BIOBRIEF
Guided Tissue Regeneration in the Esthetic Zone of a 34-Year-Old Male

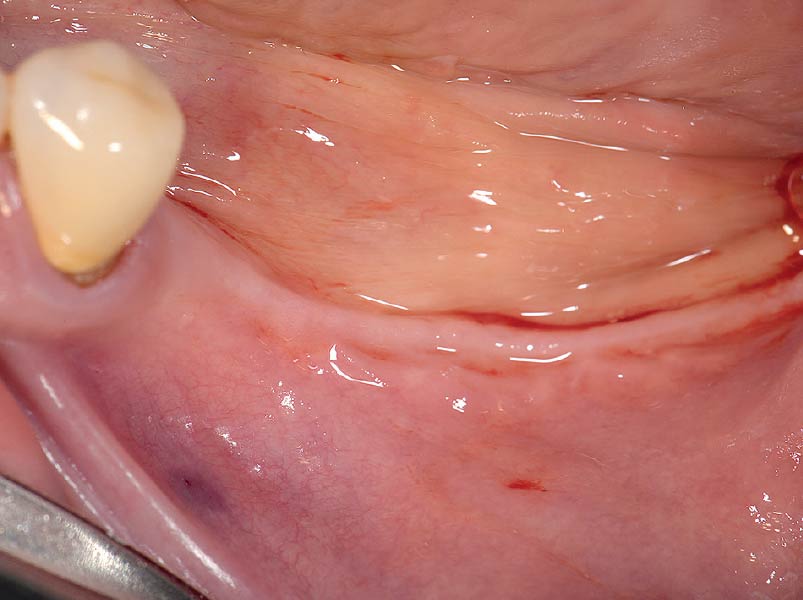
THE SITUATION
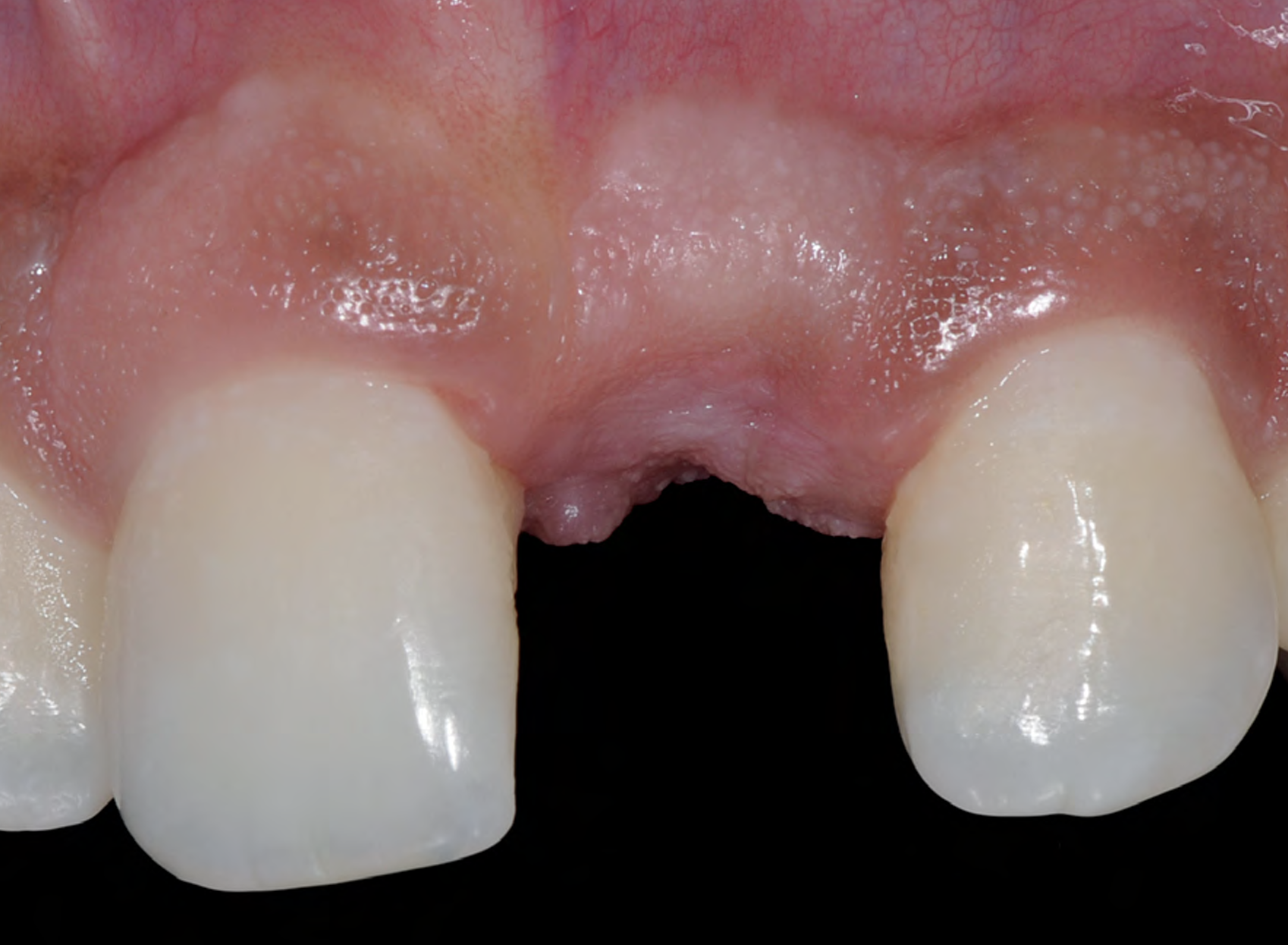
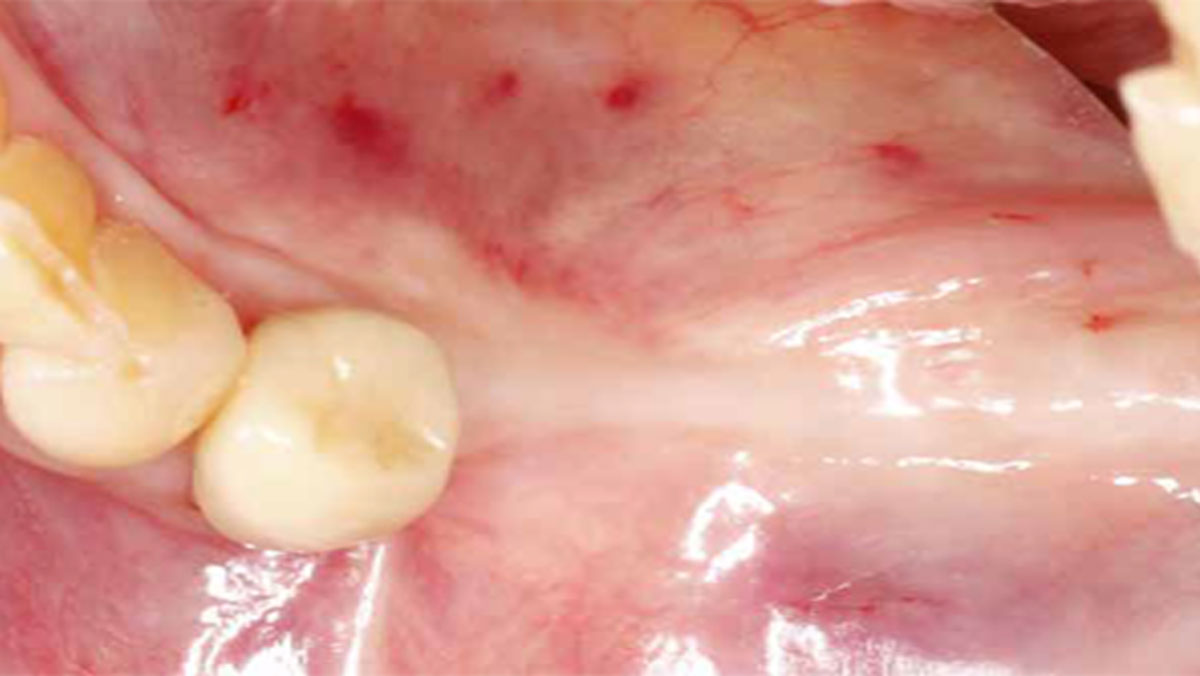
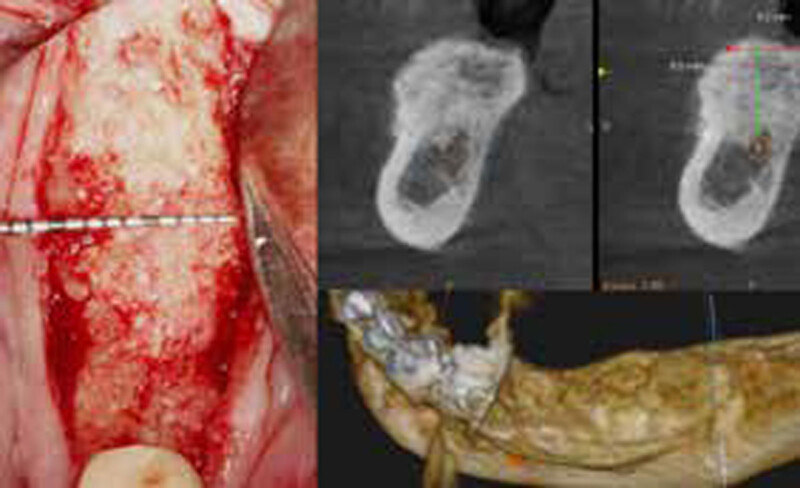
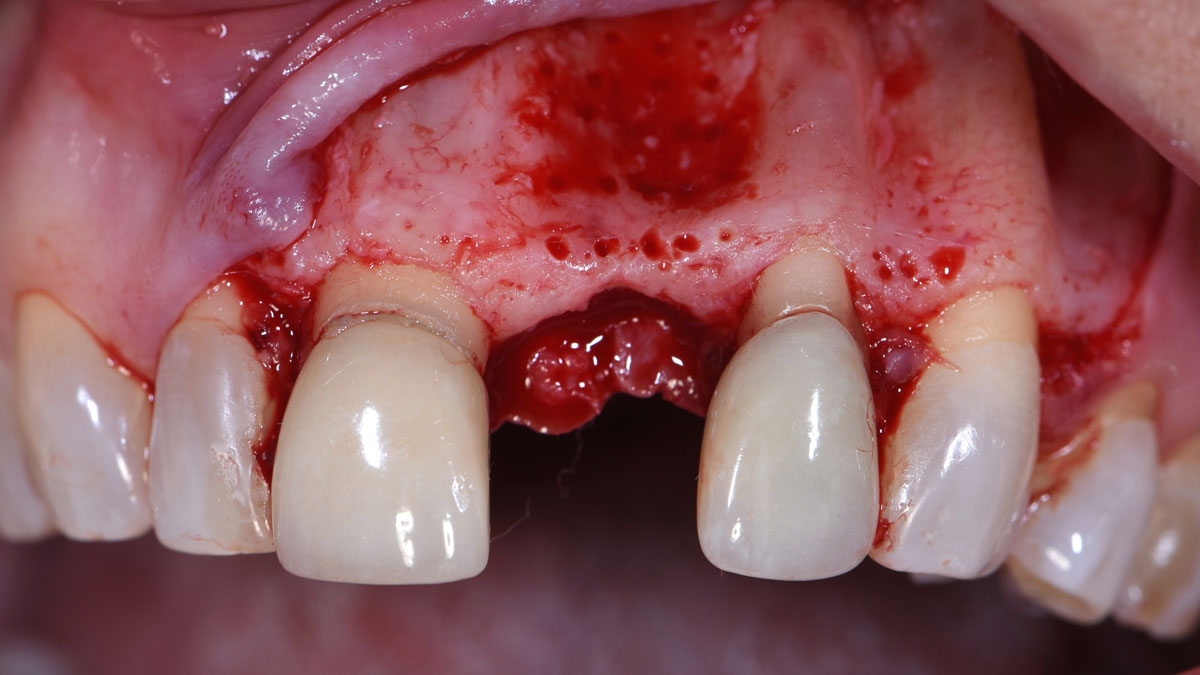
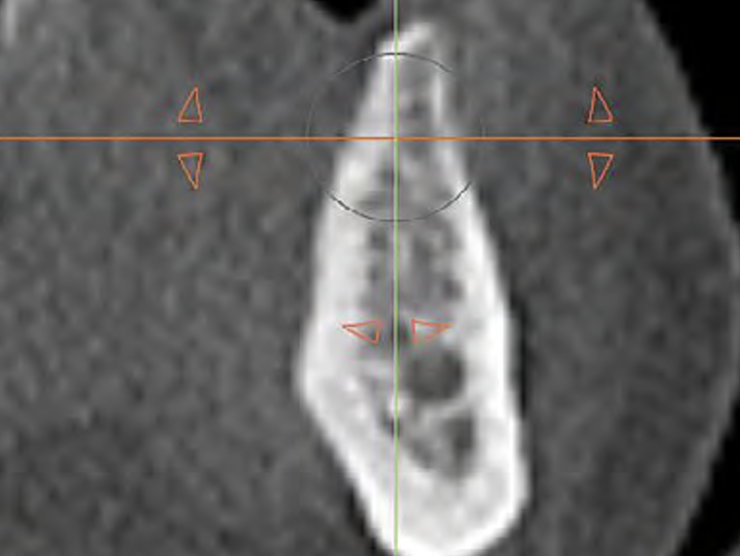
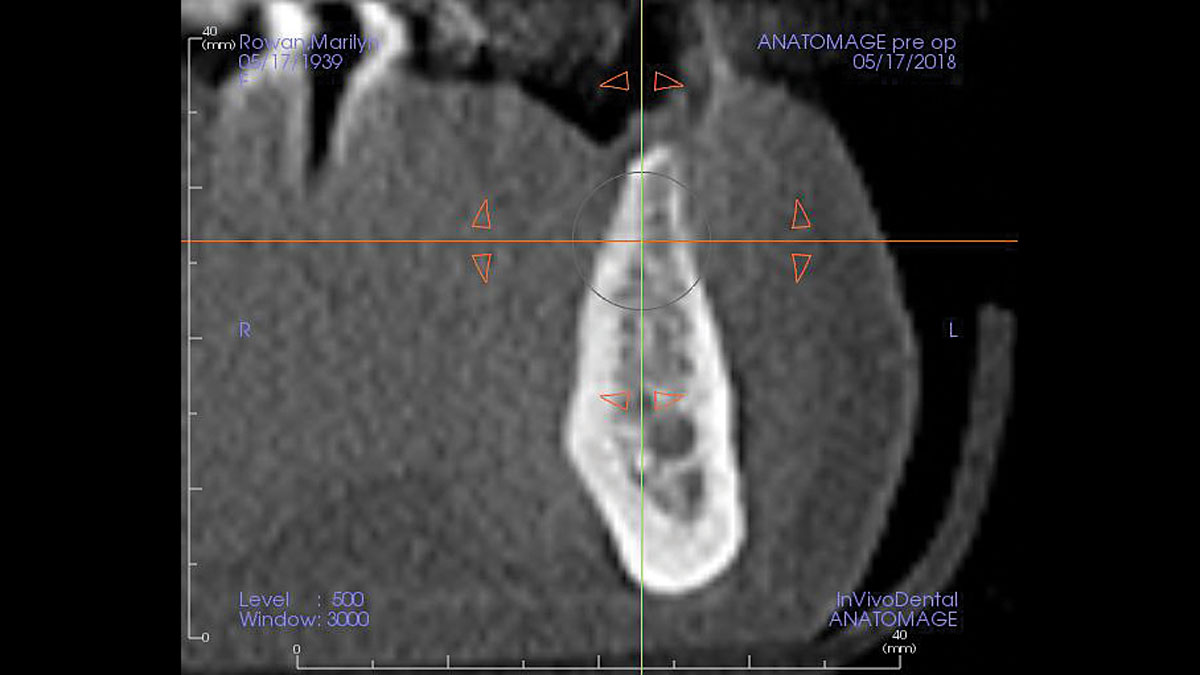
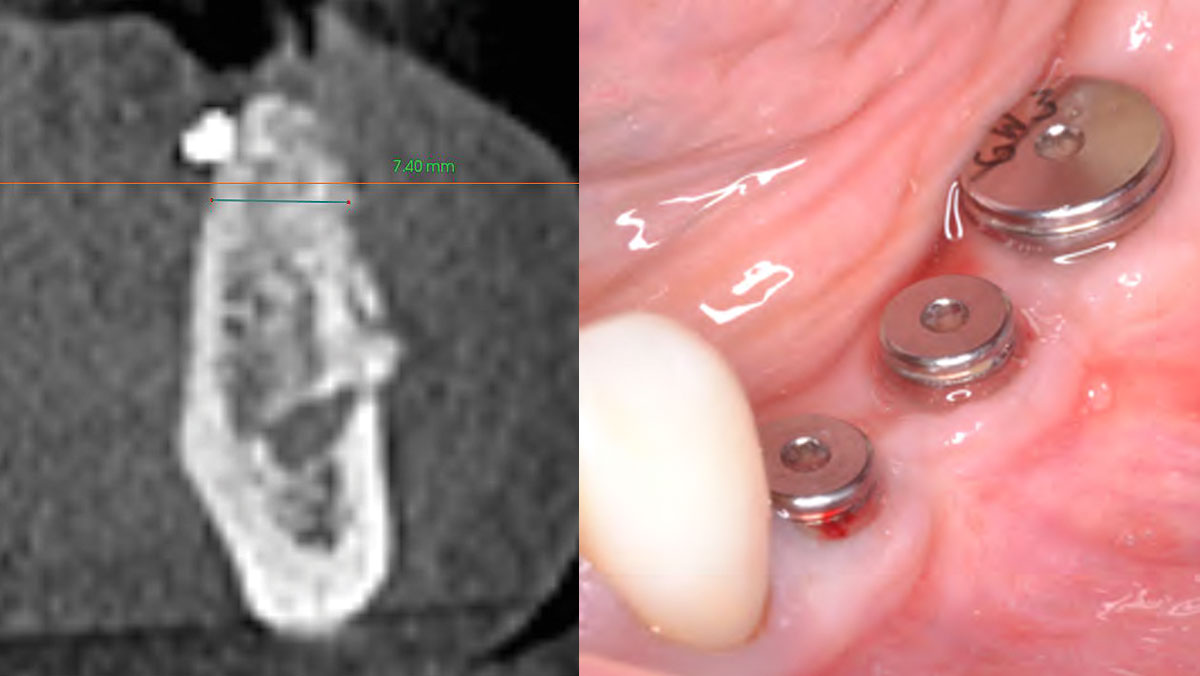
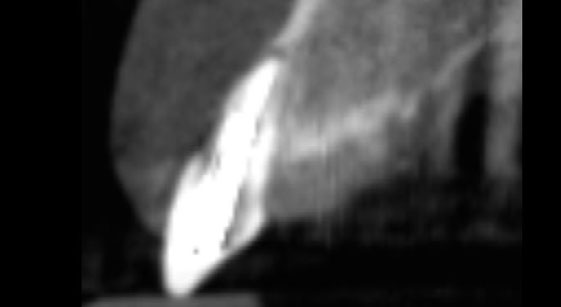
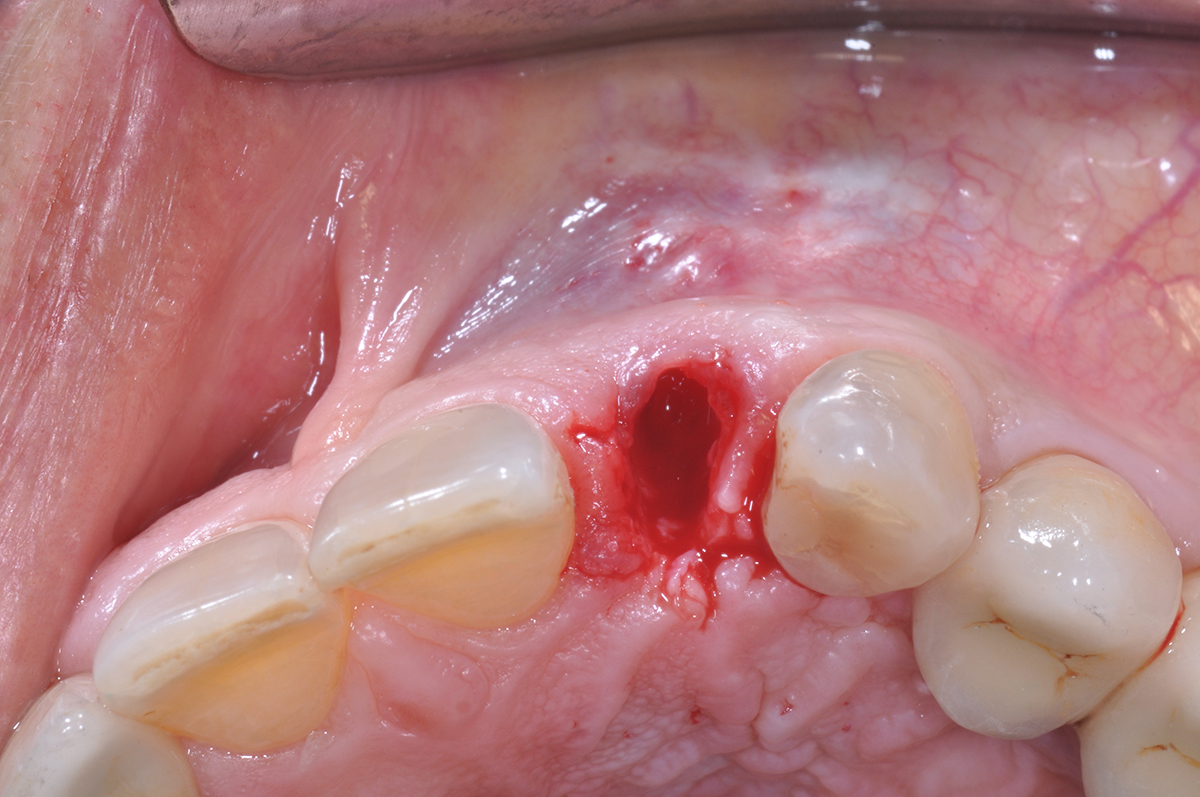
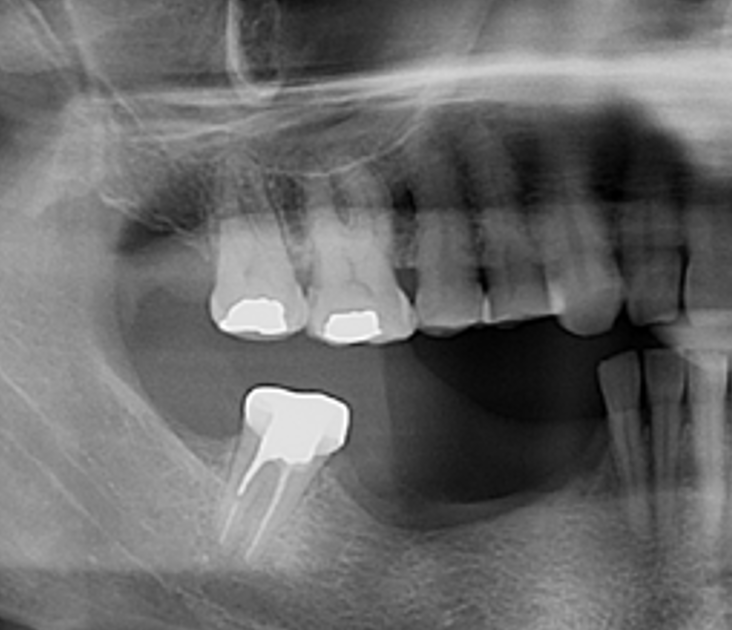
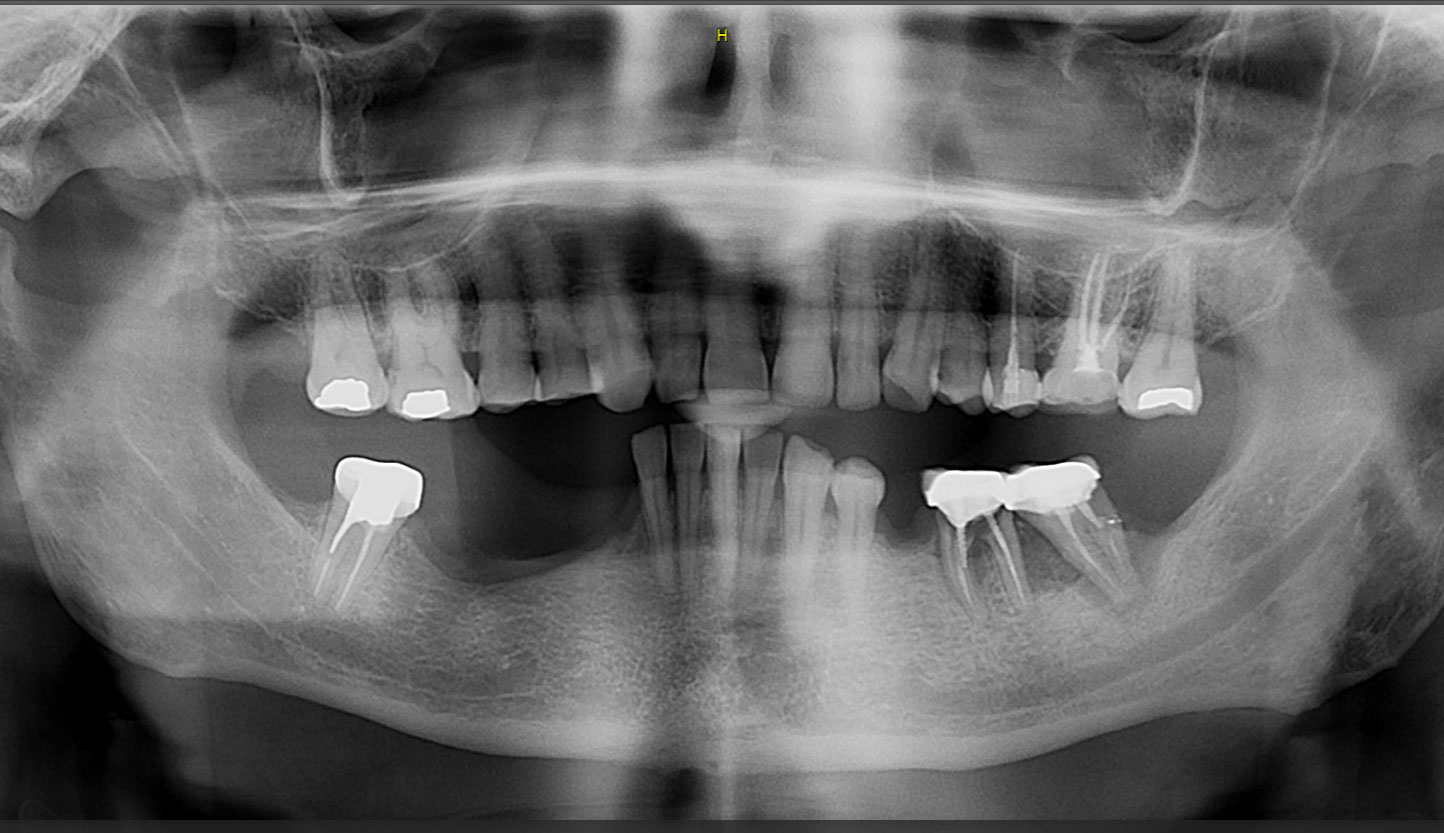
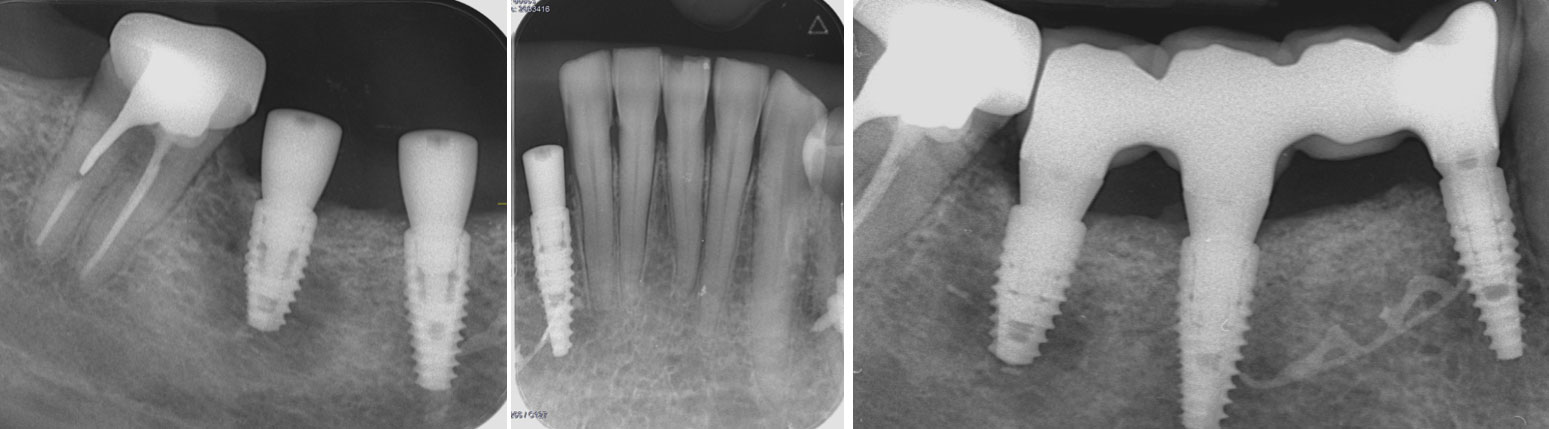
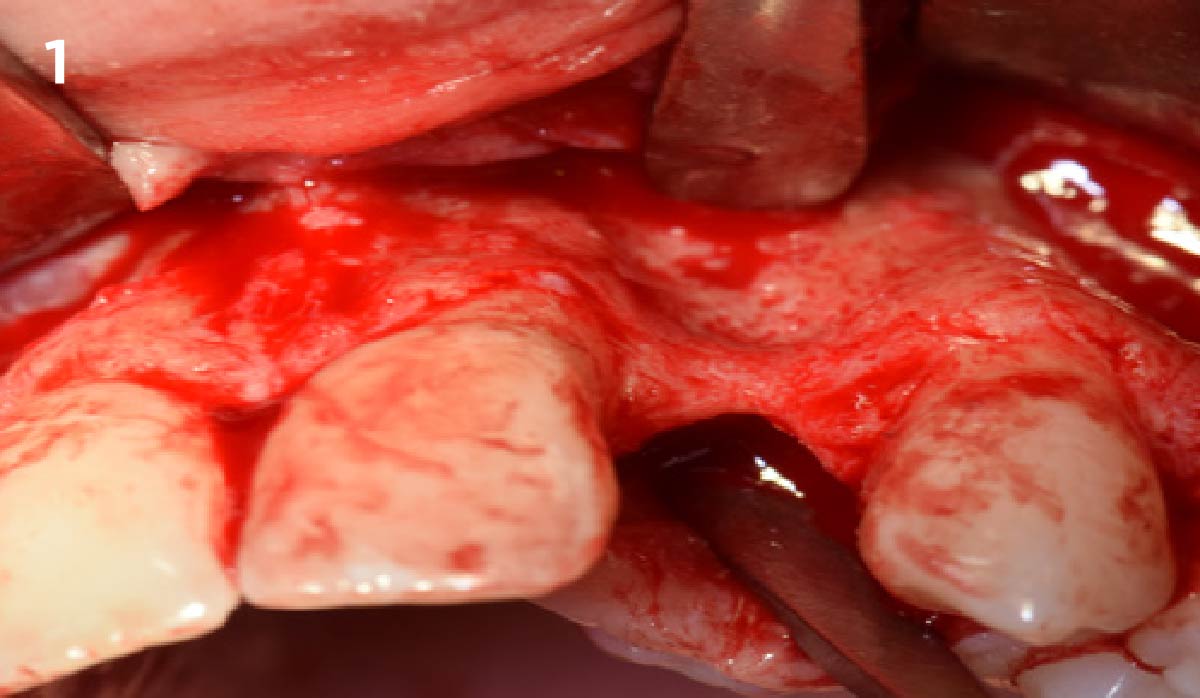
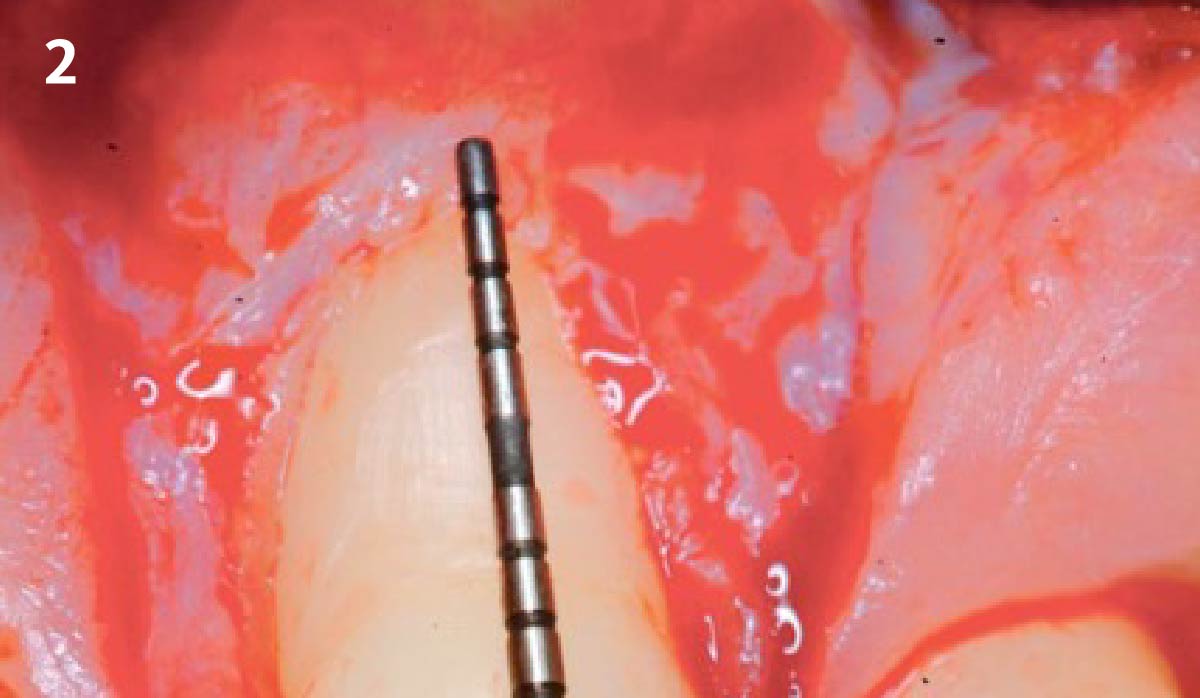
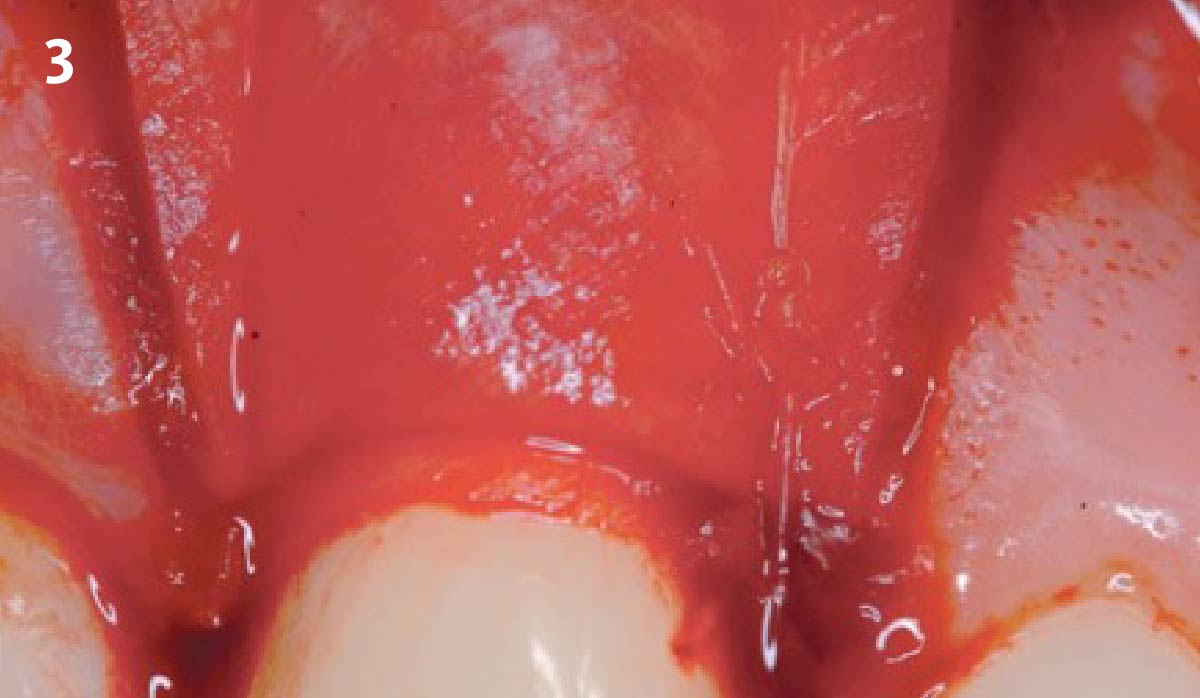
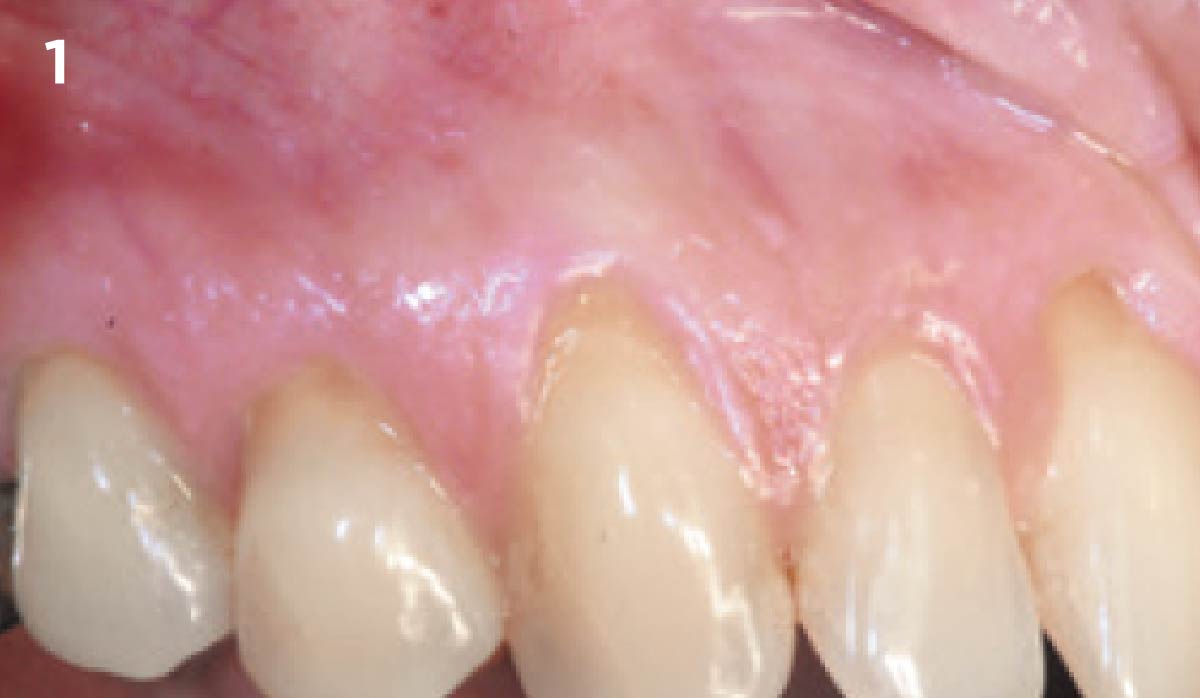
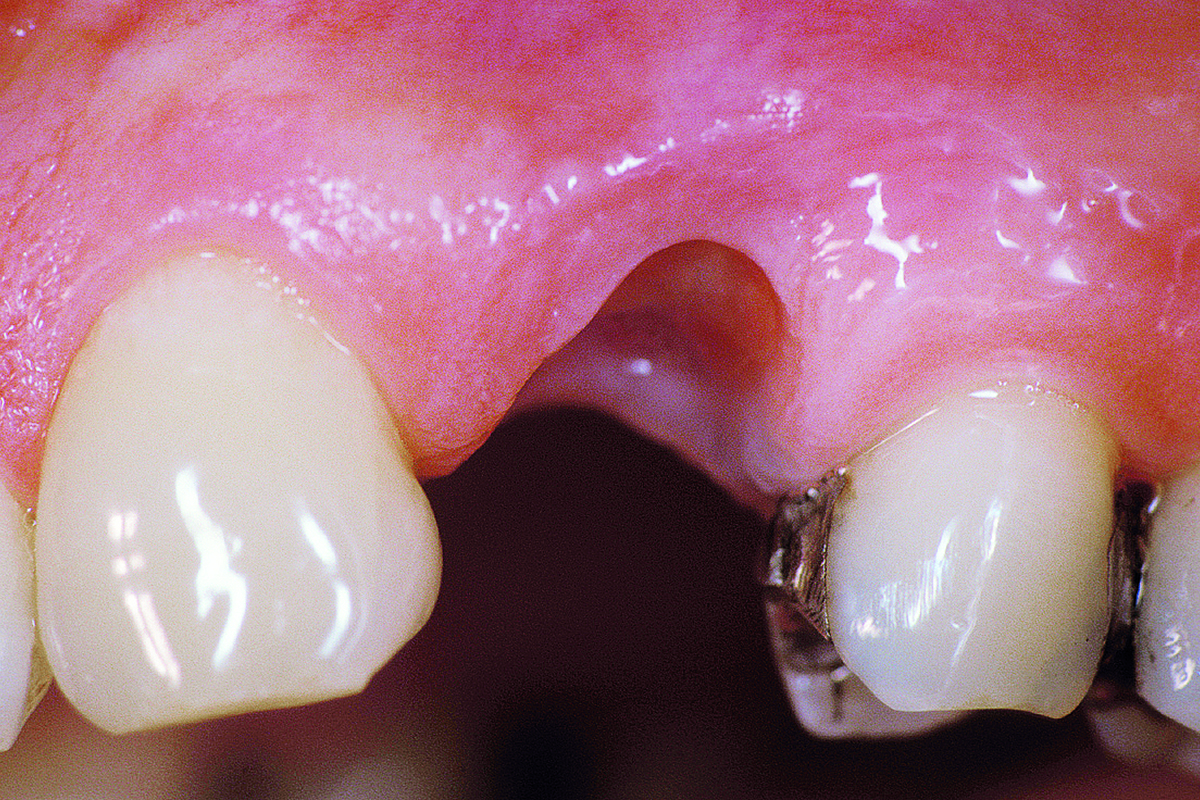
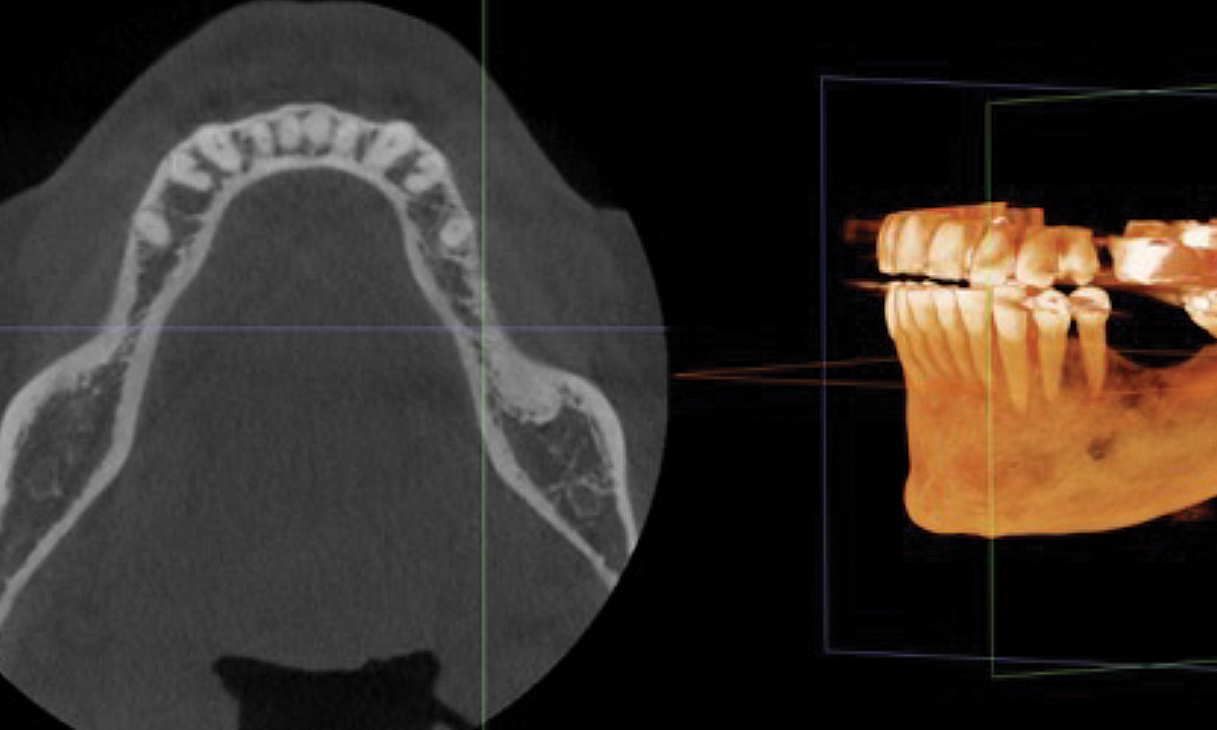
