CLINICAL CASE


THE OUTCOME
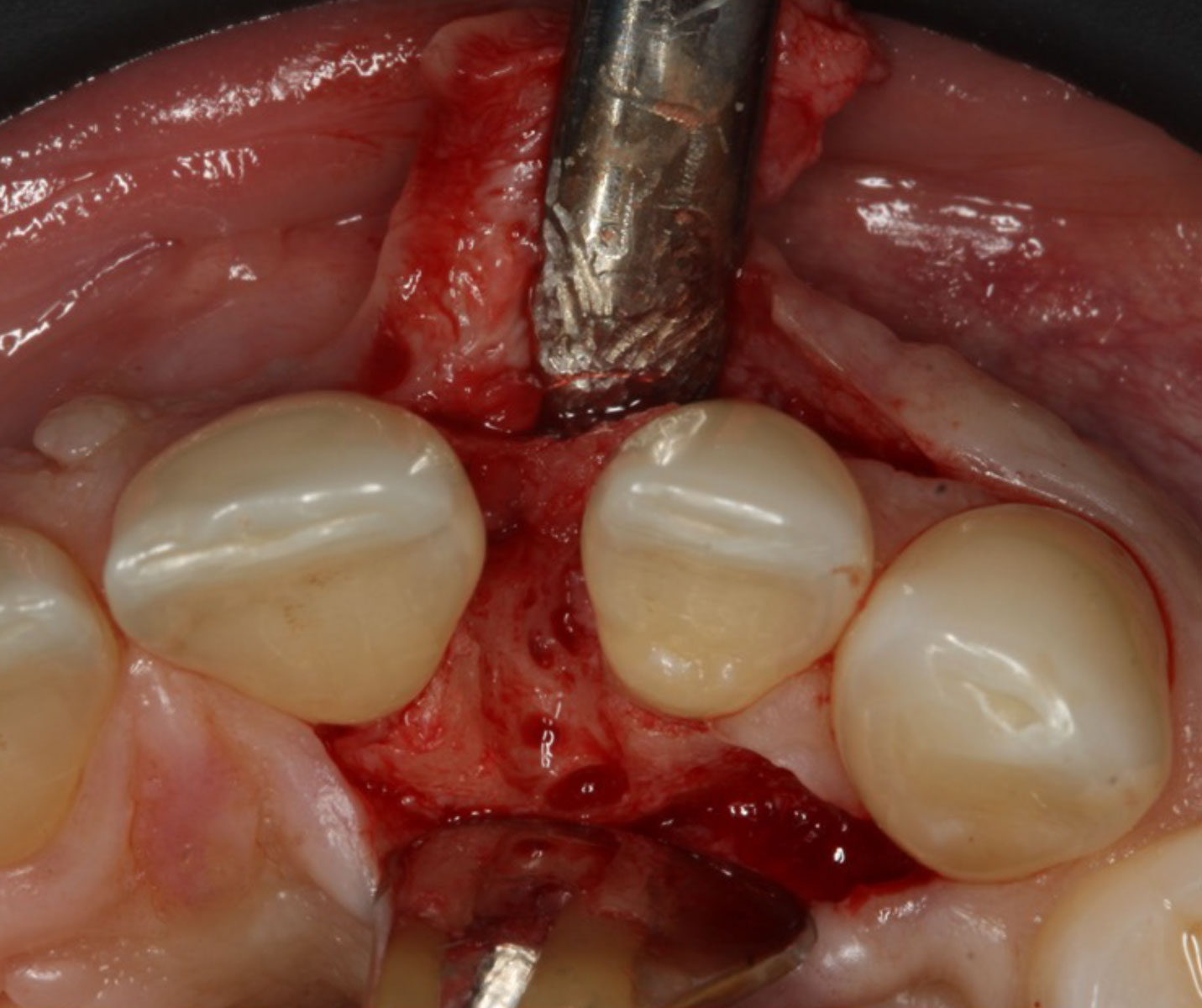
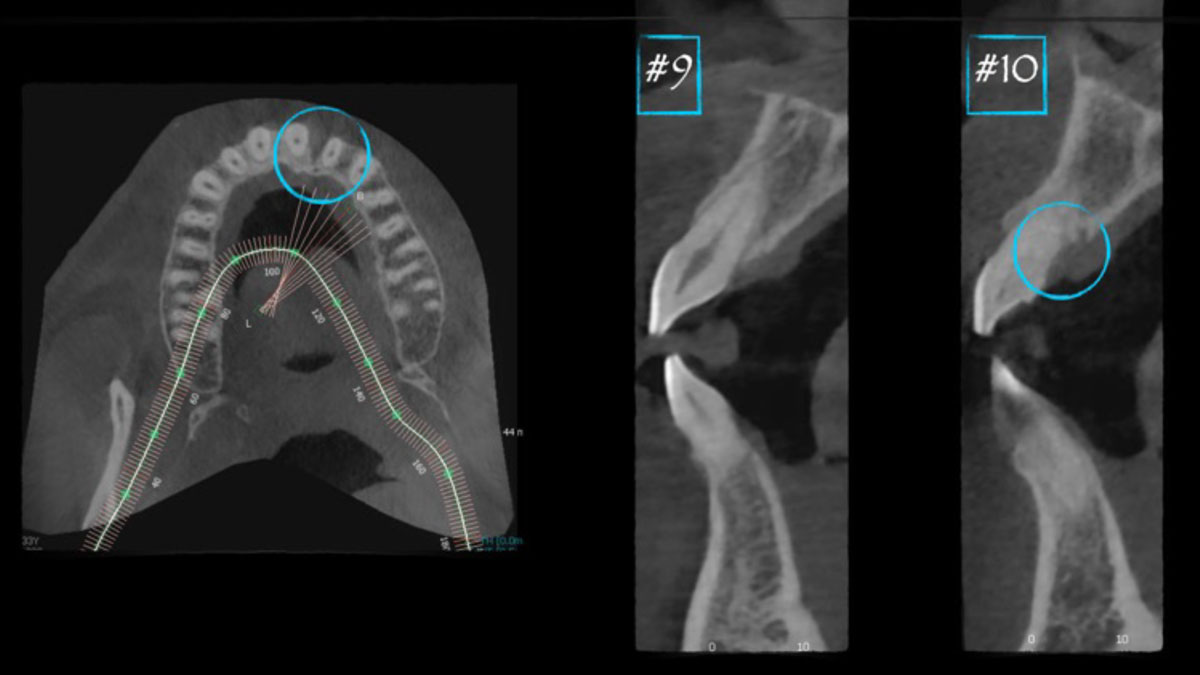
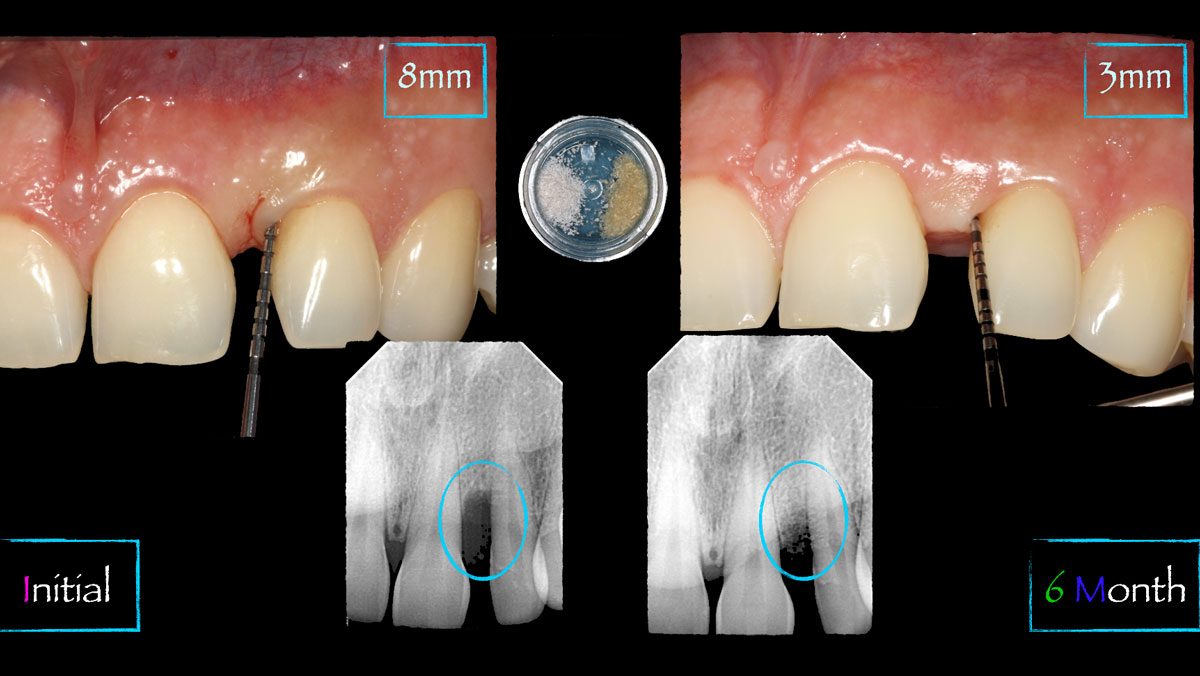
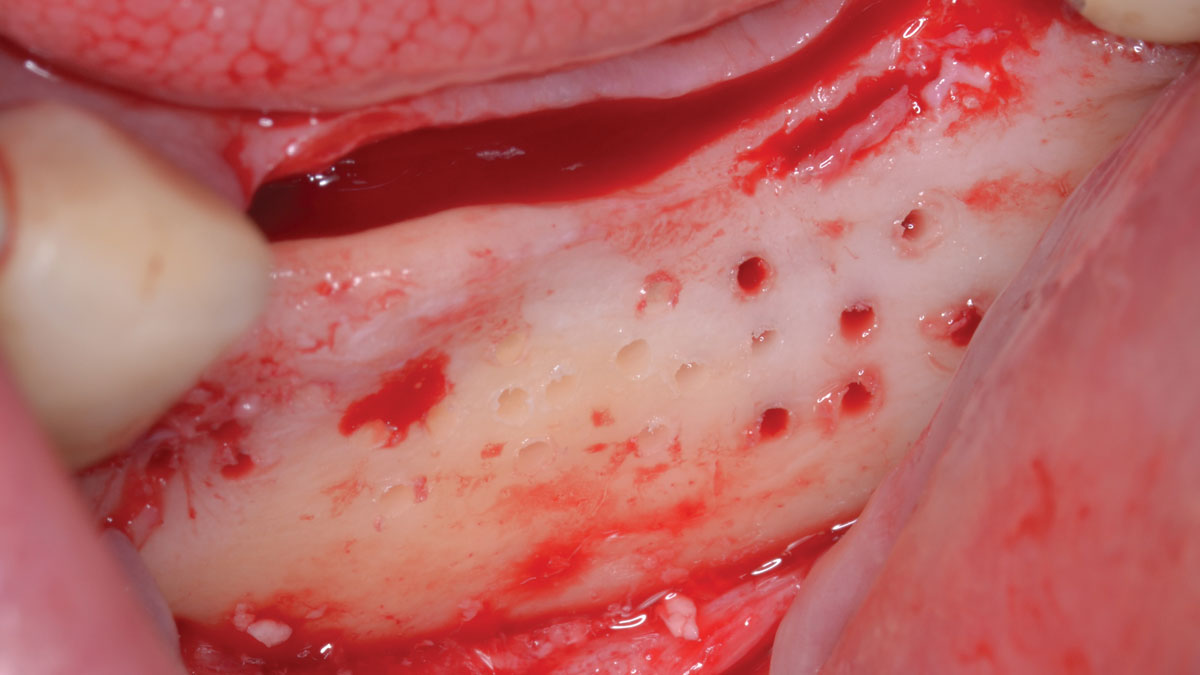
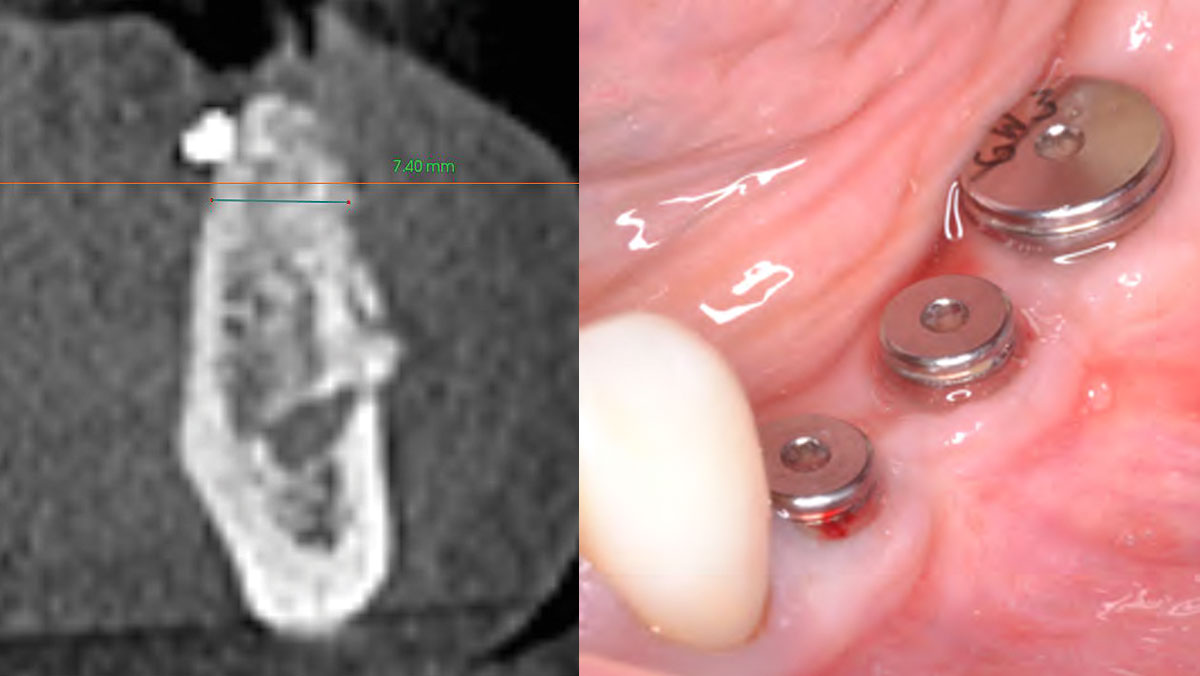
