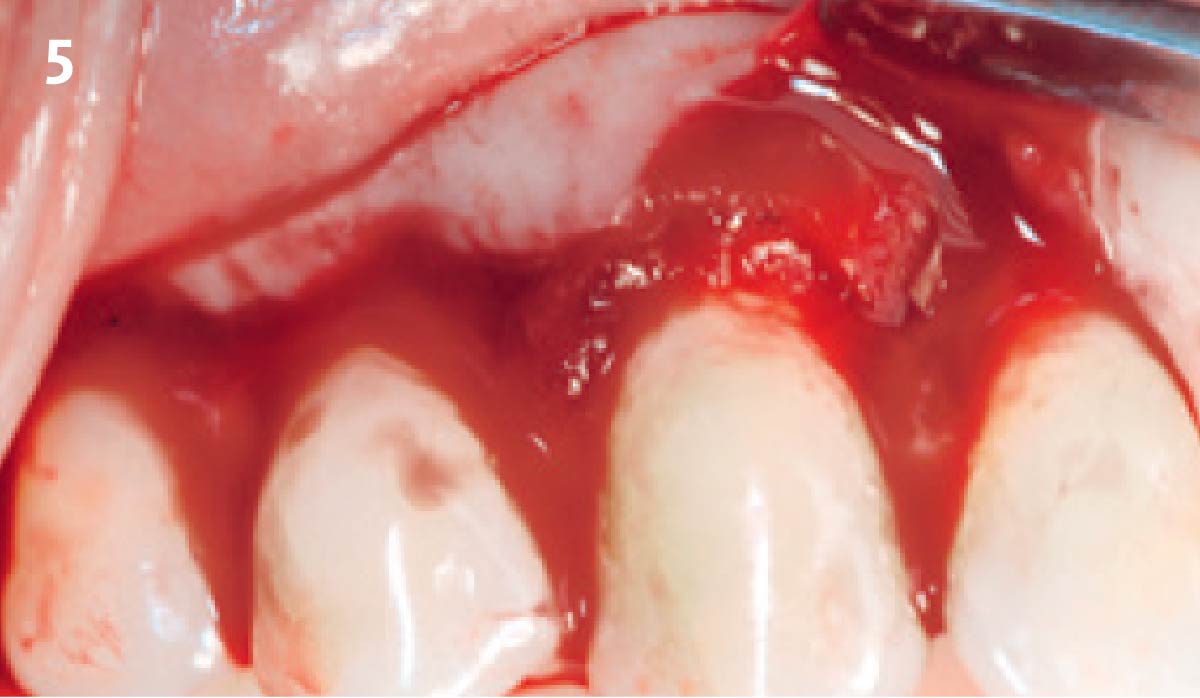
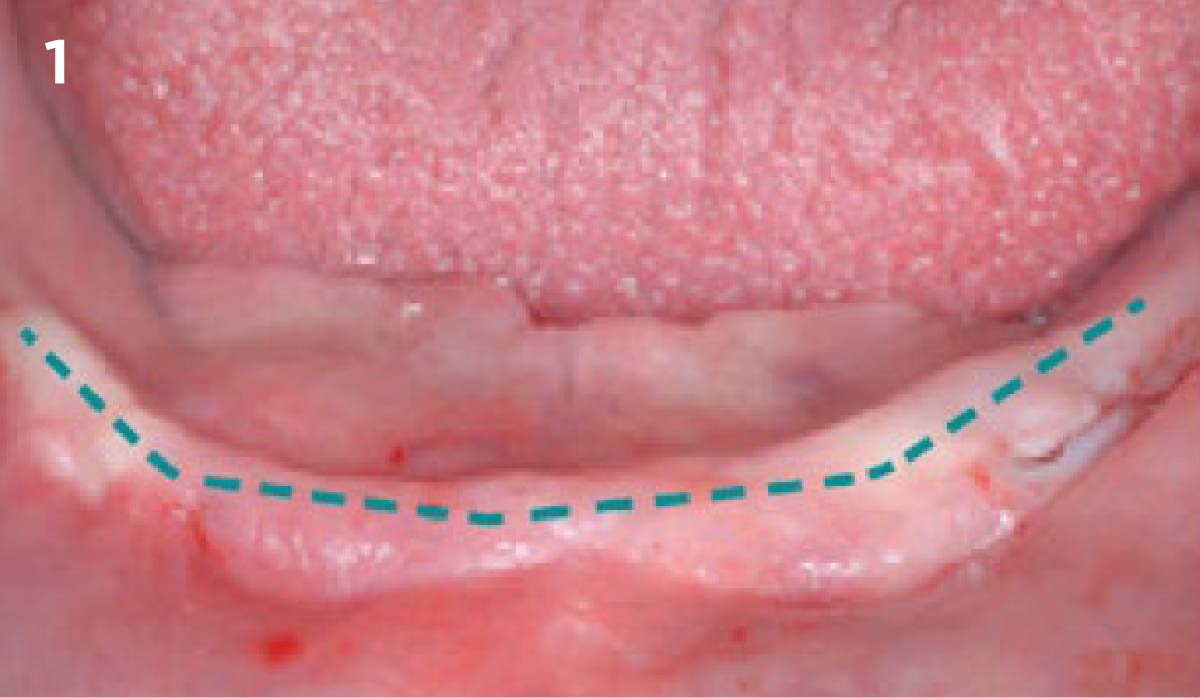
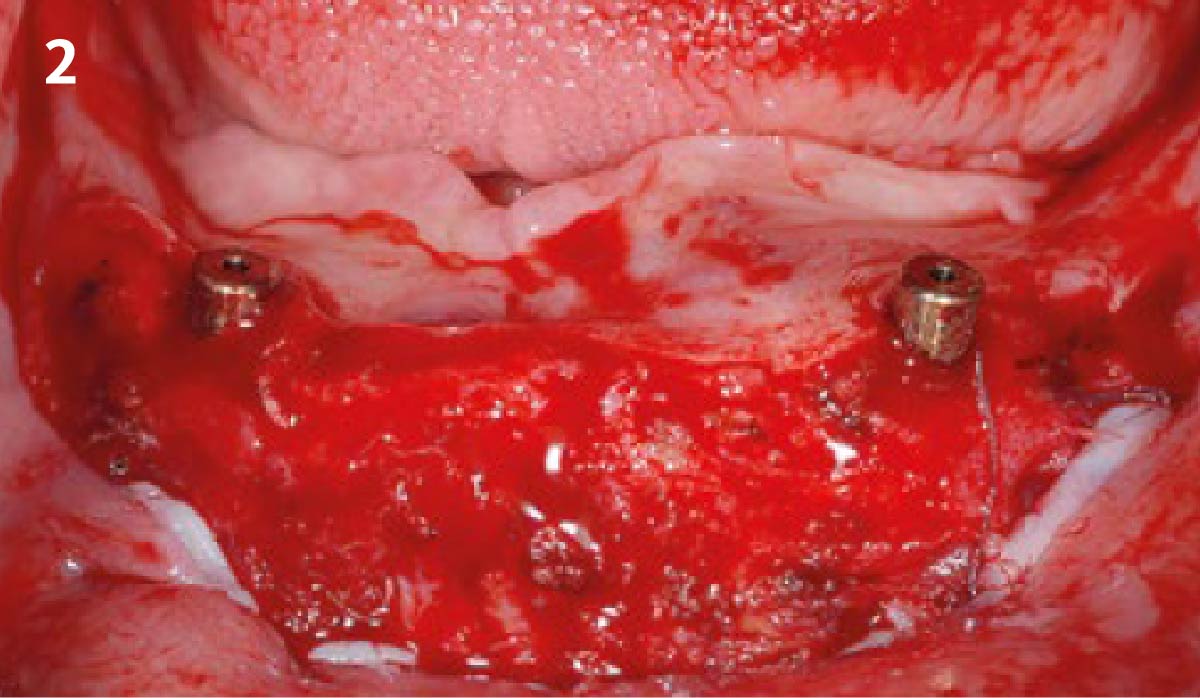
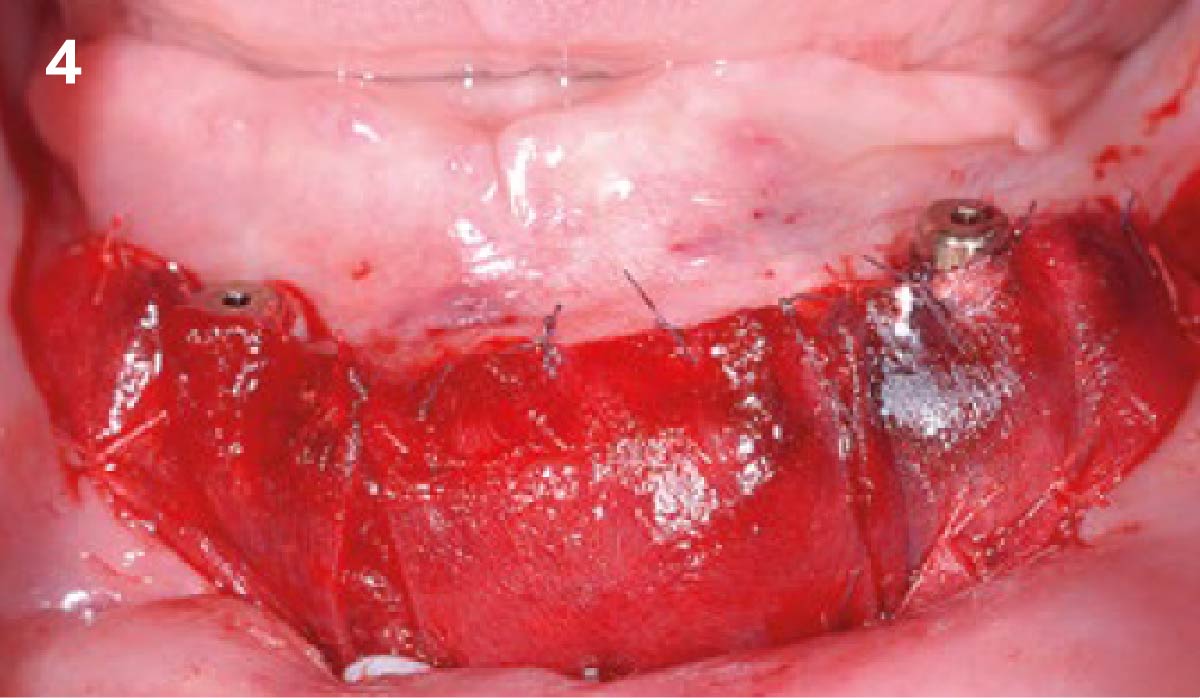
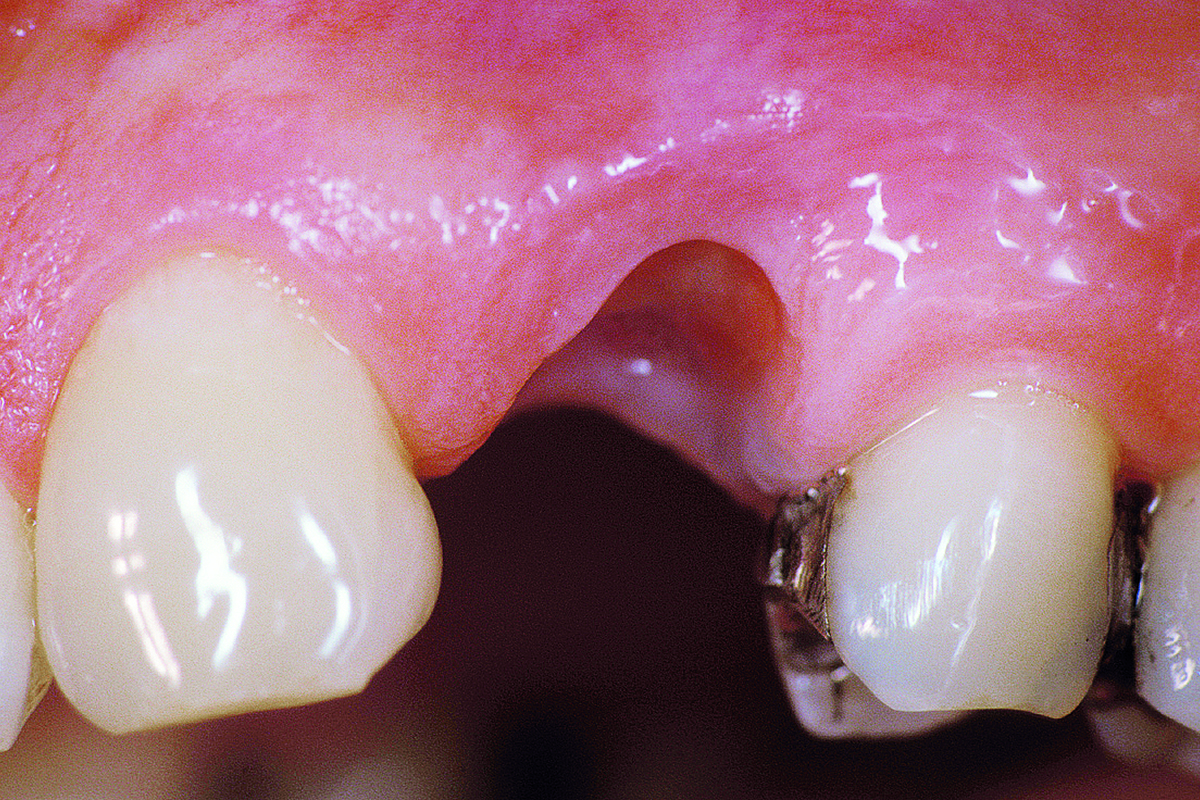
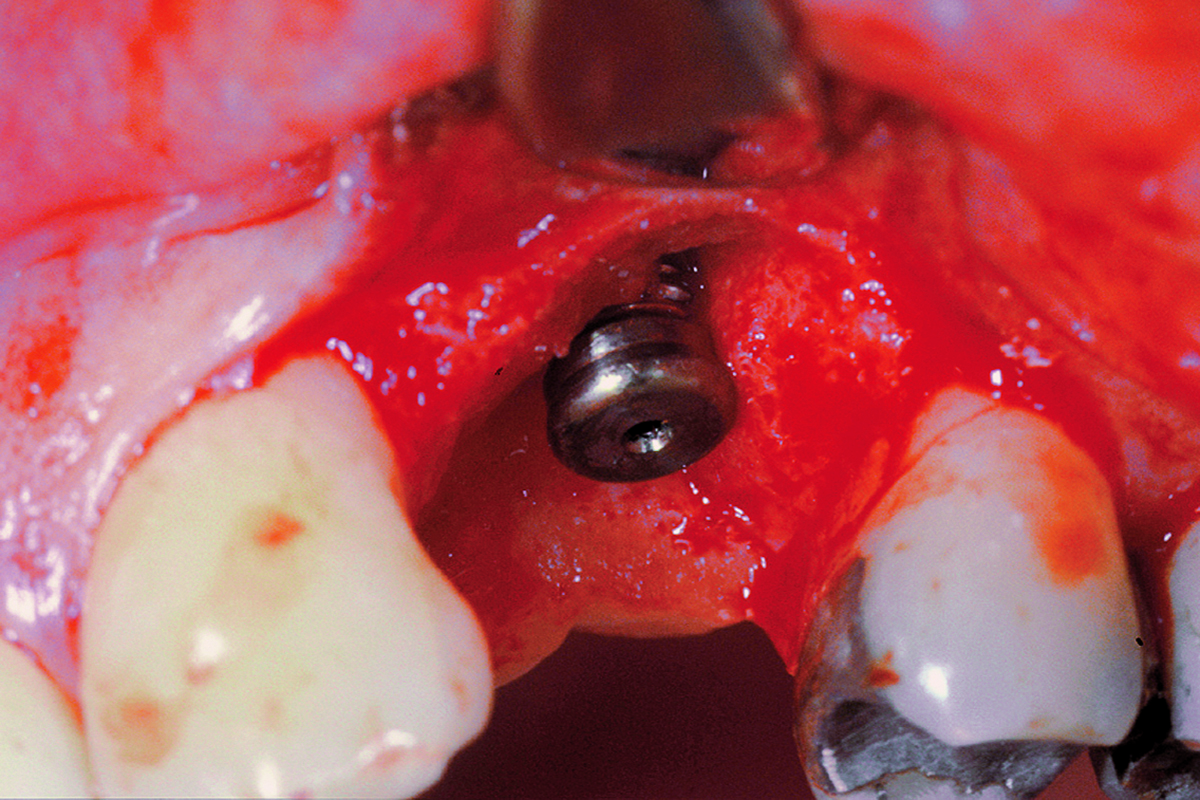