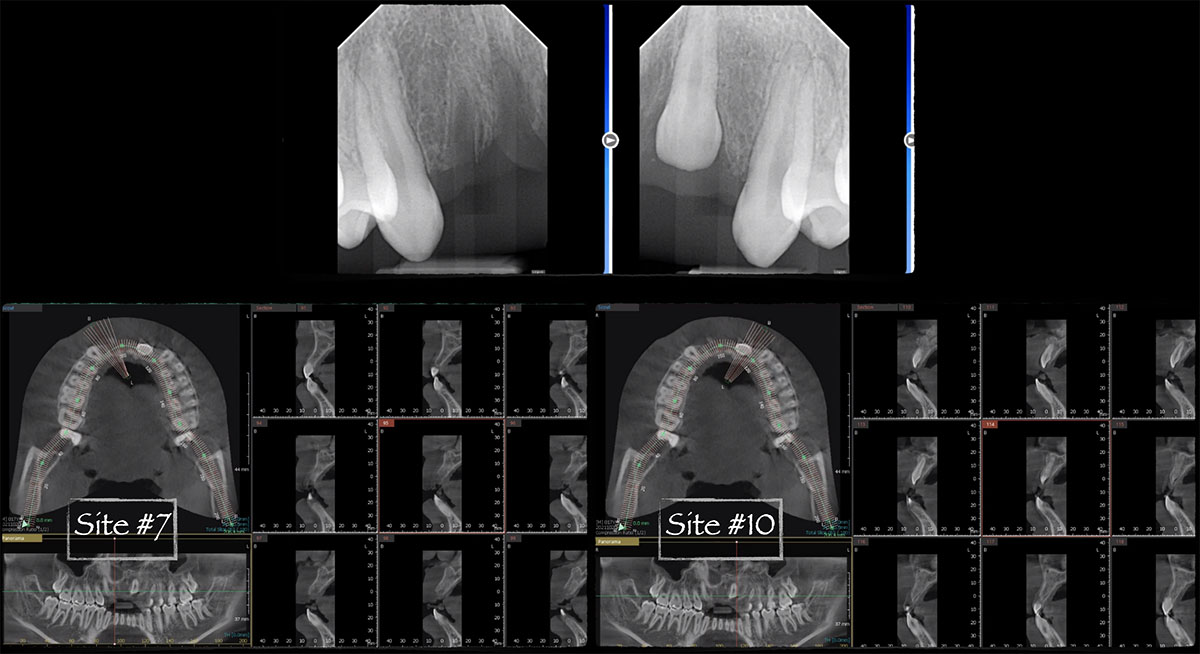
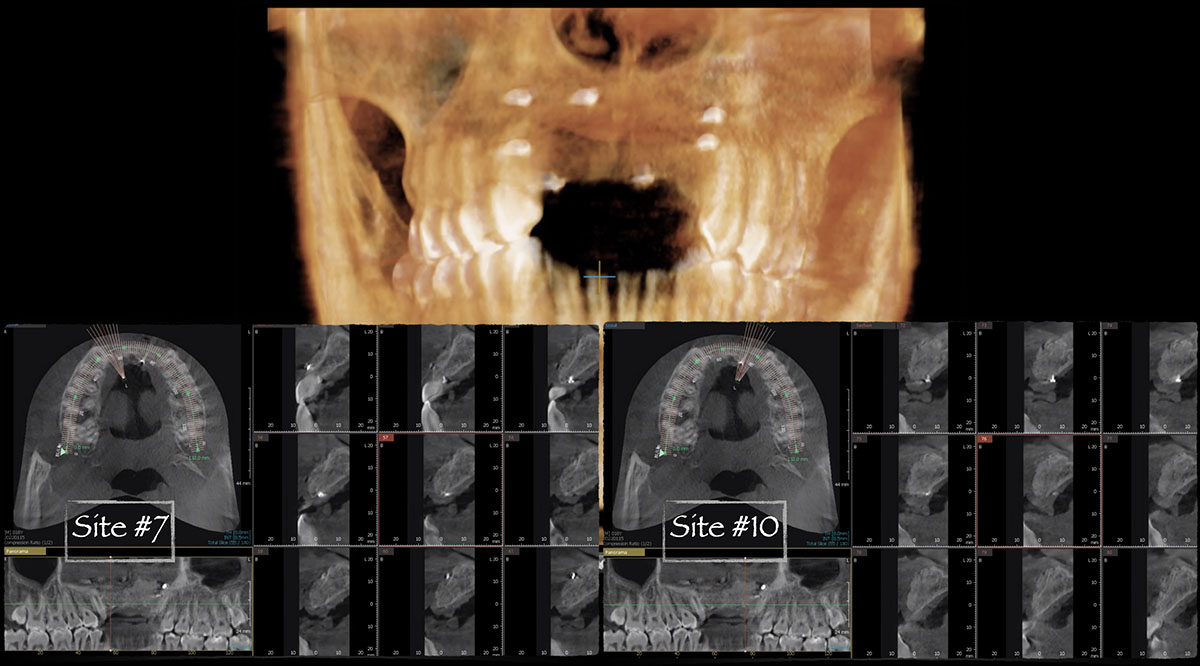
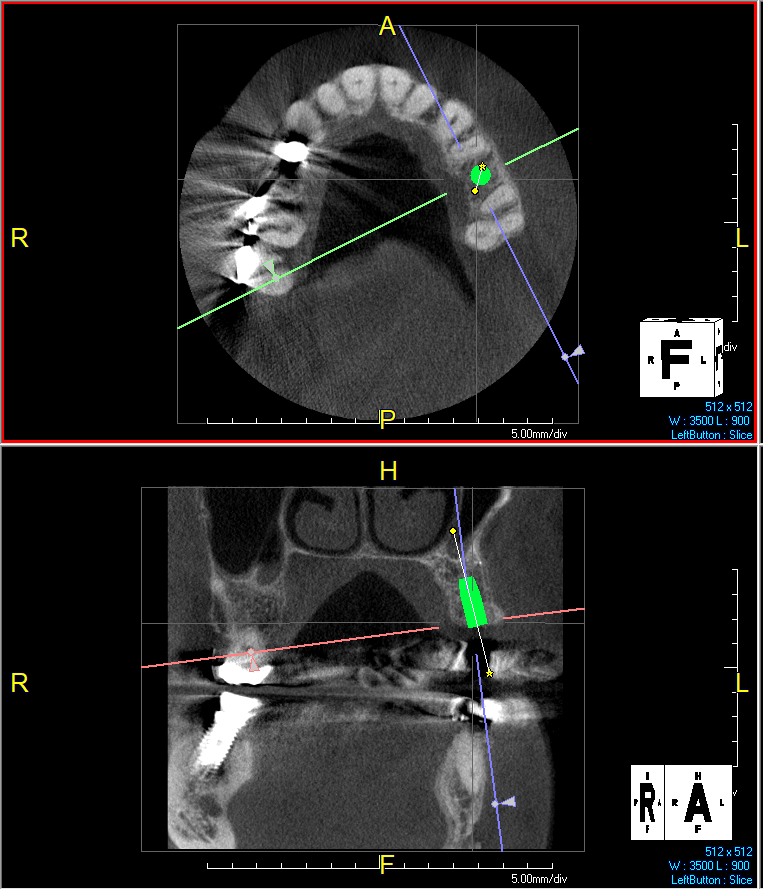
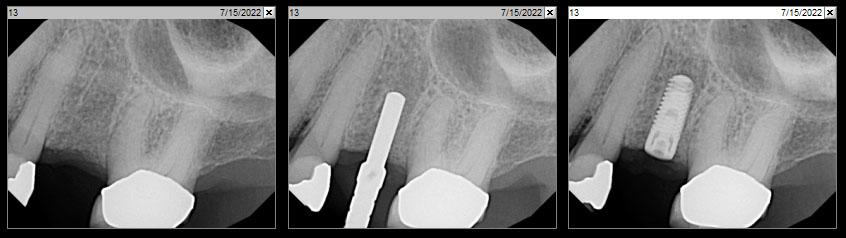
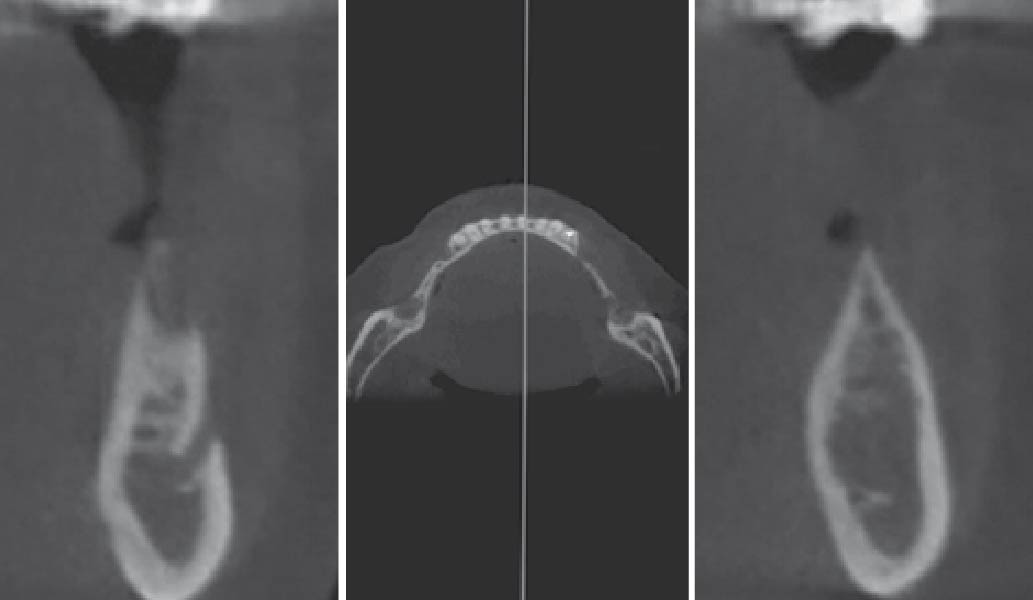
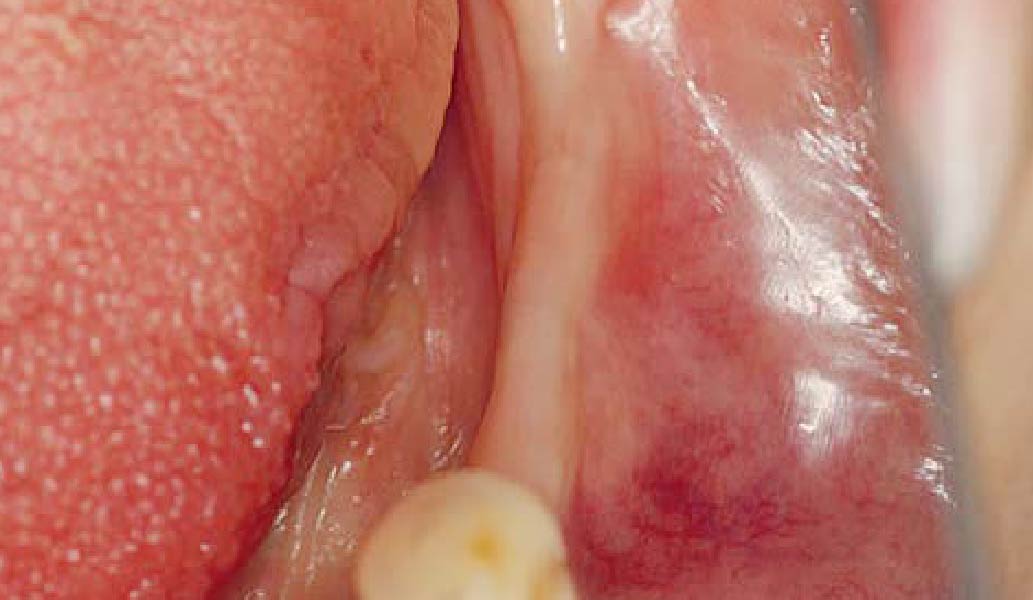
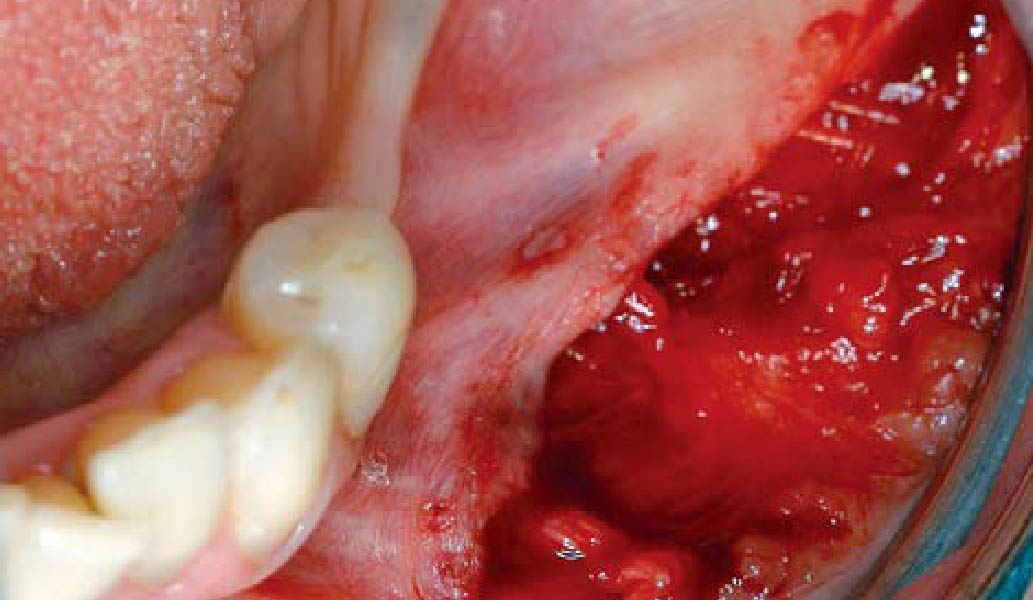
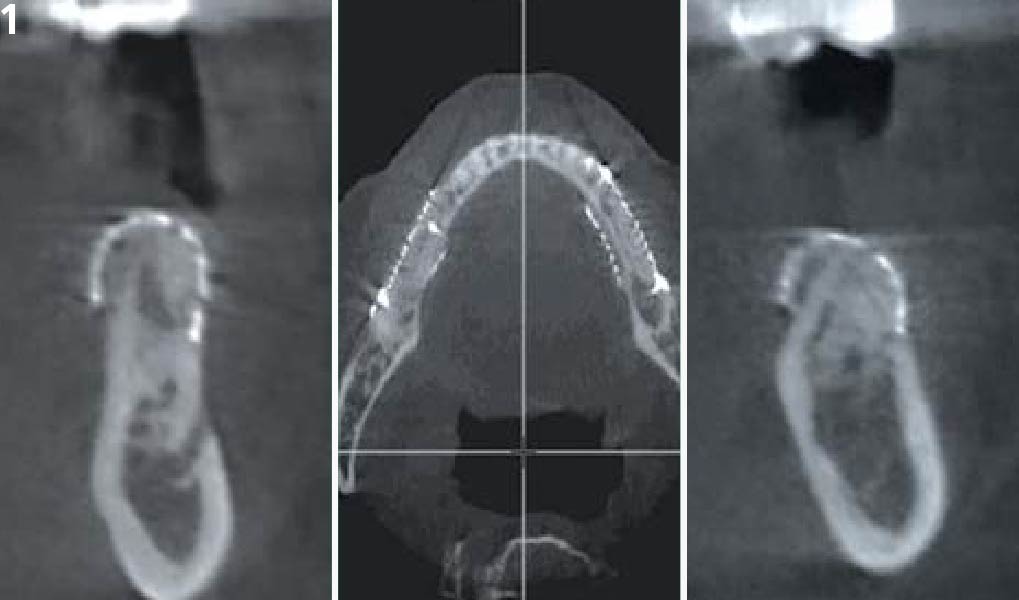
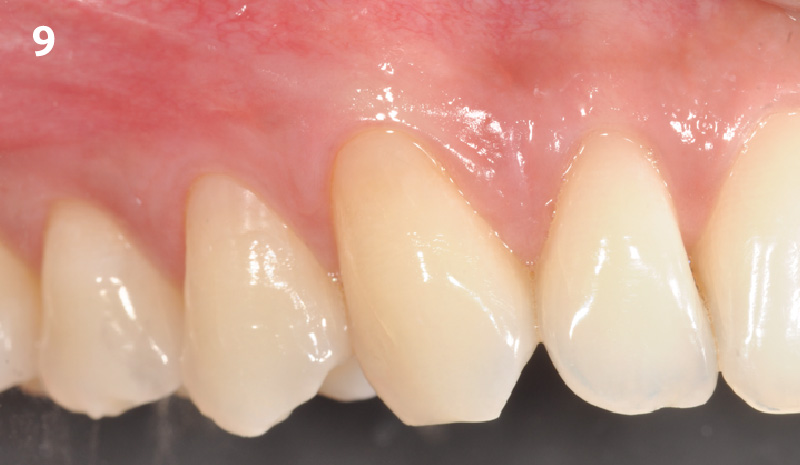
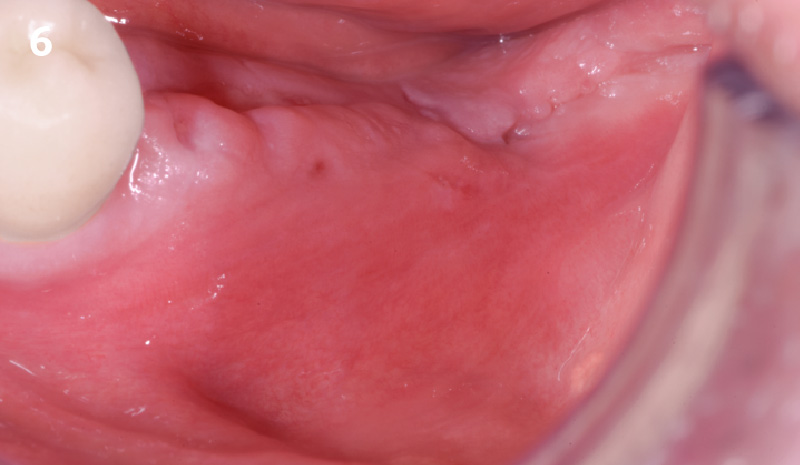
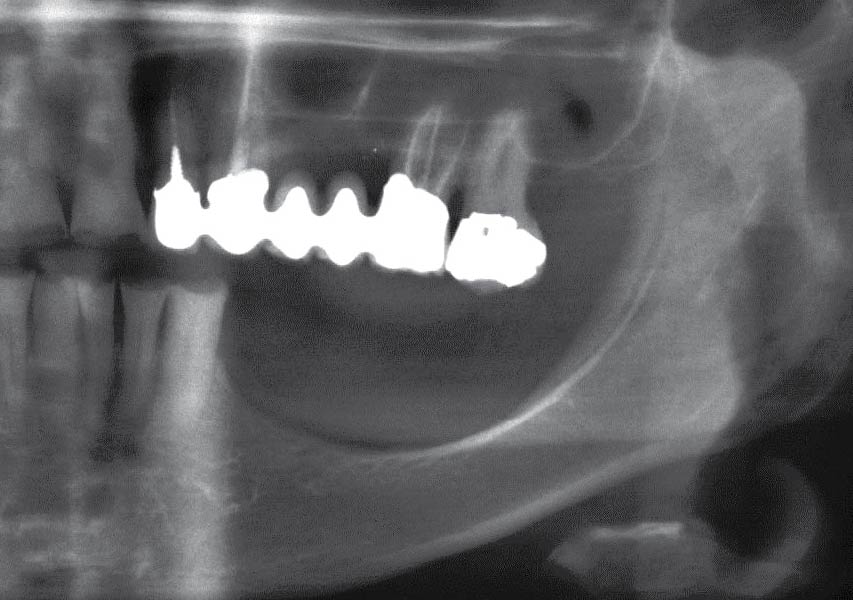
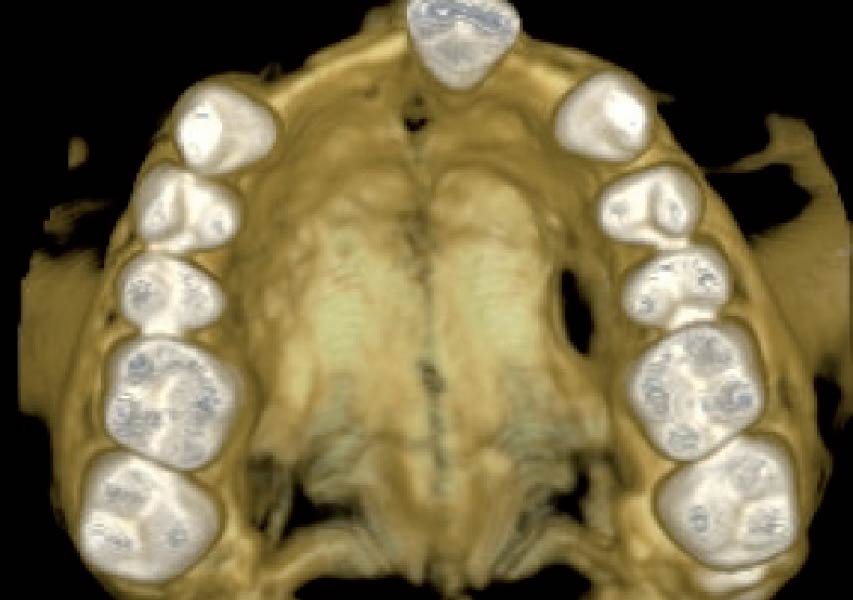
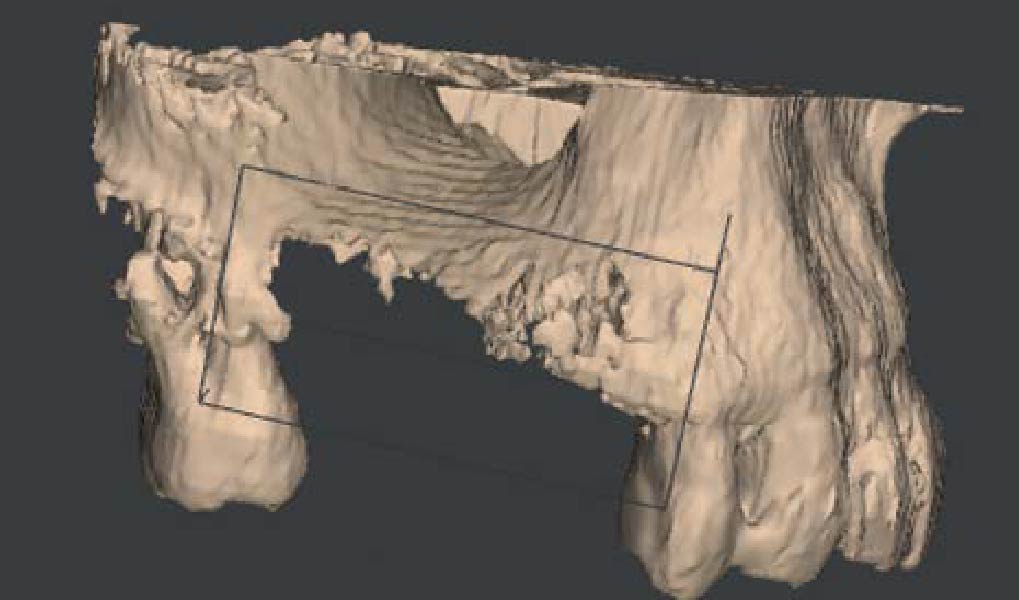
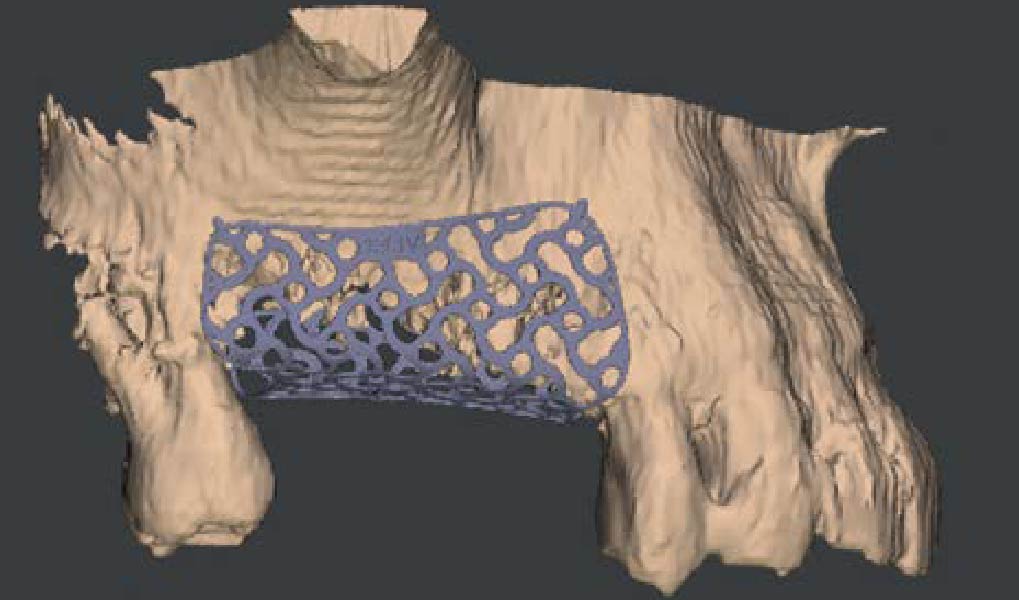
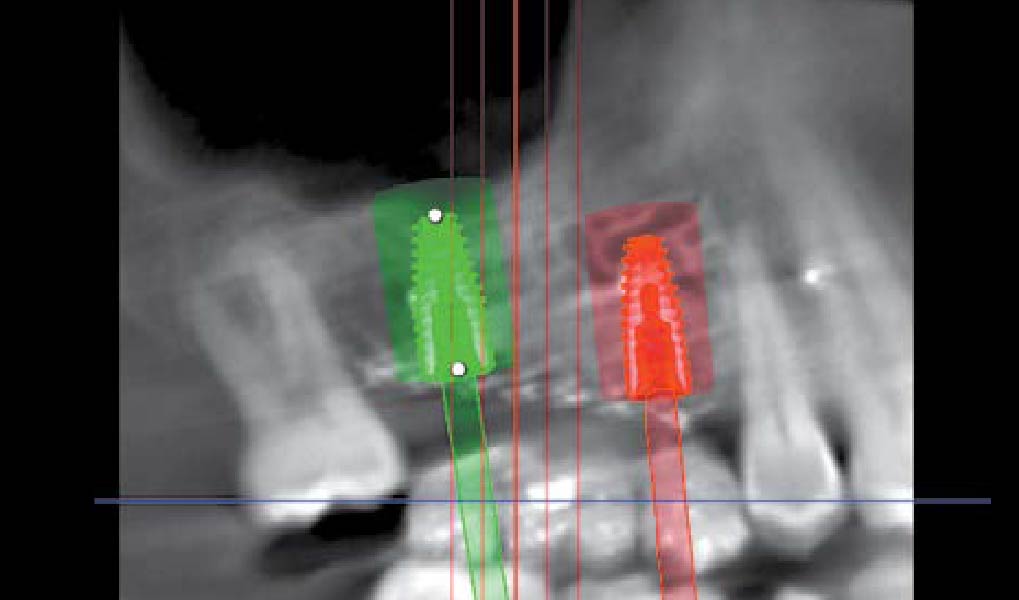
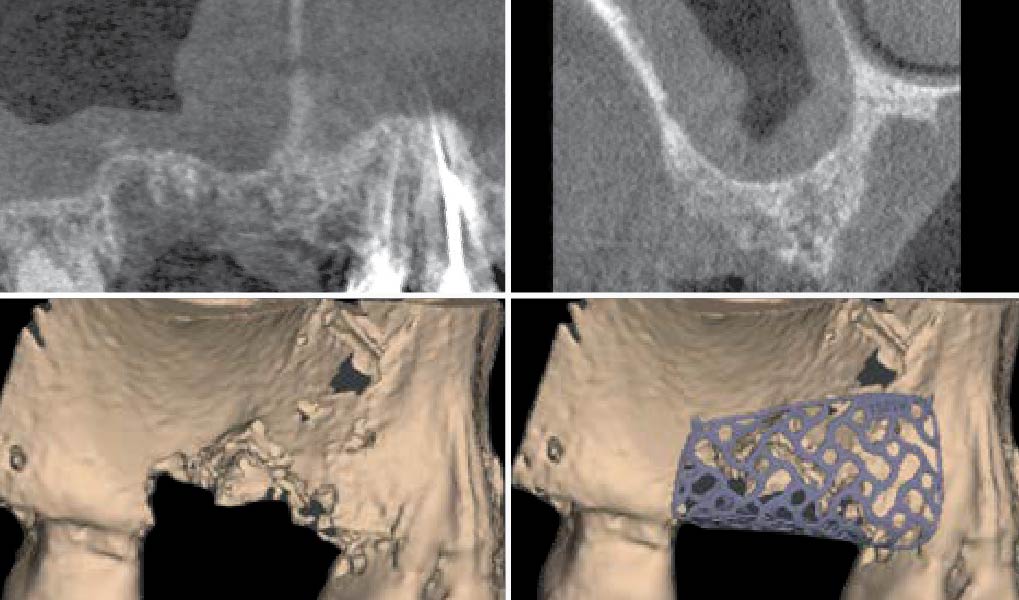
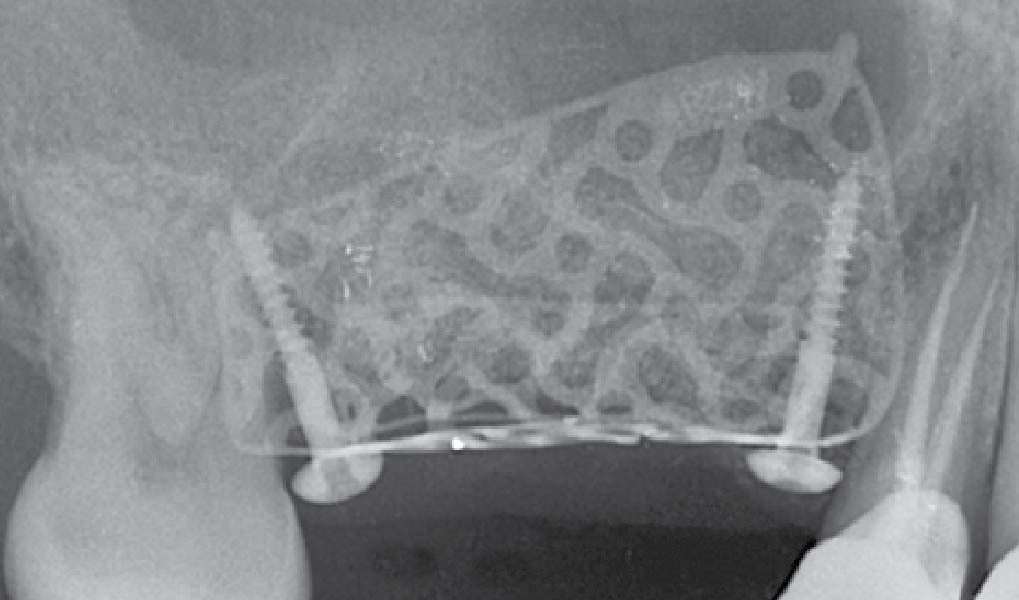
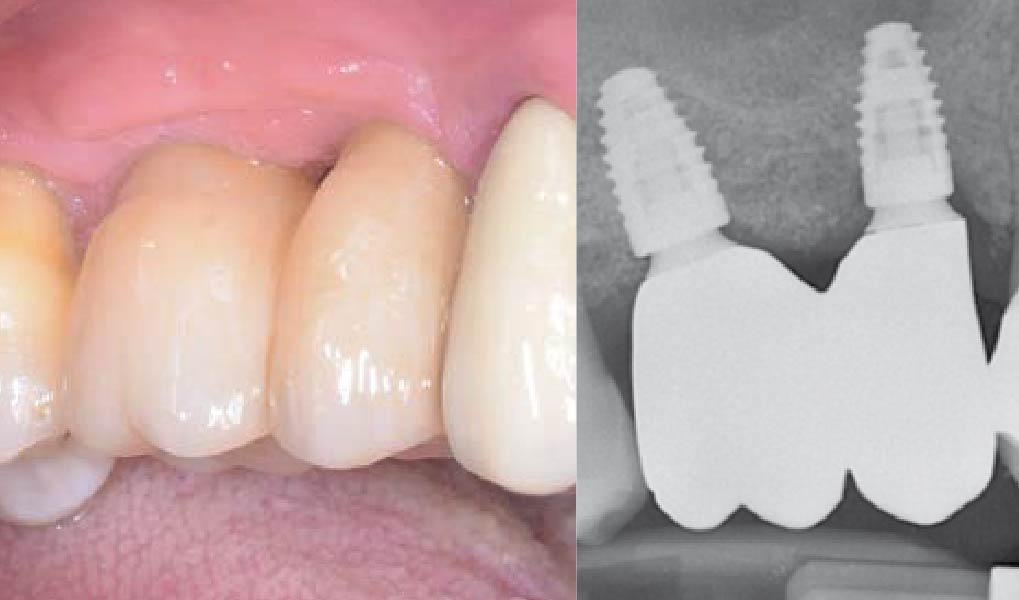
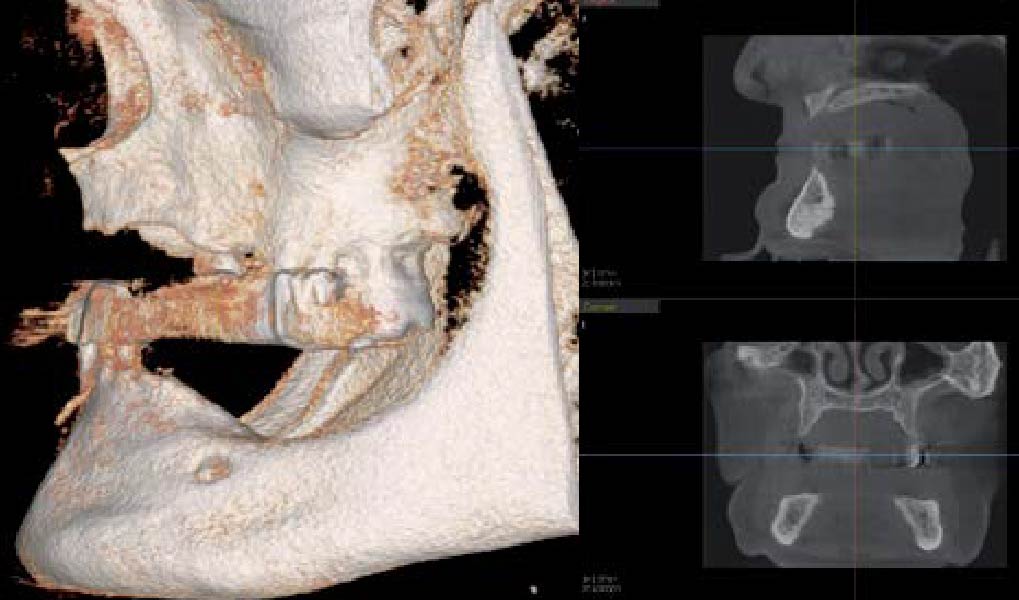
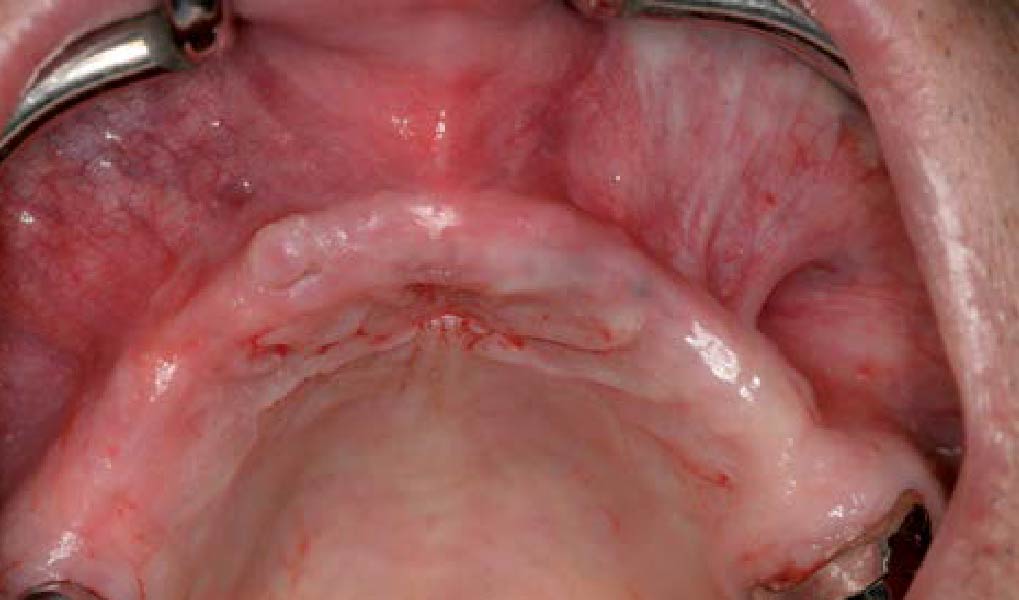