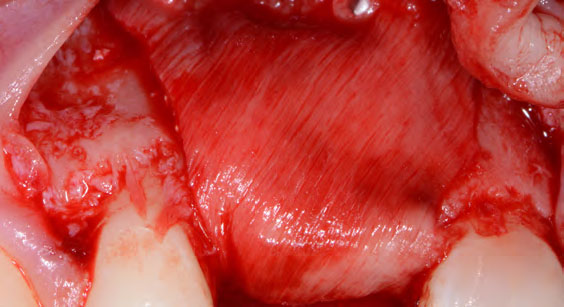
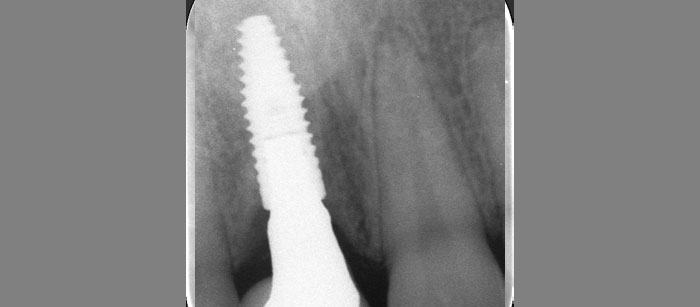
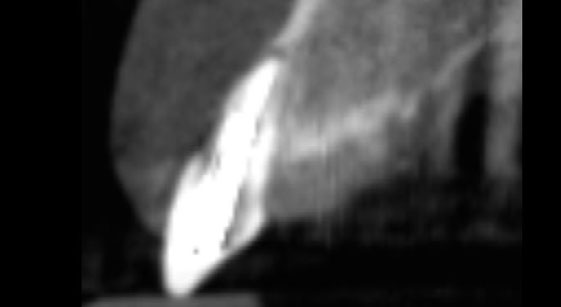
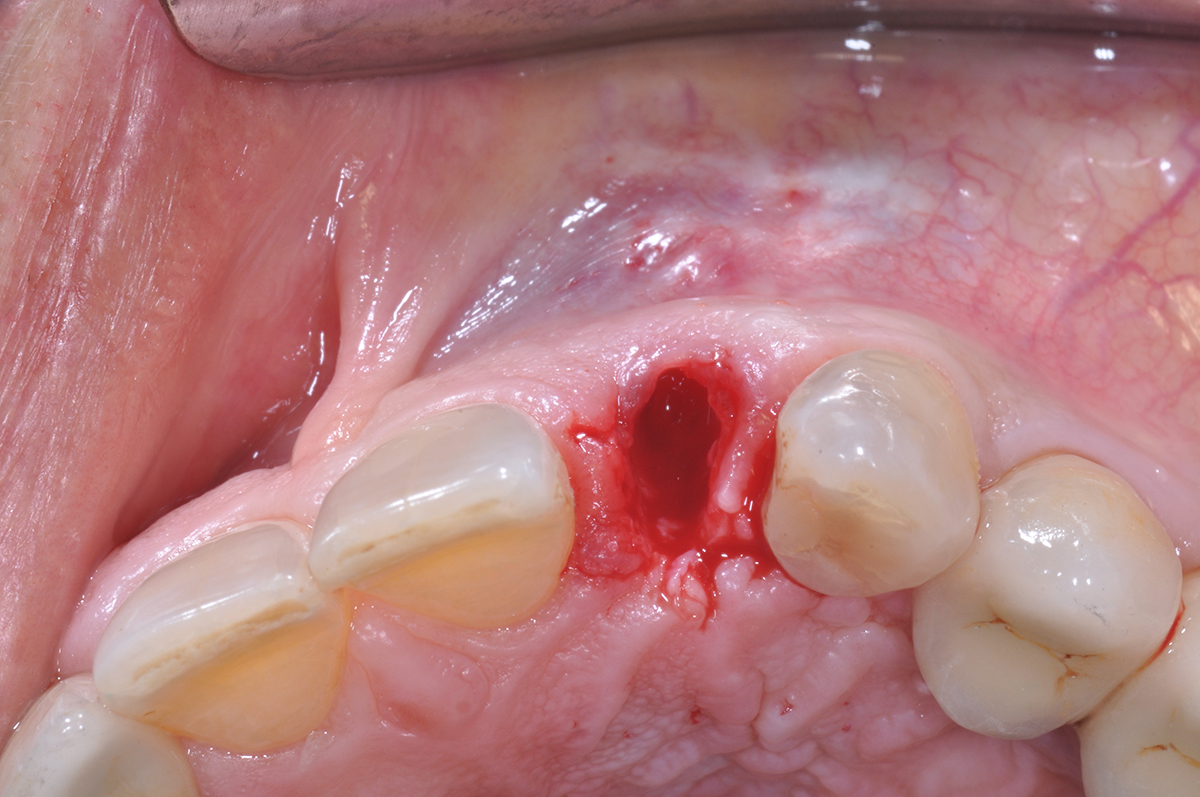
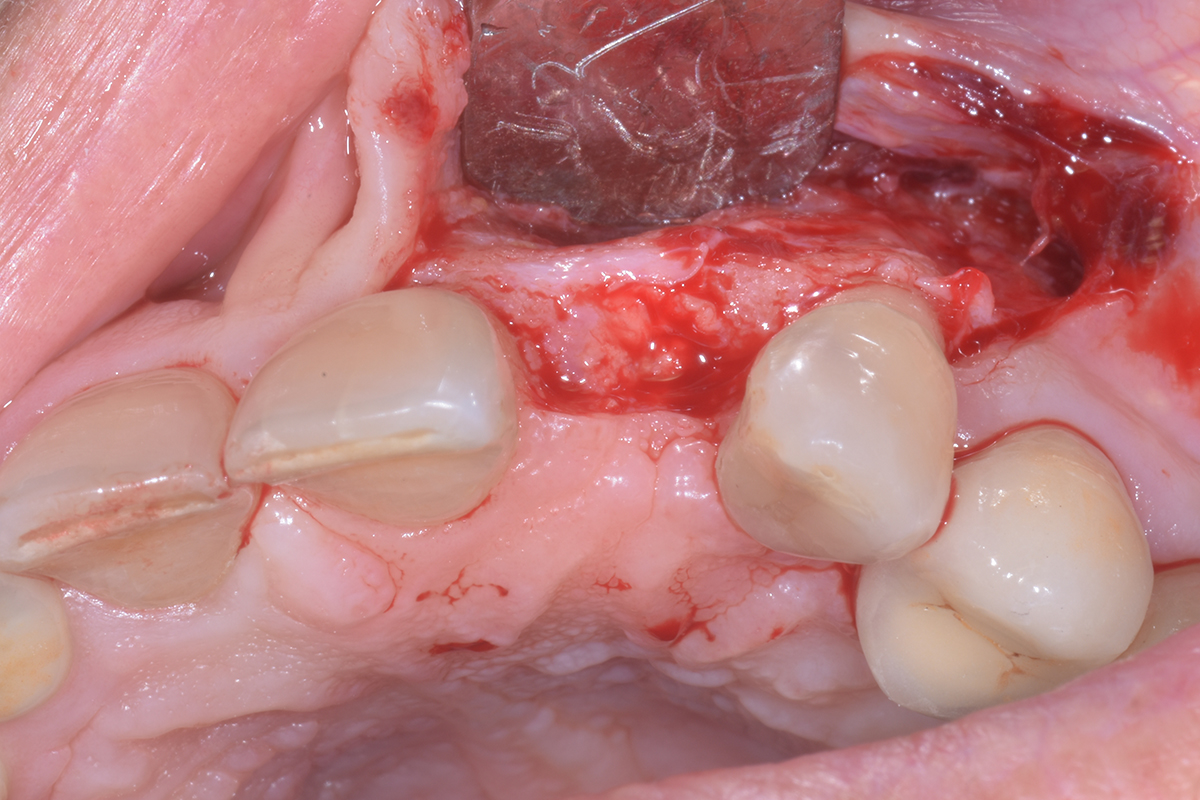
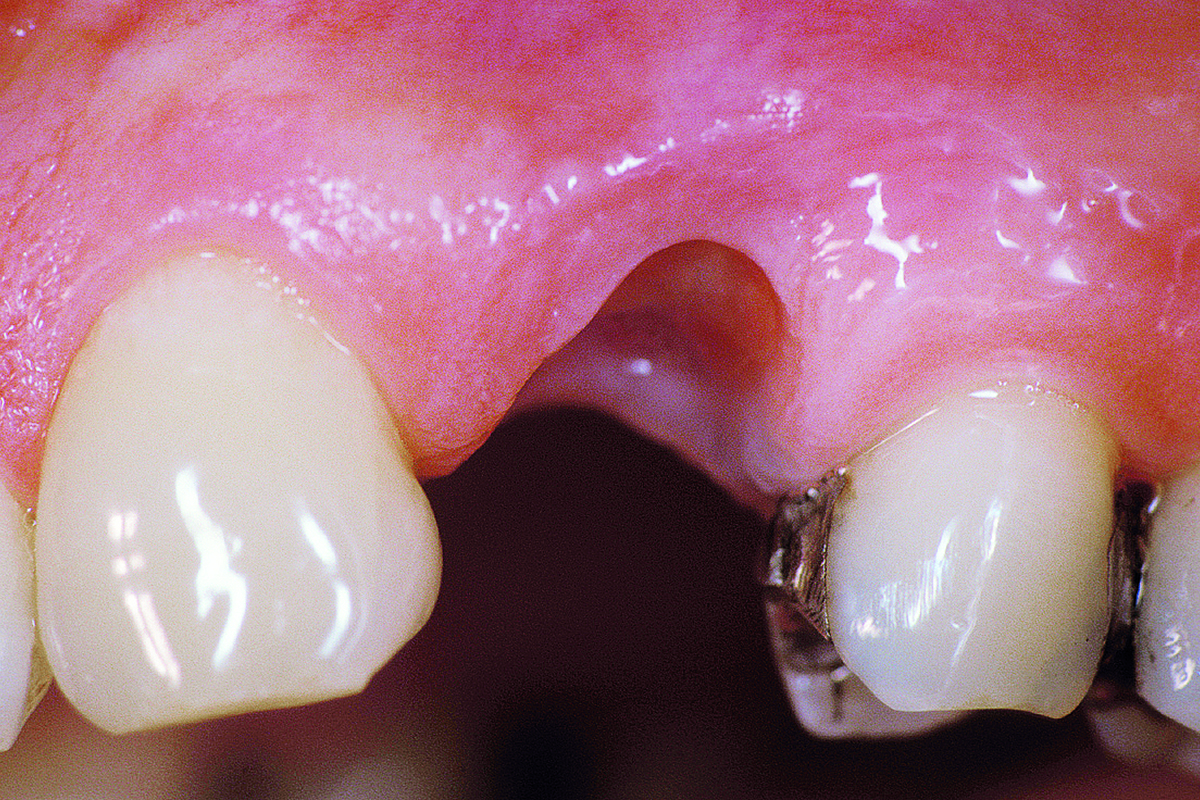
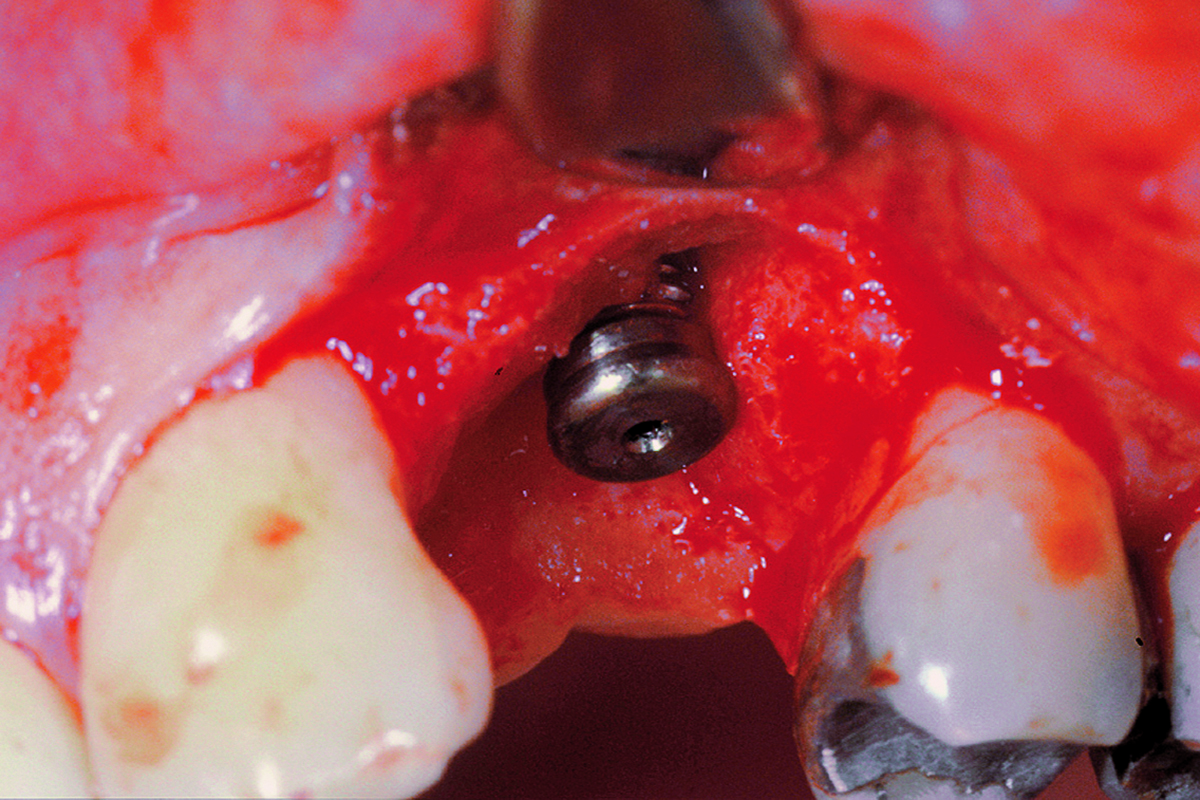