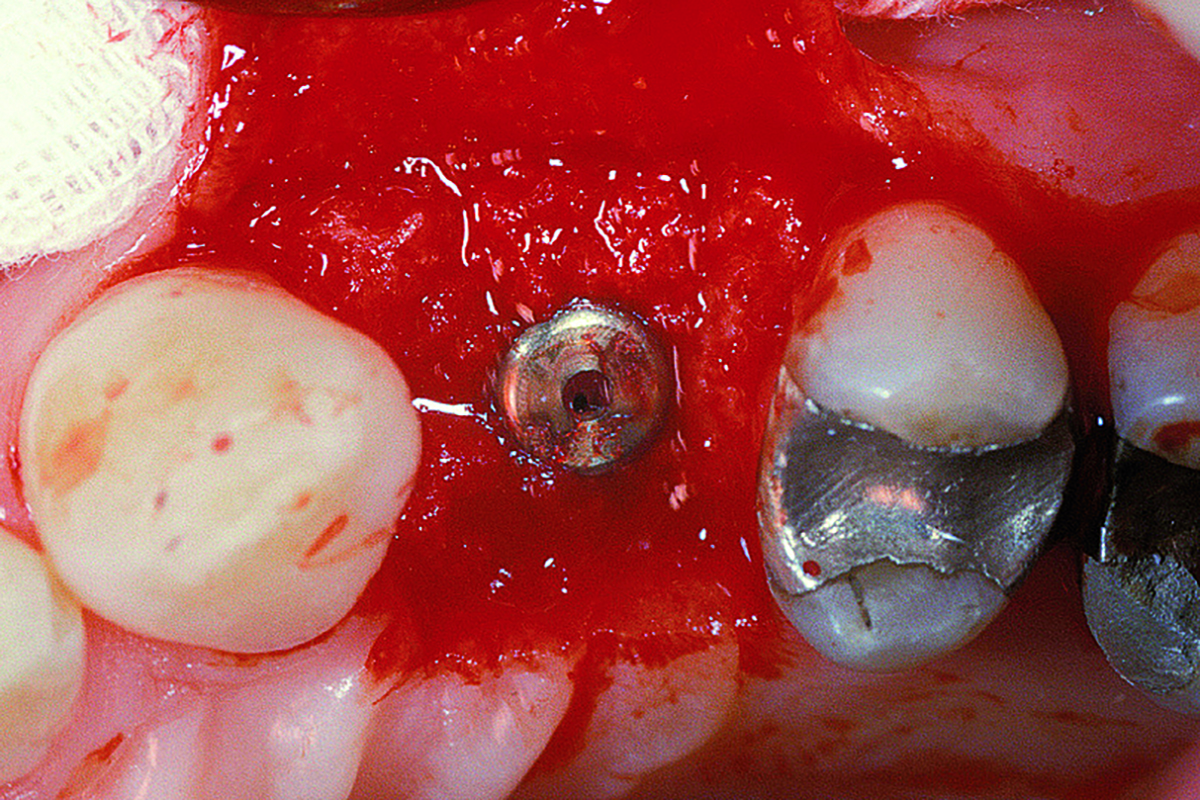
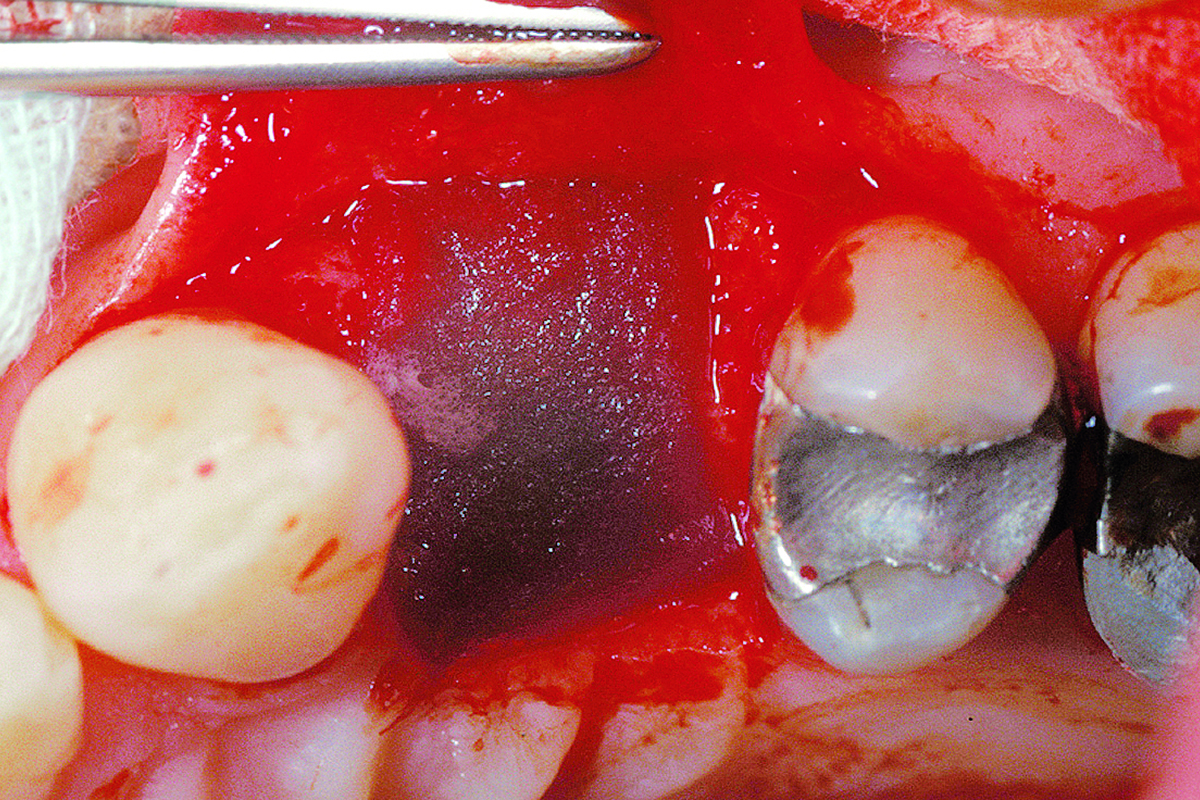
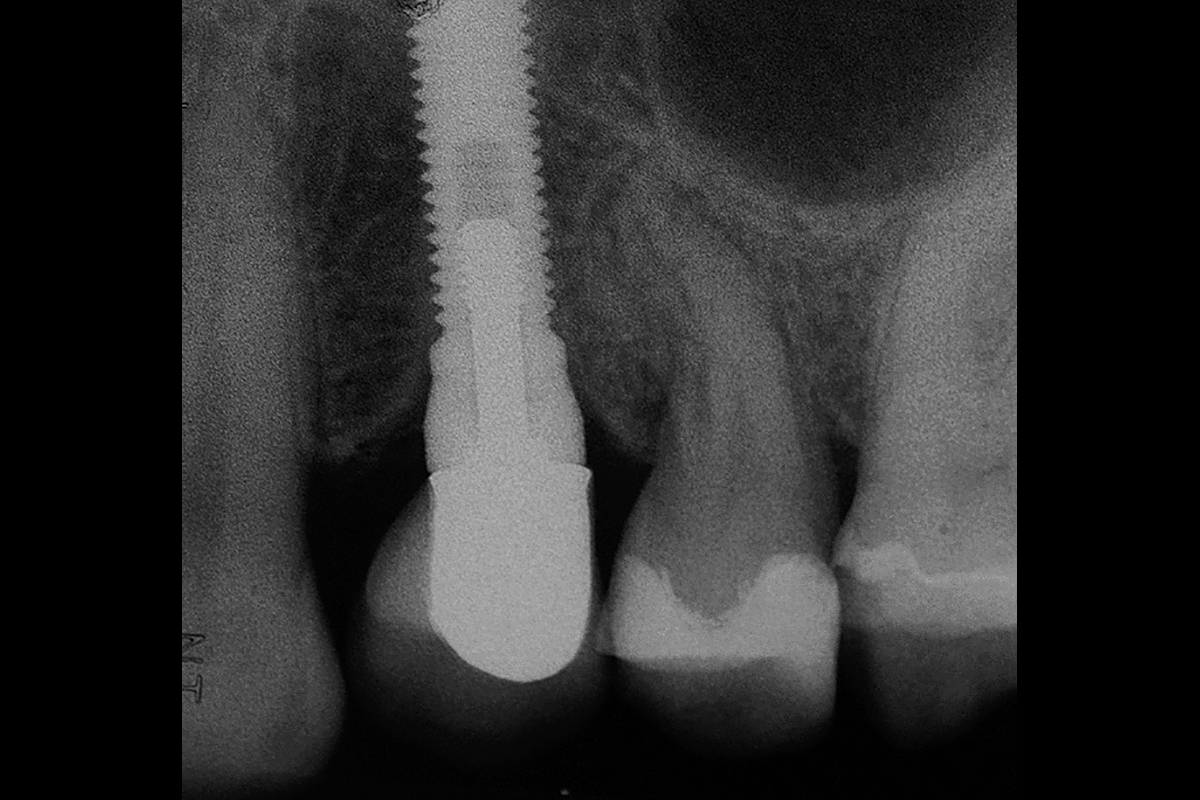
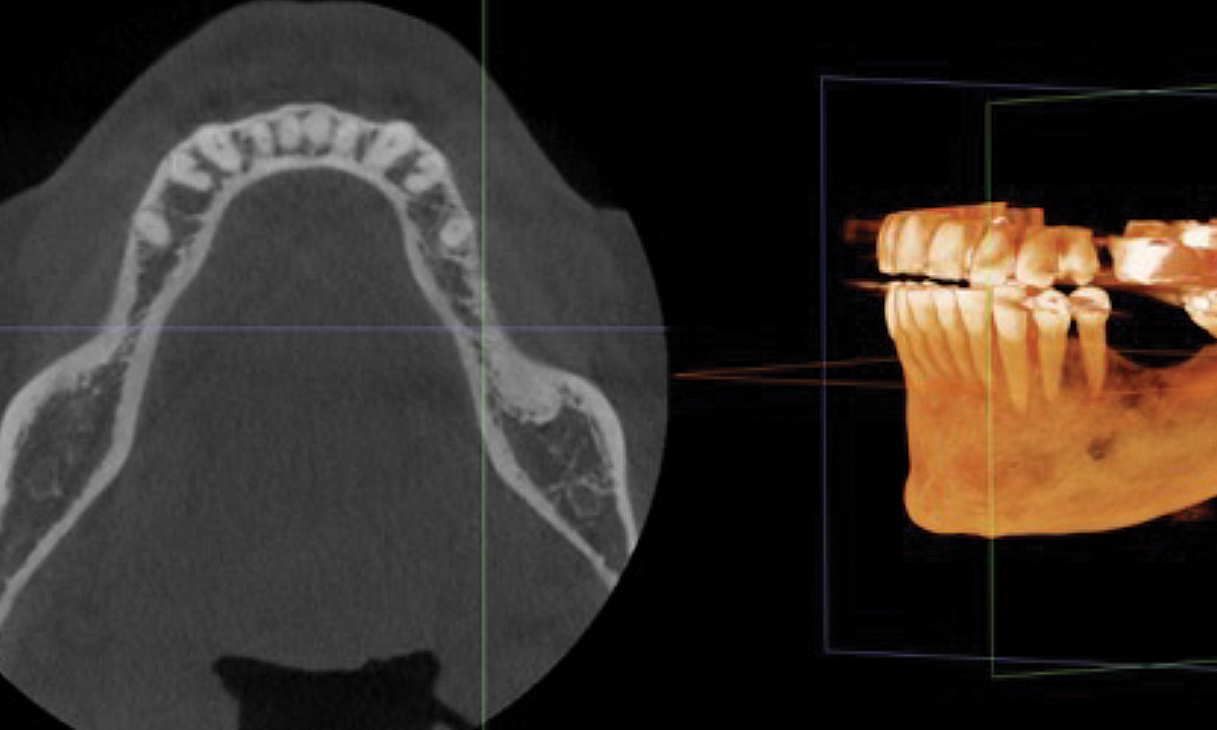
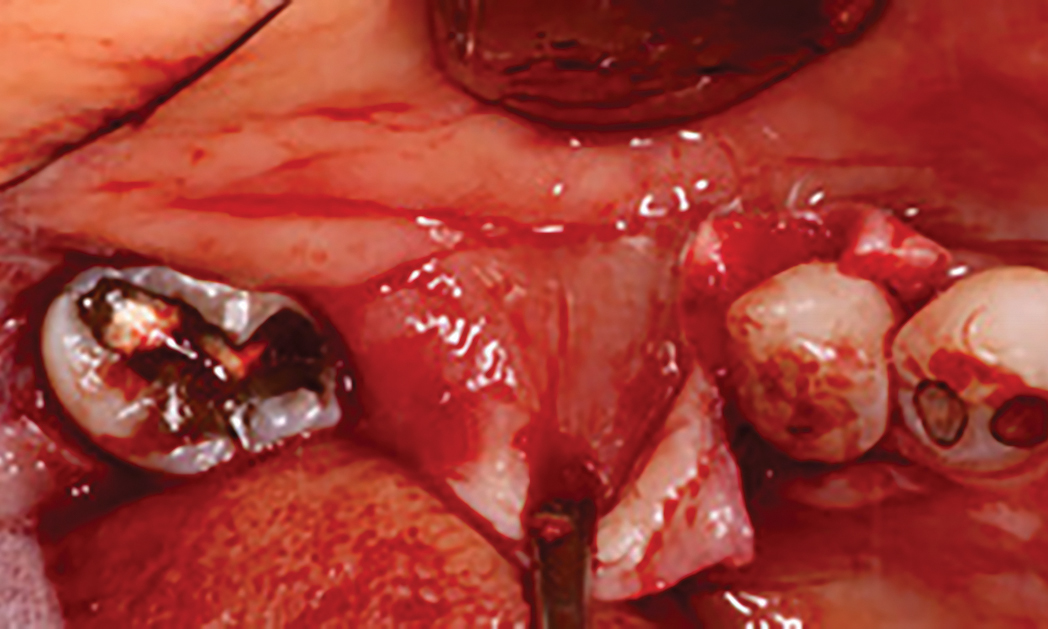
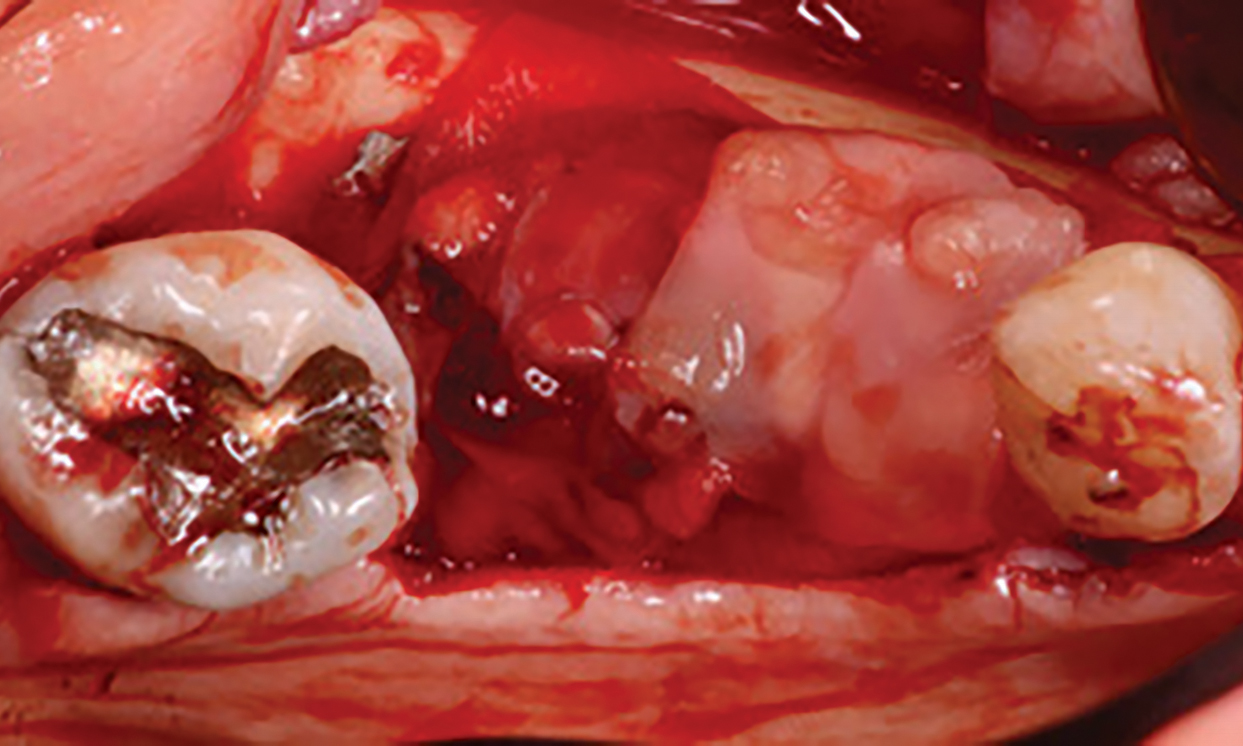