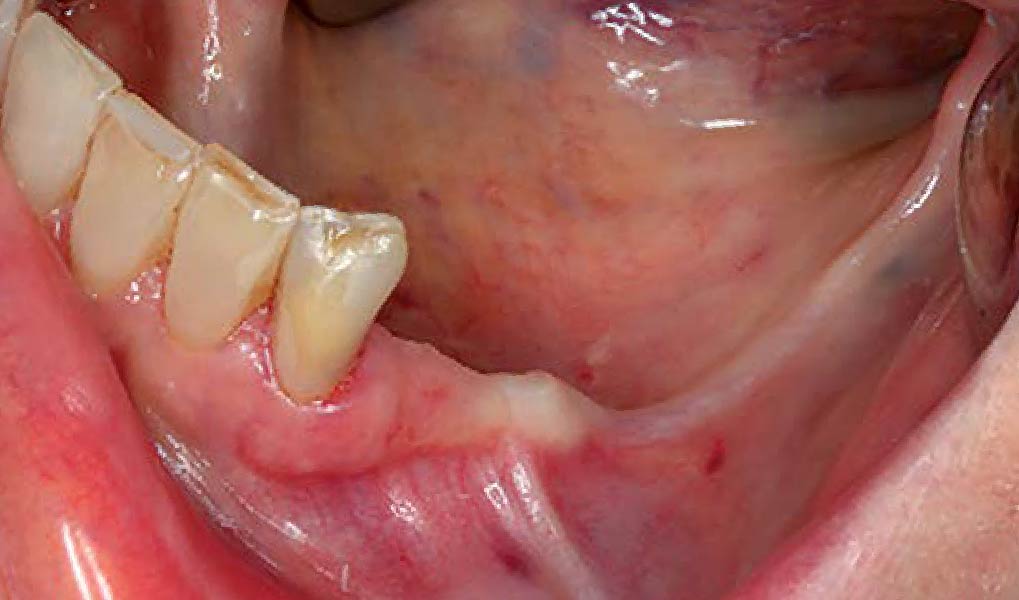
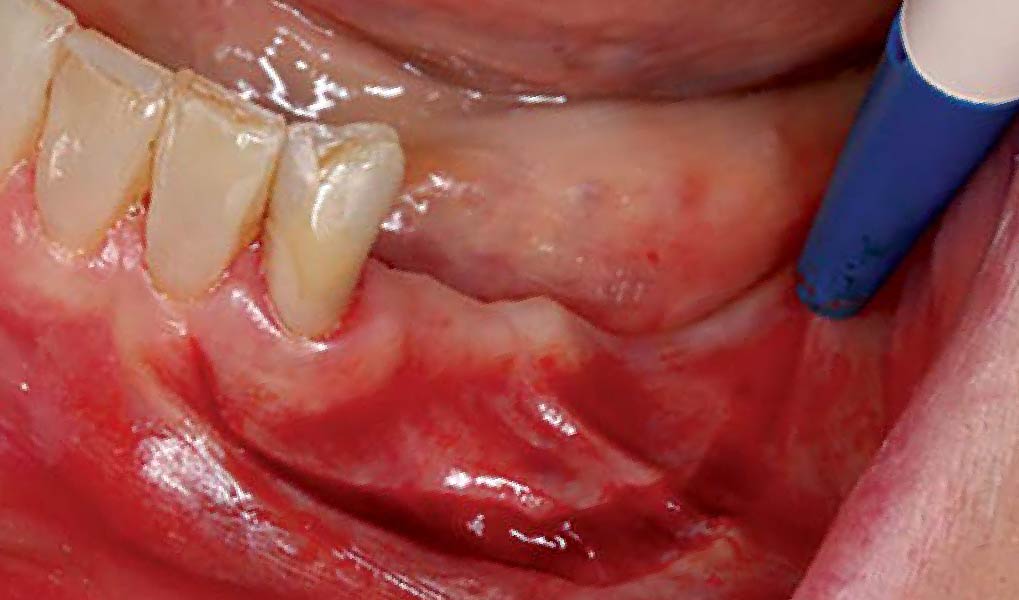
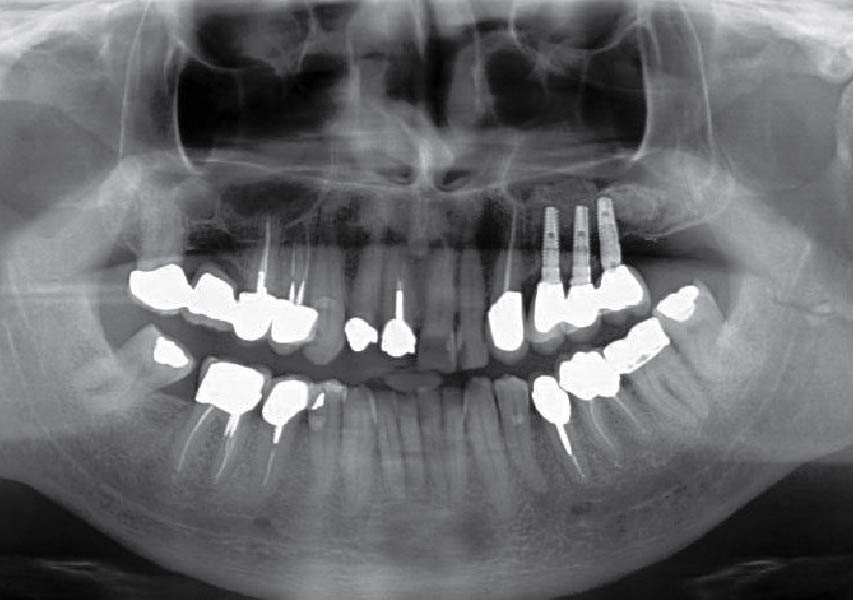
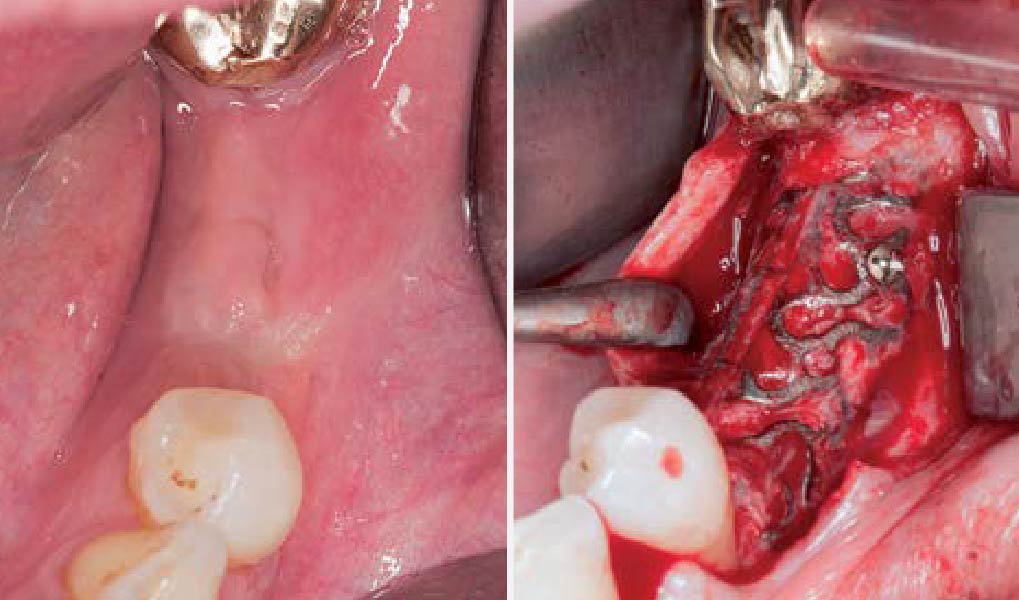
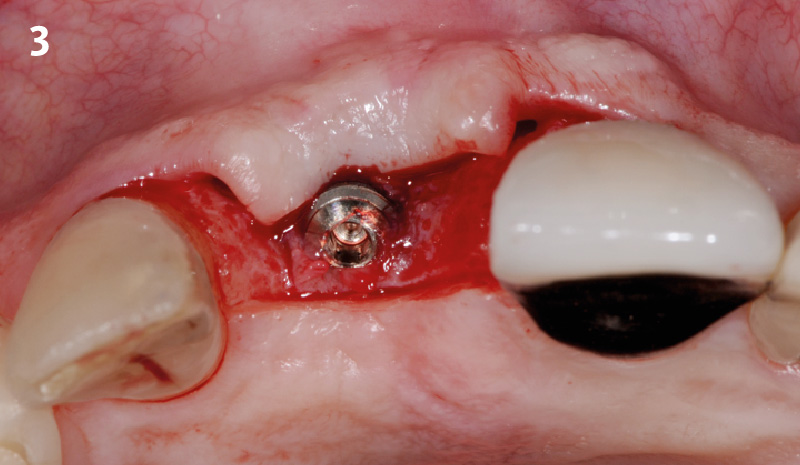
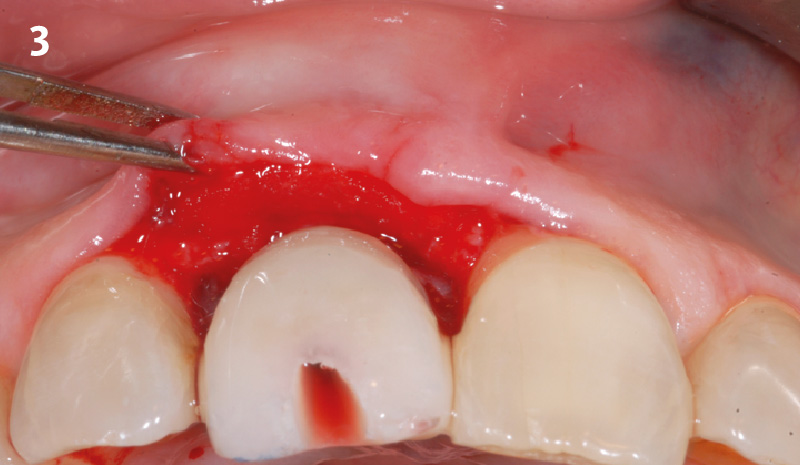
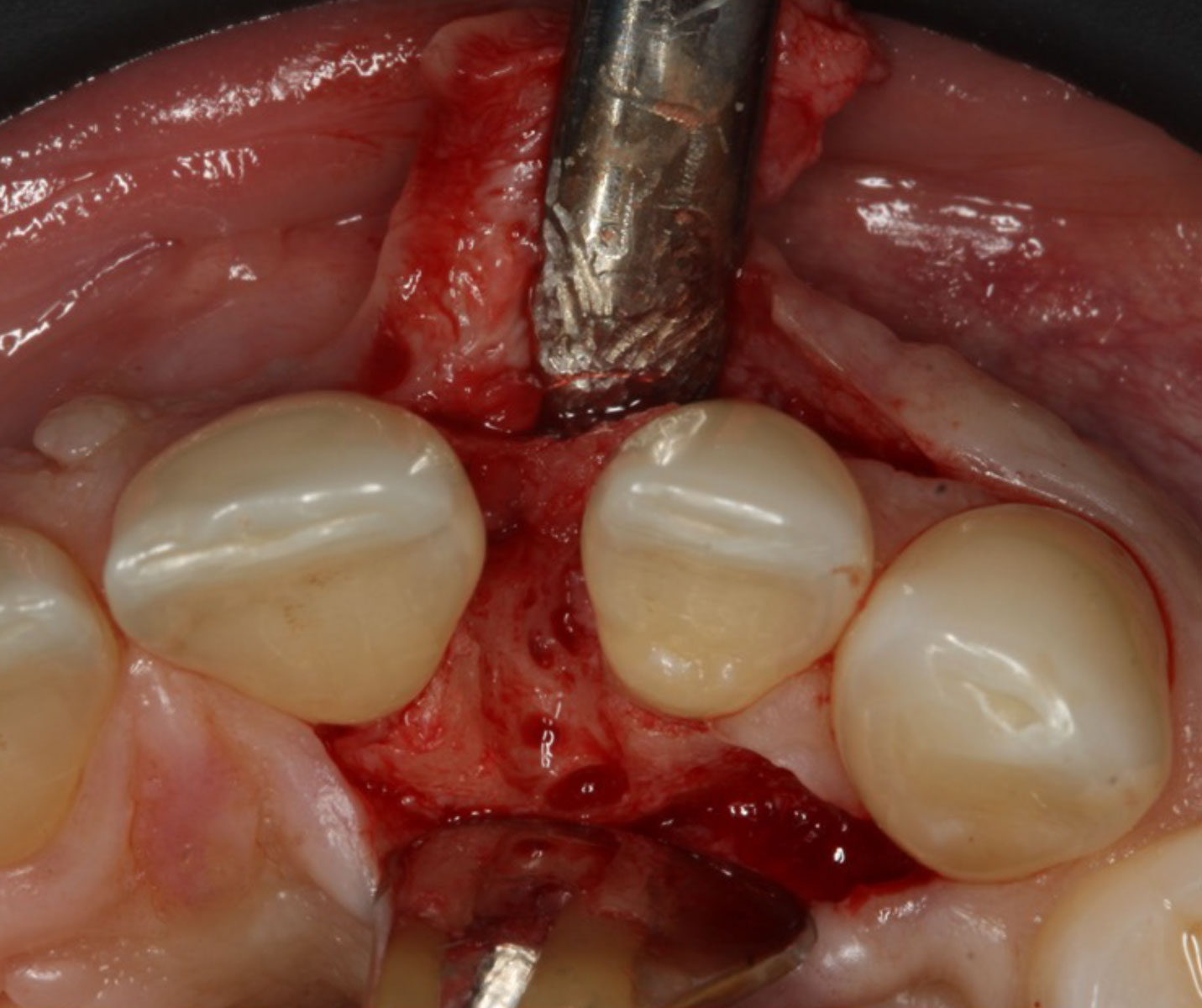
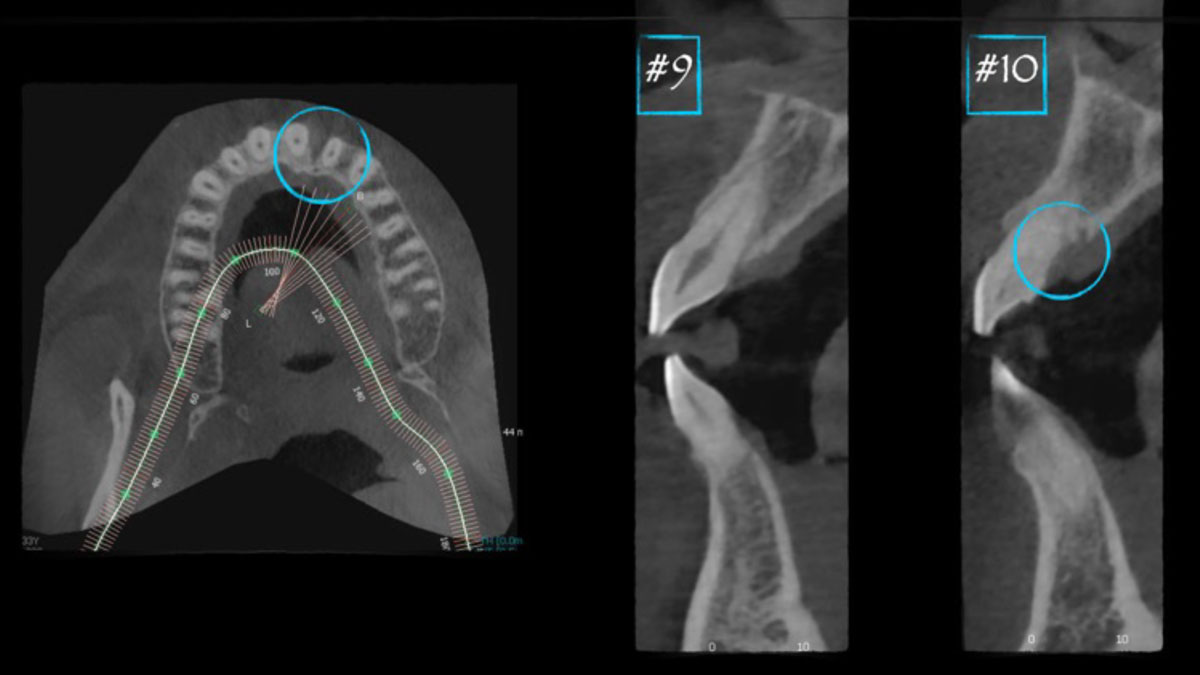
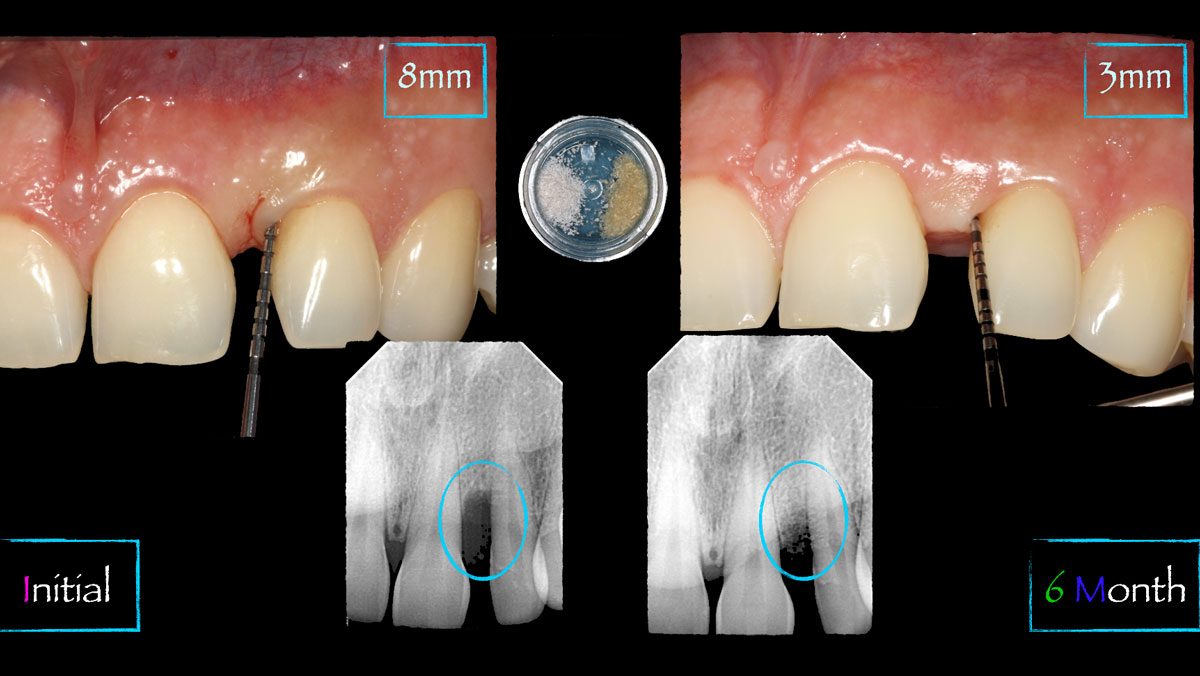
A 34-year-old healthy male presented with increased spacing between maxillary left central and lateral incisors. Clinical examination showed deep probing depths between #9-10 area. Cone-beam computed tomography (CBCT) showed vertical bone loss #9-10 wrapping around the palatal surfaces. Treatment recommendation included guided tissue regeneration (GTR) to stabilize the periodontium.
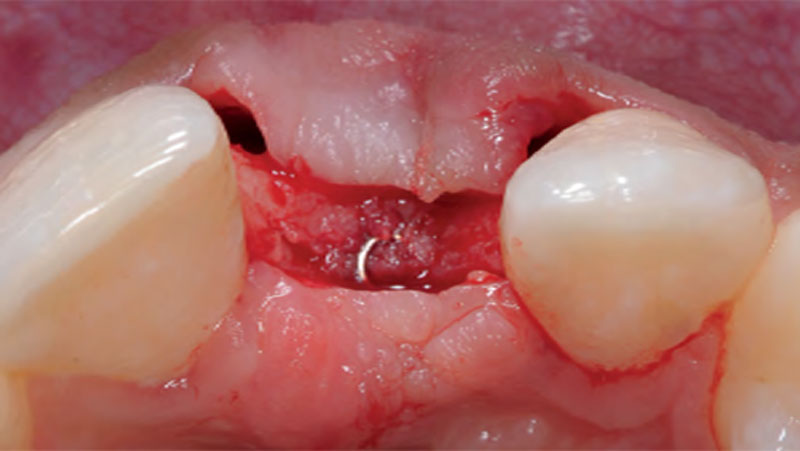
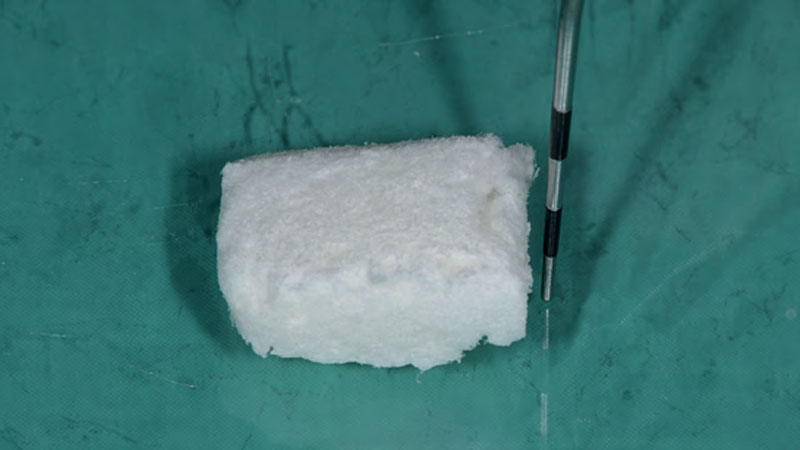
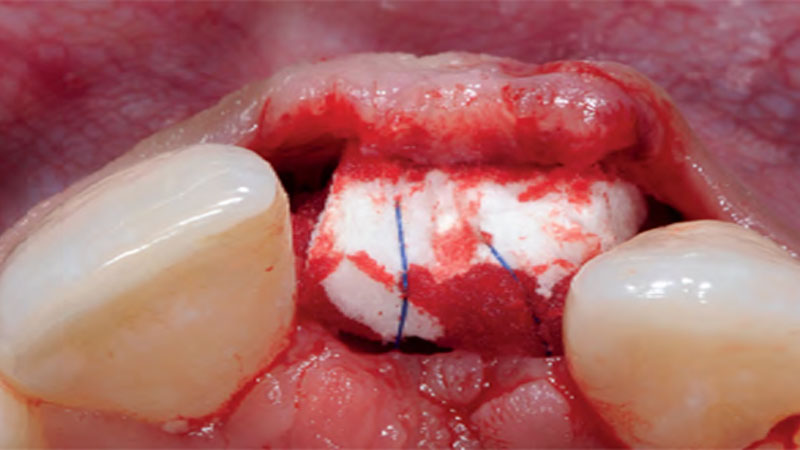