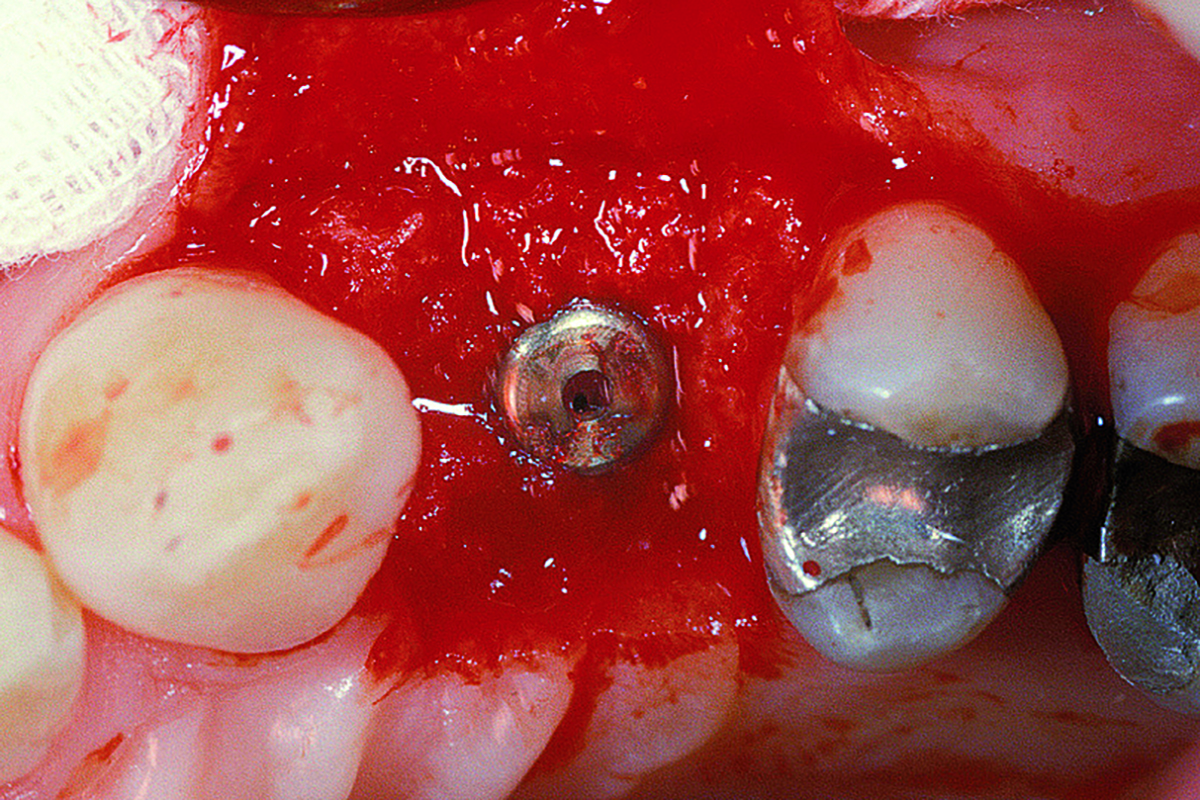
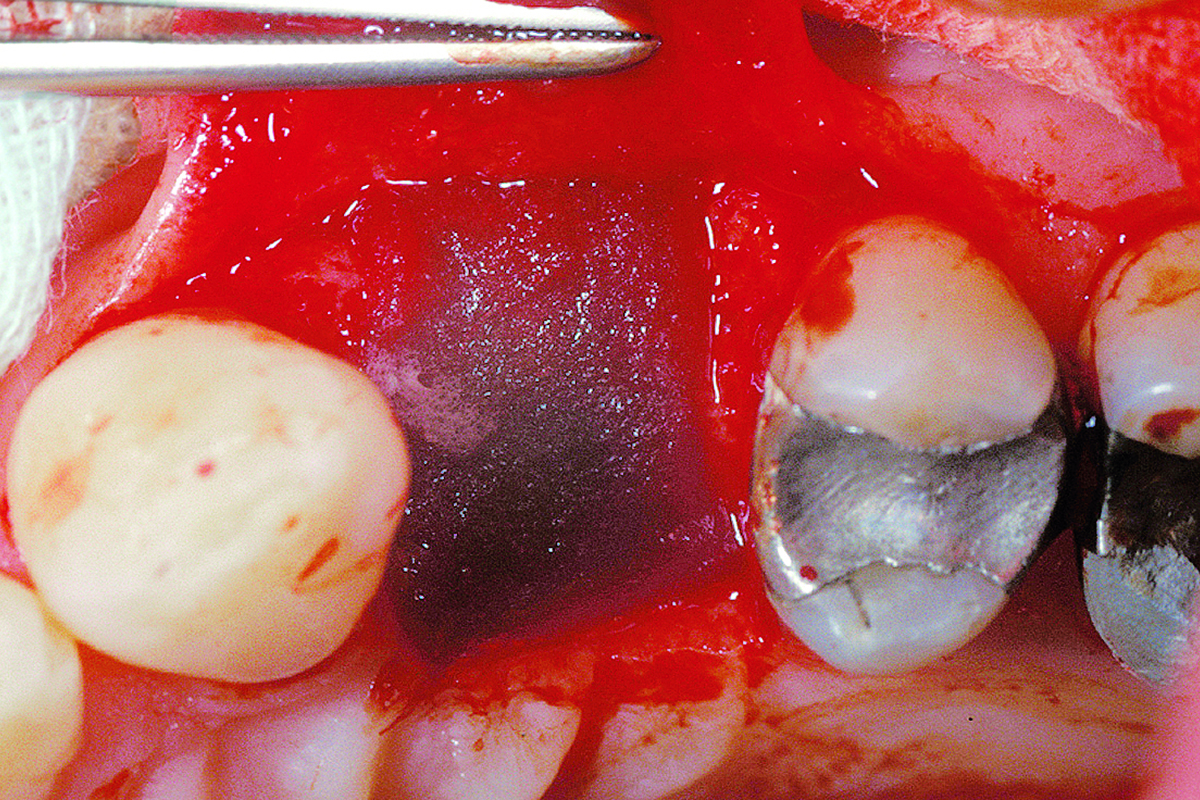
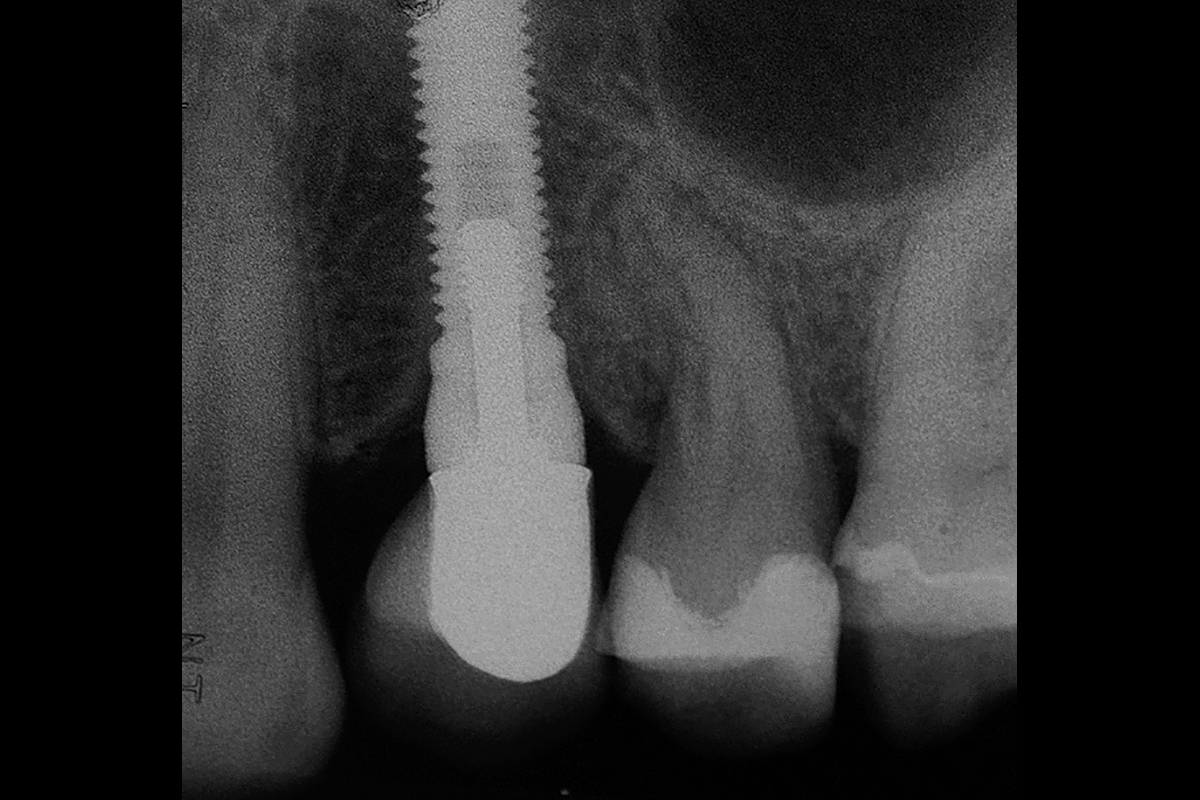
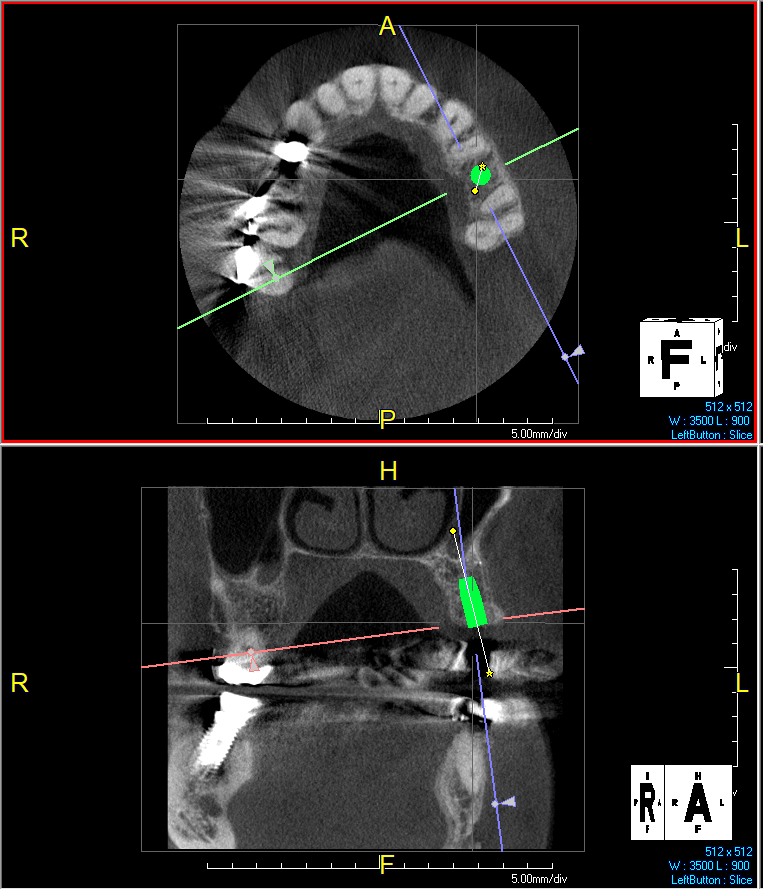
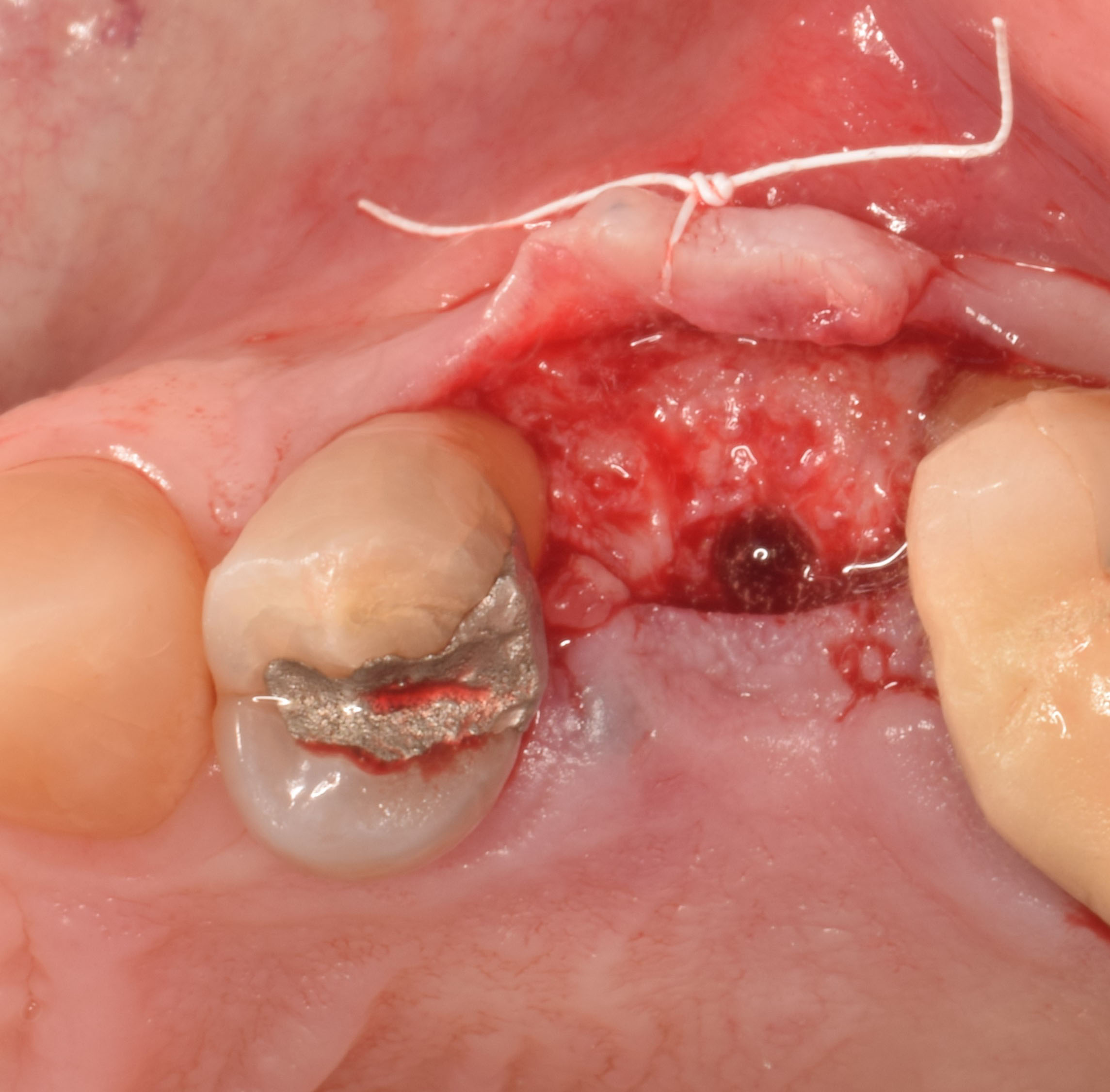
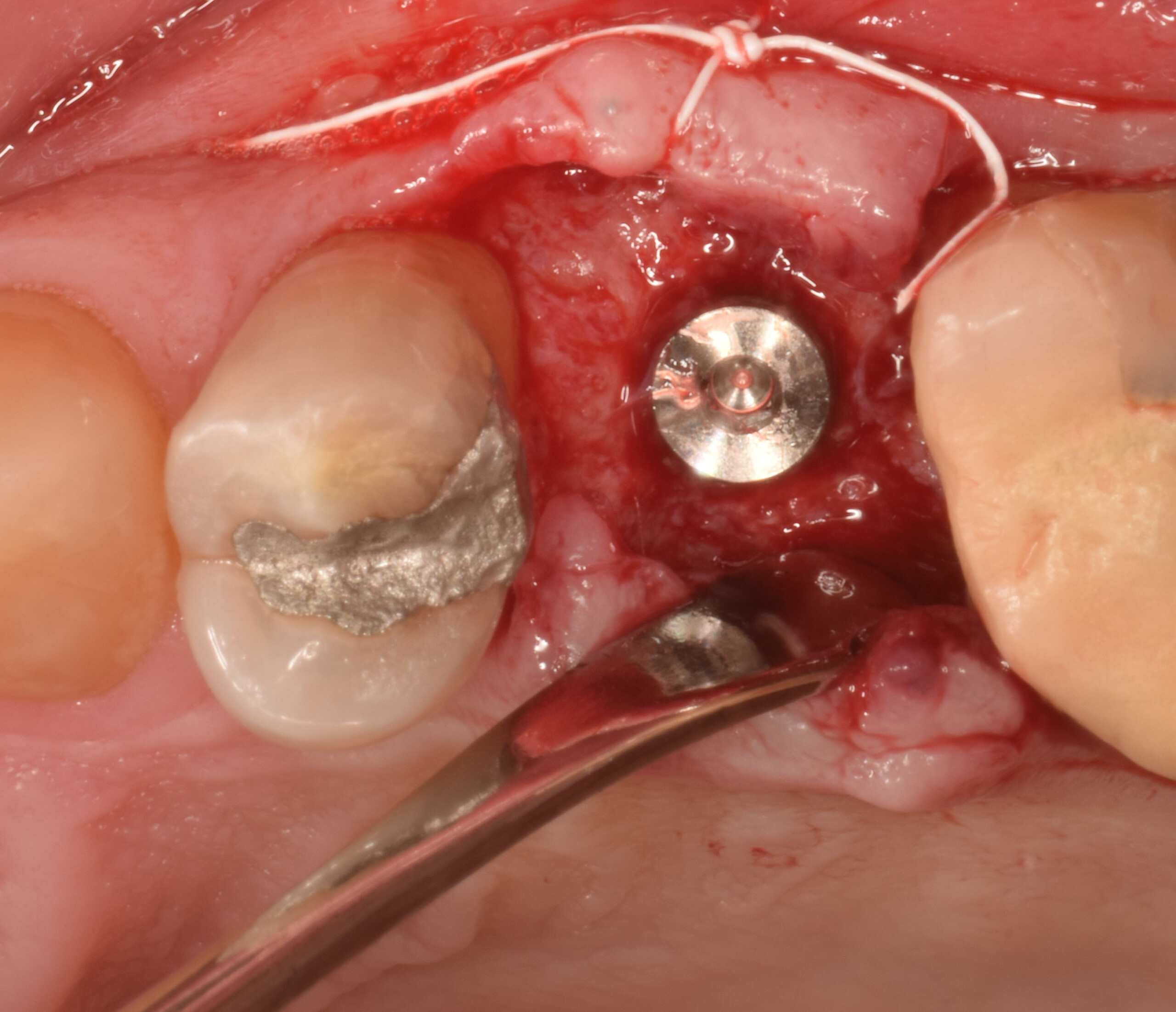