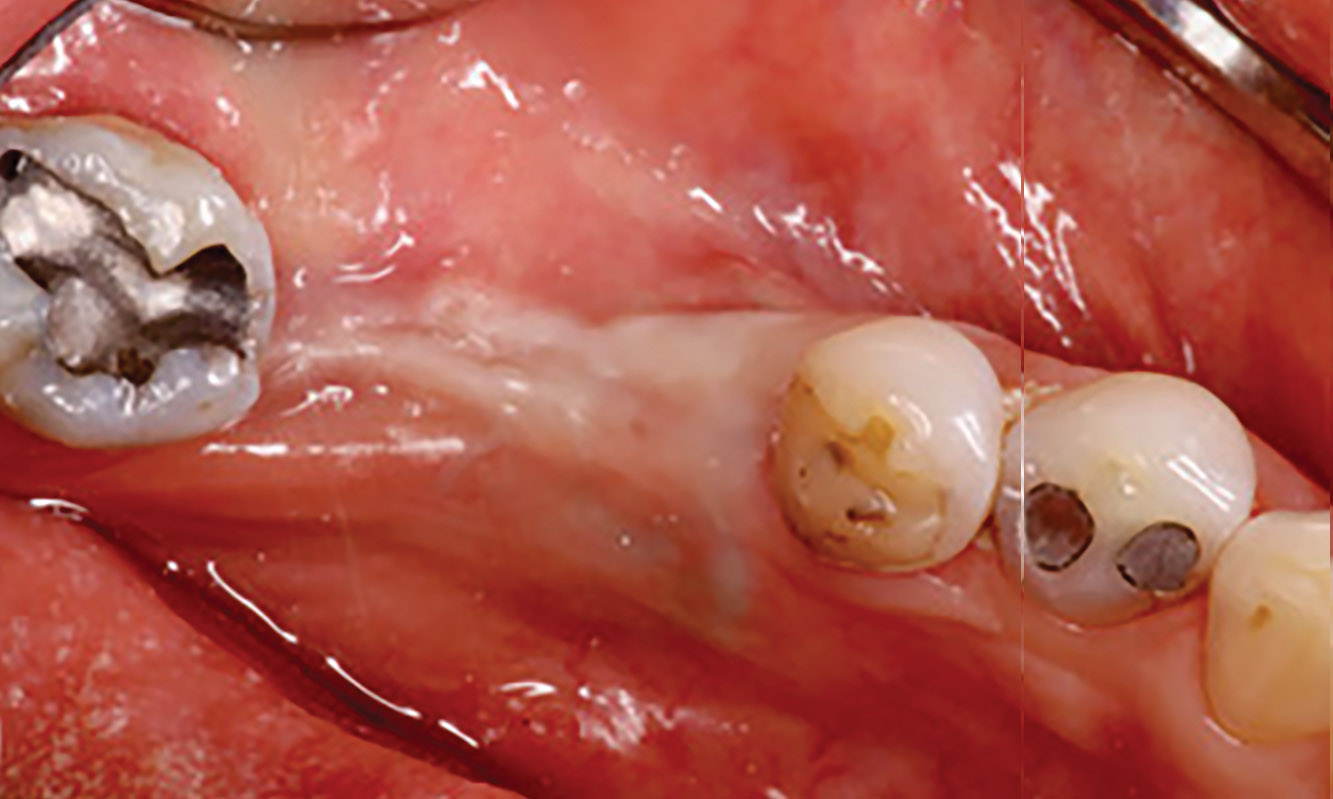
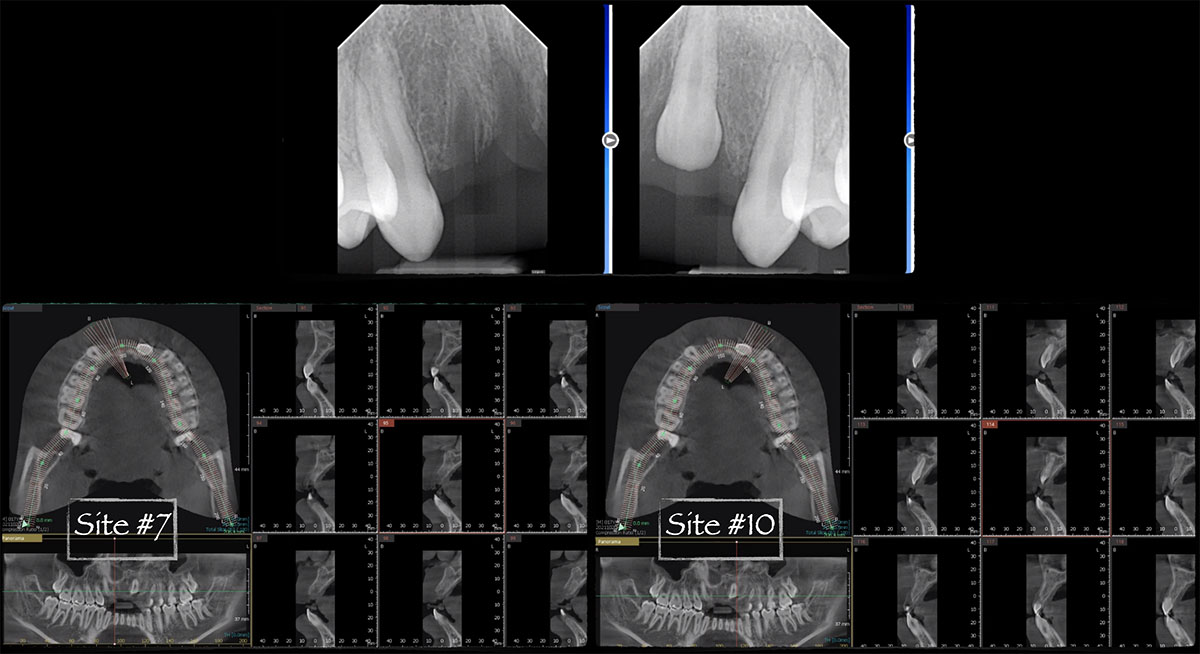
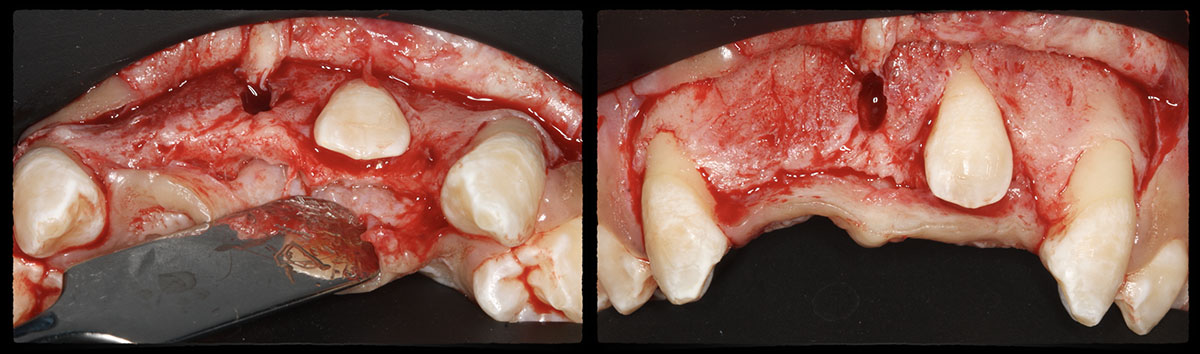
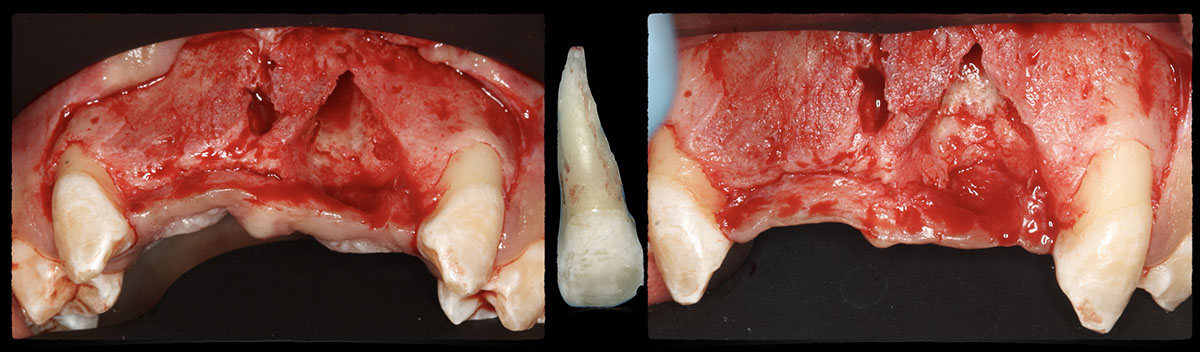
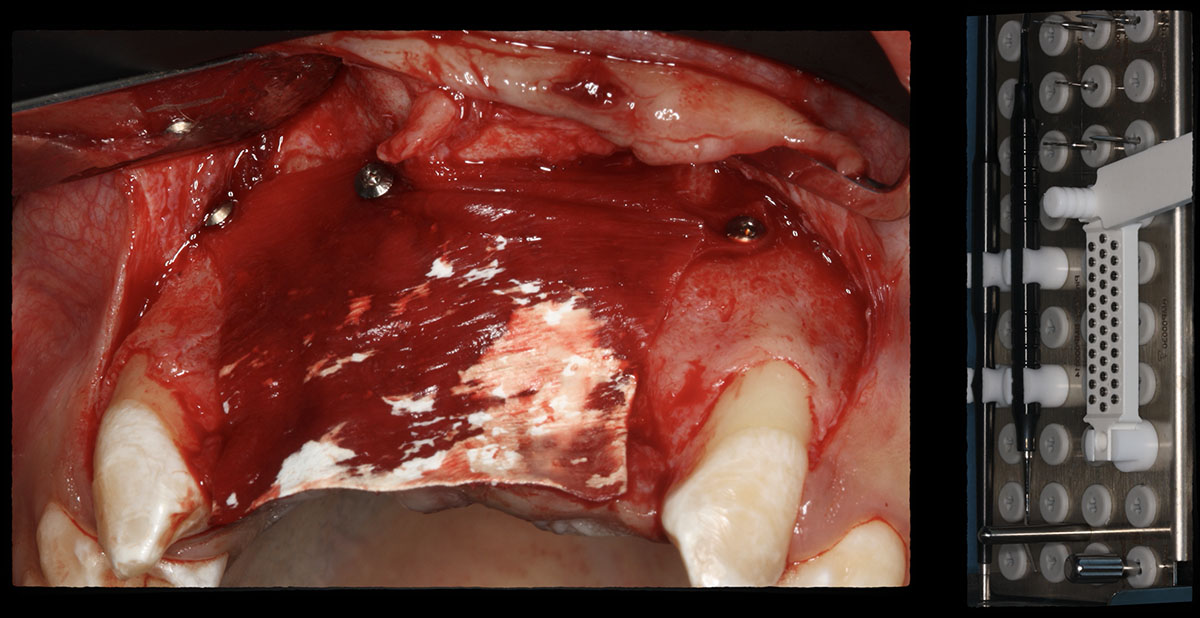