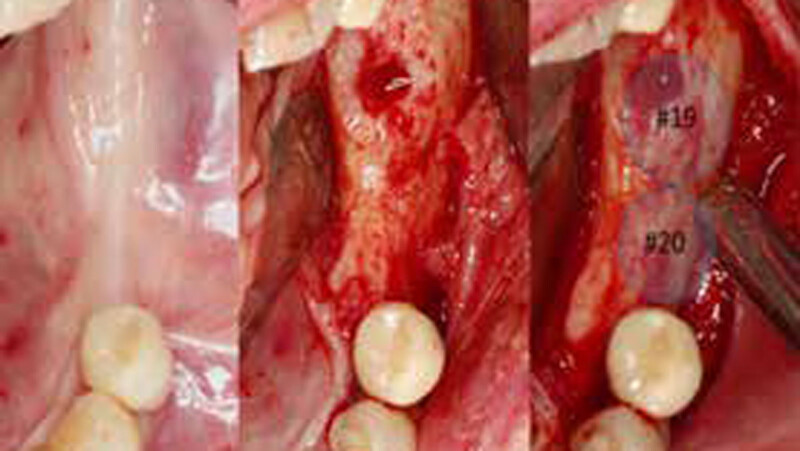
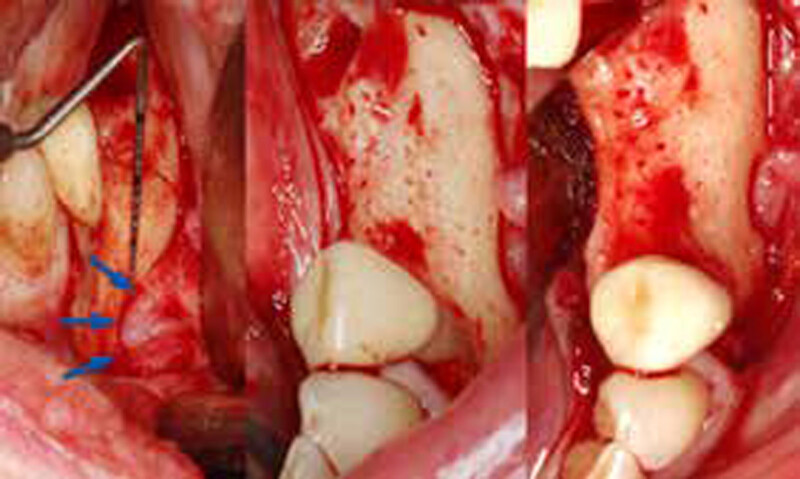
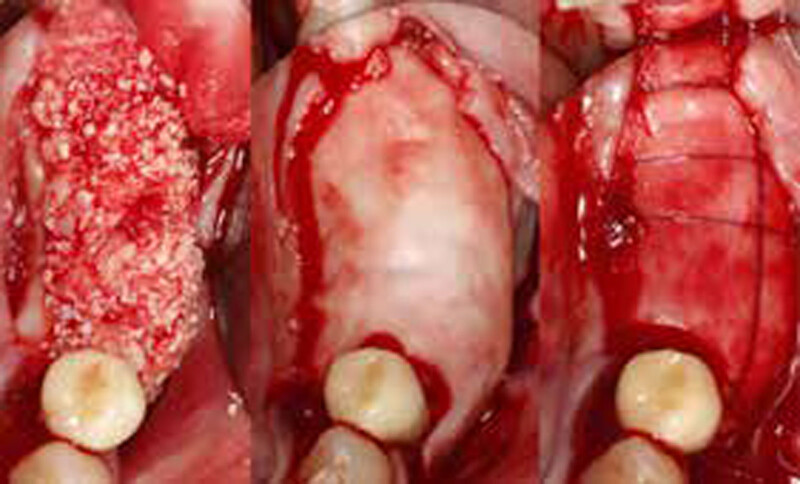
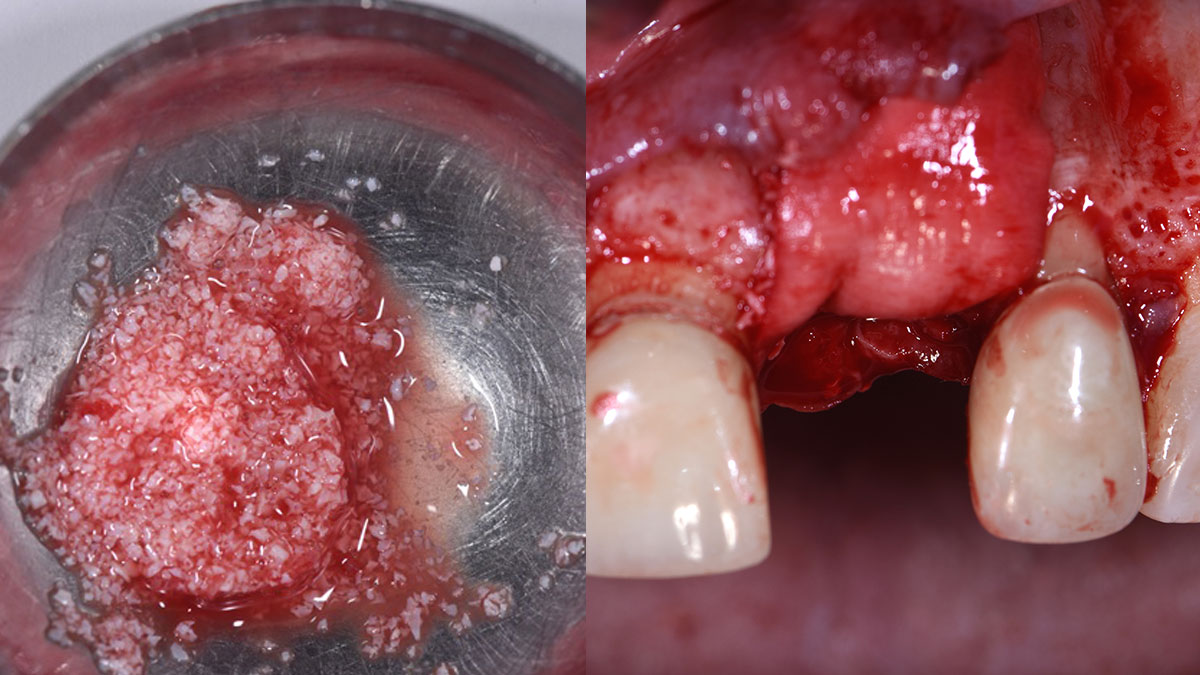
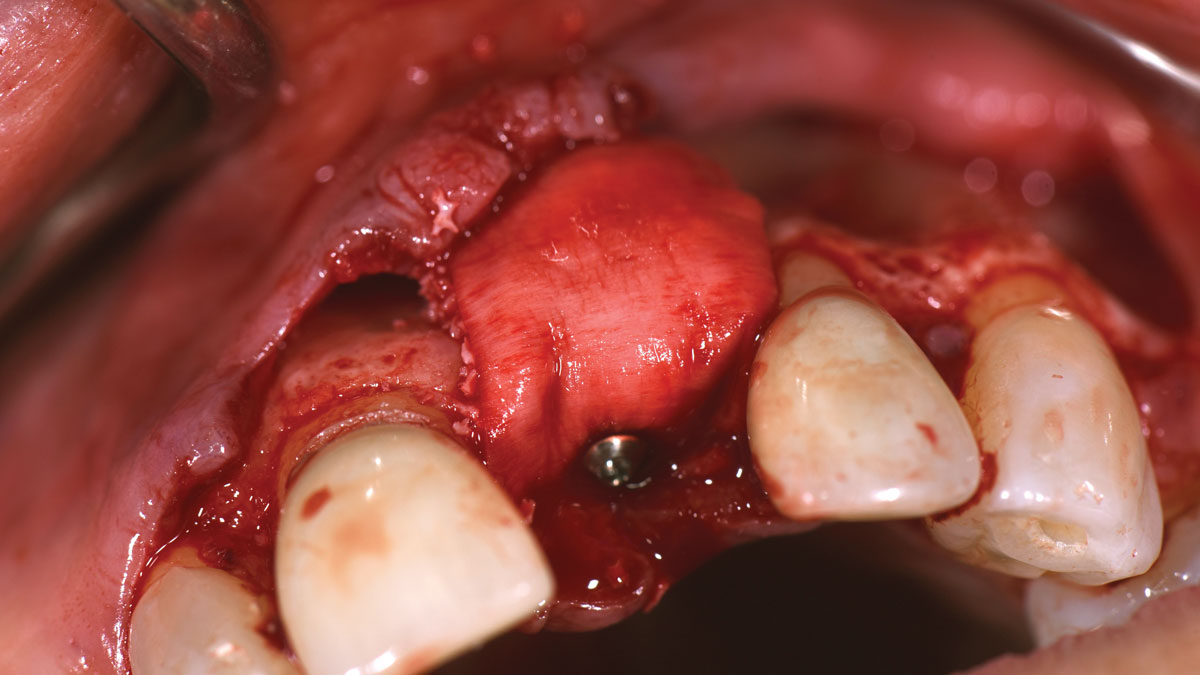
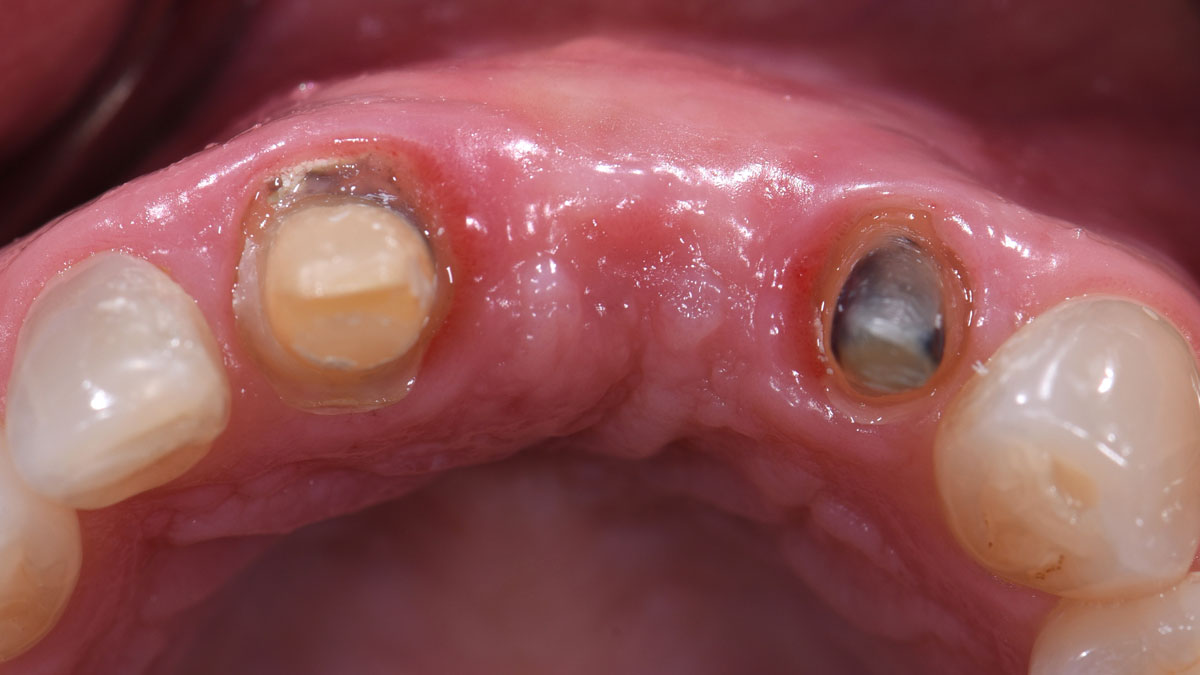
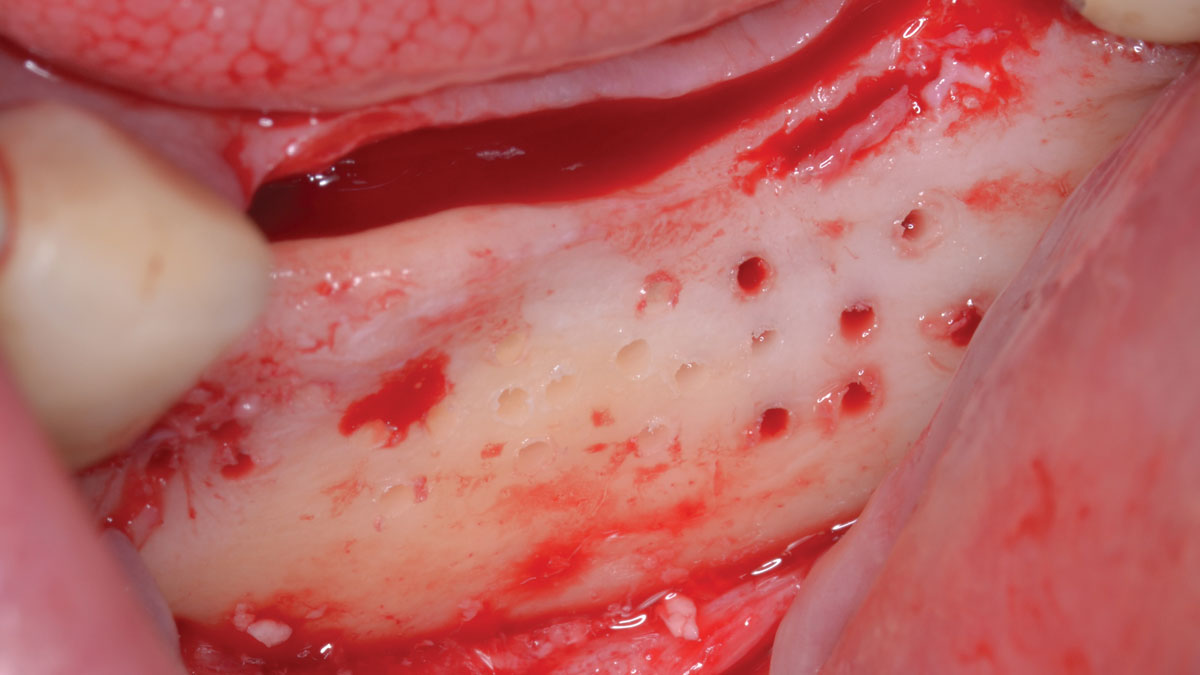
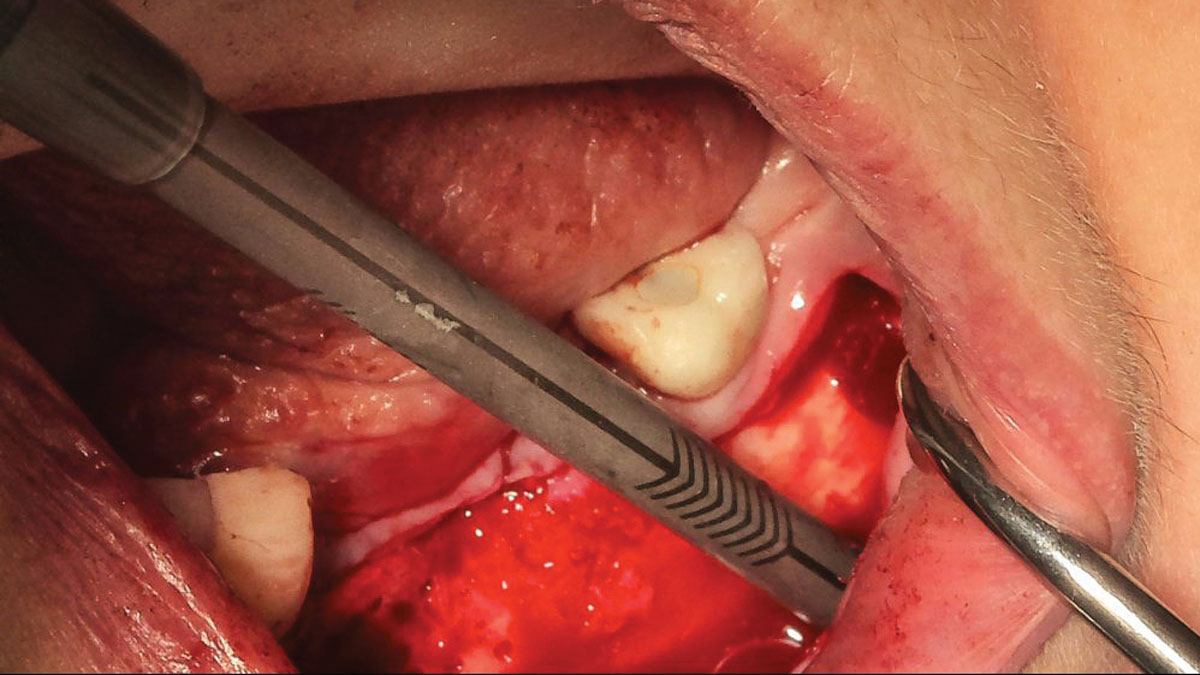
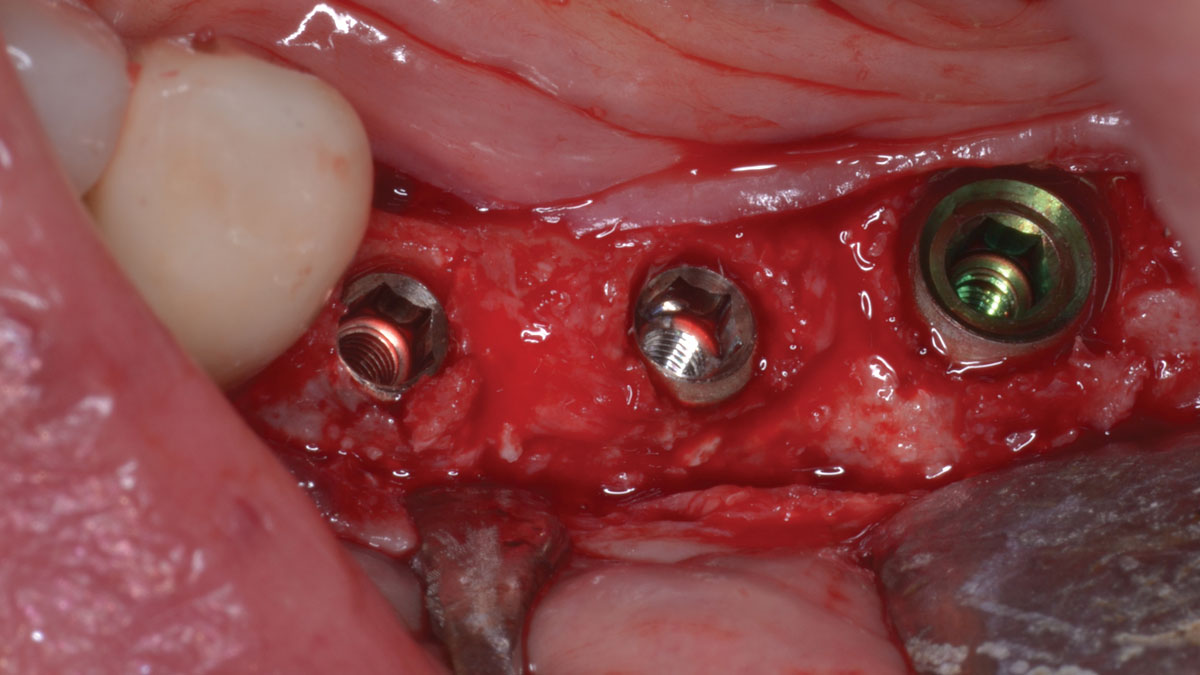
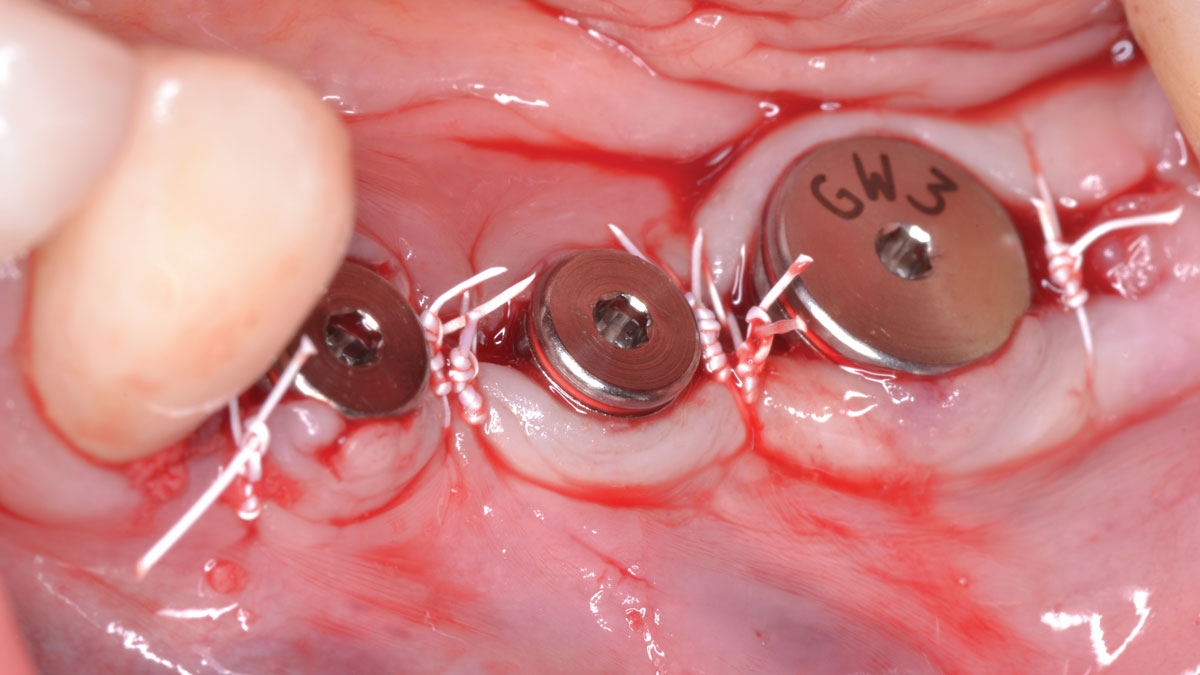
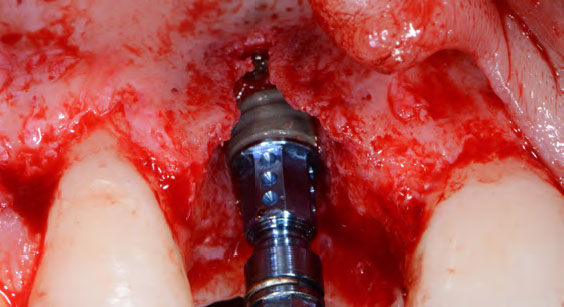
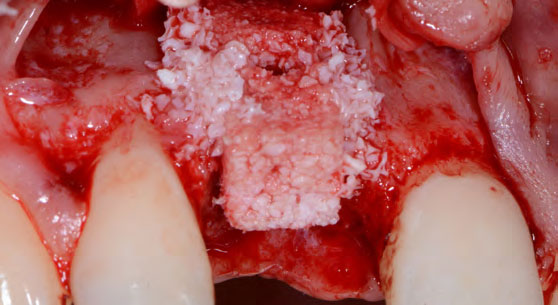
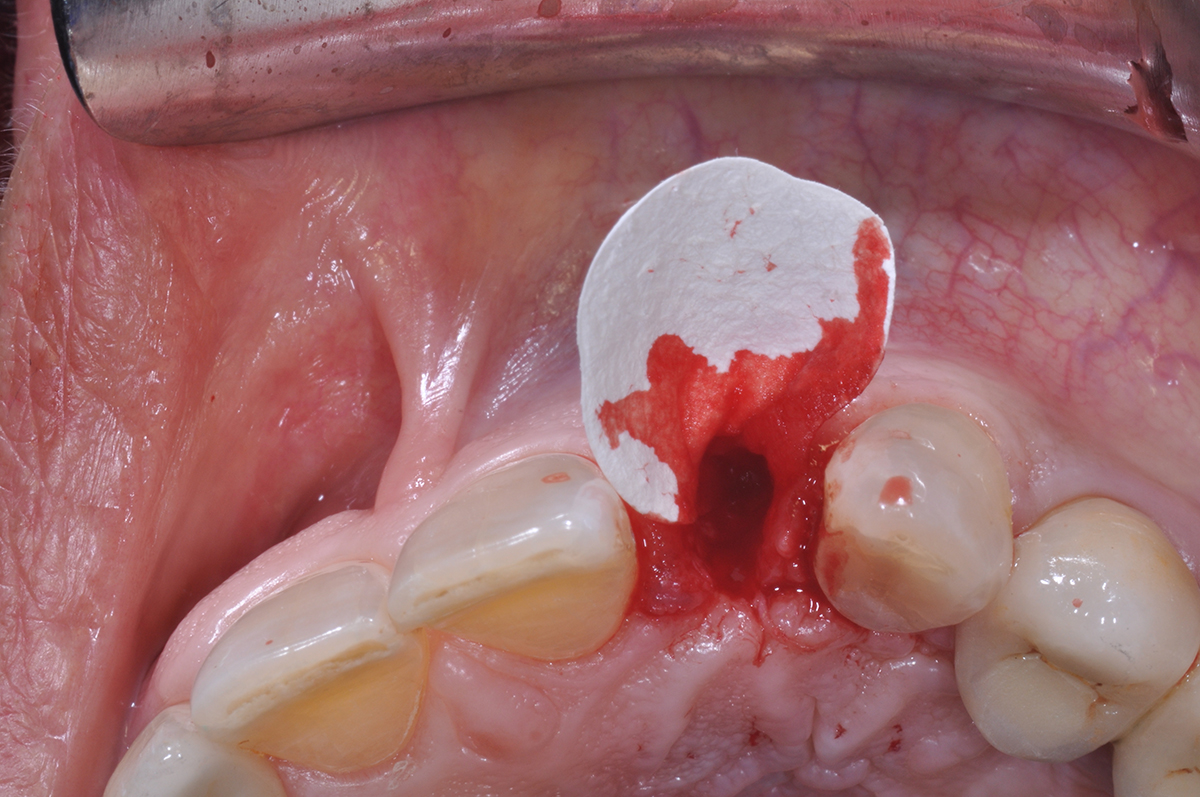
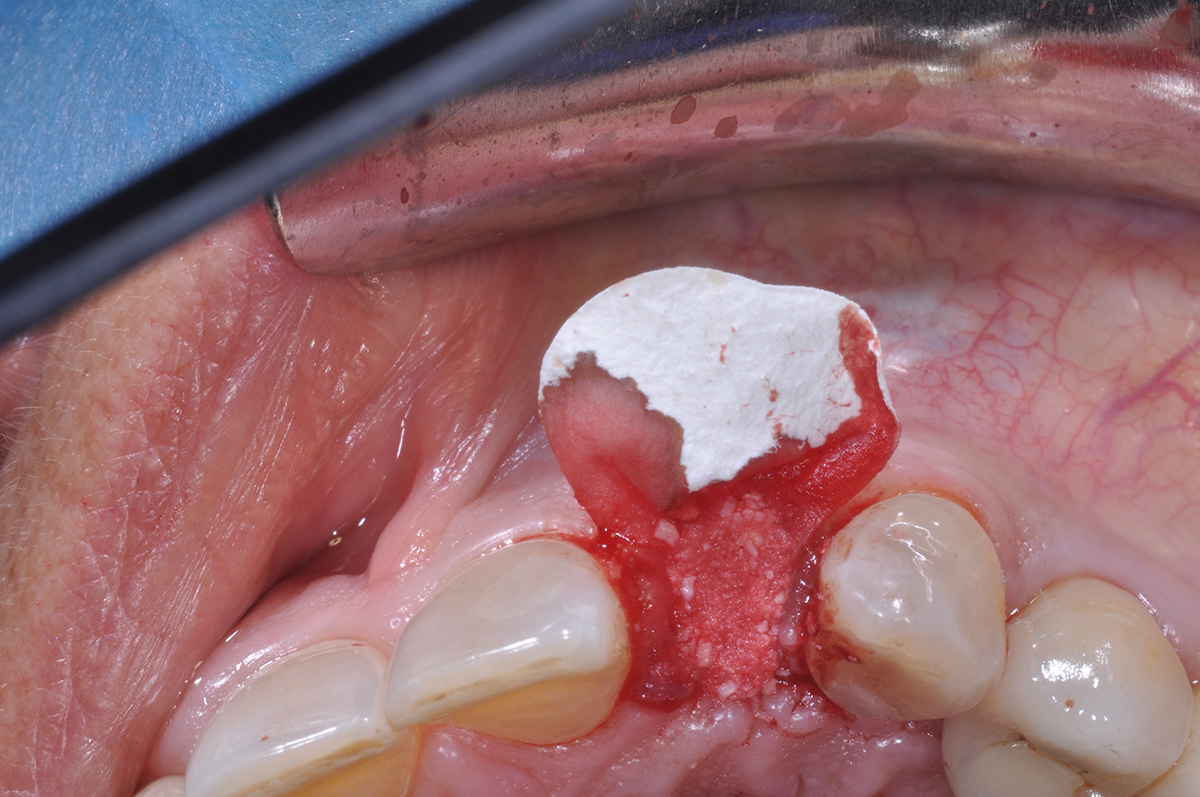
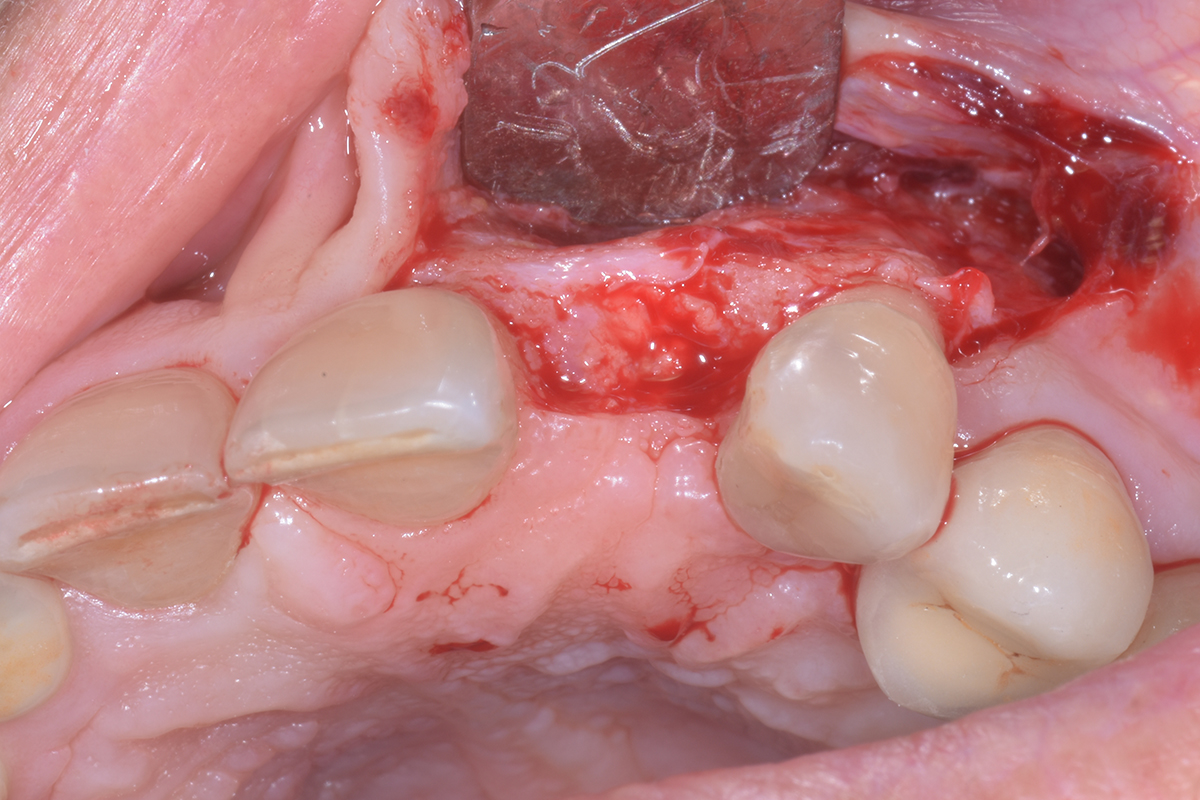
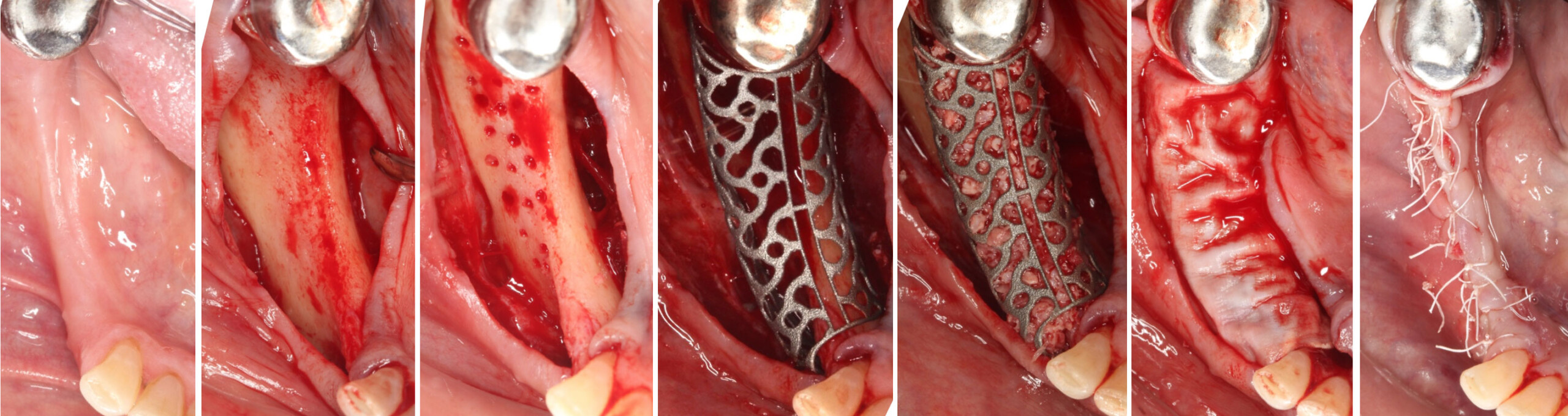
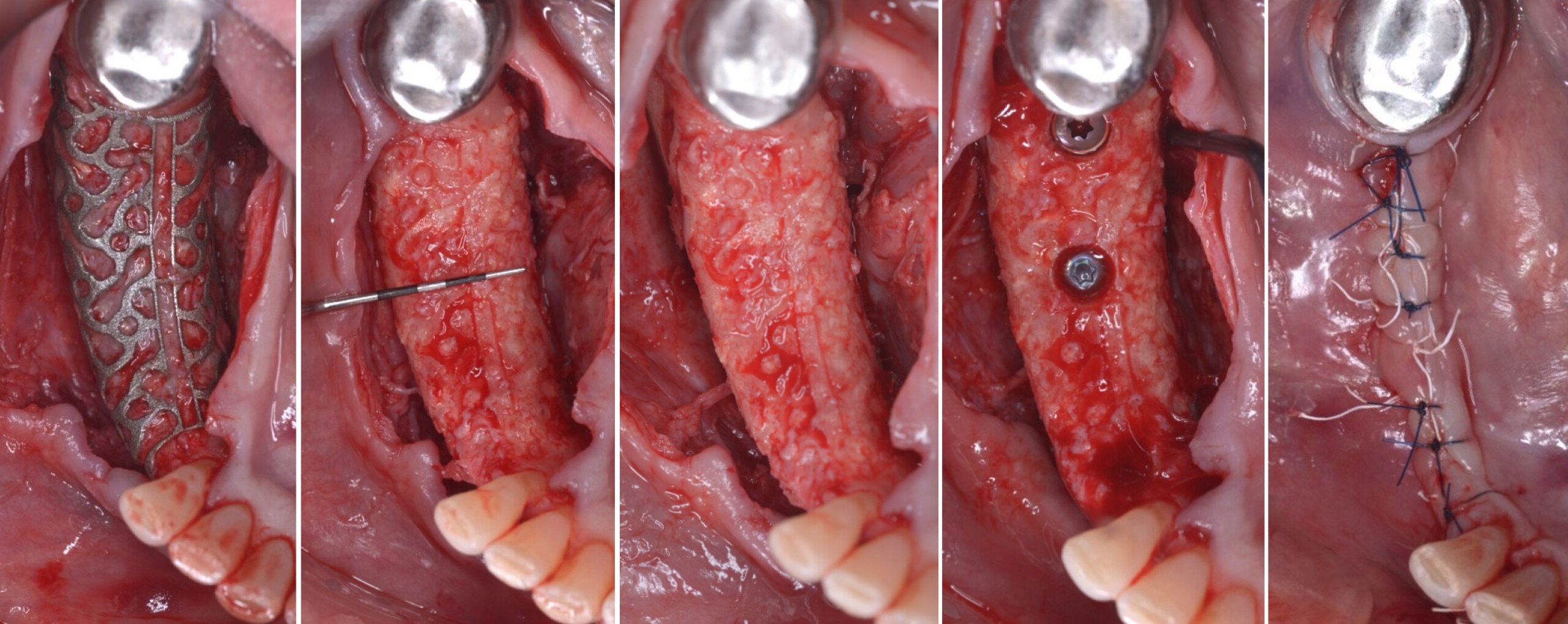
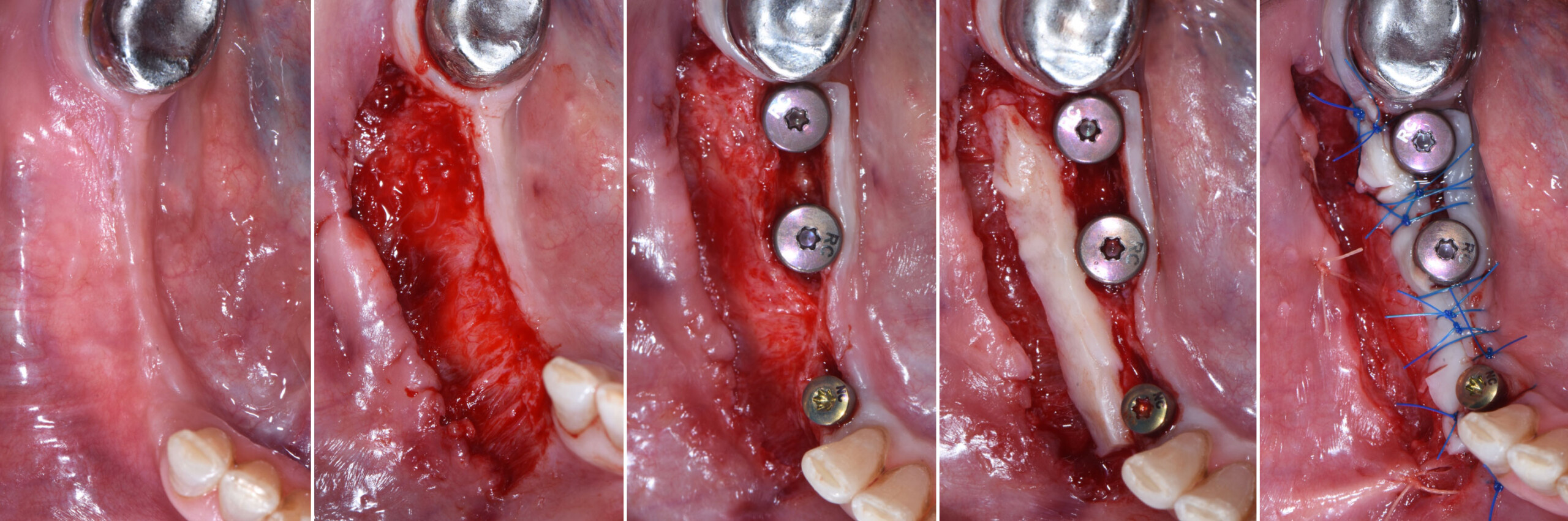
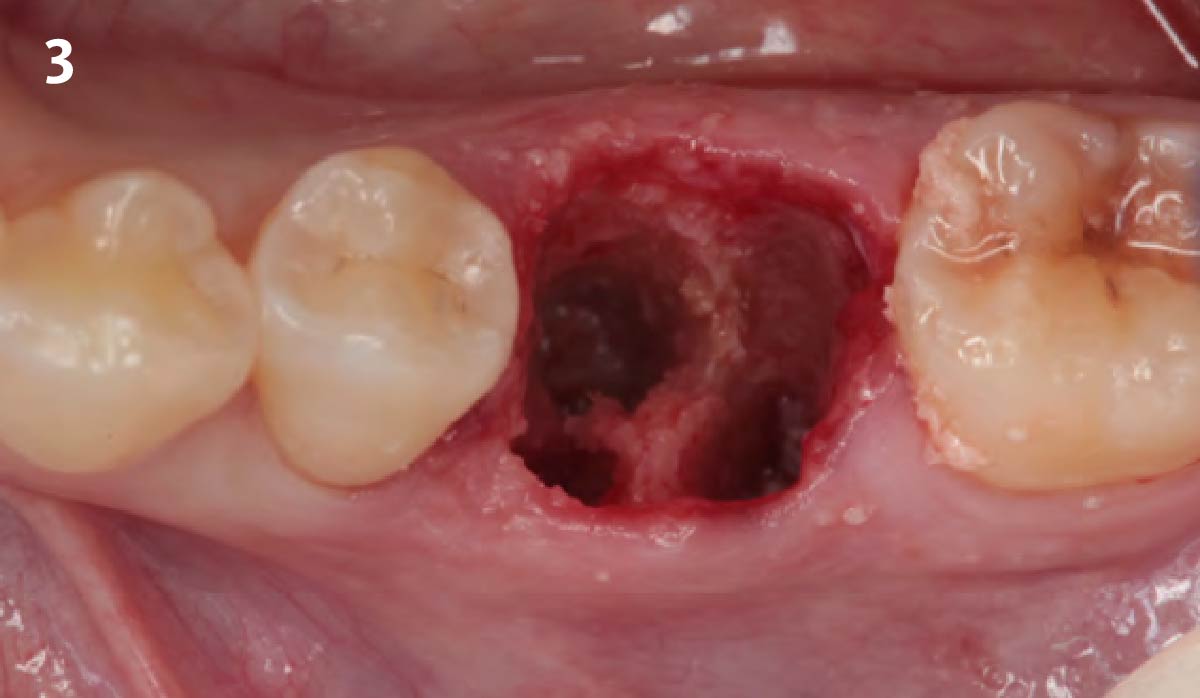
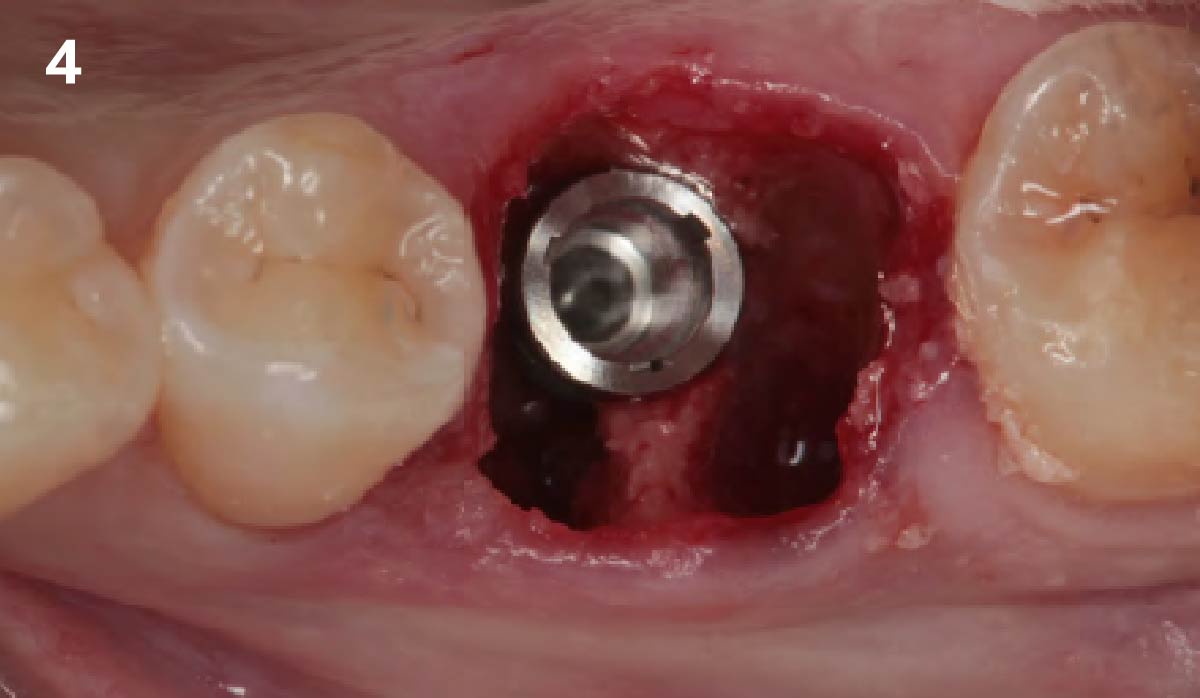
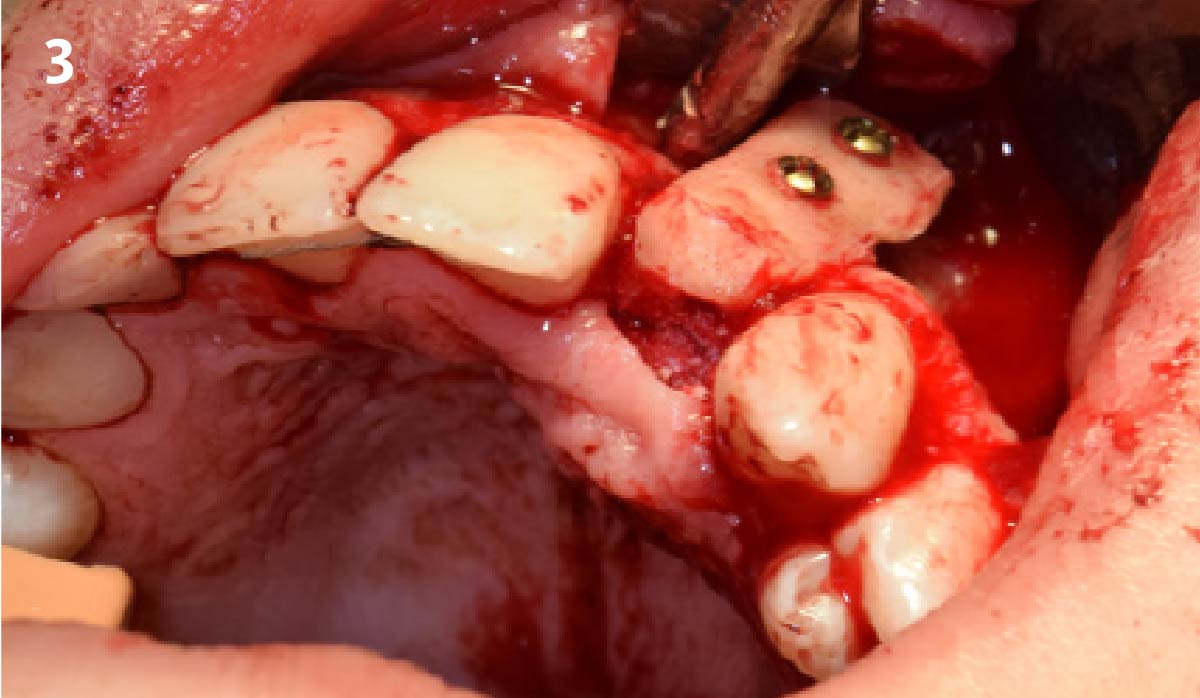