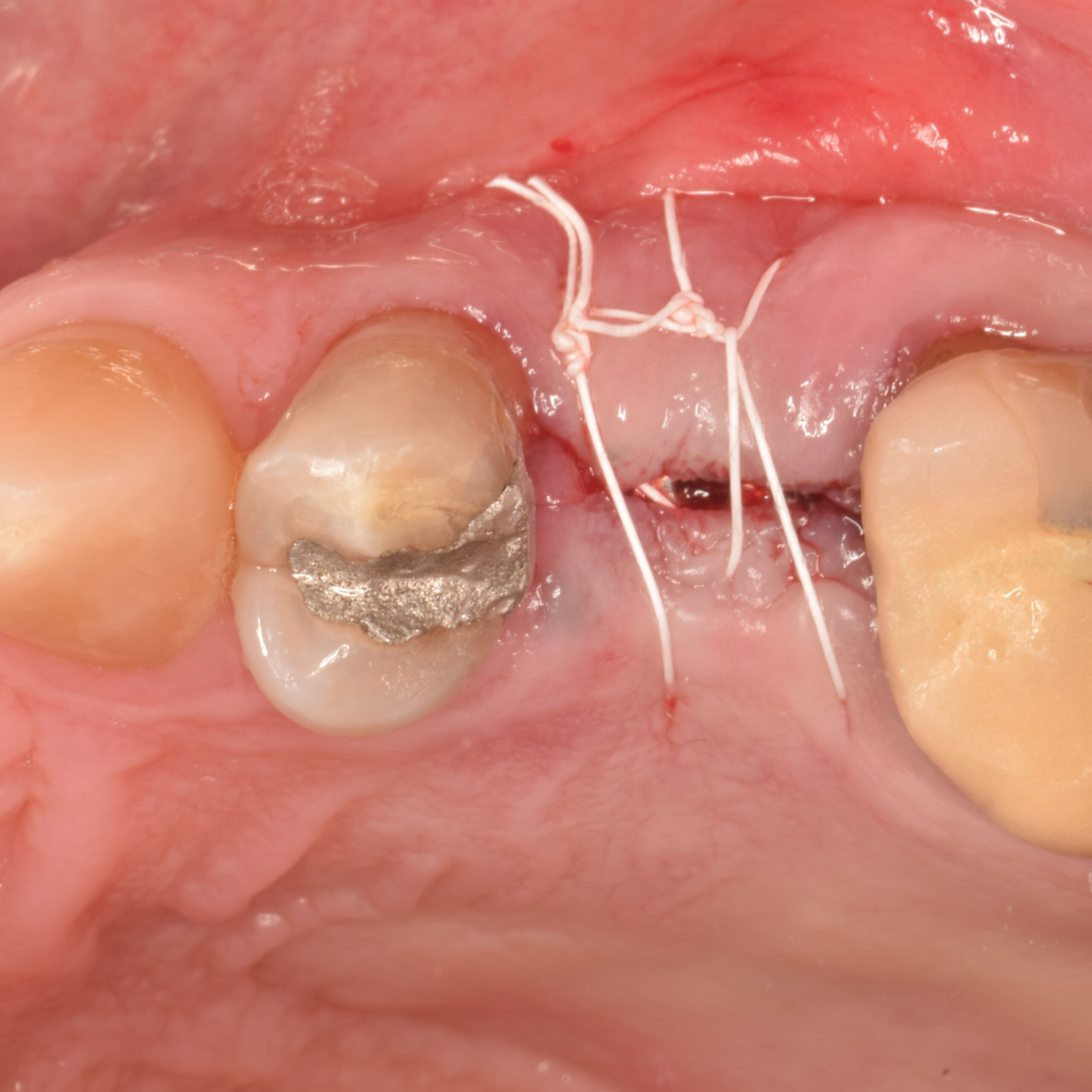
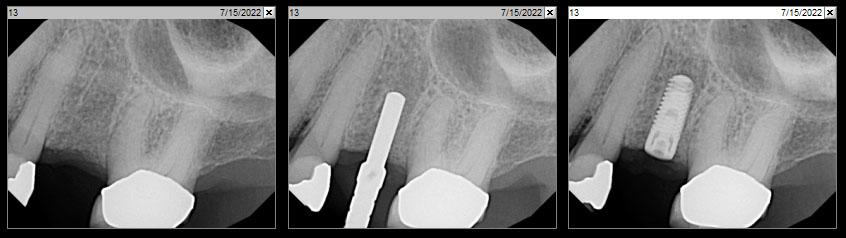
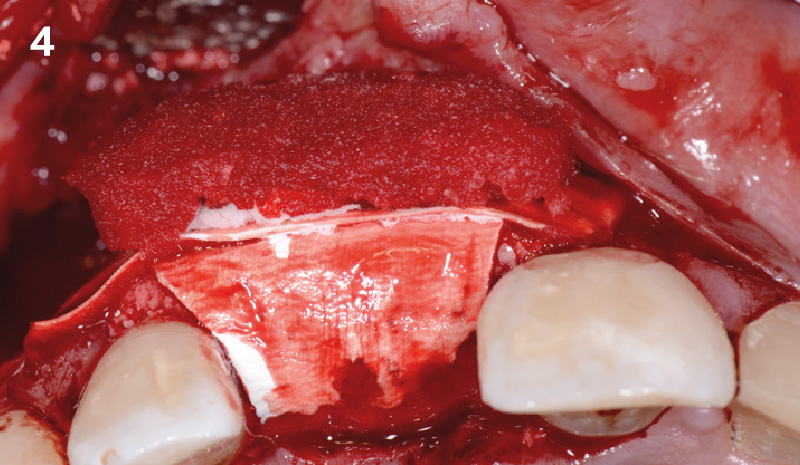
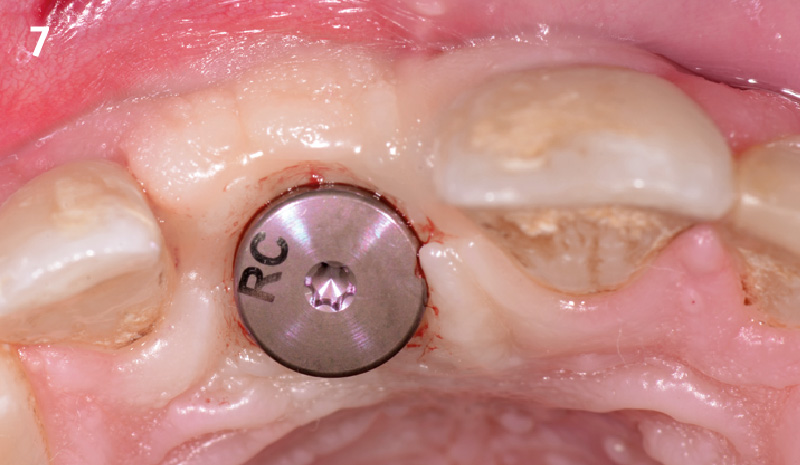
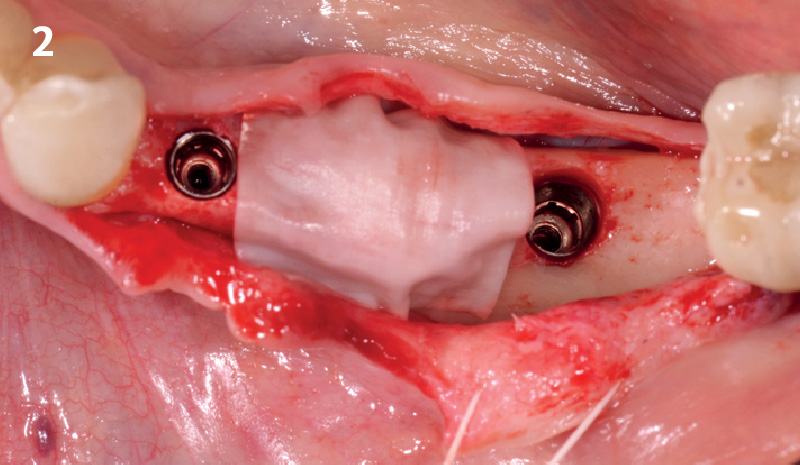
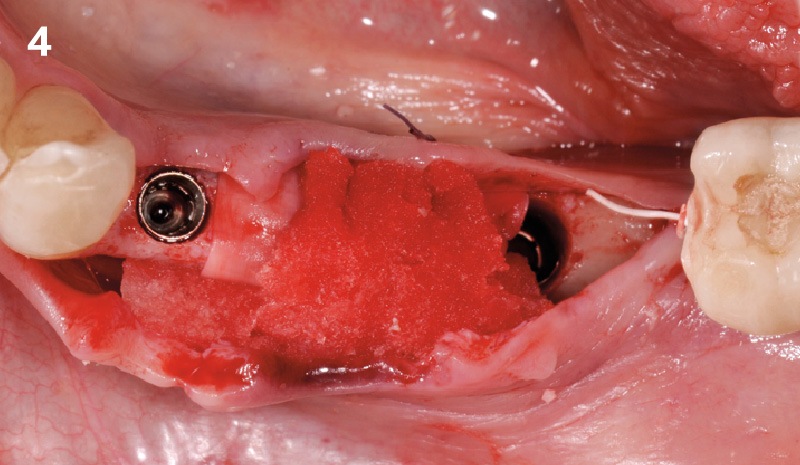