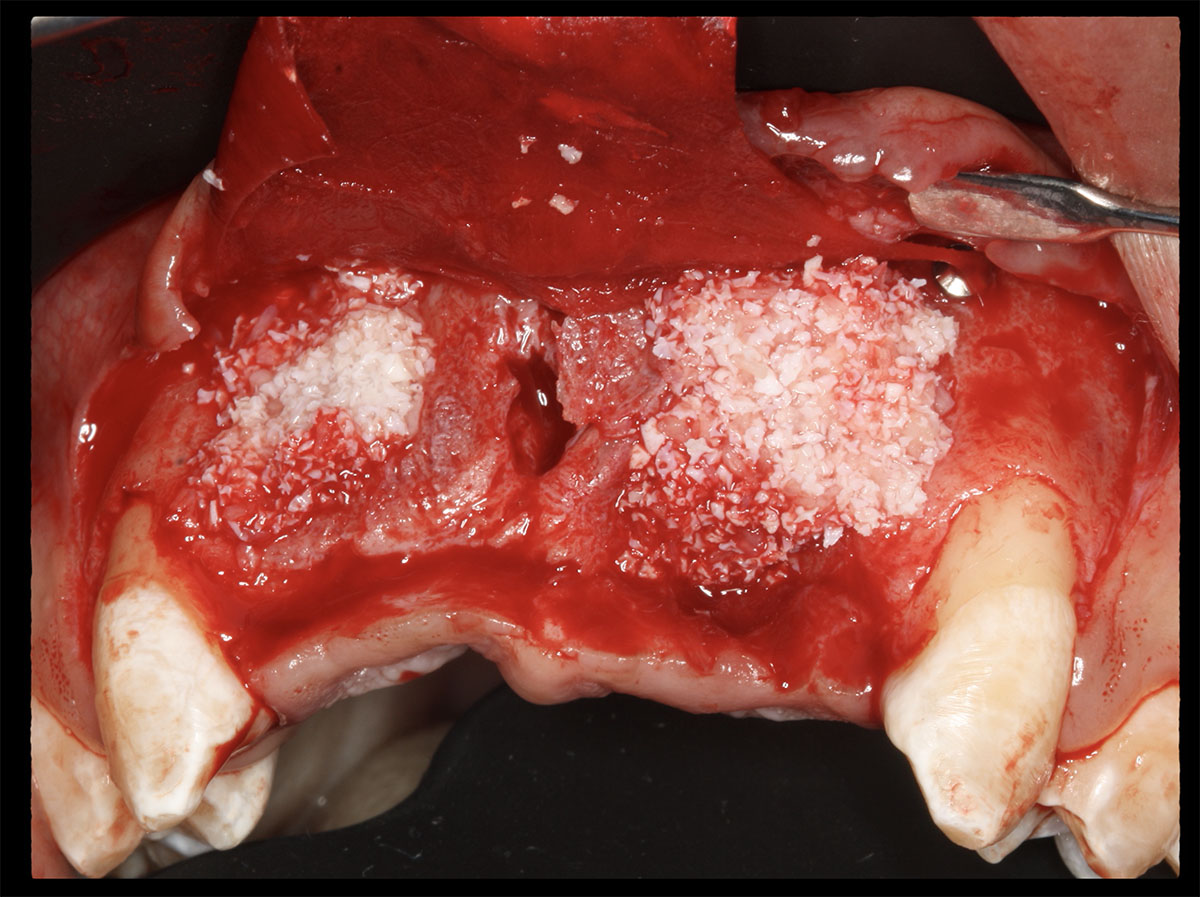
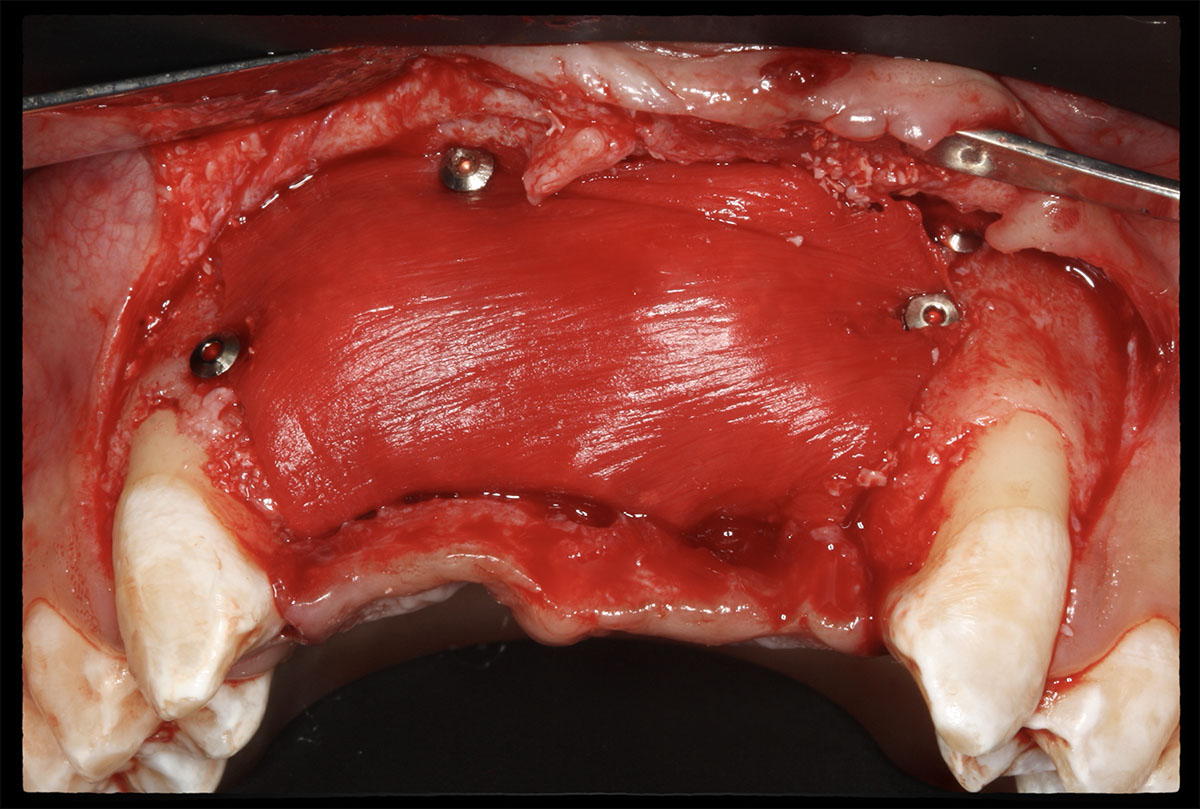
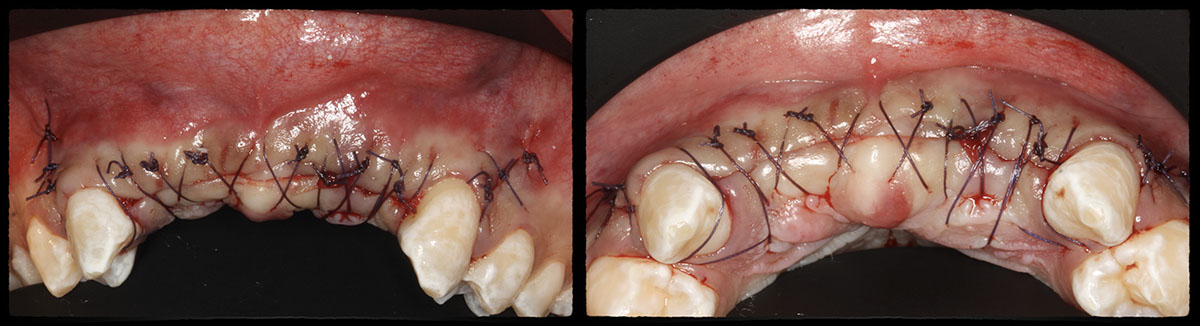
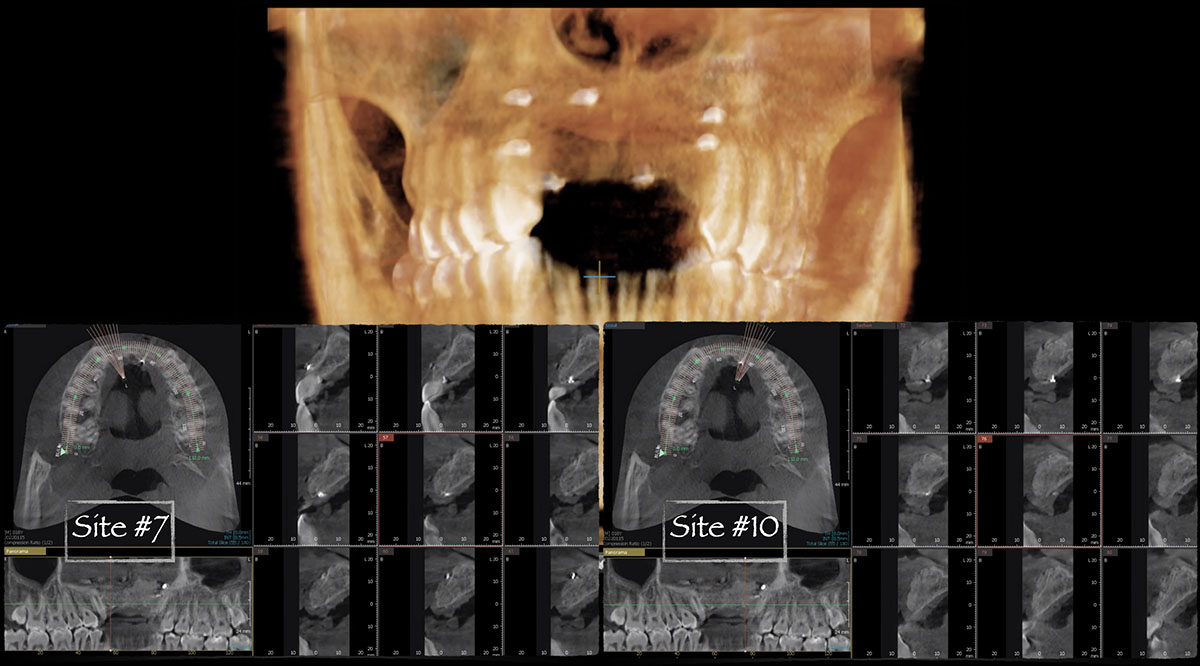
Teeth 30* and 31* had been previously extracted without alveolar ridge preservation. The site demonstrated that the site of tooth 7* had a history of implant removal with severe vertical bone deficiency & insufficient bone for implant placement. The treatment objective was bone regeneration using vallos® and Geistlich Bio-Gide® Forte.
*Universal Numbering System
Disclaimer: Case images courtesy of Karim Ghishan, BDS, MS (Periodontist, Ann Arbor, MI, USA) and Muhammad Saleh, BDS, MSD, PhD (Periodontist, Ann Arbor, MI, USA). Used with permission. Images are provided for illustrative and educational purposes only. Results are not guaranteed, and individual outcomes may vary depending on patient-specific circumstances and clinical factors. This information is for general educational purposes only and does not constitute medical advice, nor does it necessarily reflect the official position, opinion, or recommendations of Geistlich. Treatment decisions are made at the clinician’s discretion based on each patient’s unique needs.