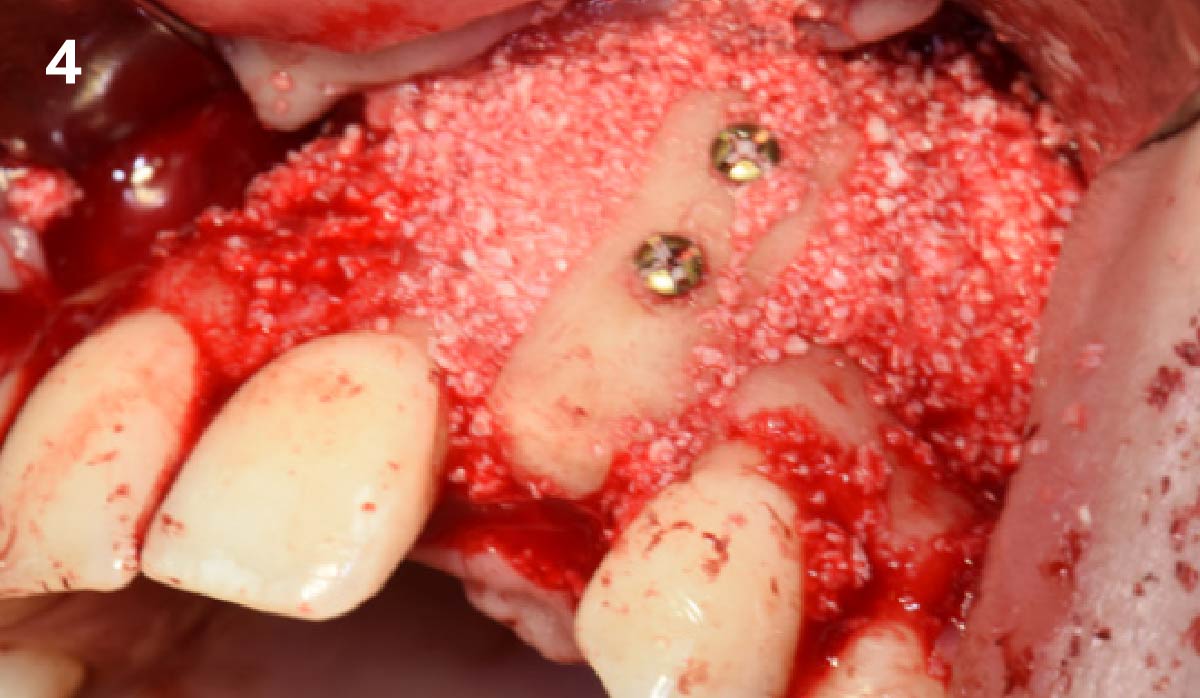
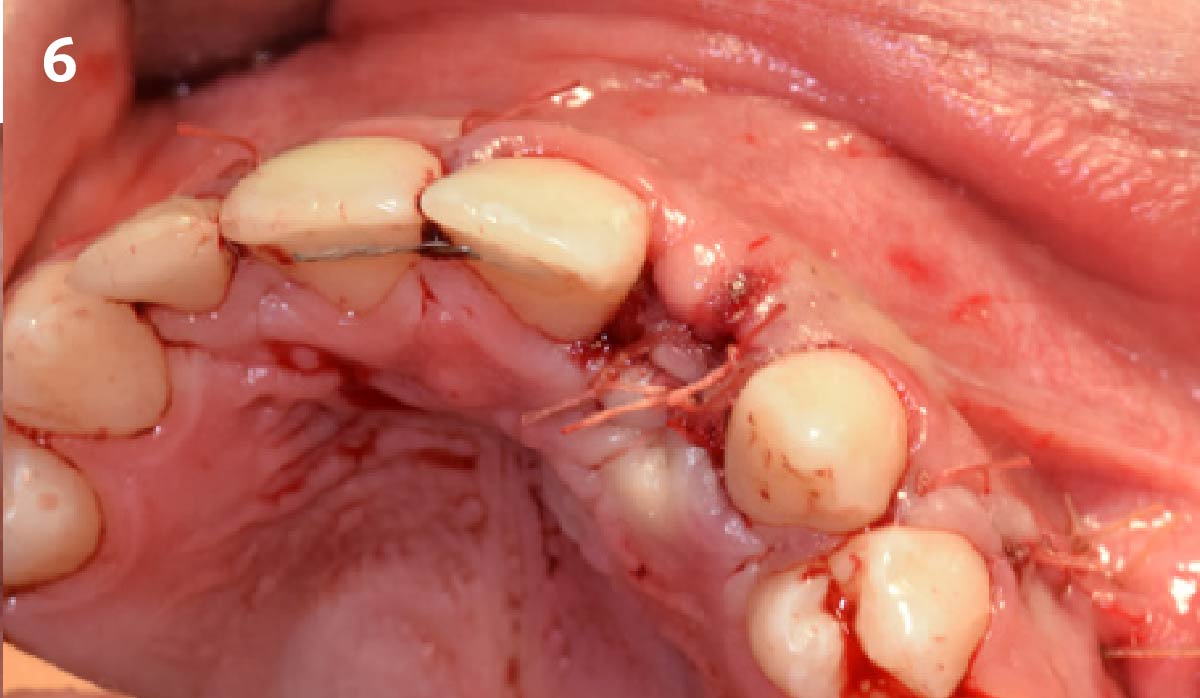
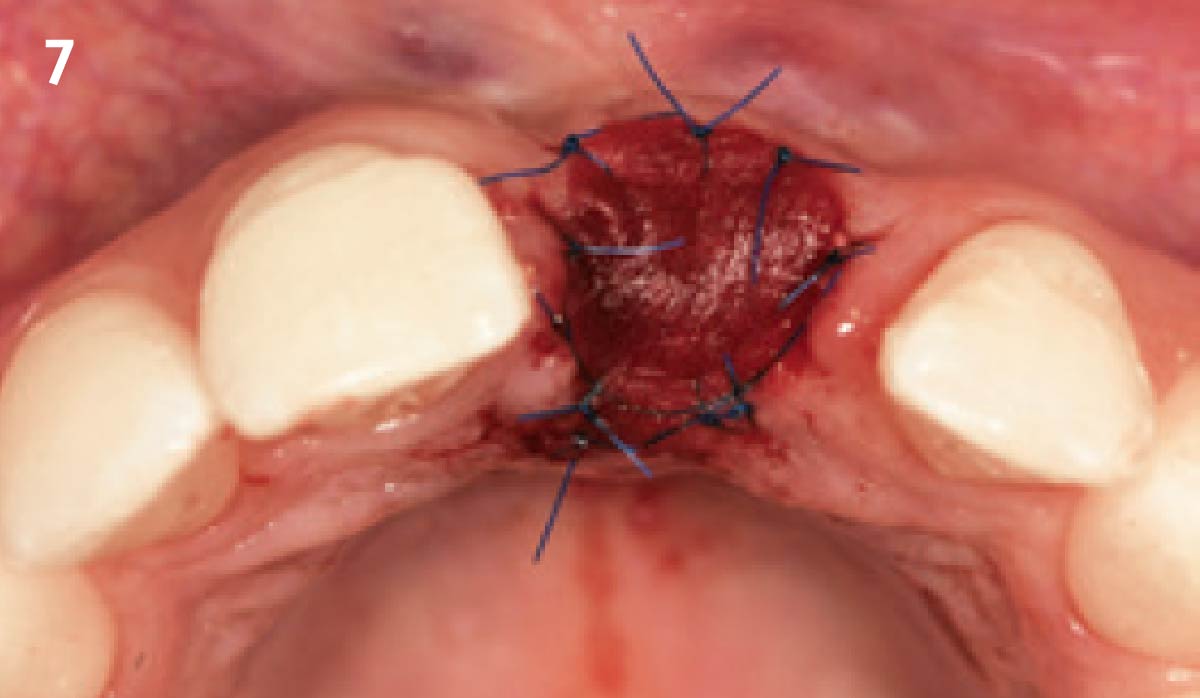
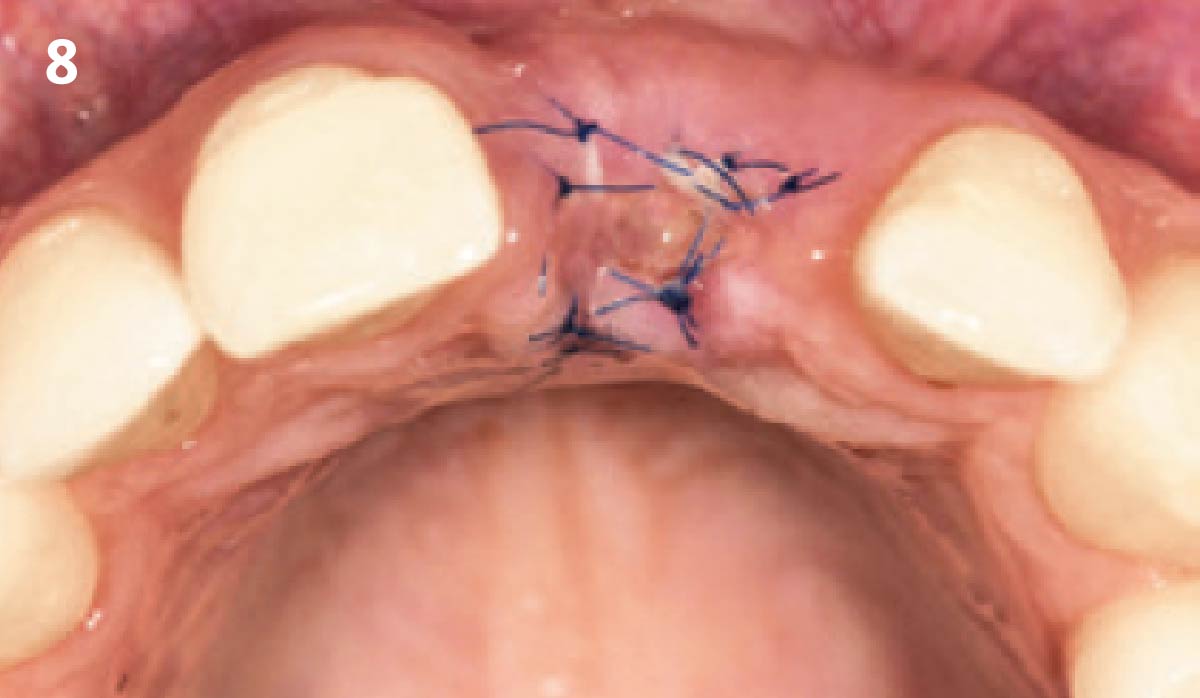
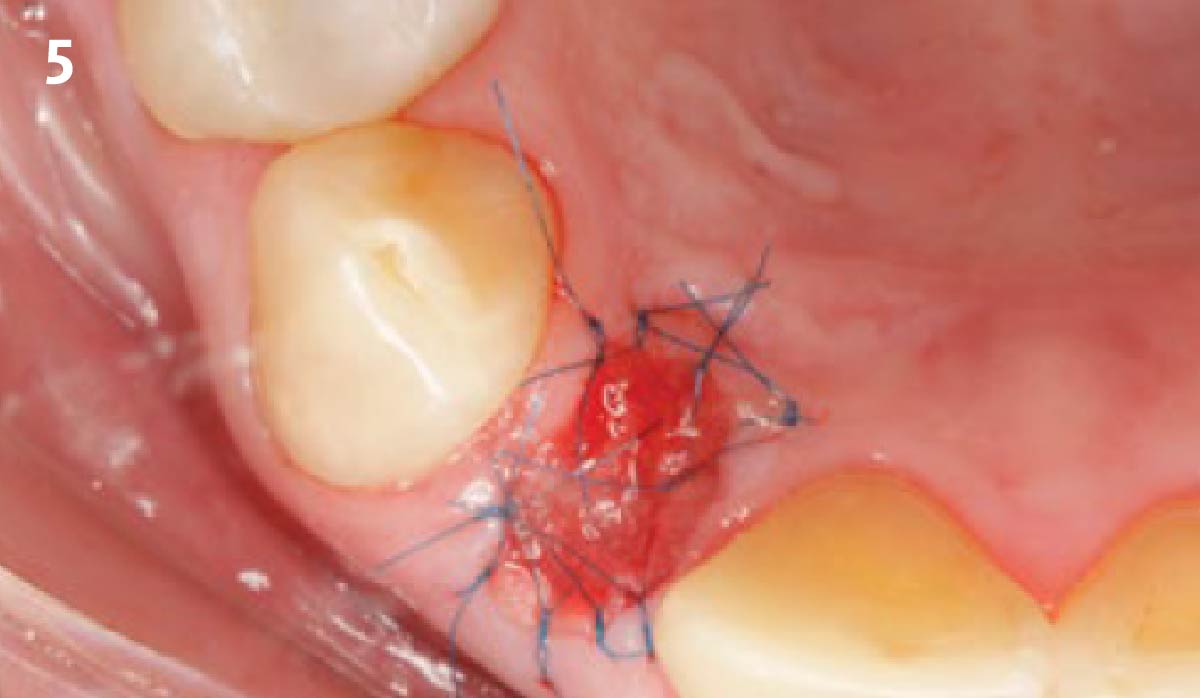
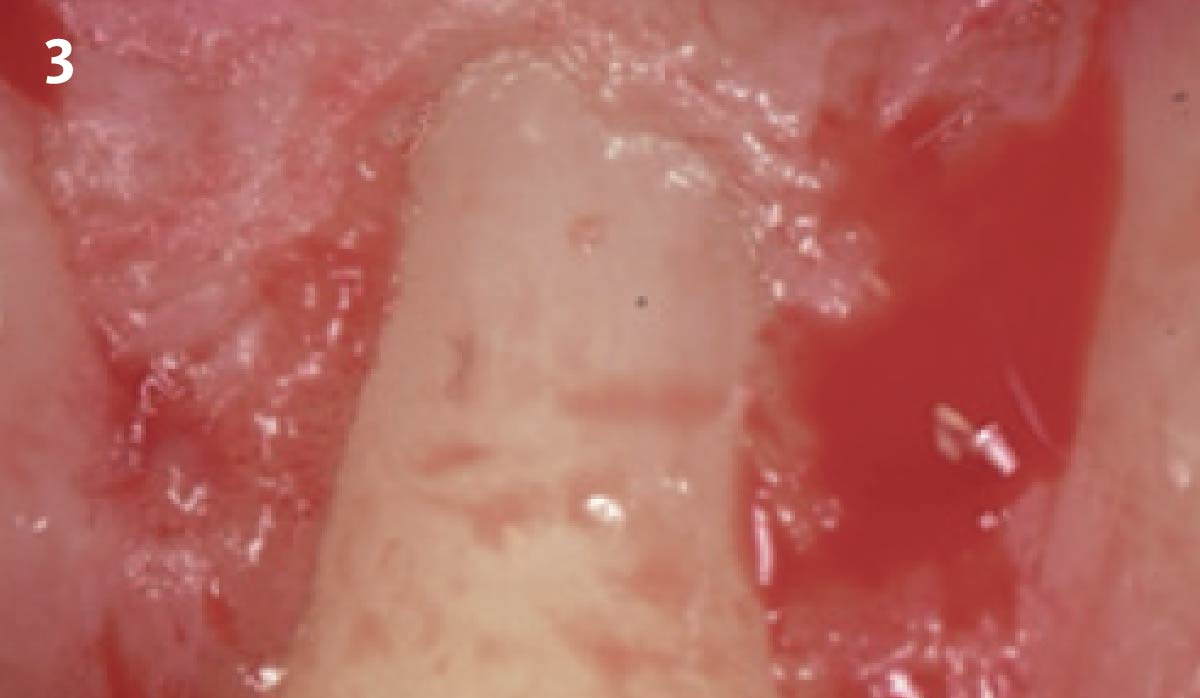
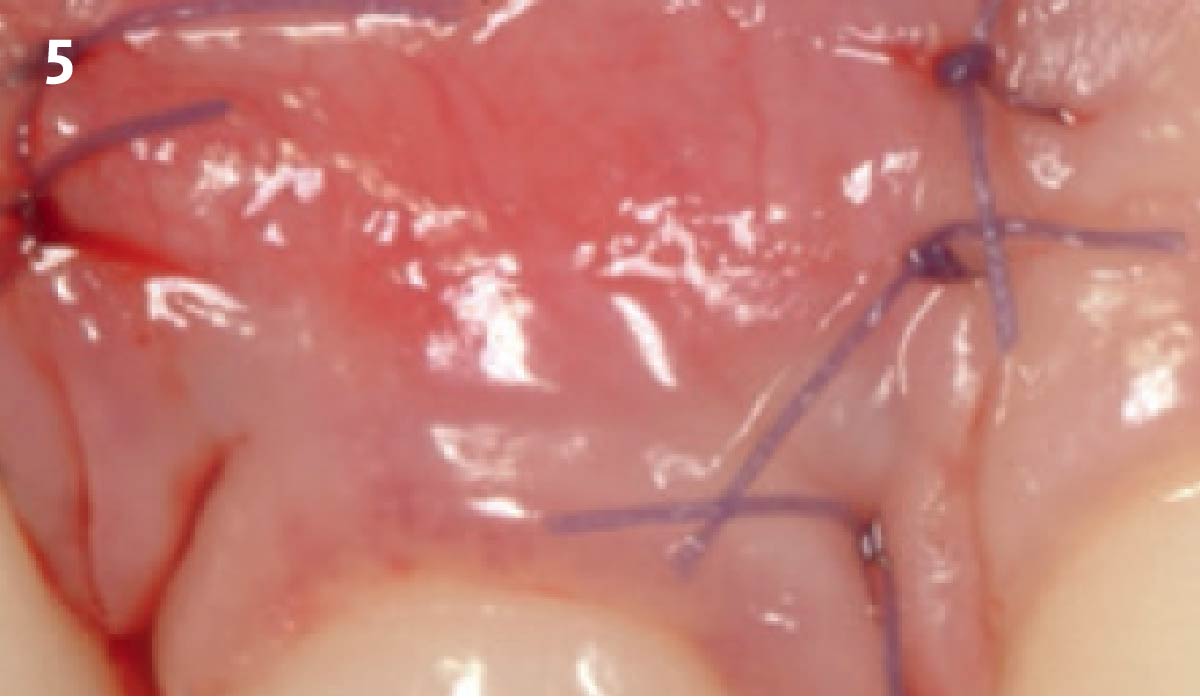
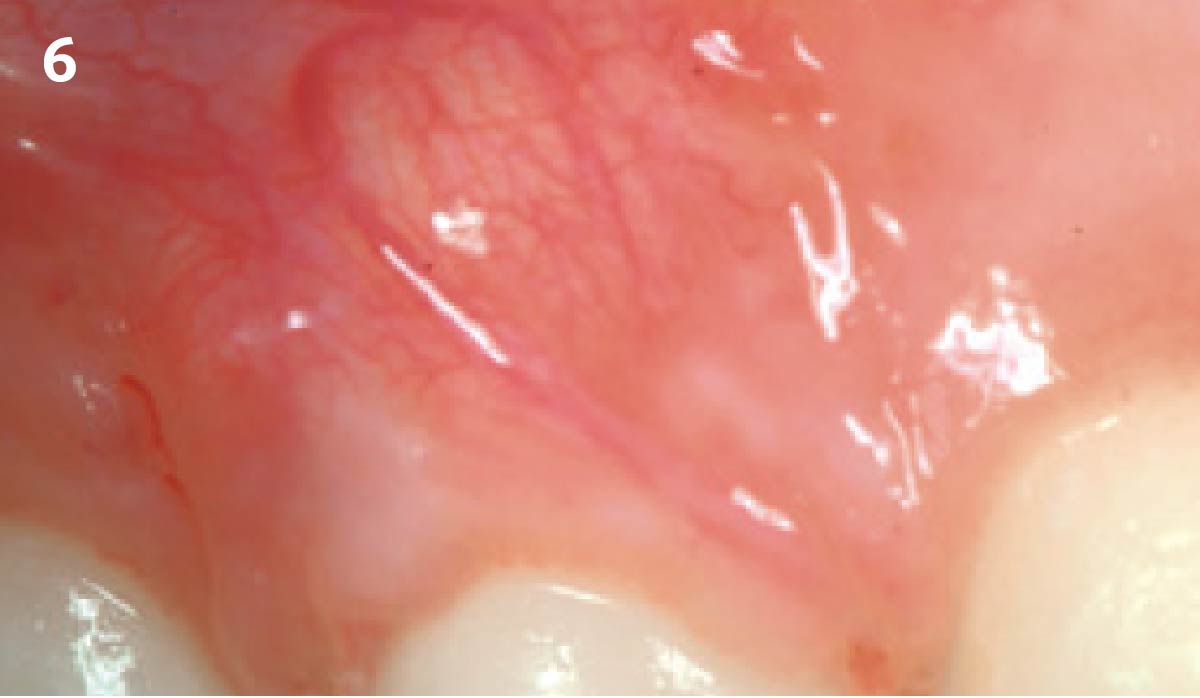
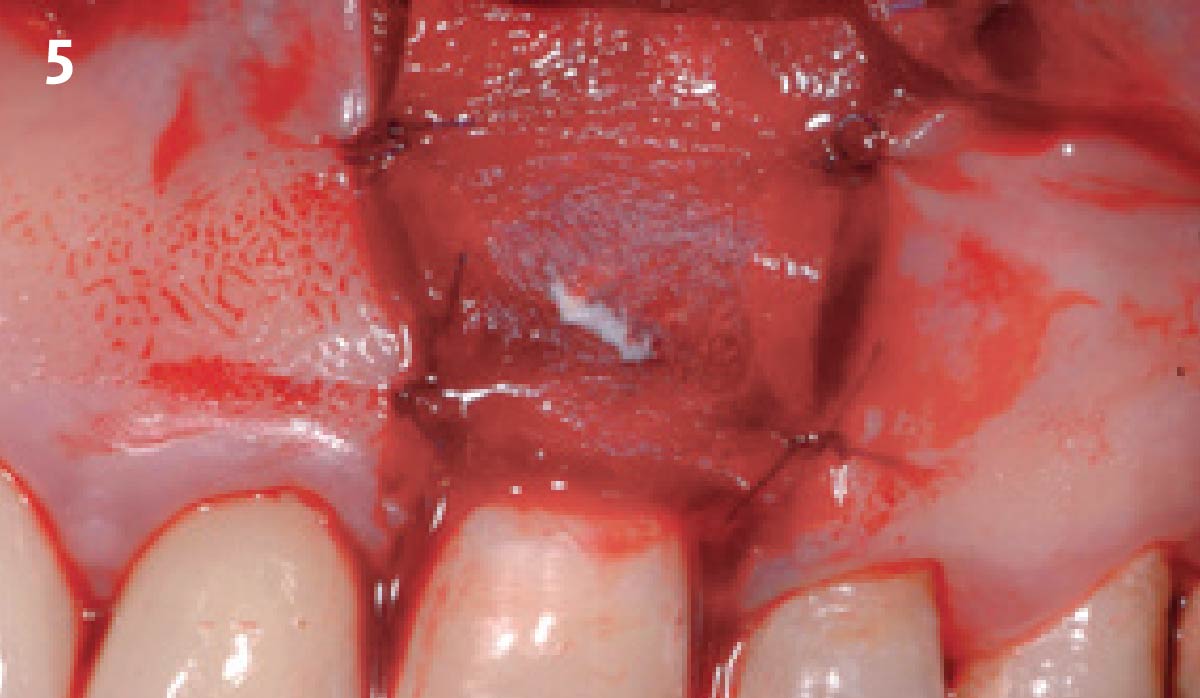
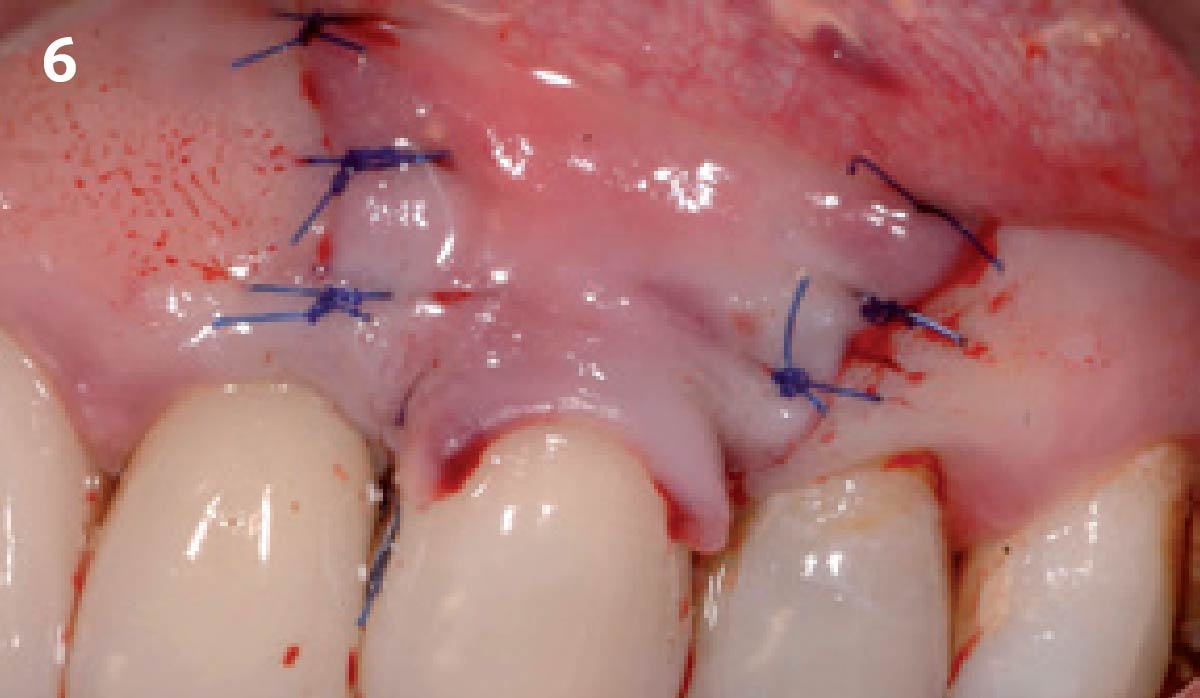
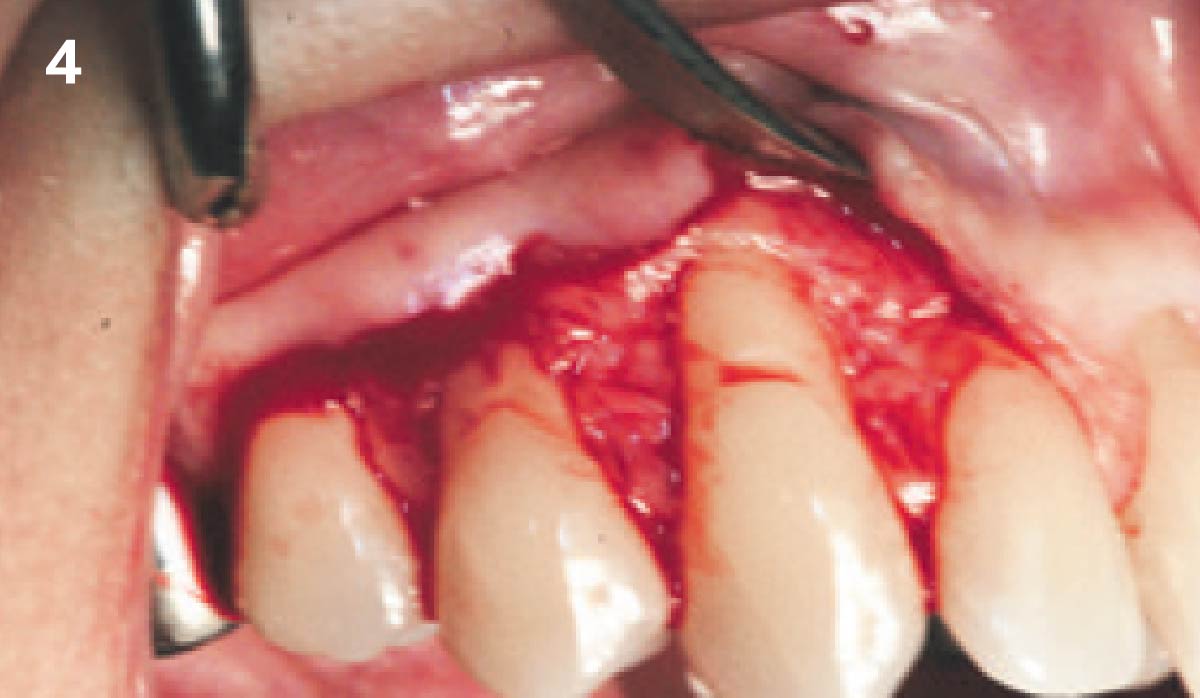
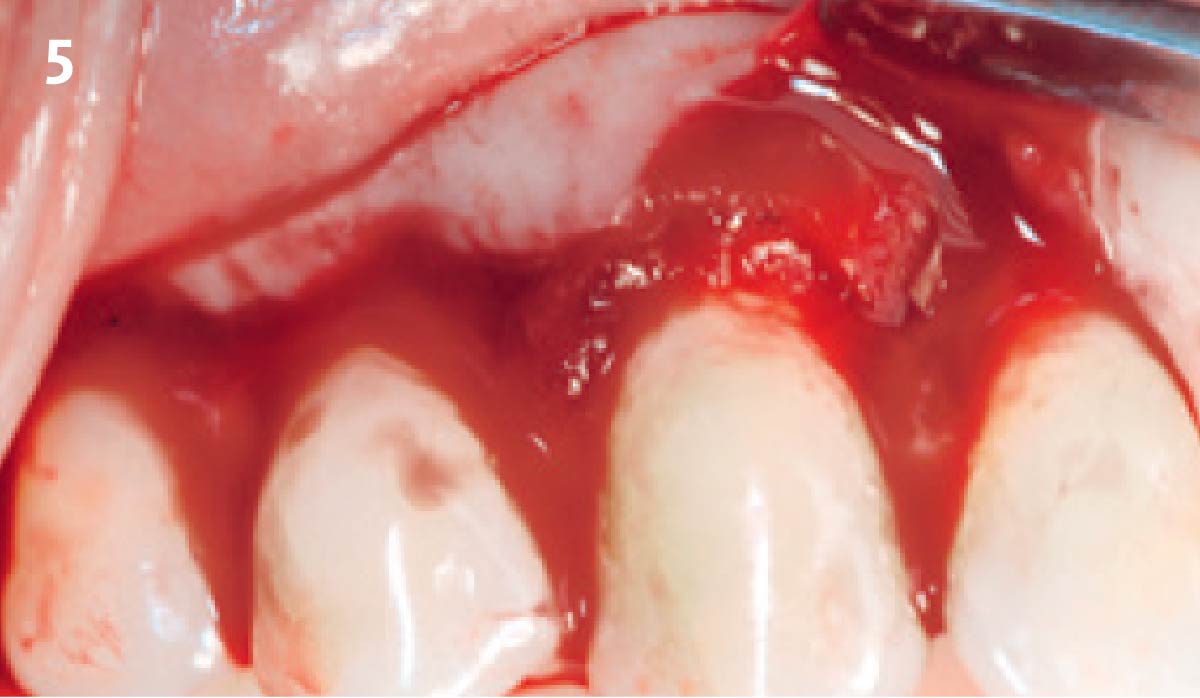
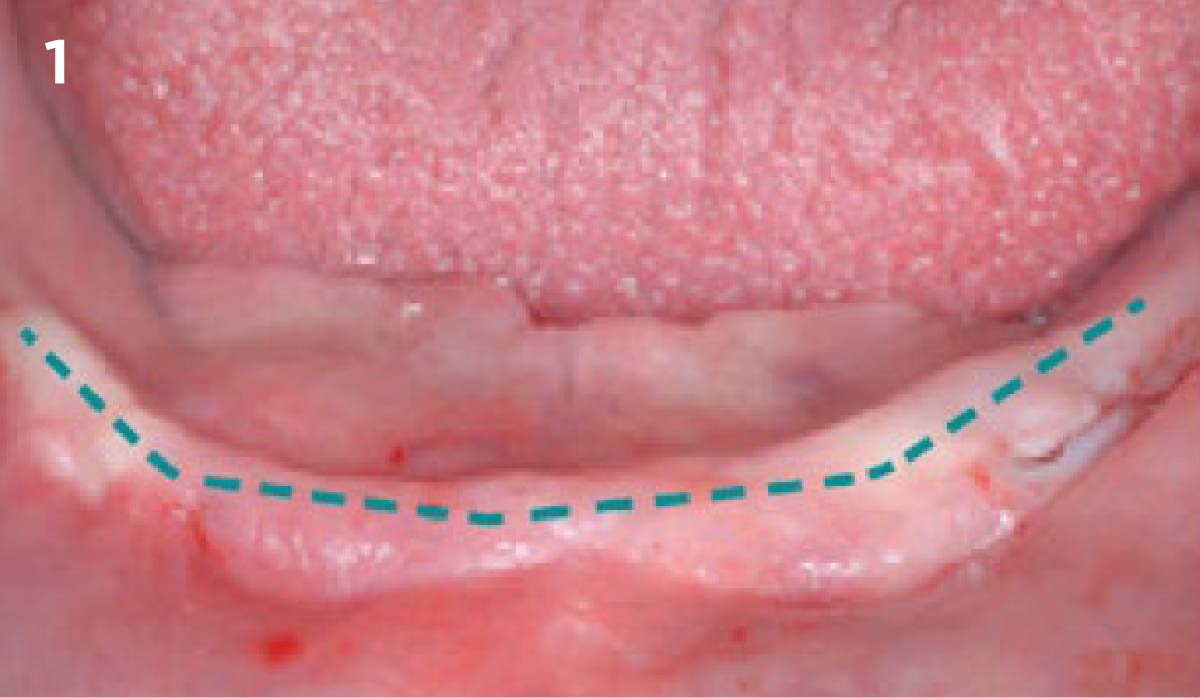
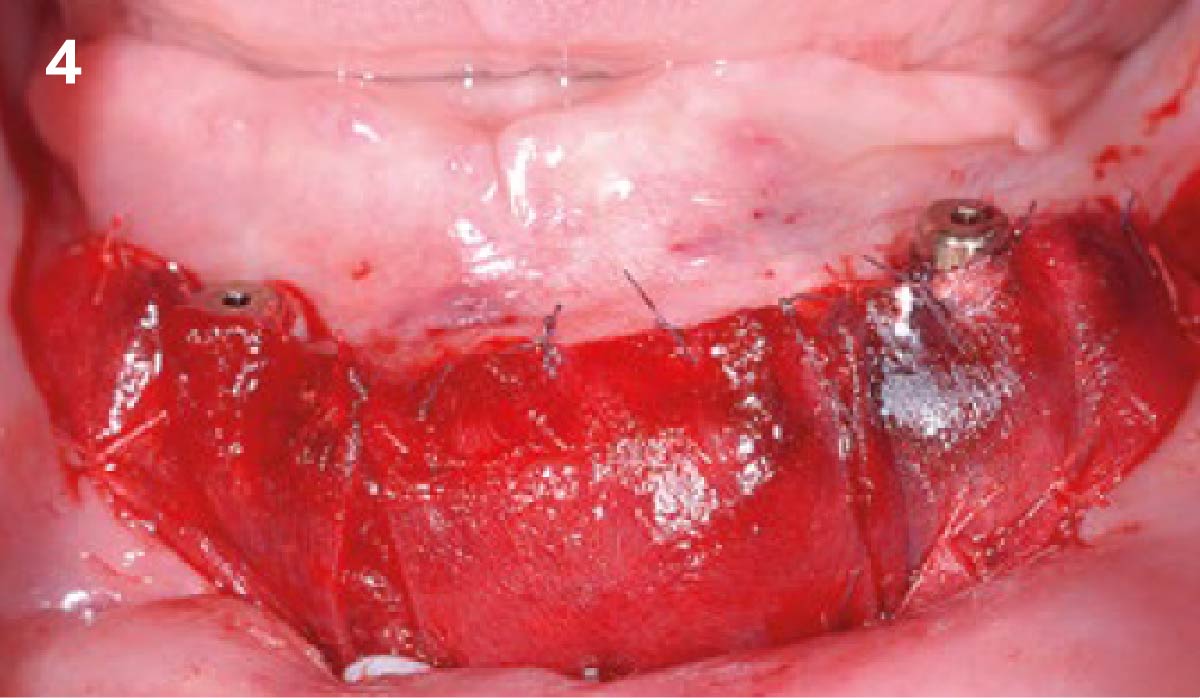
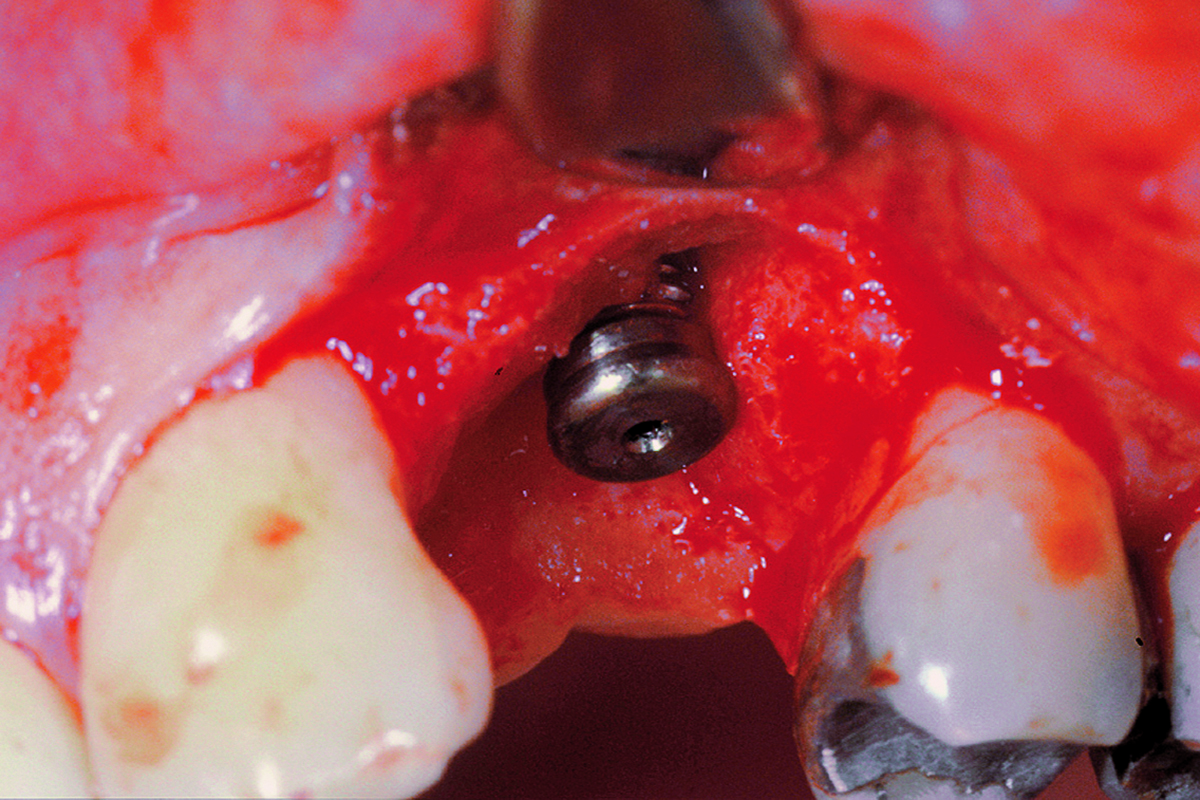
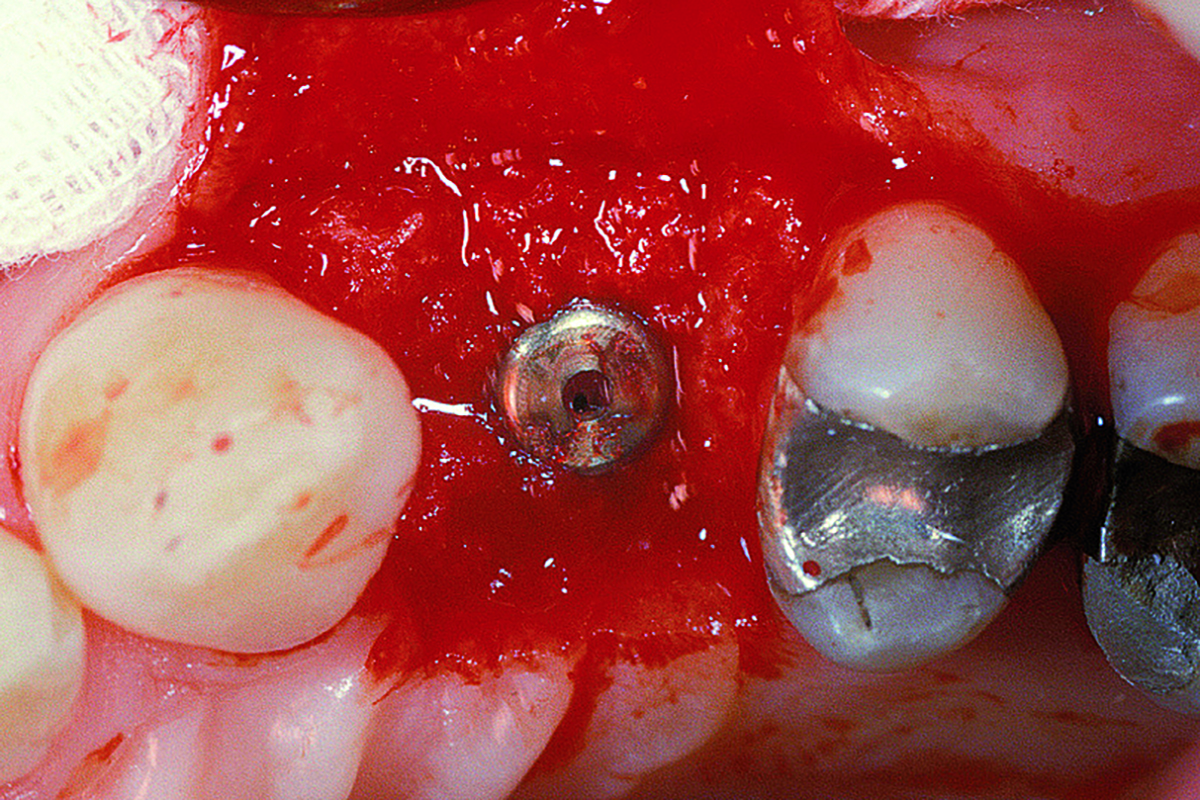
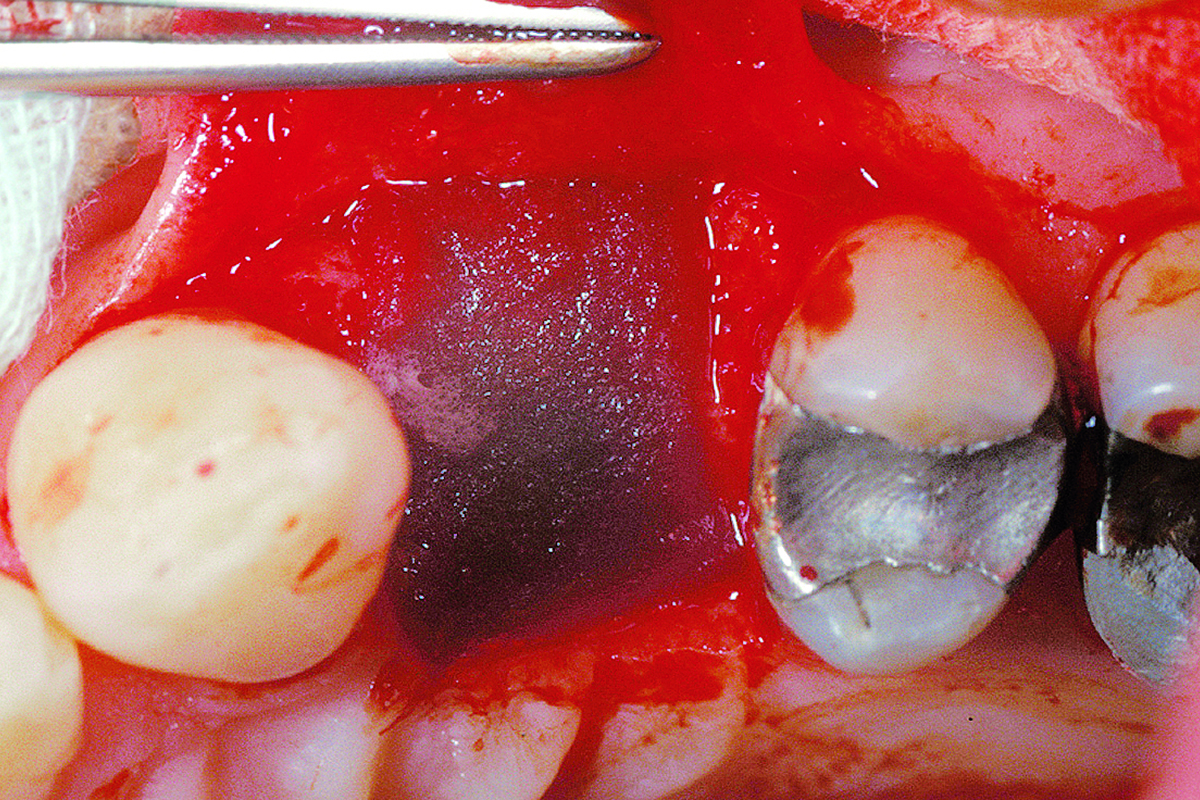
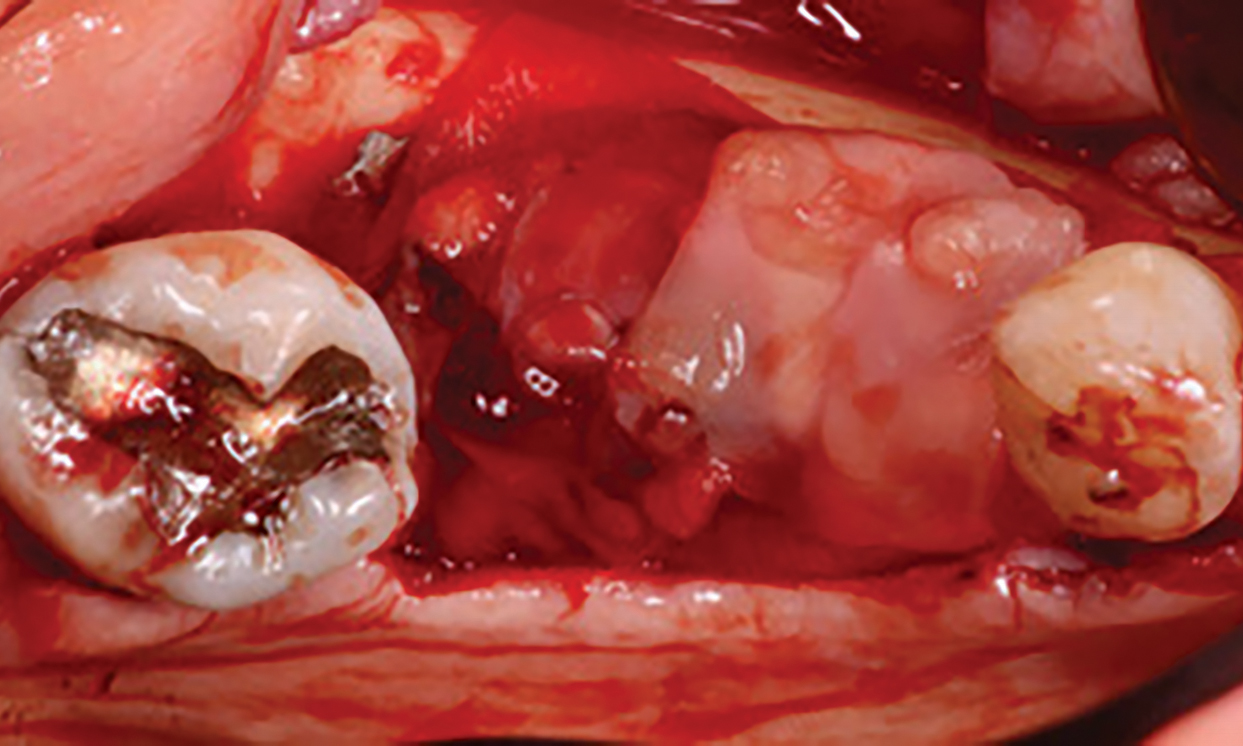
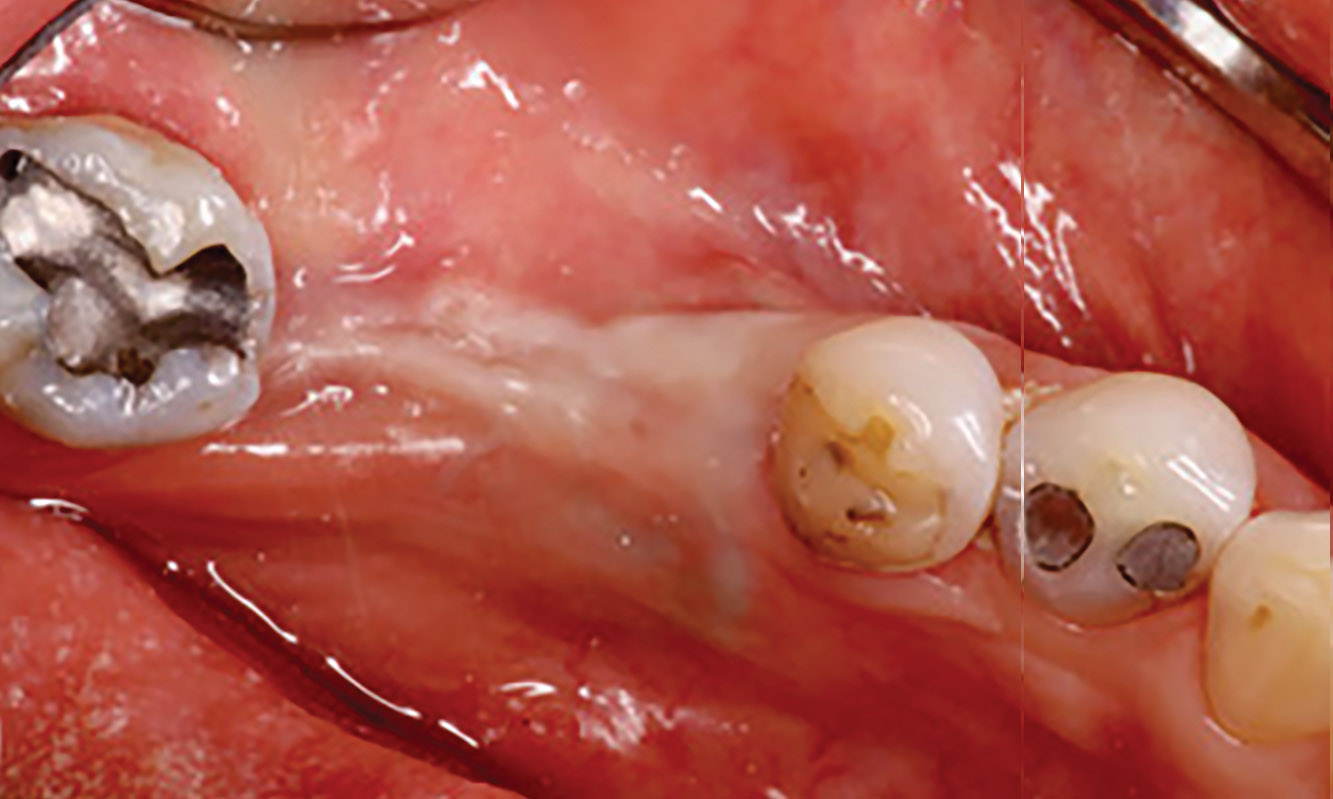
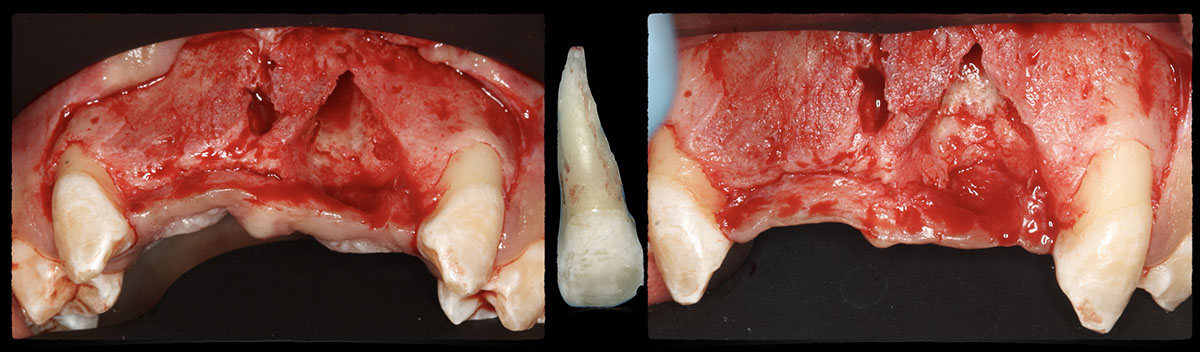
