








The Foundations of Success
in Immediate Implant Placement
Testimonials

“Immediate implant placement usually requires a bone graft to fill the gap between the implant and the socket walls. The use of bovine granules with the addition of porcine collagen (Geistlich Bio-Oss Collagen®) has demonstrated long-term stability to maintain alveolar contour and optimal bone level and soft tissue support around implants.”Dr. Waldemar Polido | Indianapolis, Indiana, USA










Challenges of Immediate Implants Without Preventive Regeneration

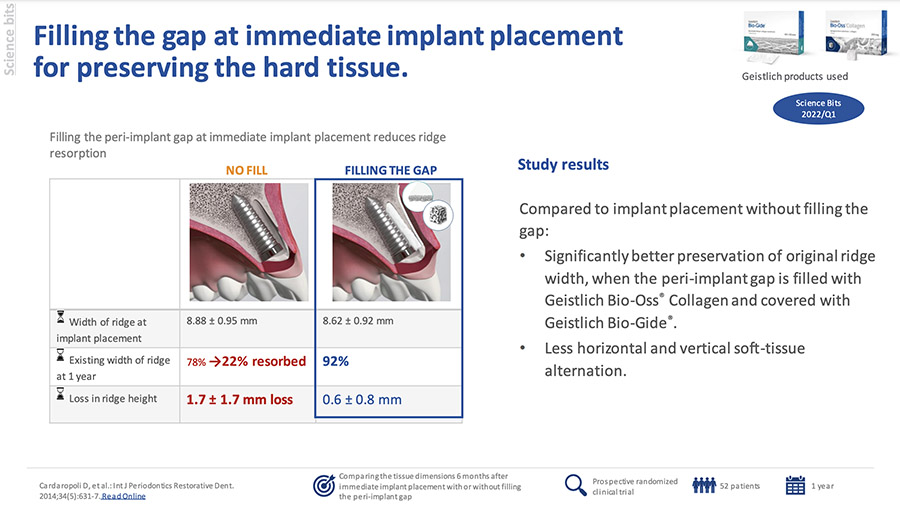
Implants alone cannot maintain the ridge volume. Studies show that after one year, 22% of the ridge width and 1.7 mm of the ridge height are lost5

Two-thirds of resorption take place within the first 3 months2

Poor maintenance of healthy peri-implant tissues leads to poor esthetic outcomes3,14

There is a 10x greater need for hard tissue augmentation at implant placement without previous ridge augmentation4
Immediate Implant Placement Proven Solutions with Geistlich Biomaterials

Unmatched Evidence:
Numerous studies on Geistlich Bio-Oss & Geistlich Bio-Oss Collagen showcase extensive implants and long followup periods. Alternatives have limited to no data in comparison, and Geistlich Bio-Oss & Geistlich Bio-Oss Collagen have the largest number of studies on Immediate Implant Placement.15
Cost Effective Choice:
Choosing alternatives may increase the risk of implant failure. 14x more patients and implants were treated with Geistlich Bio-Oss & Geistlich Bio-Oss Collagen than all other alternatives combined.15