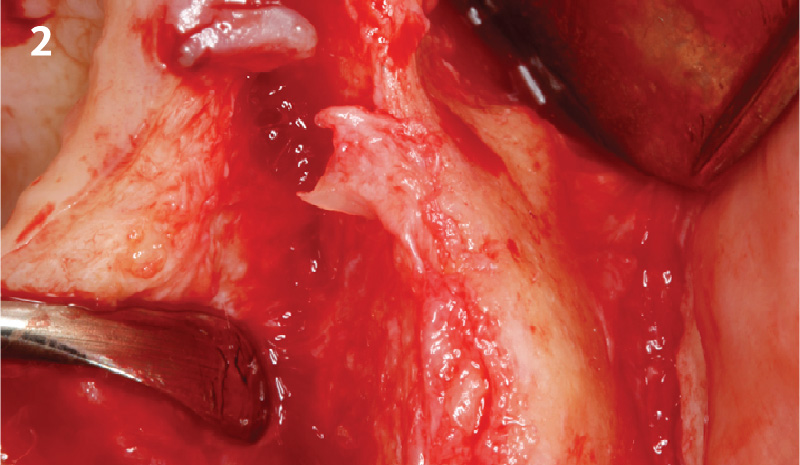
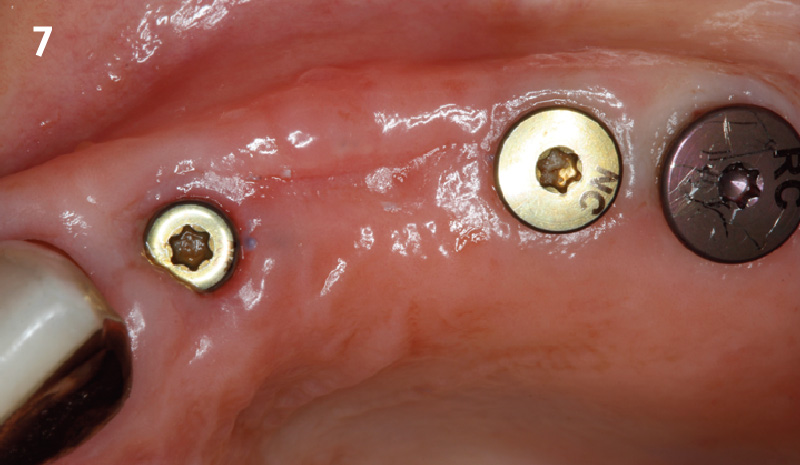
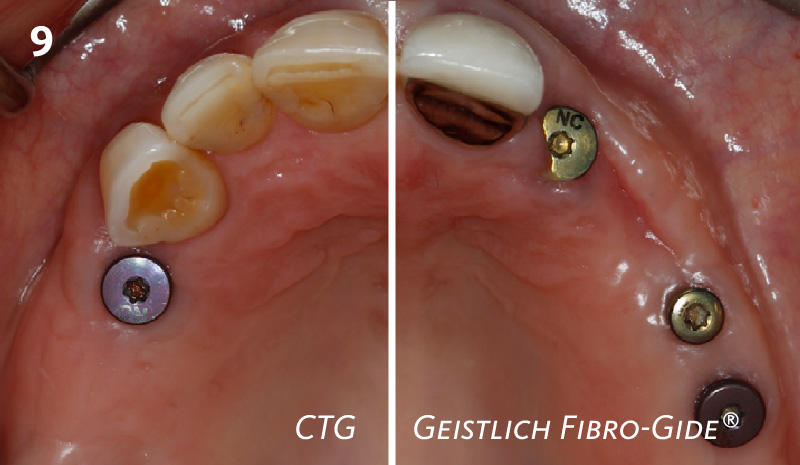
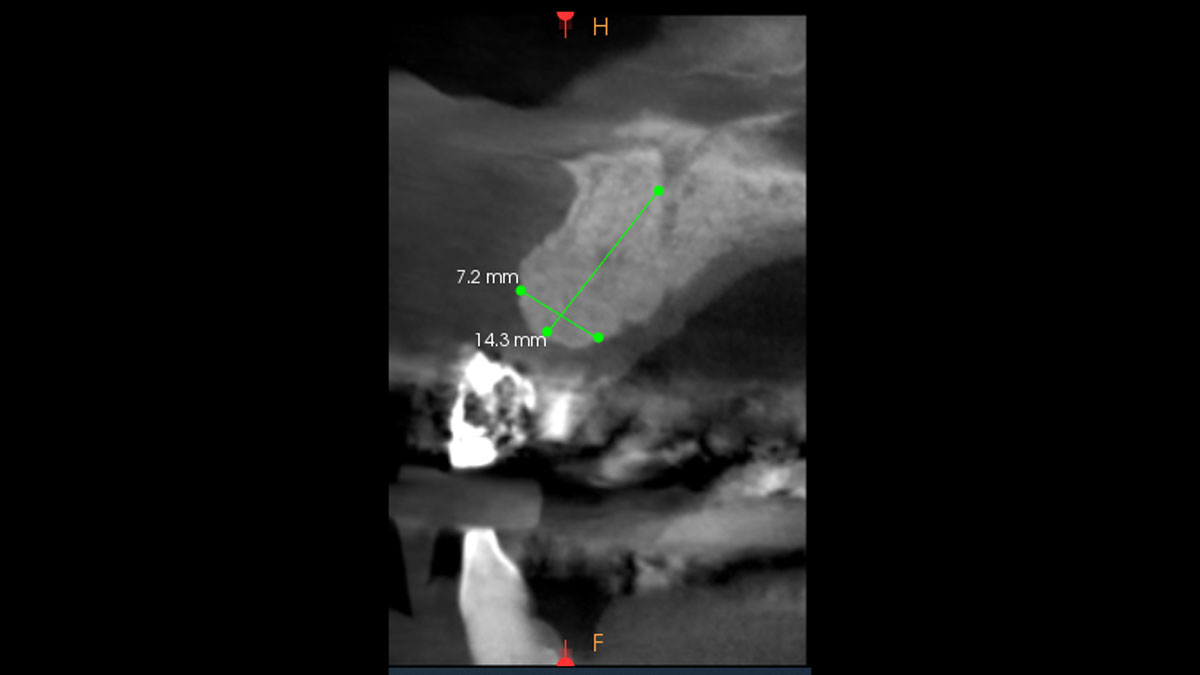
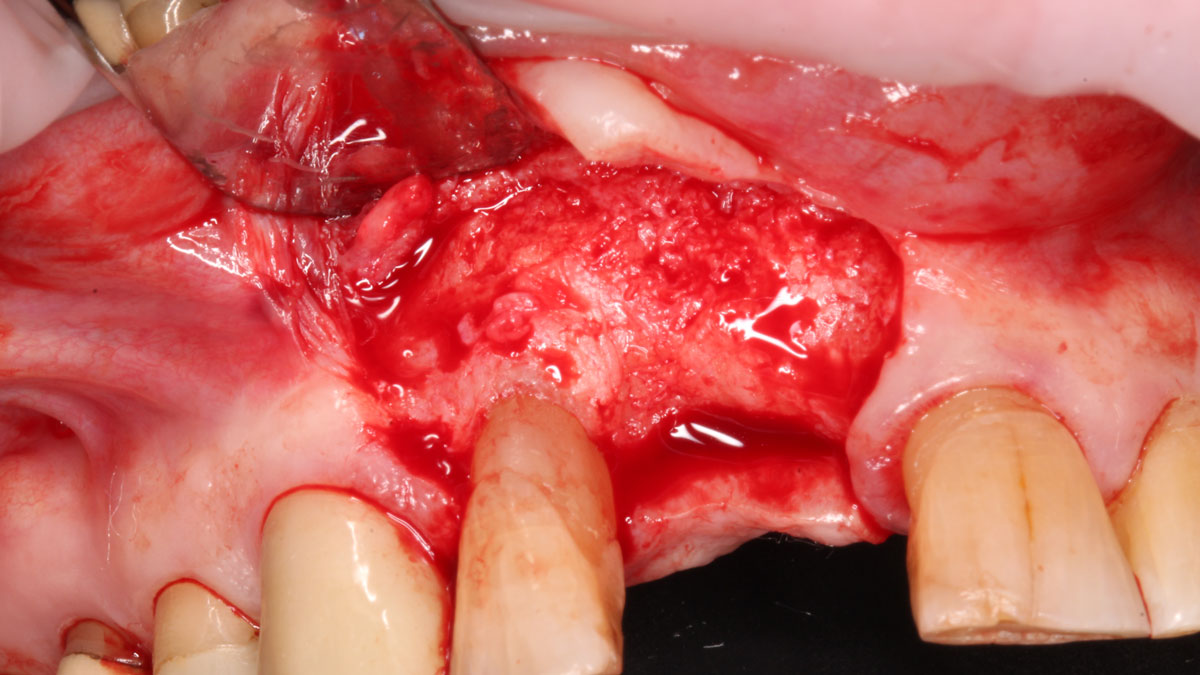
At 6 months, healing was complete with a bone fill of 10x10x6.5 mm. Tooth #7, affected by the combined defect, was fully regenerated. The adjacent ridge defect was also restored, enabling the placement of a regular-sized implant without the need for additional grafting.
Disclaimer: These results are not guaranteed; individual outcomes may vary depending on patient circumstances. This information is for informational purposes only and may not reflect Geistlich’s official position, opinion, or recommendation. Treatment decisions are made at the physician’s discretion, based on the unique needs of each patient.
GEM 21S® has not been approved by FDA for use in ridge augmentation in the US and the safety and effectiveness of GEM 21S® for this use has not been established by FDA.