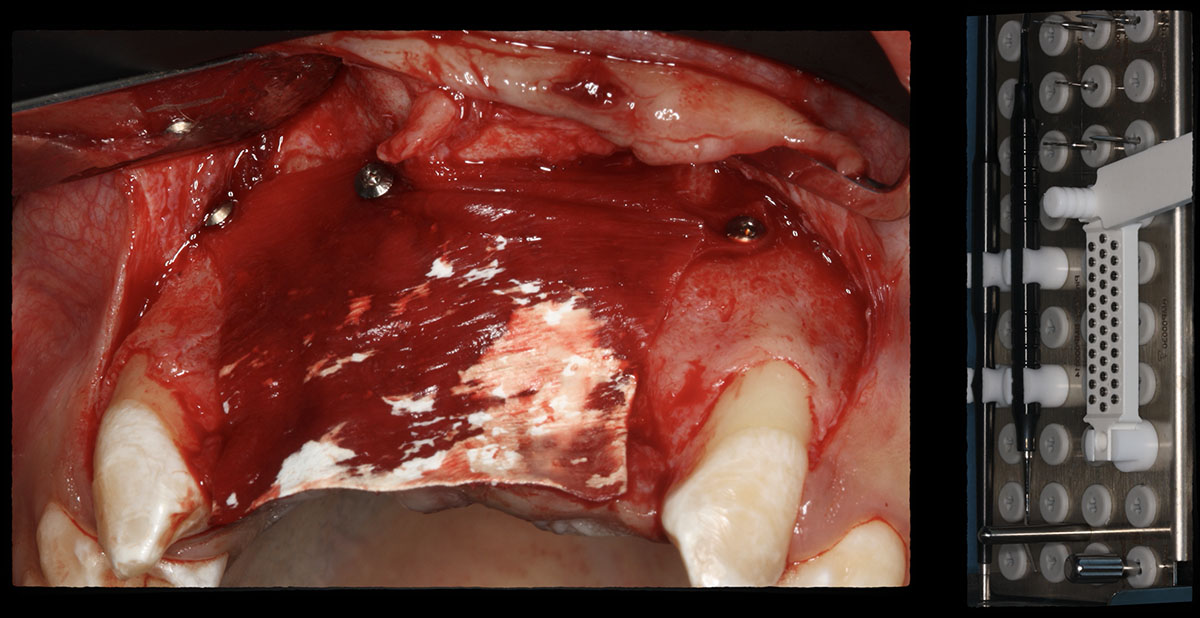
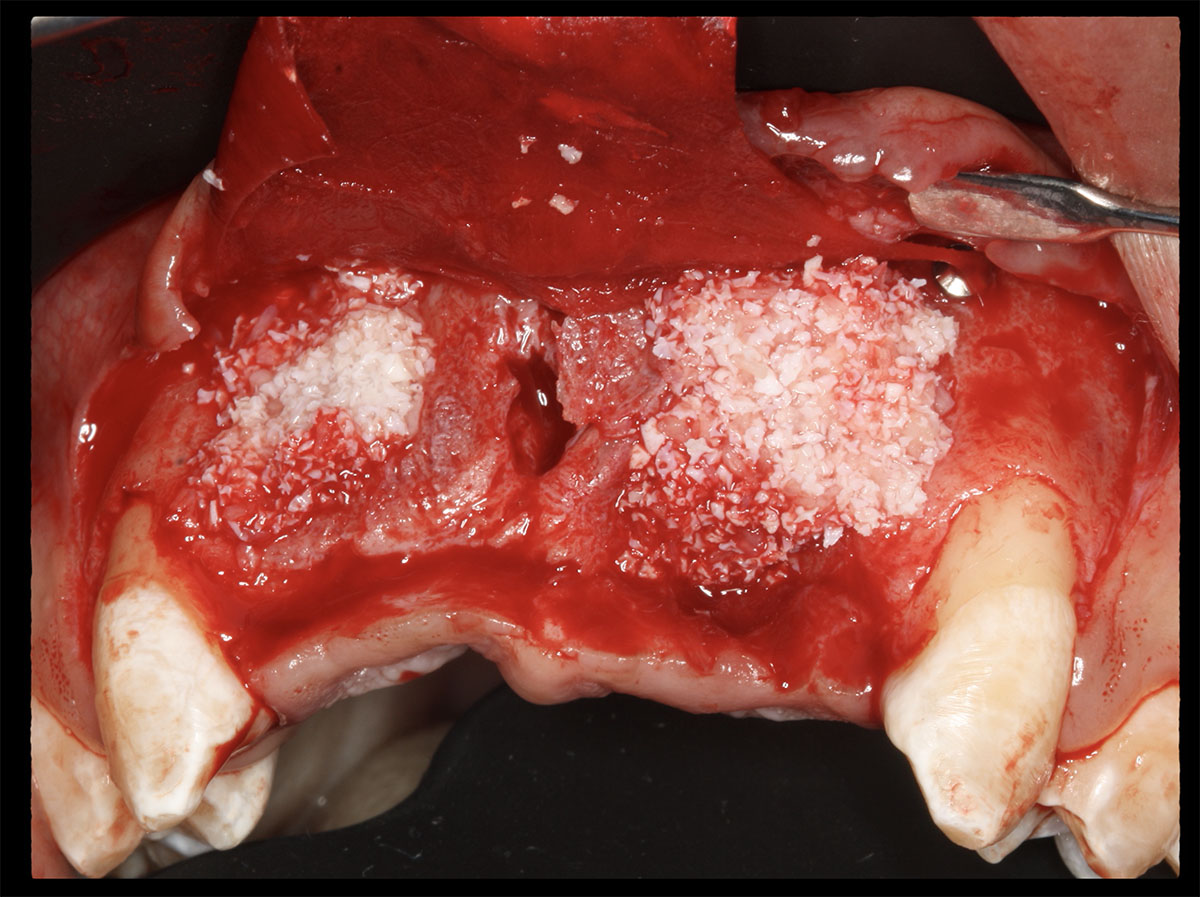
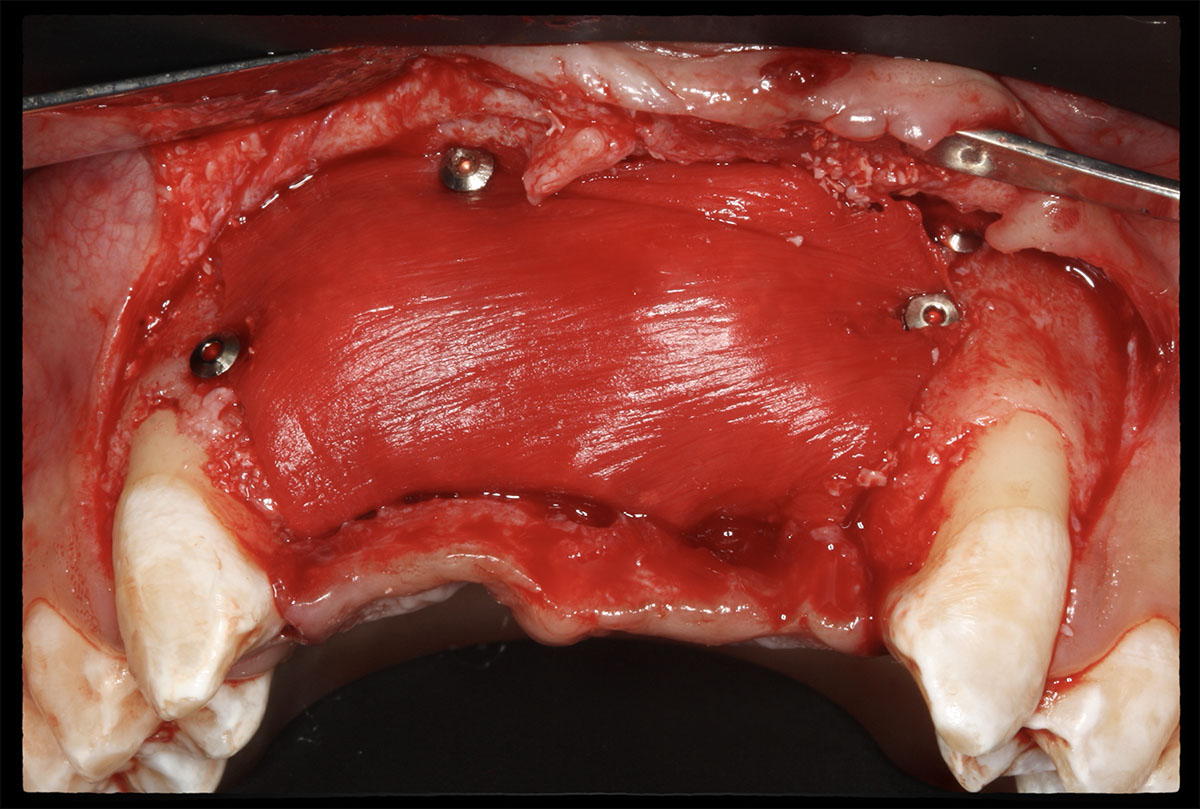
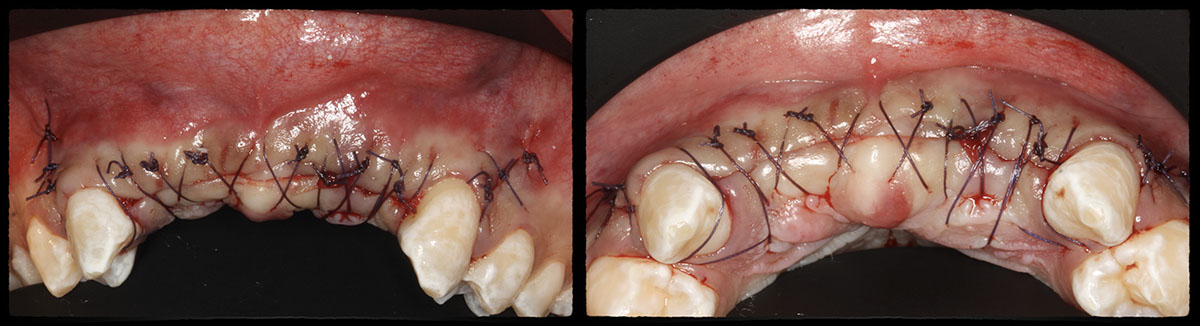
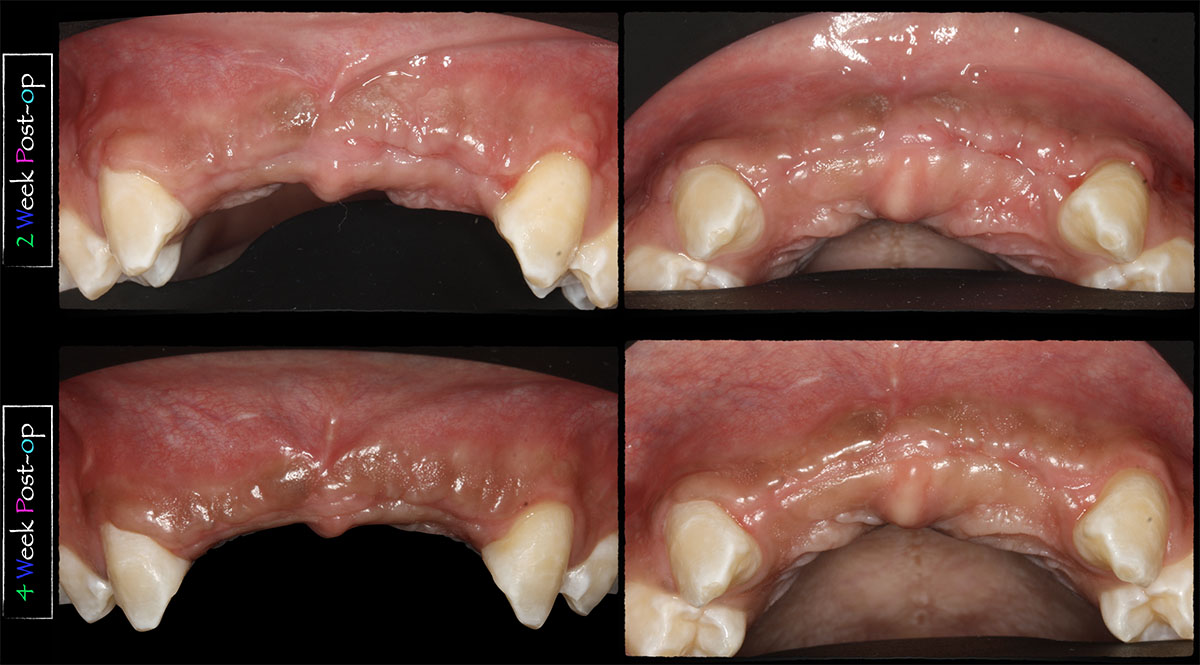
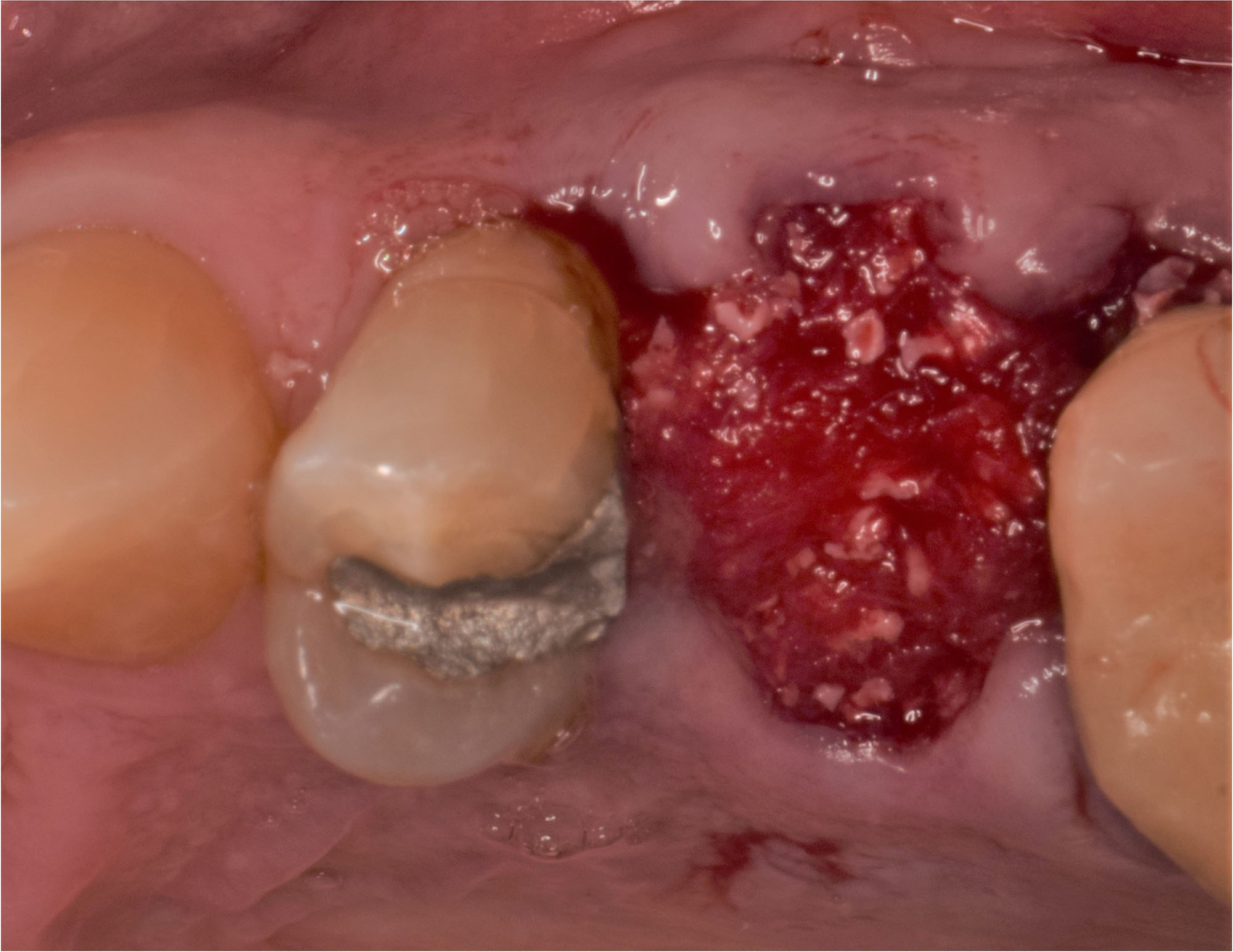
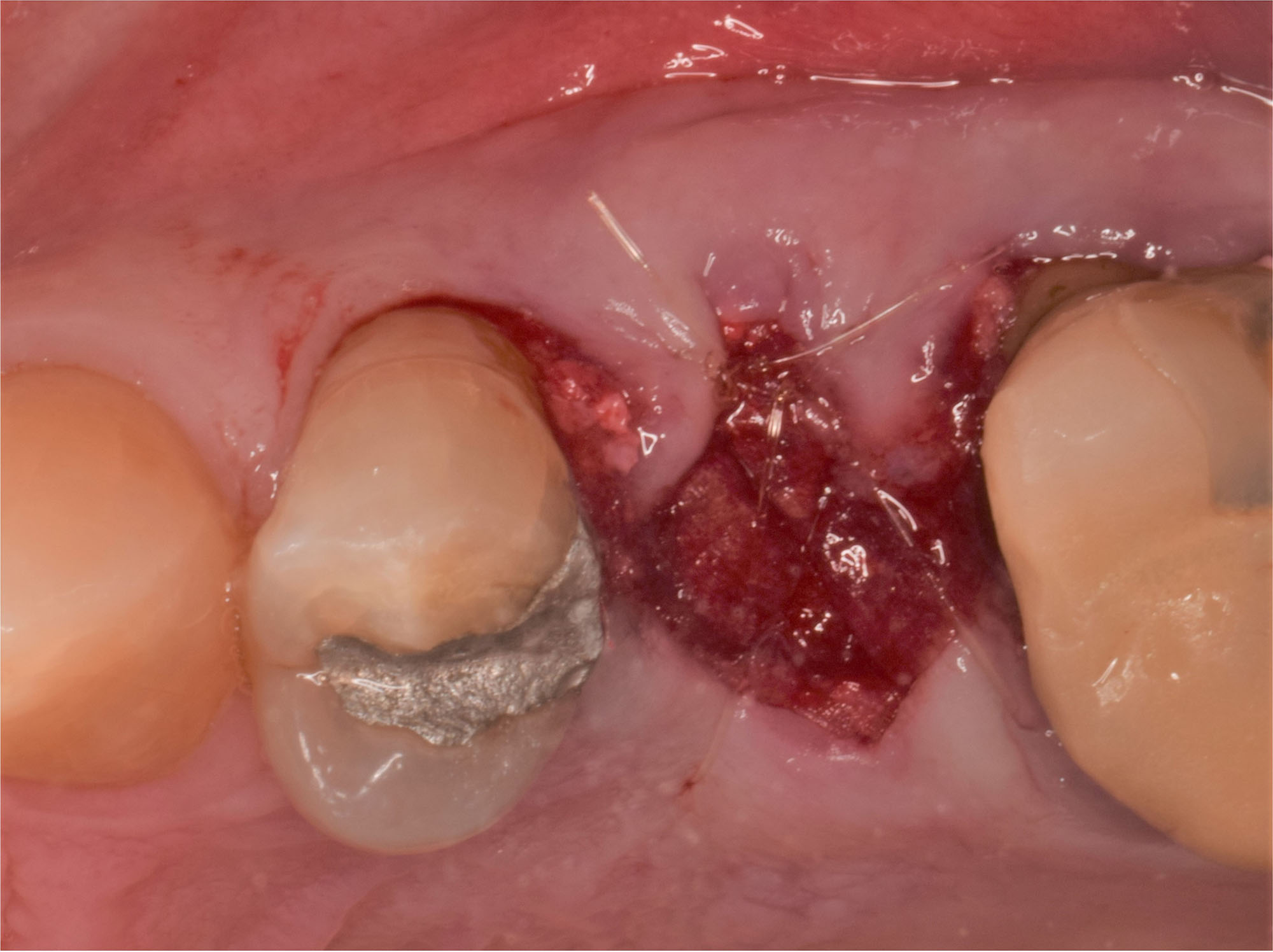
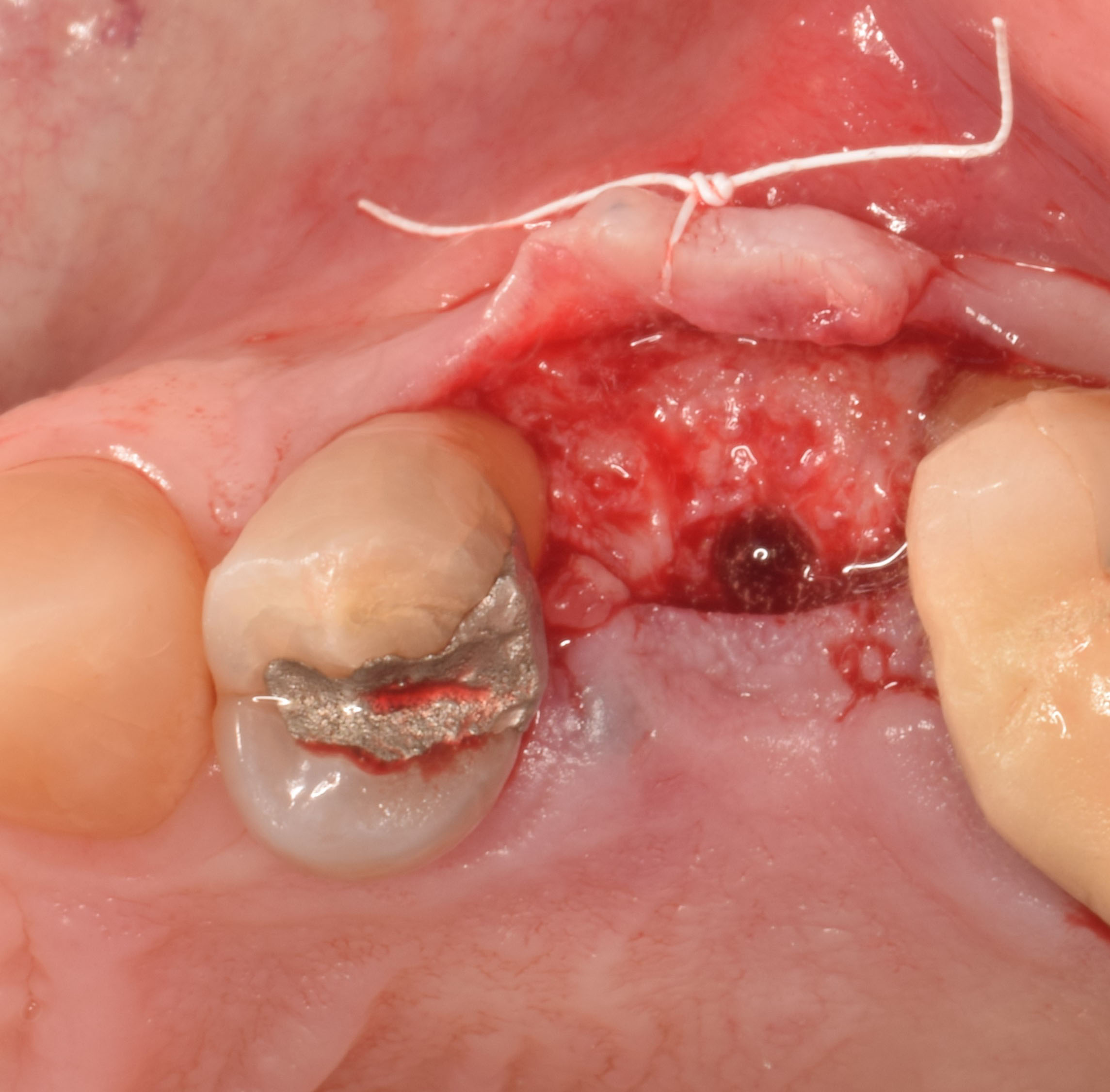
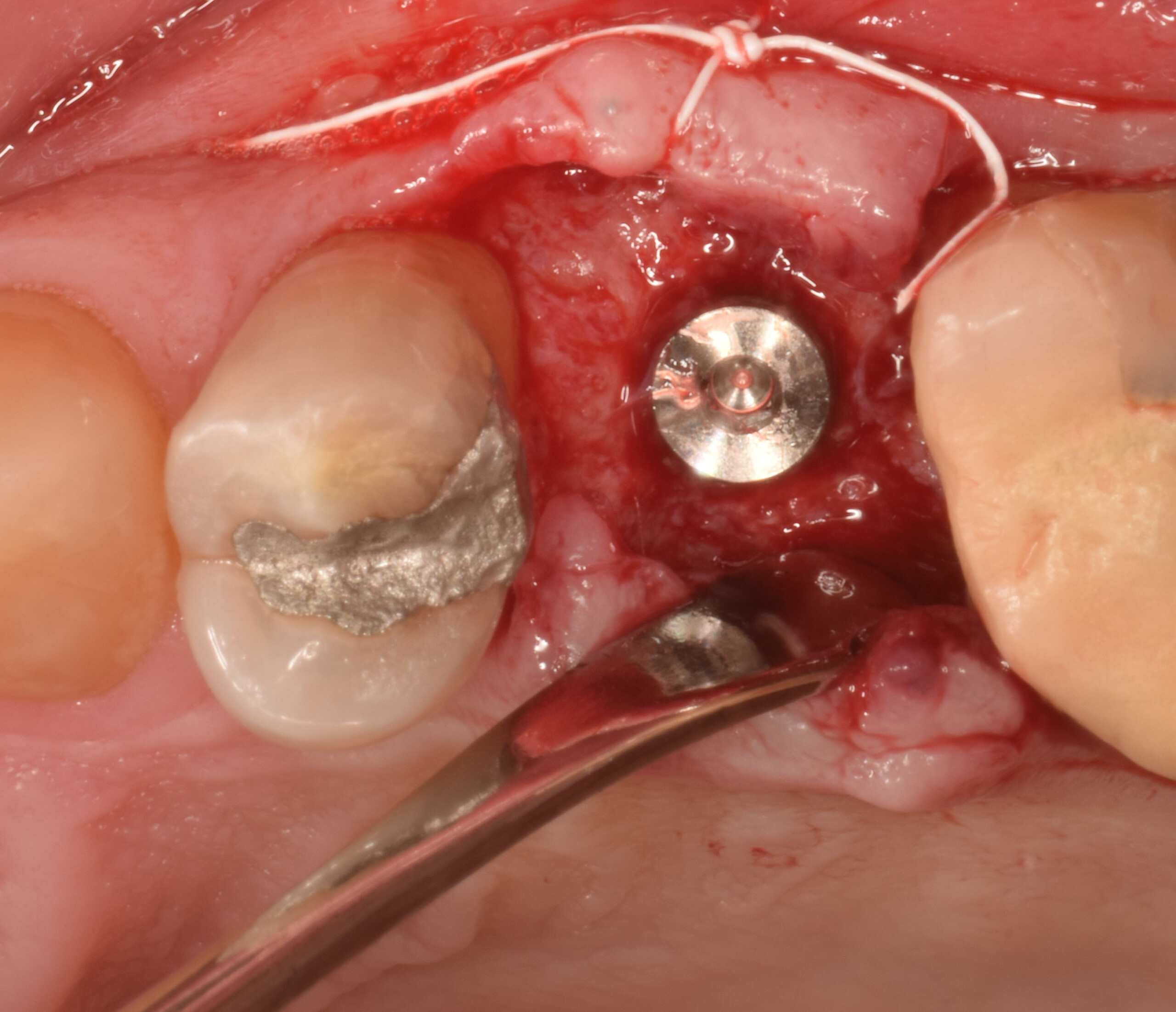
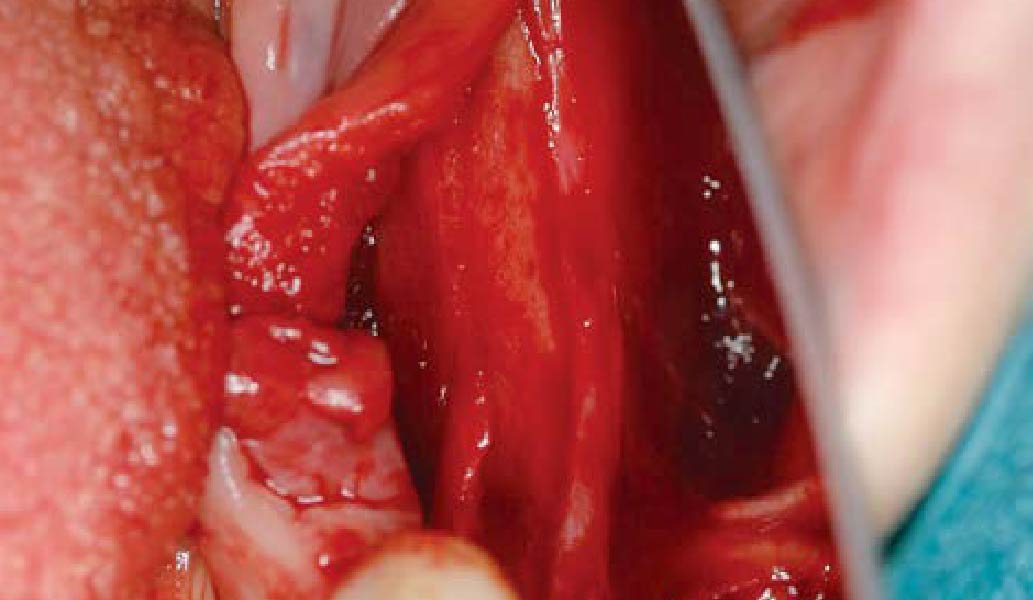
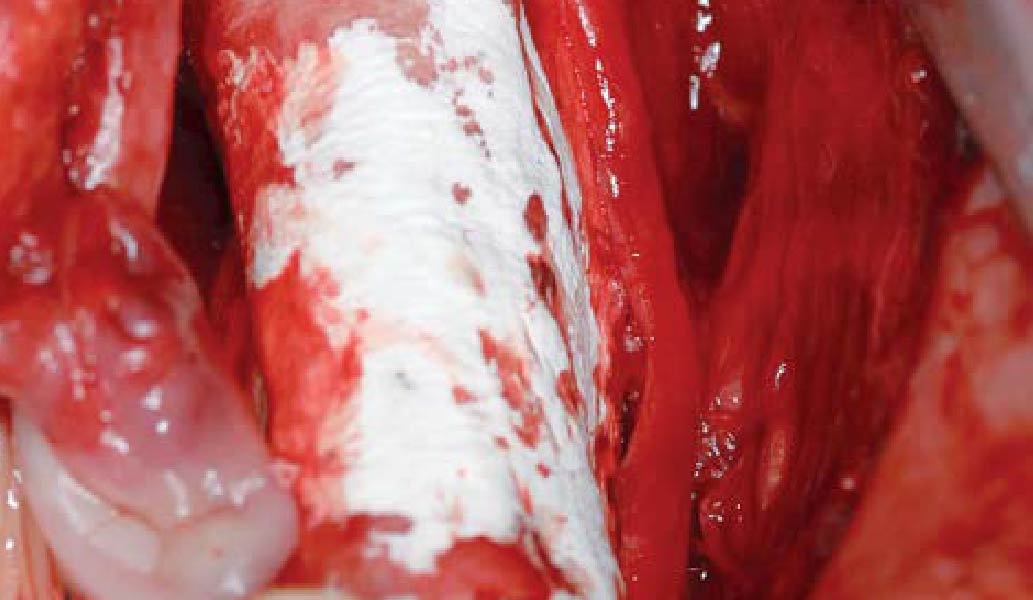
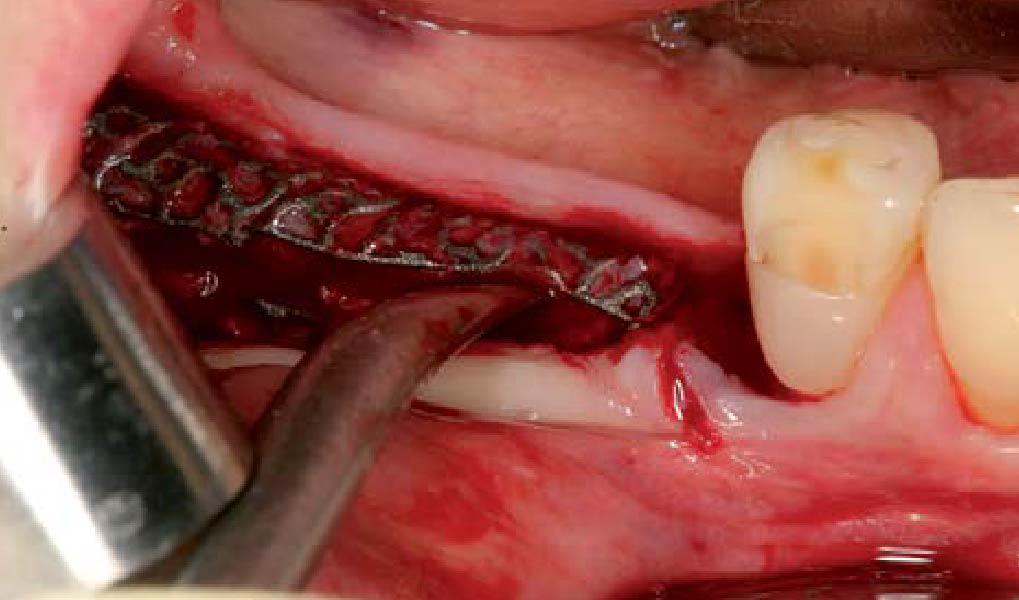
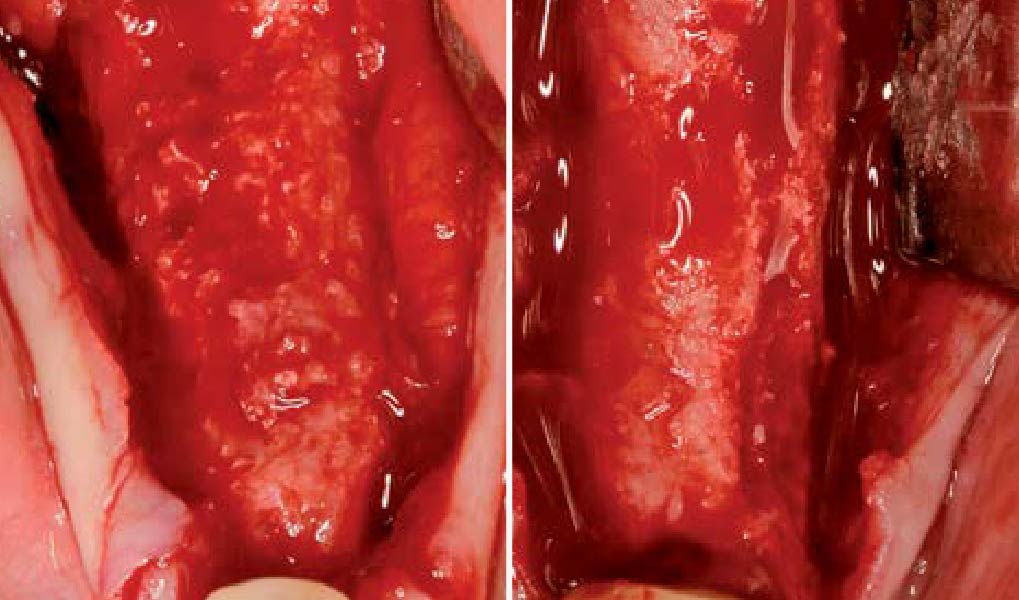
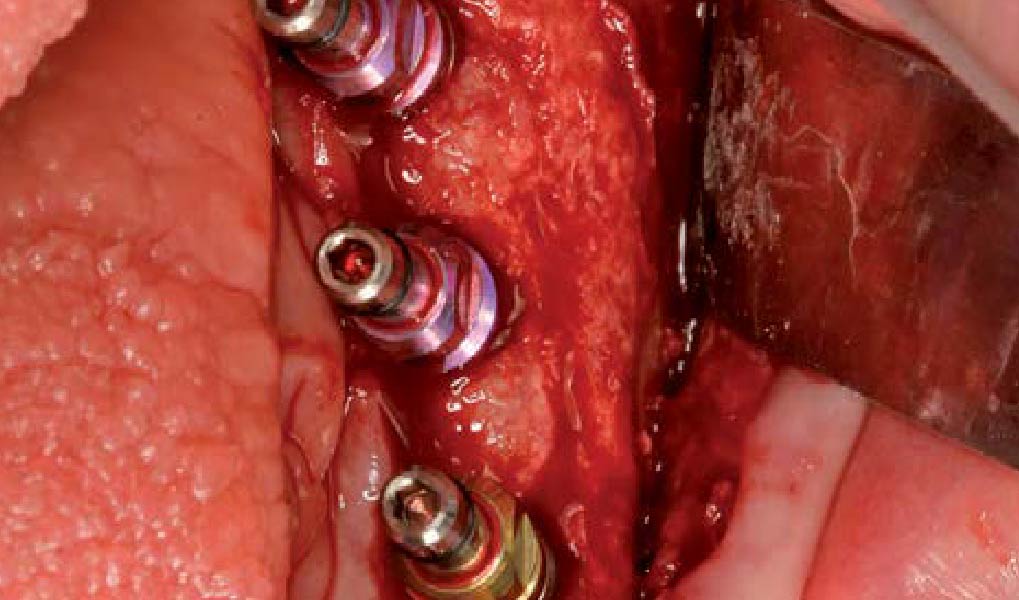
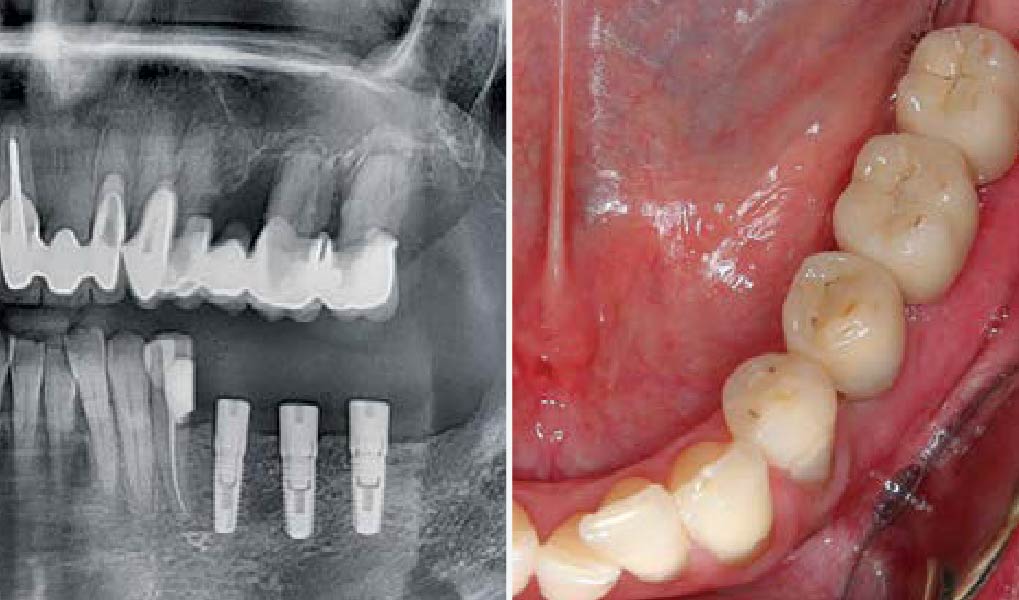
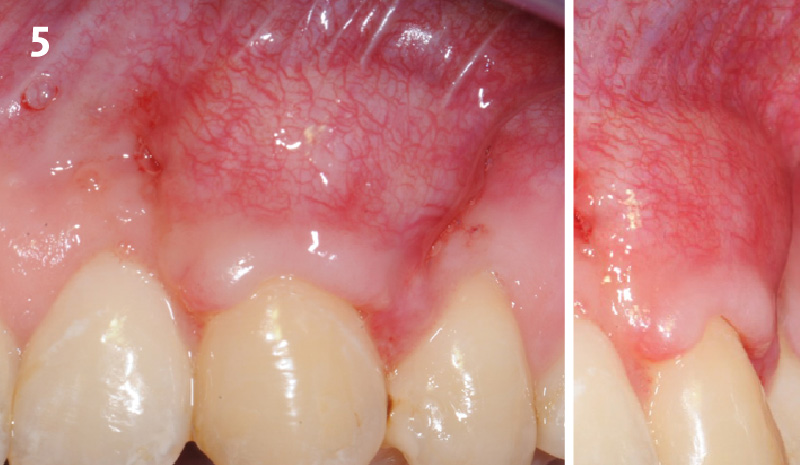
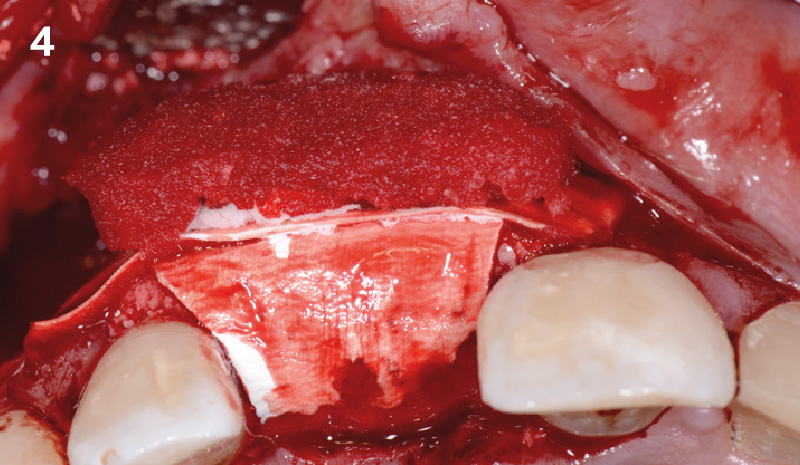
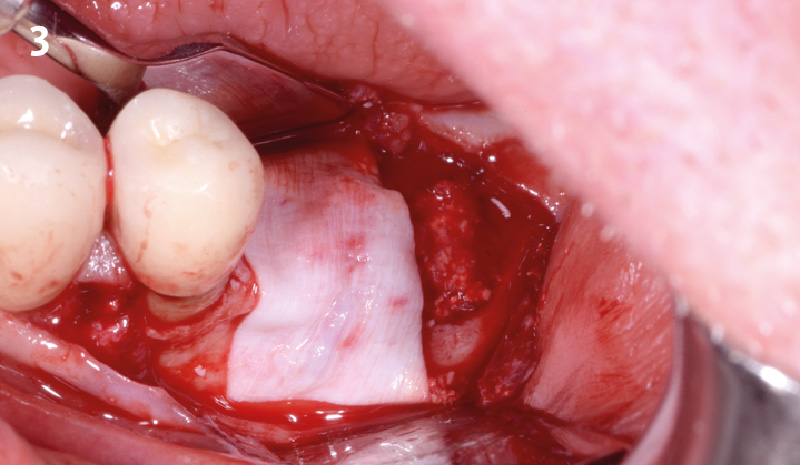
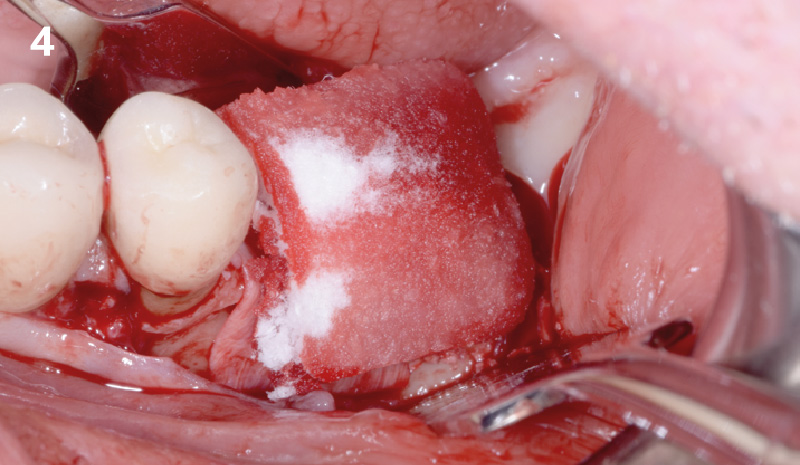
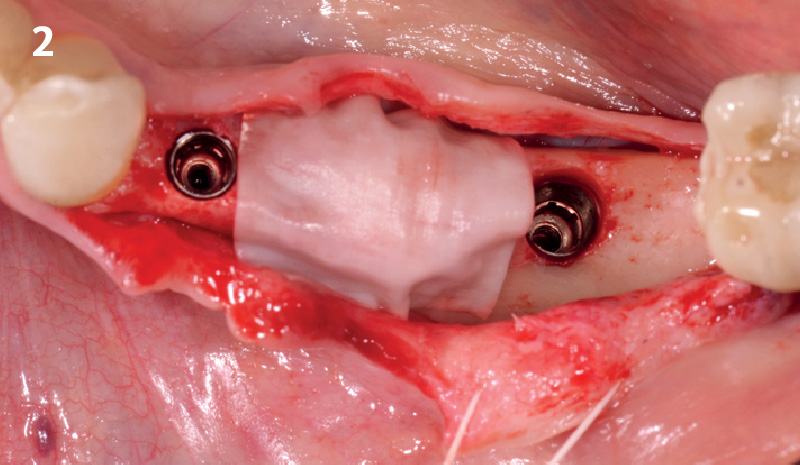
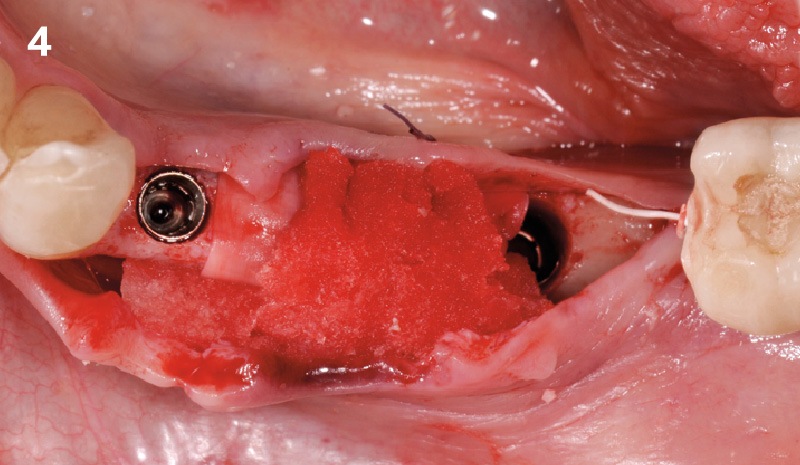