IIP Comparative Technical Brief
What can I do to minimize bone volume resorption around my patient’s immediate implant?
Fill The Gap
Fill-the-gap in extraction sockets with
preserved buccal bone wall1
Fill-the-gap in extraction sockets with
defective buccal bone wall3
Seamless Solutions:
For the best clinical outcomes the choice is clear: Fill The Gap.
Geistlich products make this Simple and Effective.
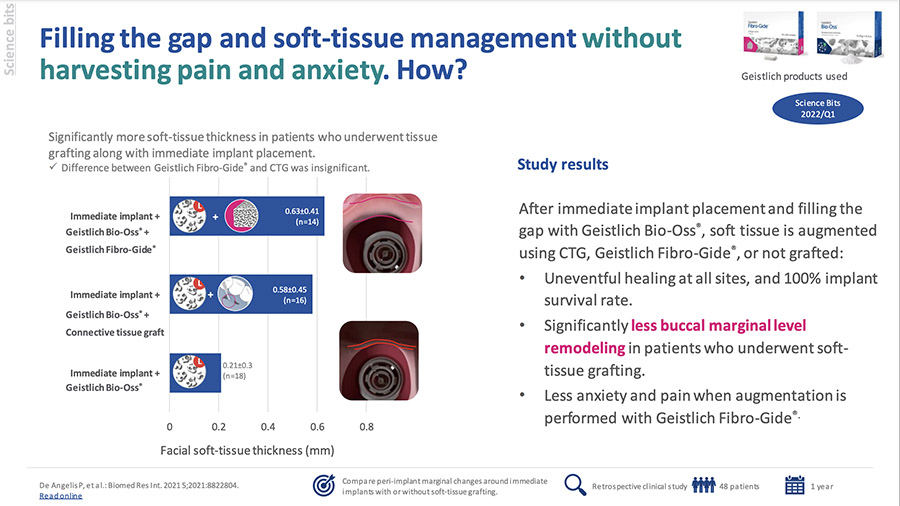
- Filling the peri-implant gap with Geistlich Bio-Oss® Collagen and Geistlich Bio-Gide® preserved 92% of the original ridge width.5
- Filling the peri-implant gap with Geistlich Bio-Oss® Collagen resulted in better soft and bone tissue outcomes than immediate implants alone.⁶
- Geistlich biomaterials can largely compensate for bone loss and preserve the contour of the alveolar ridge.1,7,8
- Reduced number of surgeries per patient.5,10-13
- Preserves soft tissue volume, leading to an improved treatment outcome.⁹
Treatment of the Failed Maxillary Central Incisor Tooth: “10 Keys” for Successful Esthetic Zone Single Immediate Implants
Regeneration all-around:
One portfolio, many treatment options
The choice is clear – Fill the Gap with Our Regenerative Products
for Immediate Implant Placements!

The Original Xenograft Bone Substitute

Reshape Your
Expectation
An Allograft that Set the Pace for Regeneration
Intelligently Designed to Guide Your Success

The Ideal Matrix for Gain of Keratinized Tissue and Recession Coverage
The use of premium products with extensive clinical documentation is key to protecting your investment and bringing another level of excellence to your practice. Treat your patients confidently with Geistlich regenerative solutions.
Related Content

Bone Grafting and Immediate Implant Placement in the Maxillary First Molar Region

Ramal Bone Graft for Congenitally Missing Maxillary Lateral Incisor

Immediate Mandibular Molar Transition
Knowledge Boost:
Predictability and Esthetic Outcomes in Immediate Implant Placement

Implant Survival in Augmented Bone versus Native Bone
Soft Tissue Contour Changes at Immediate Implants
Influence of Immediate Implant Placement and Provisionalization…
- Cardaropoli D, et al. Int J Periodontics Restorative Dent. 2014 Mar–Apr;34(2):211-7. (Clinical study)
- Schropp L, et al. Int J Periodontics Restorative Dent. 2003 Aug;23(4):313-23. (Clinical study)
- Vignoletti F, et al. Clin Oral Implants Res. 2012 Feb;23 Suppl 5:22-38. (Systematic review)
- Weng D, et al. Eur J Oral Implantol. 2011;4 Suppl:59-66. (Systematic review)
- Cardaropoli, D. et al. Int J Periodontics Restorative Dent. 2014;34 (5):631-7. (clinical study)
- Girlanda, FF., et al. Clin Oral Investig. 2019 Oct;23(10):3885-3893. (clinical study)
- Jung RE, et al. J Clin Periodontol. 2013 Jan;40(1):90-8. (Clinical study)
- Cardaropoli D, et al. Int J Periodontics Restorative Dent. 2012 Aug;32(4):421-30. (Clinical study)
- Ackermann KL, Extraction site management using a natural bone mineral containing collagen: rationale and restrospective case study.
The International Journal of Periodontics and Restorative Dentistry 2009; 29: 489-497 - Cardaropoli, D. et al. Int J Periodontics Restorative Dent. 2015;35:677-85. (clinical study)
- Tarnow DP et al. Int J Periodontics Restorative Dent. 2014 May-Jun;34(3):323-31. (clinical study)
- Al-Sabbah M et al. Dent Clin North Am. 2015 Jan;59(1):73-95. (clinical review)
- Sanz M et al. Clin Oral Implants Res. 2017 Aug;28(8):902-910. (clinical study)
- Schlee M, Esposito M: Eur J Oral Implantol 2009; 2(3):209-17. (Clinical study)
- Data on file, Geistlich Literature Search Evaluation Report, 2024, Geistlich Pharma AG