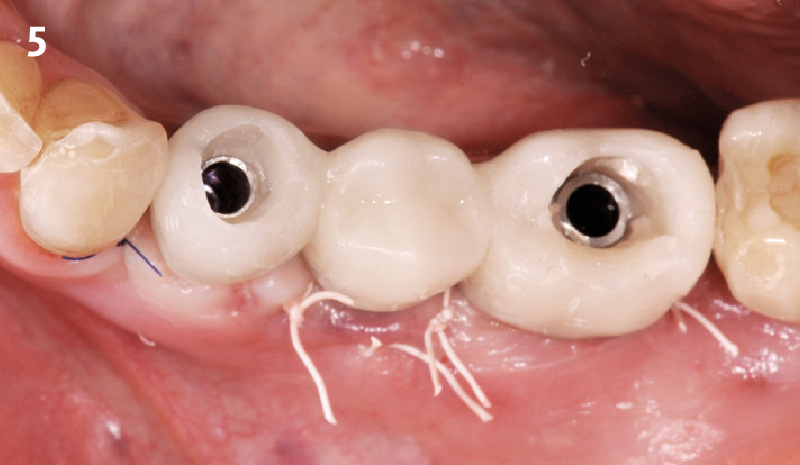
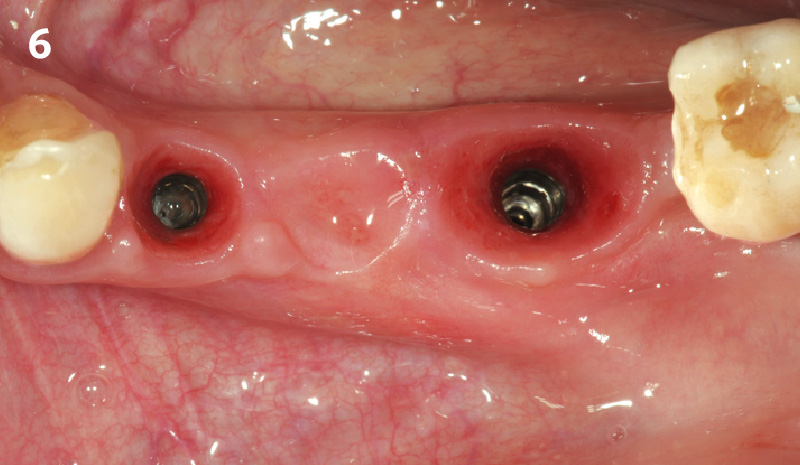
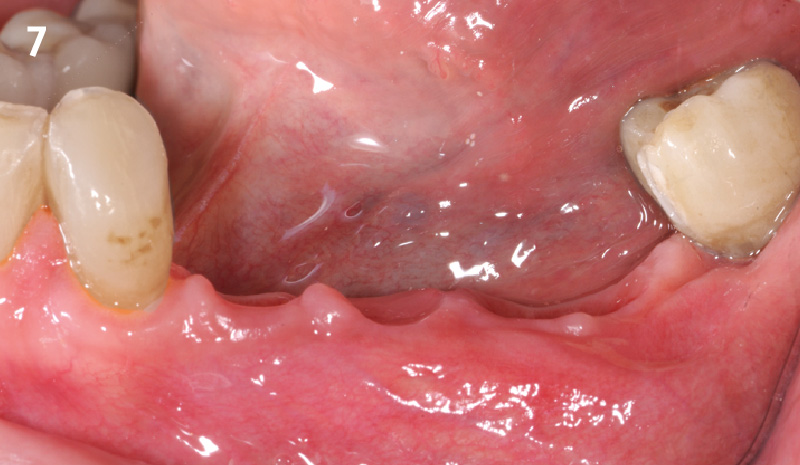
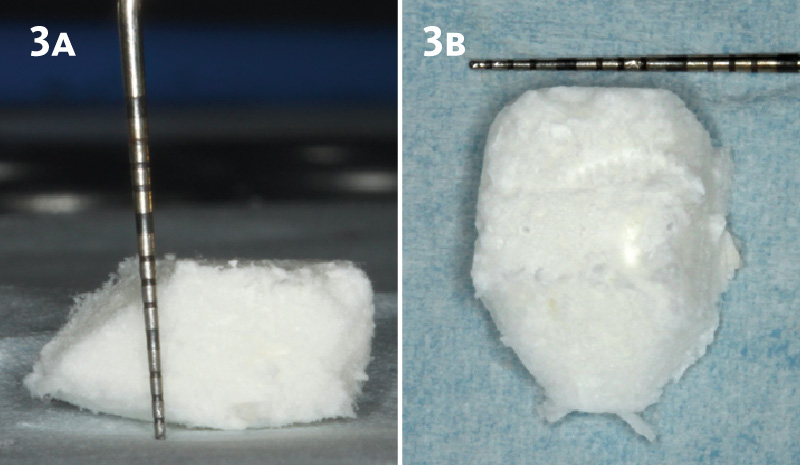
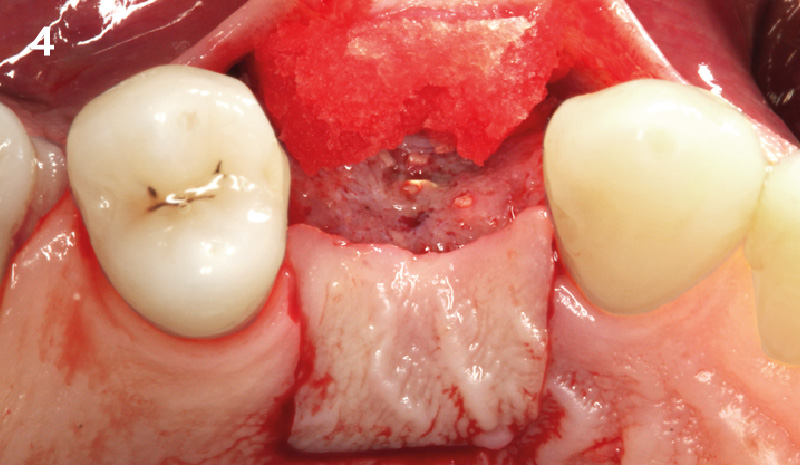
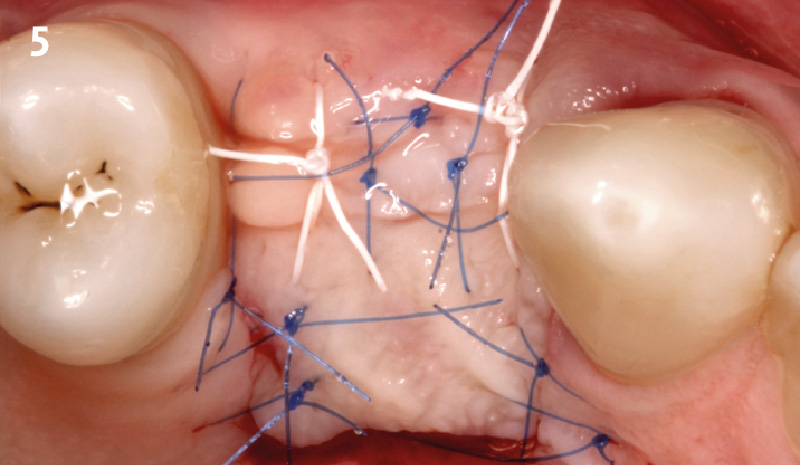
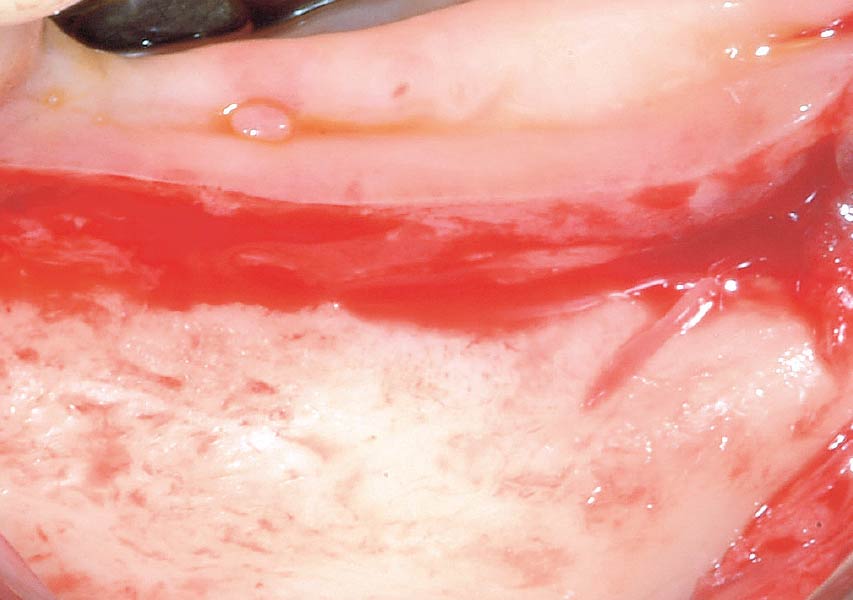
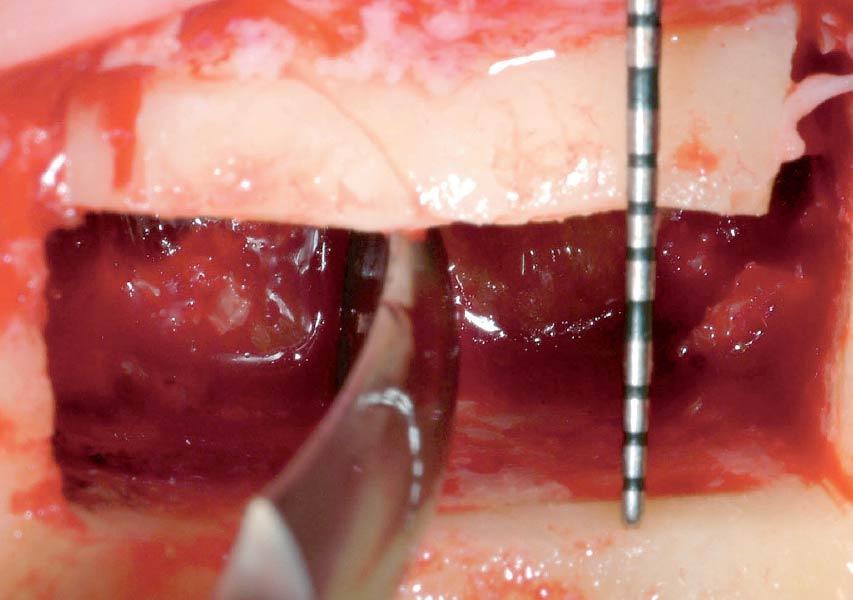
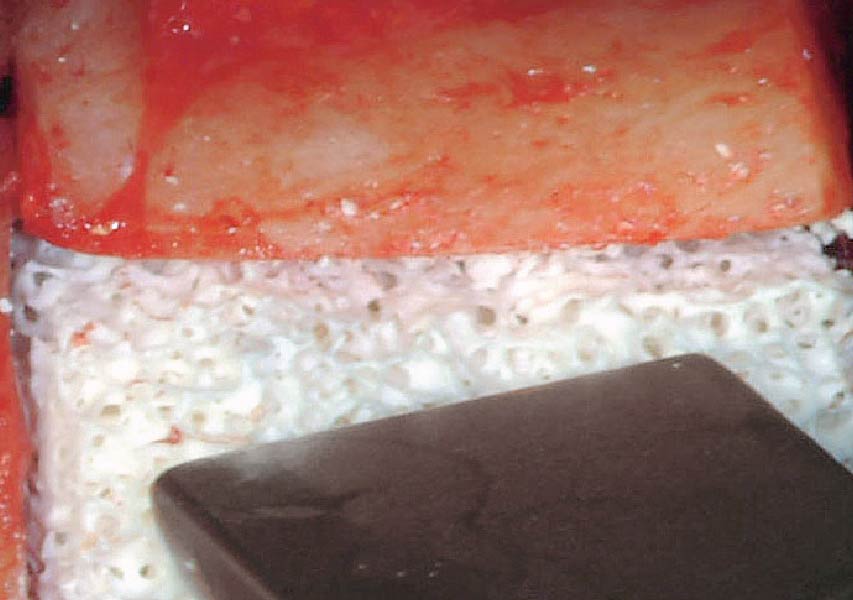
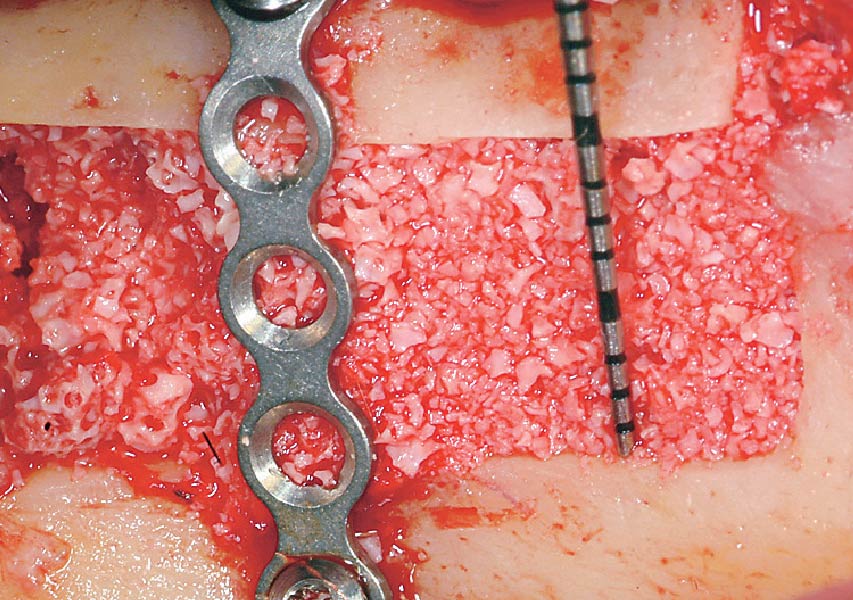
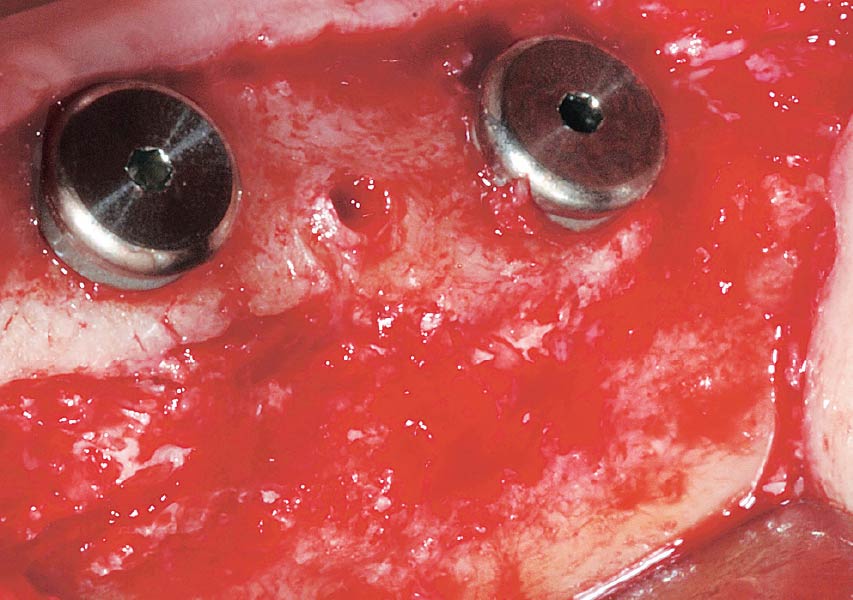
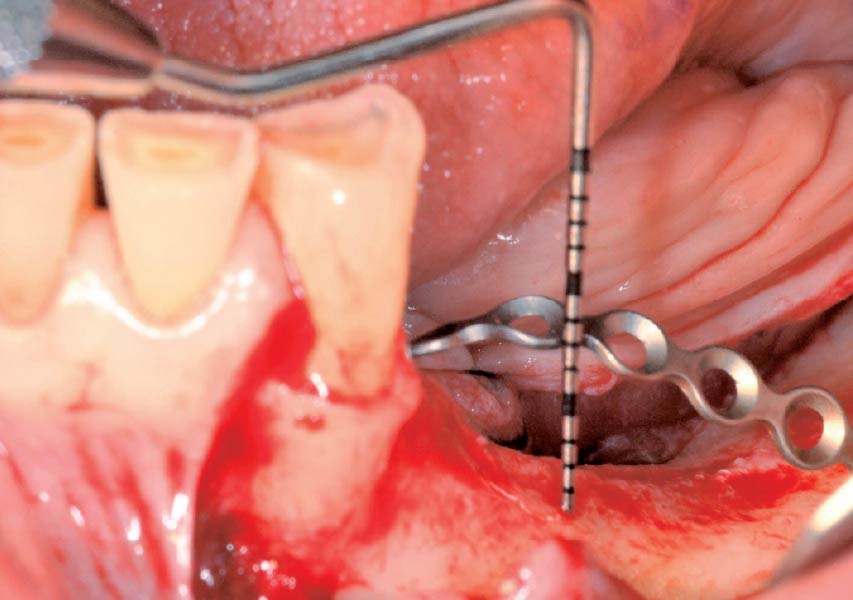
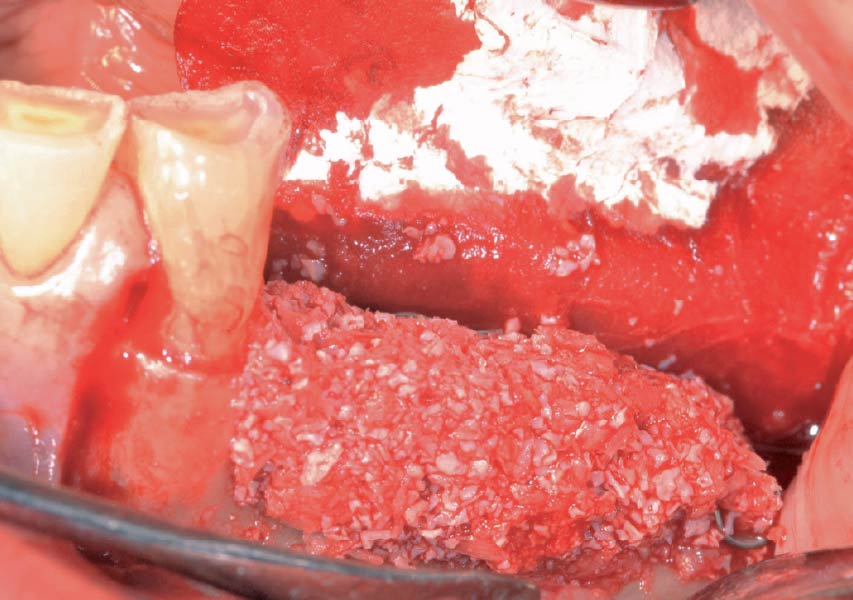
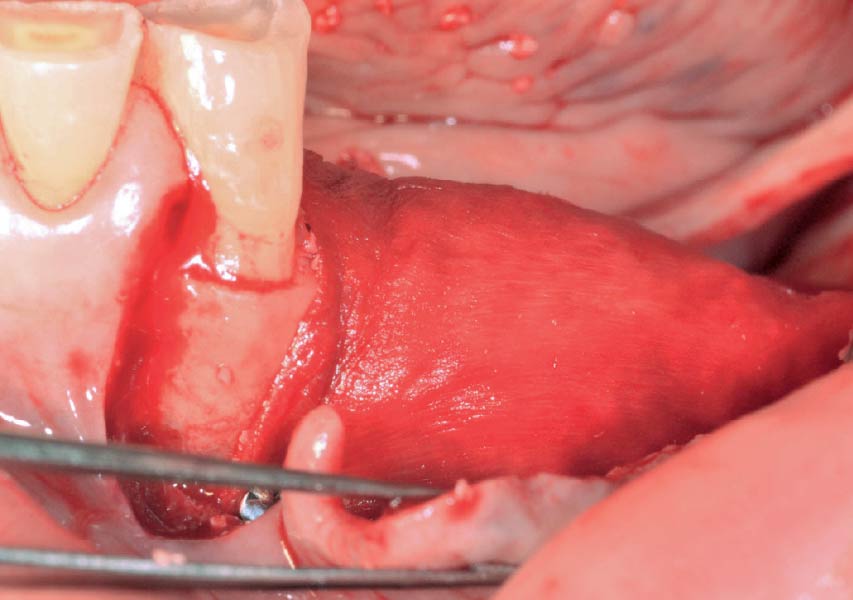
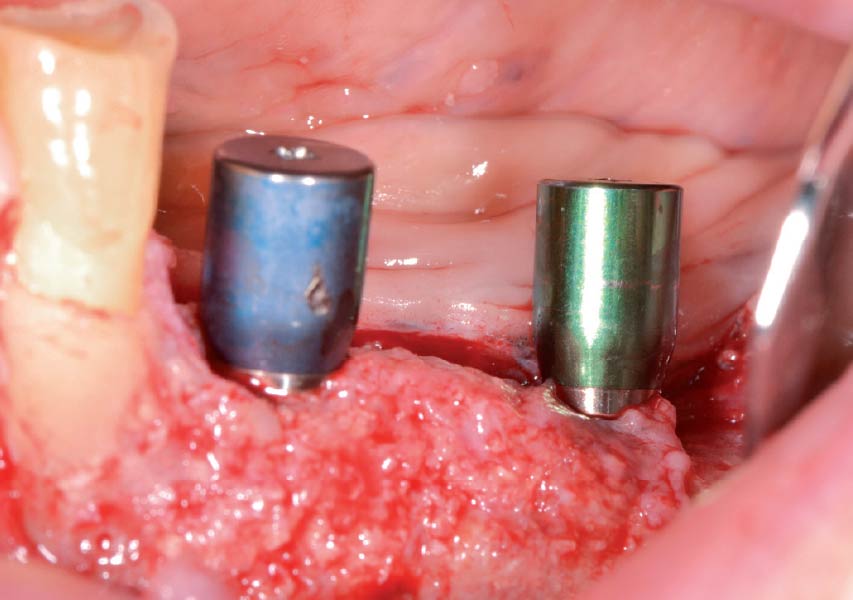
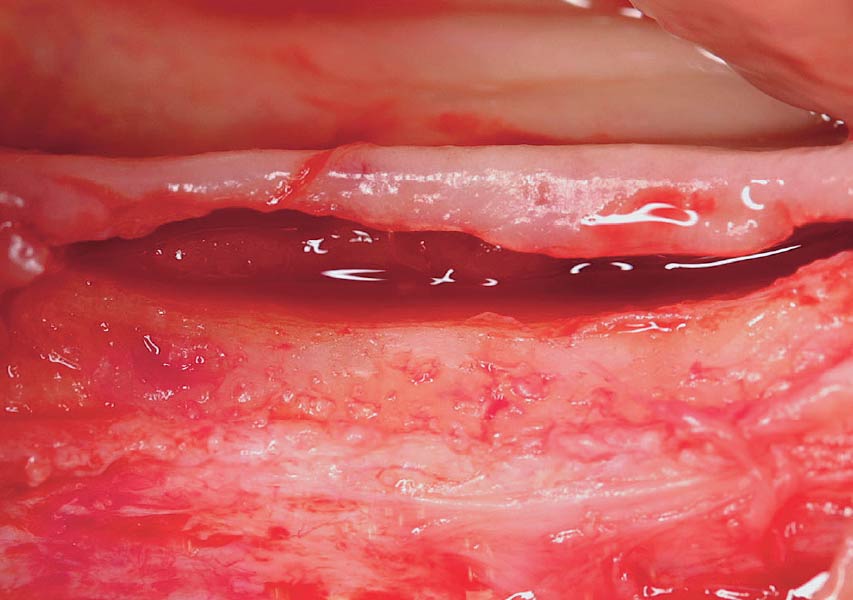
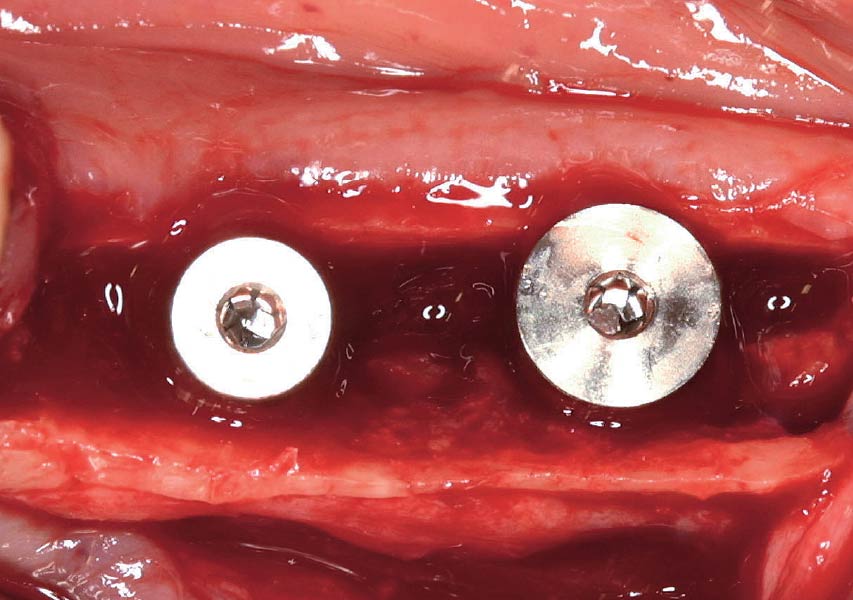
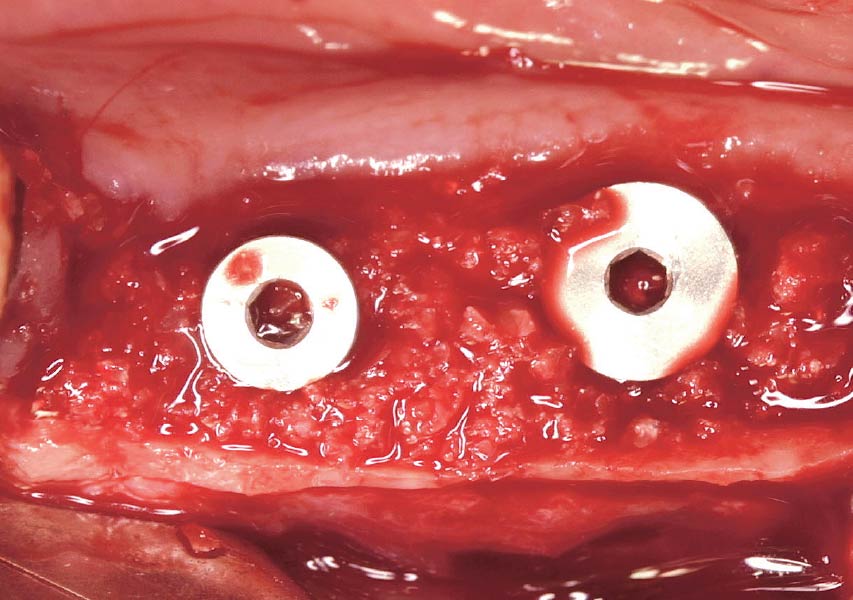
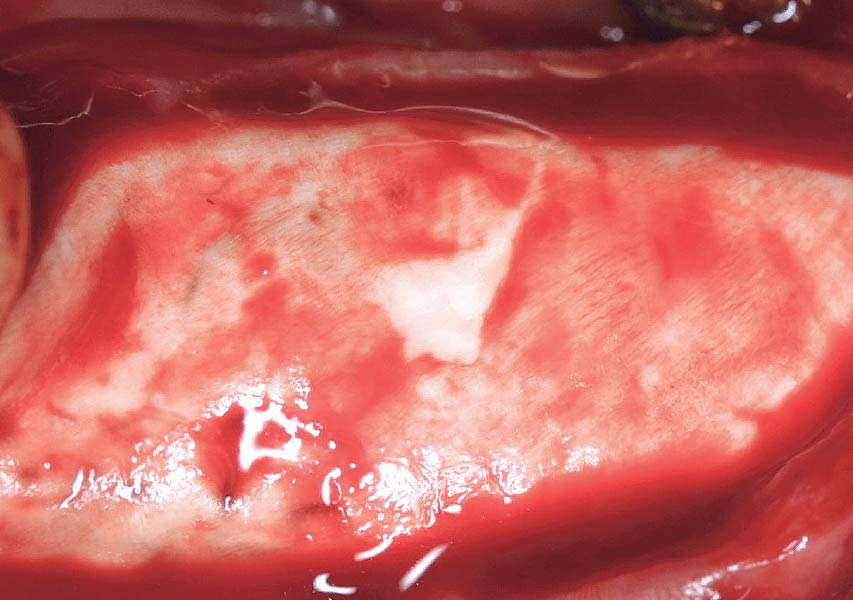
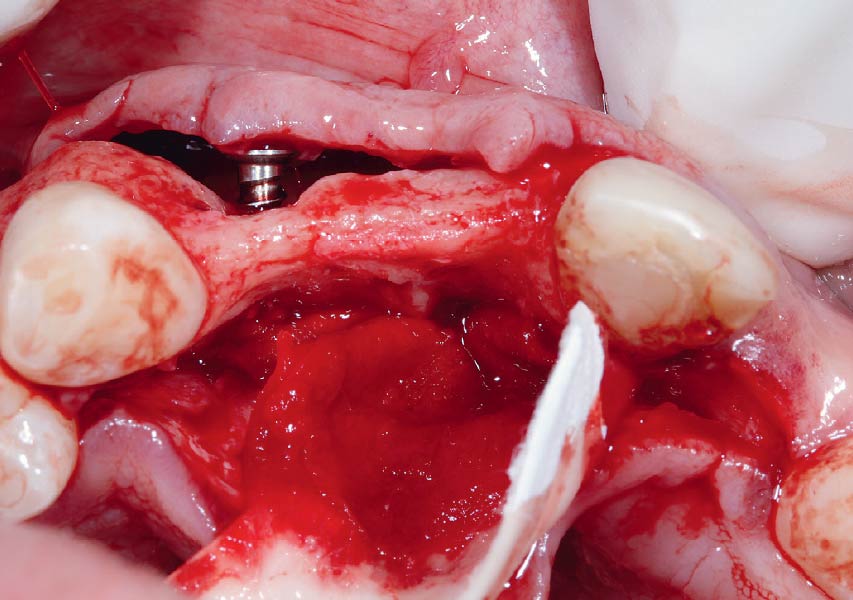
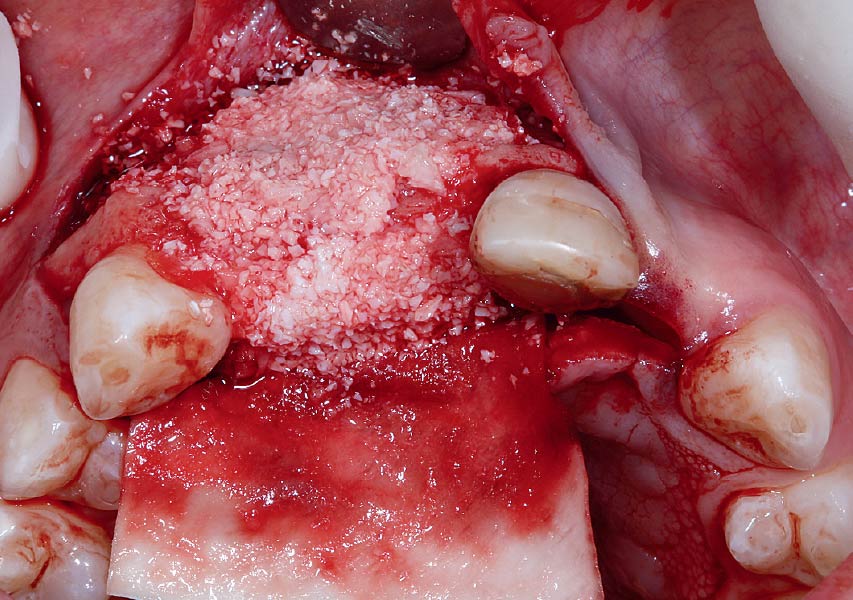
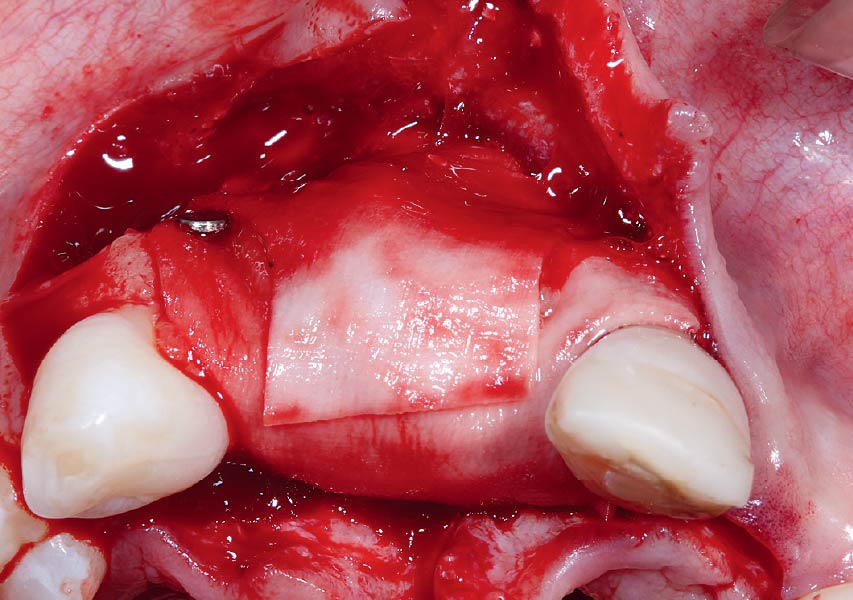
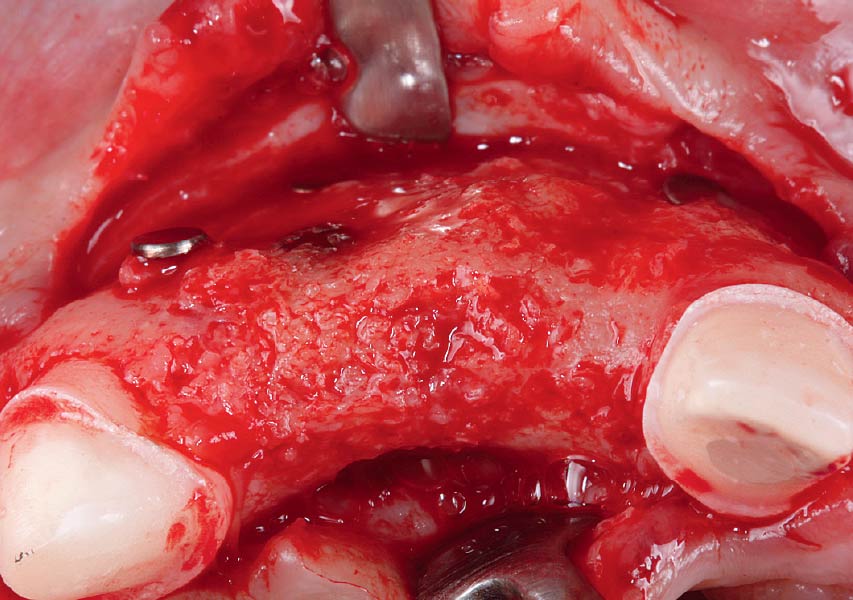
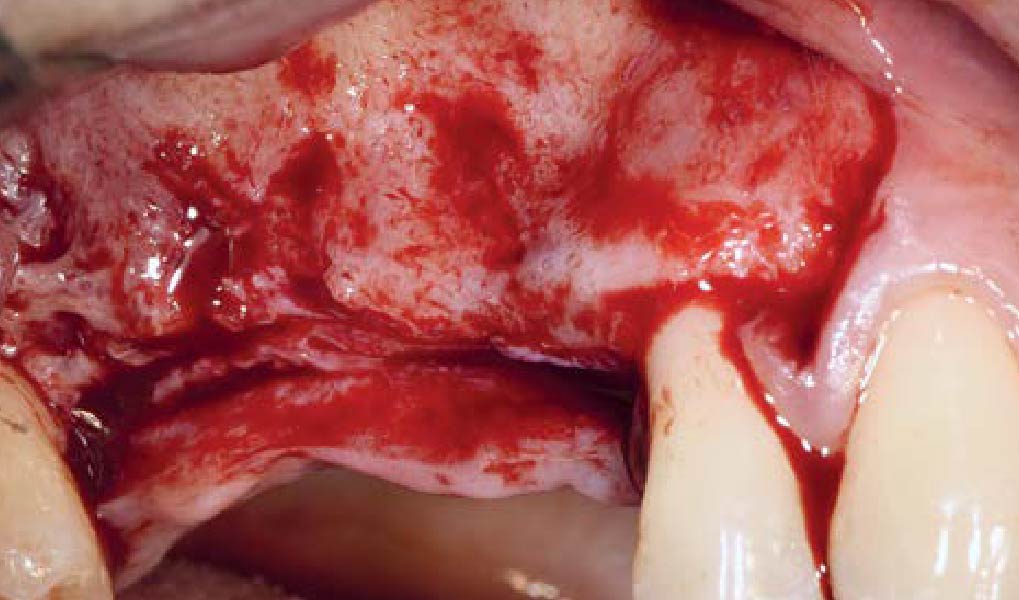
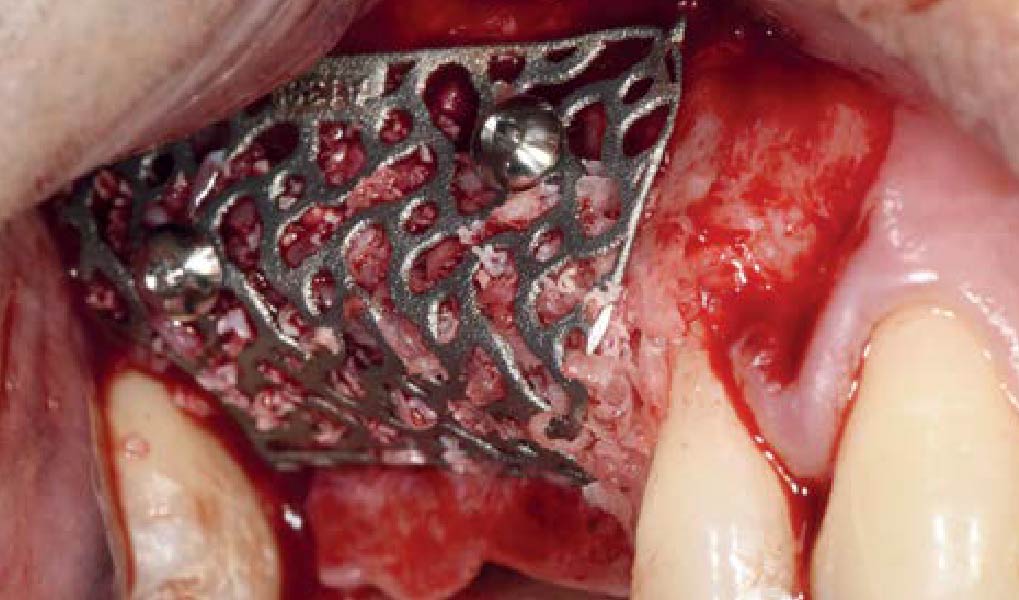
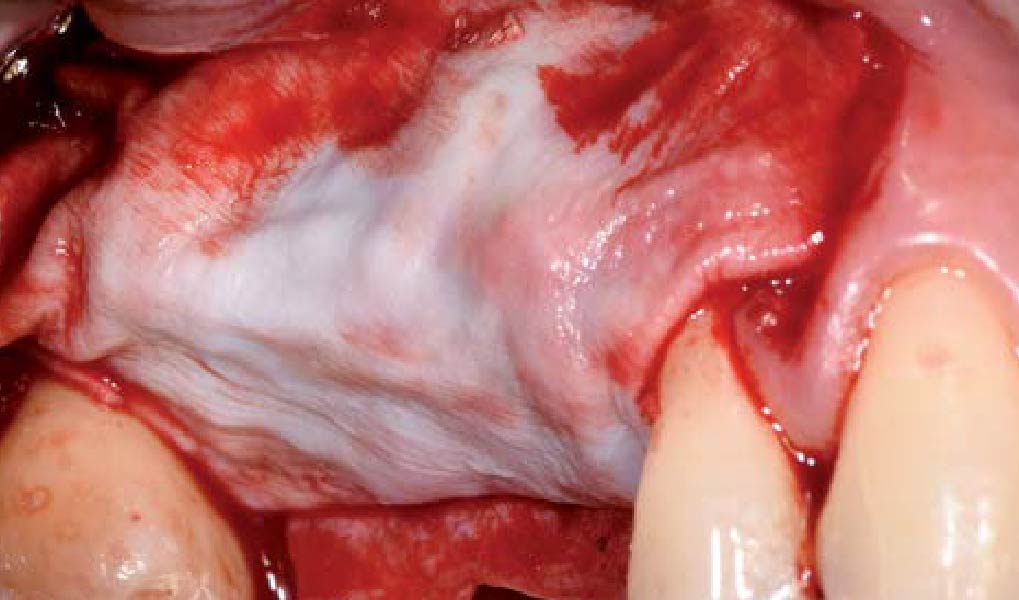
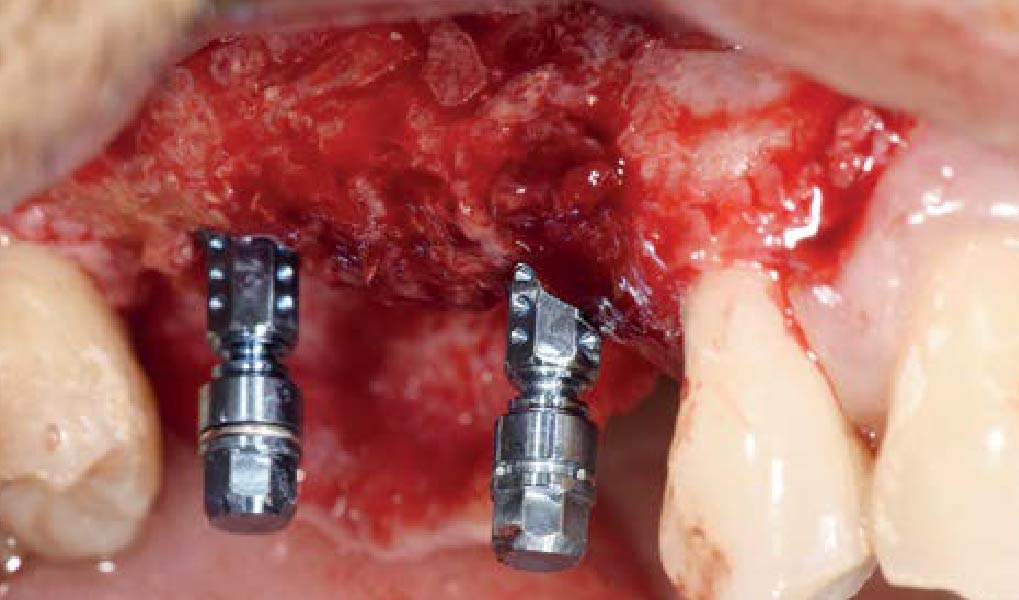
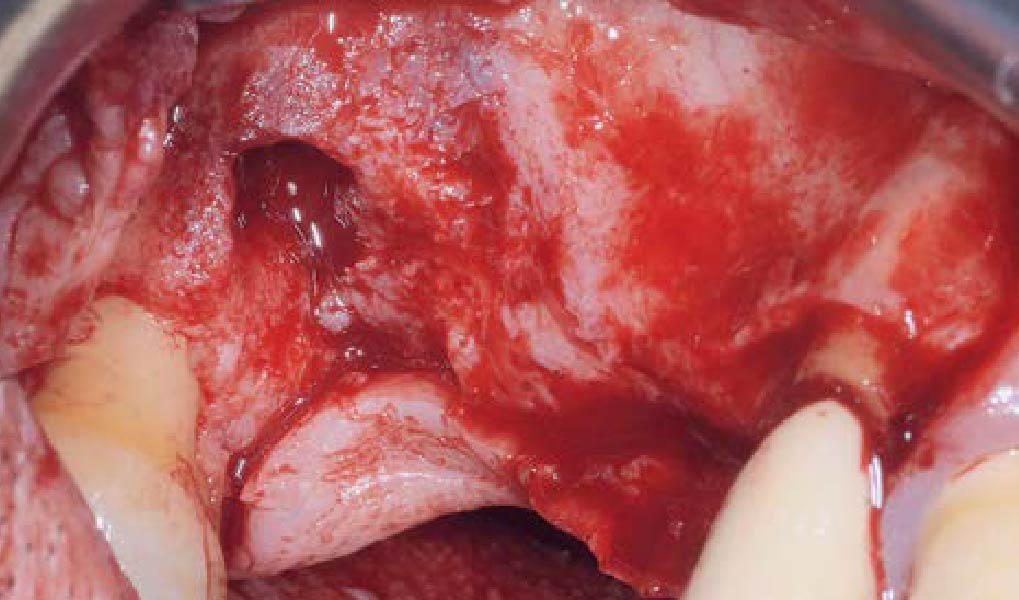
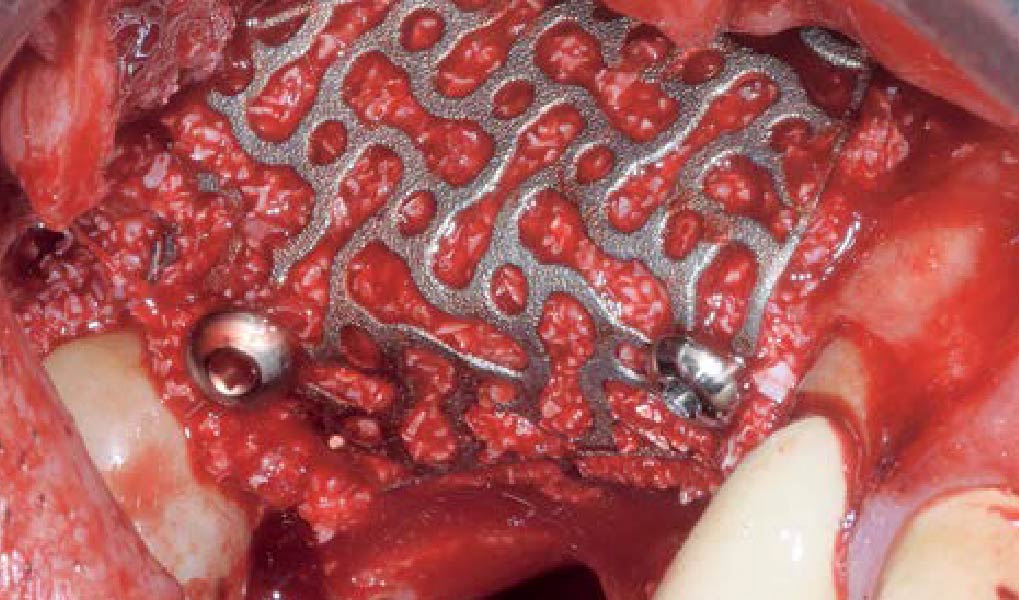
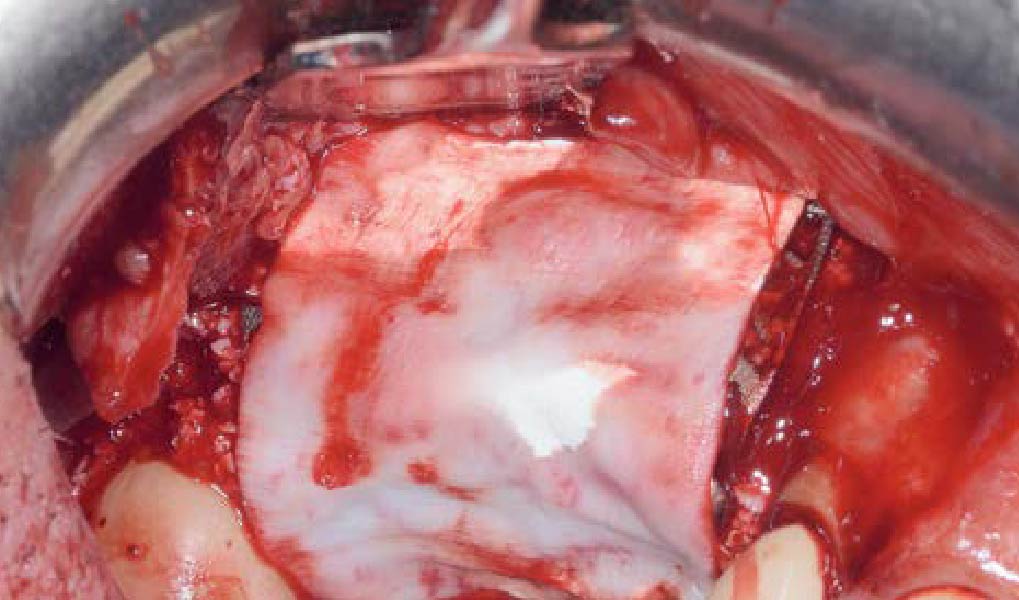
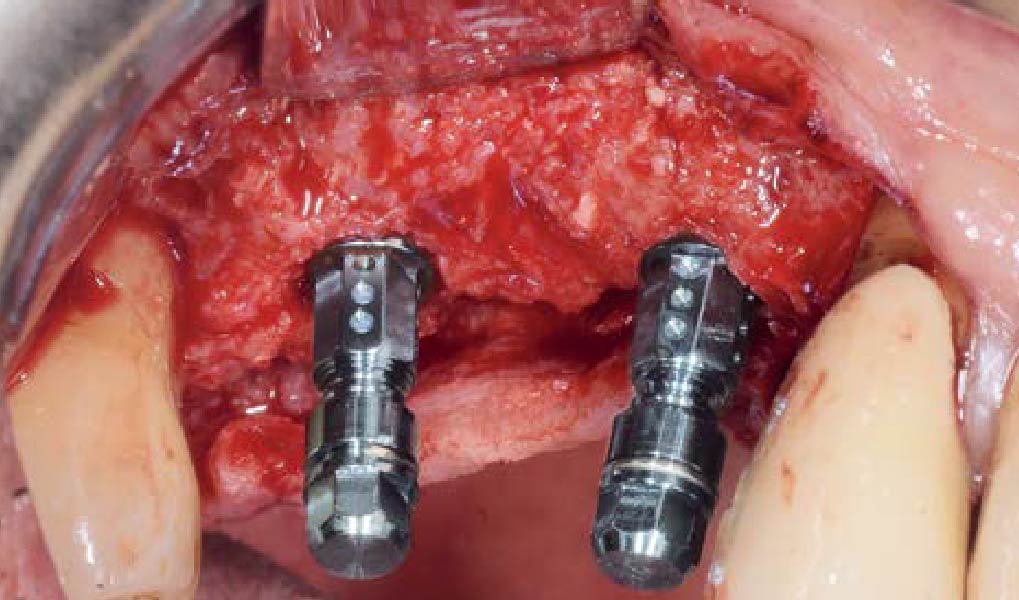
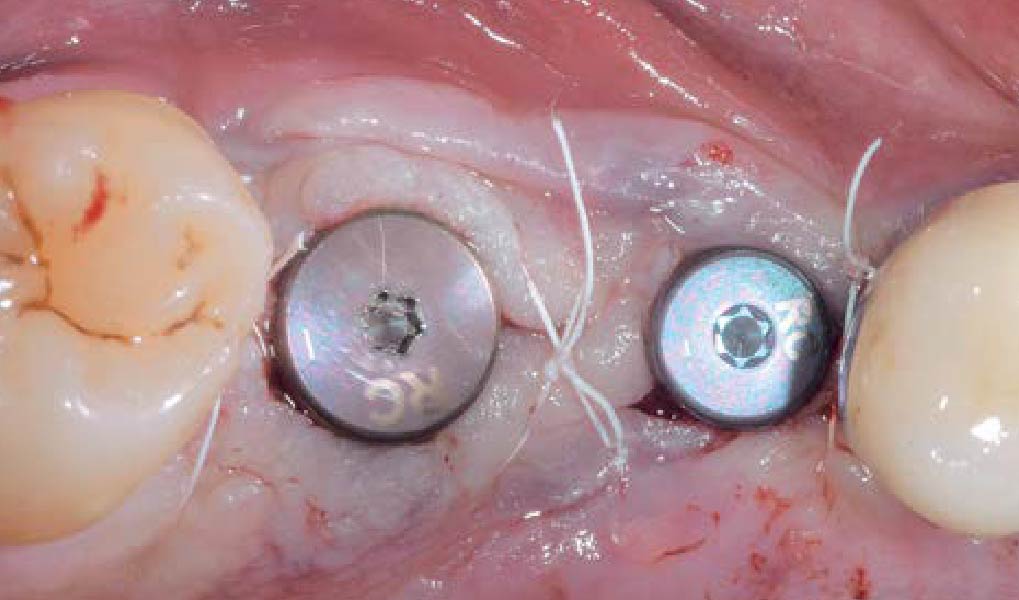
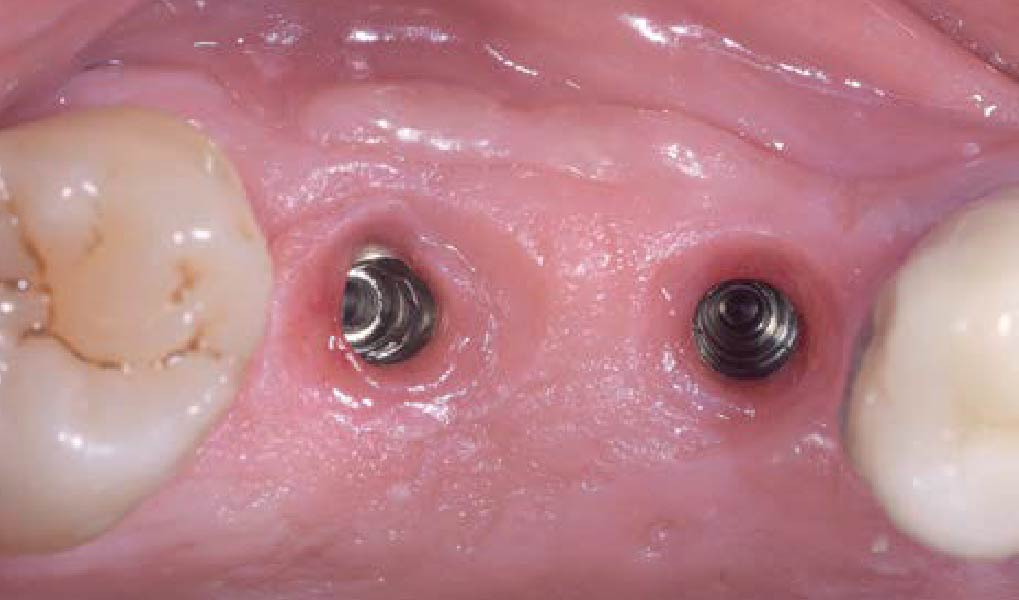
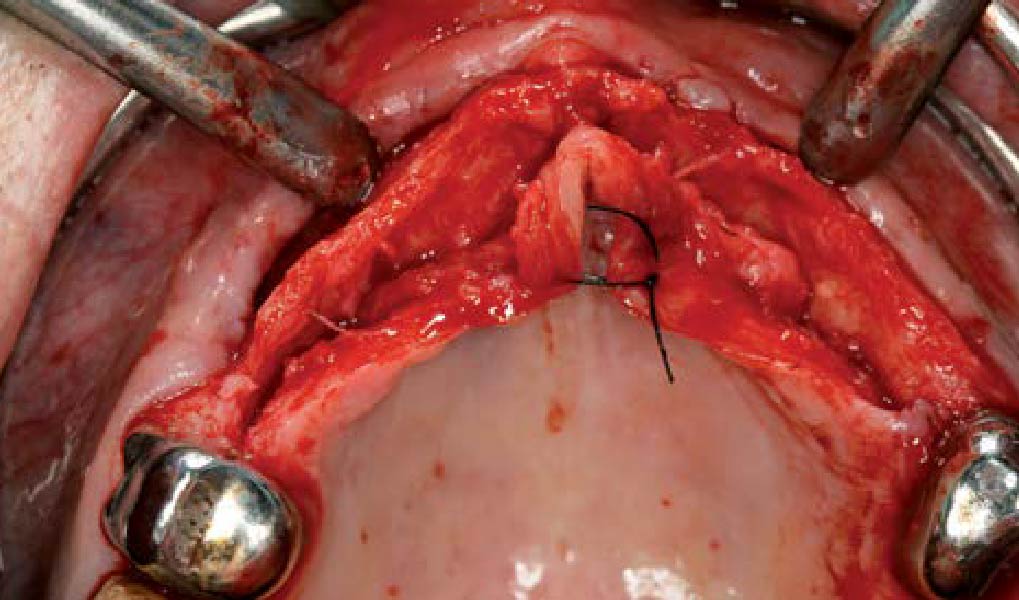
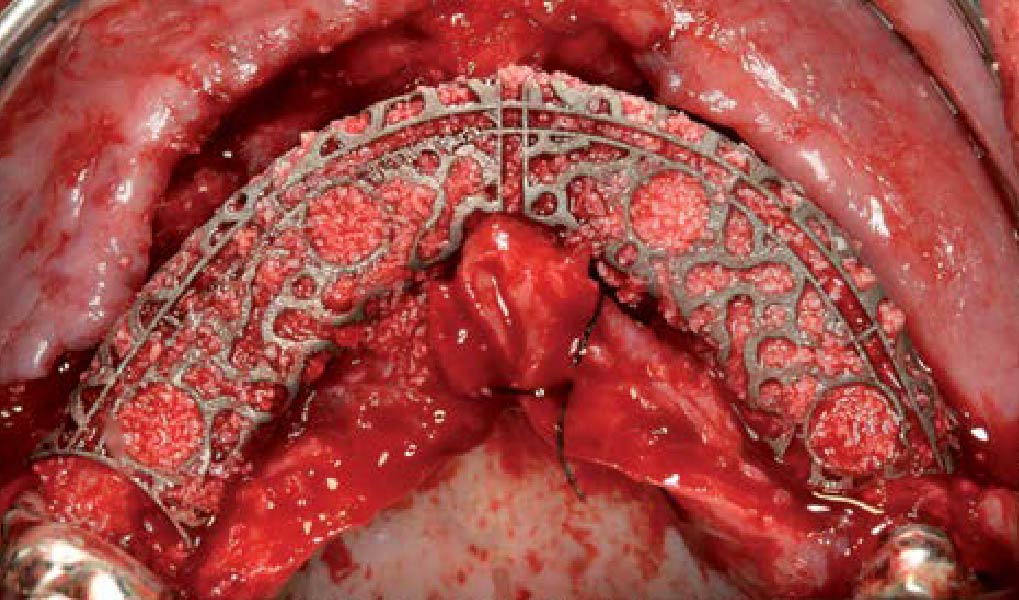
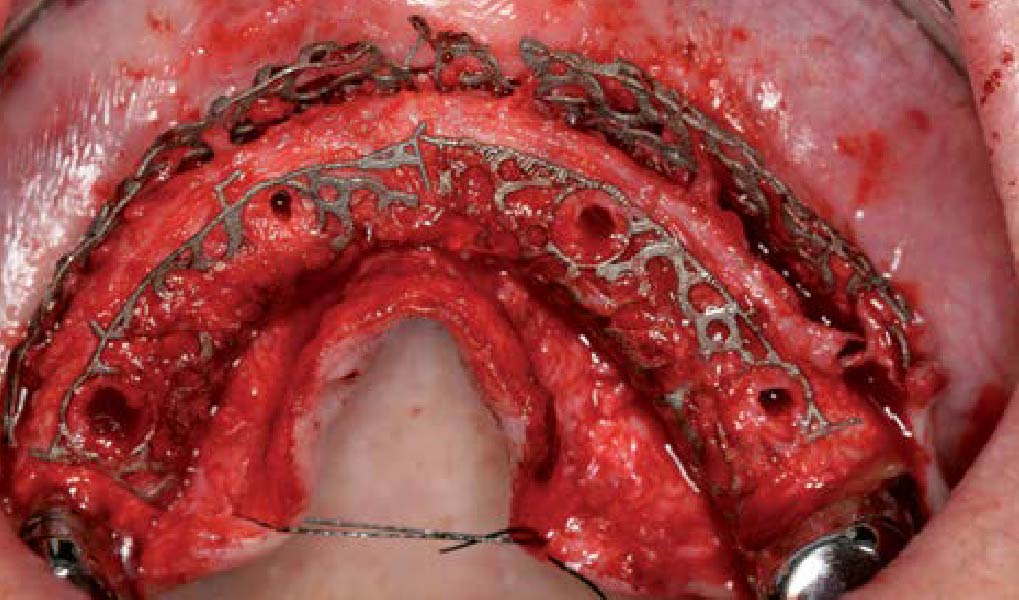
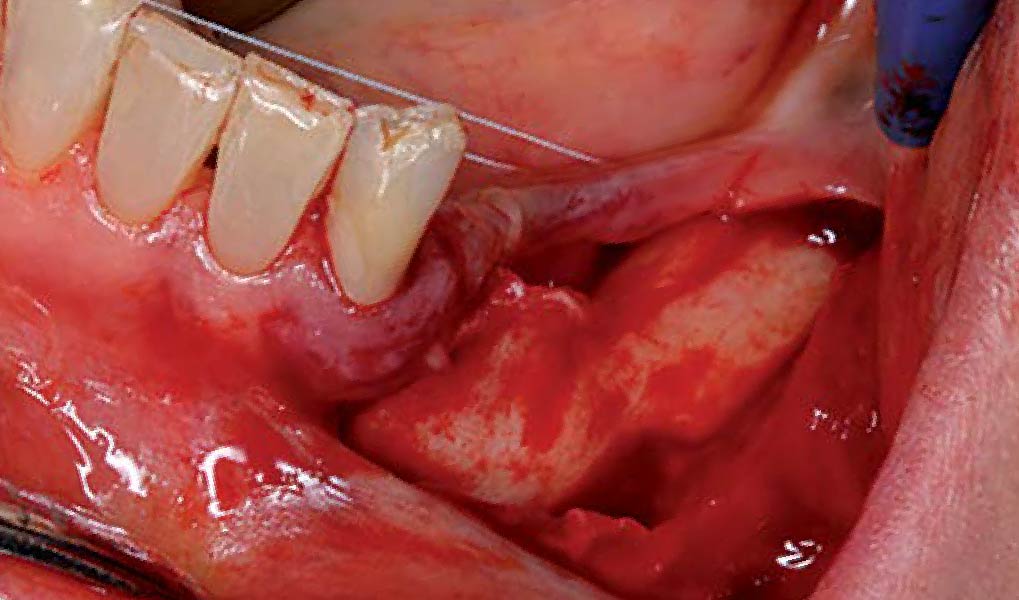
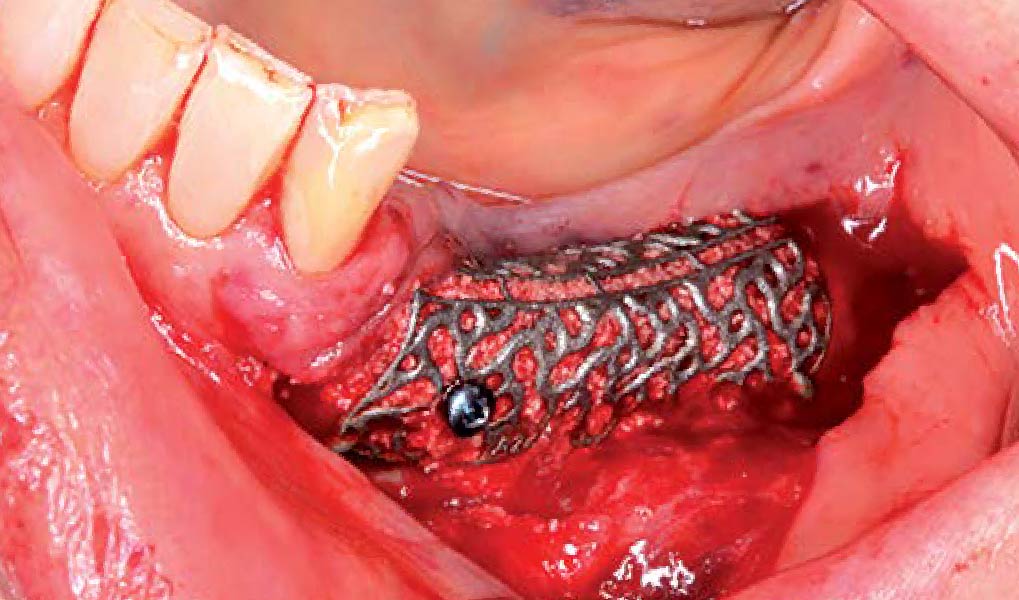
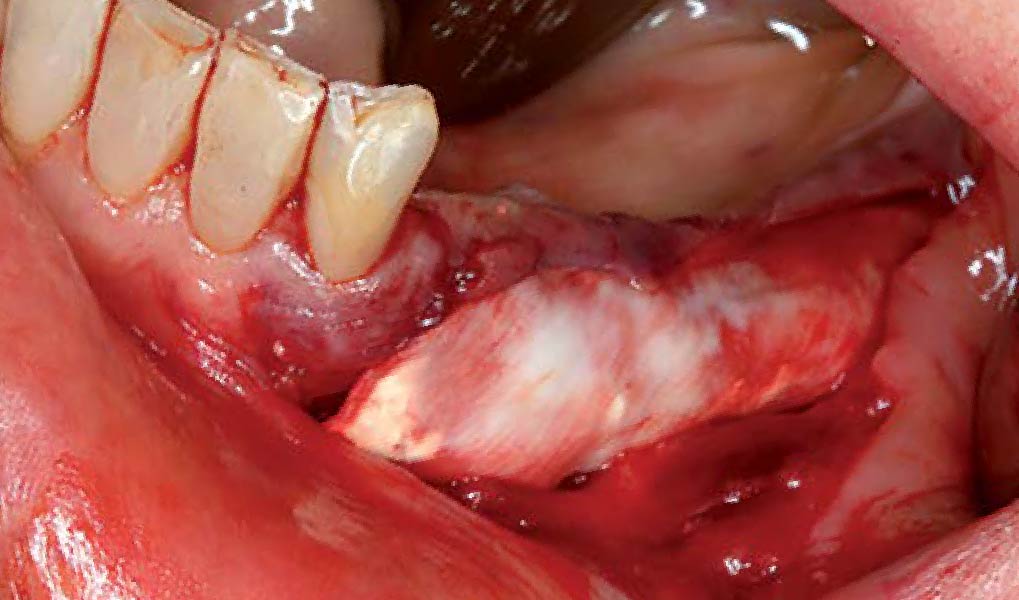
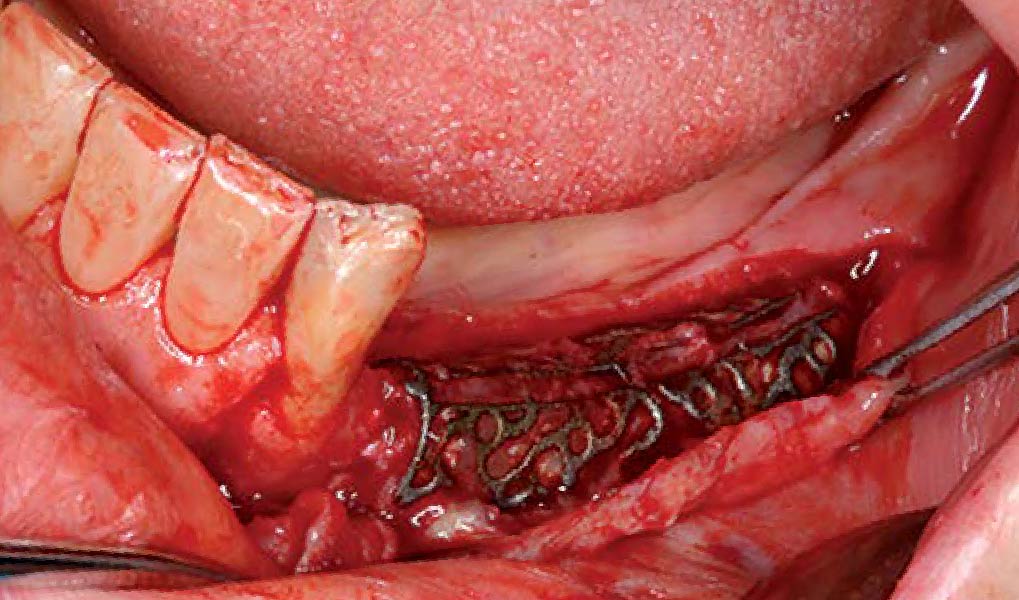
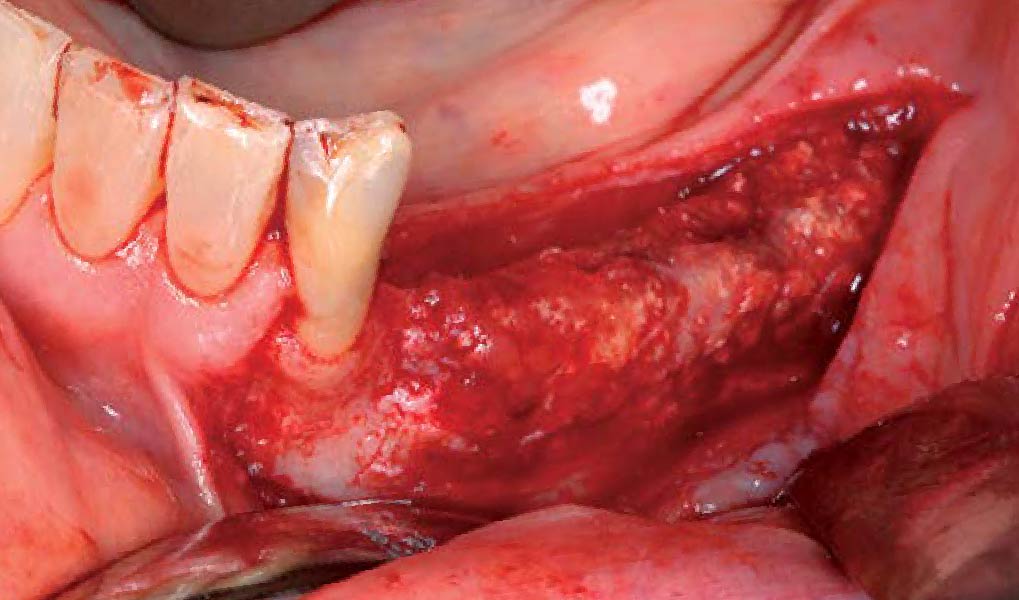
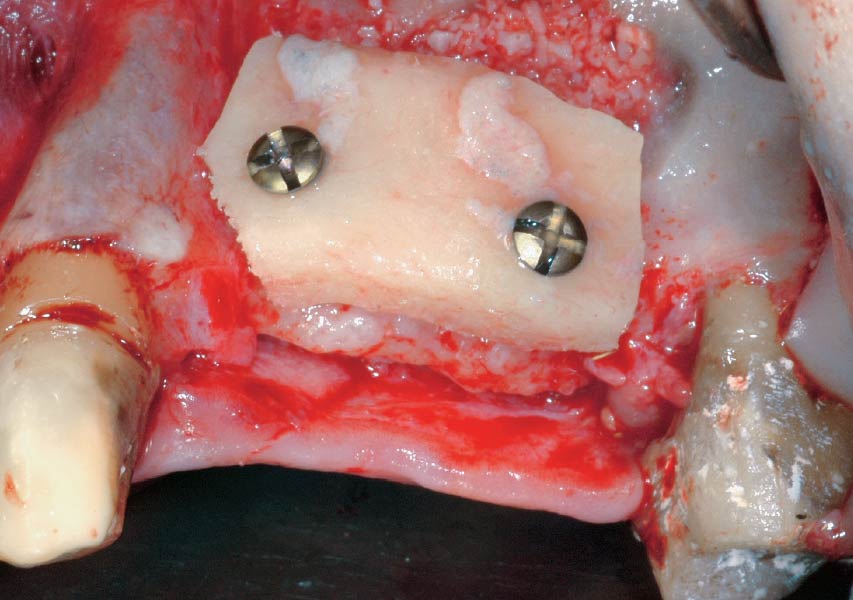
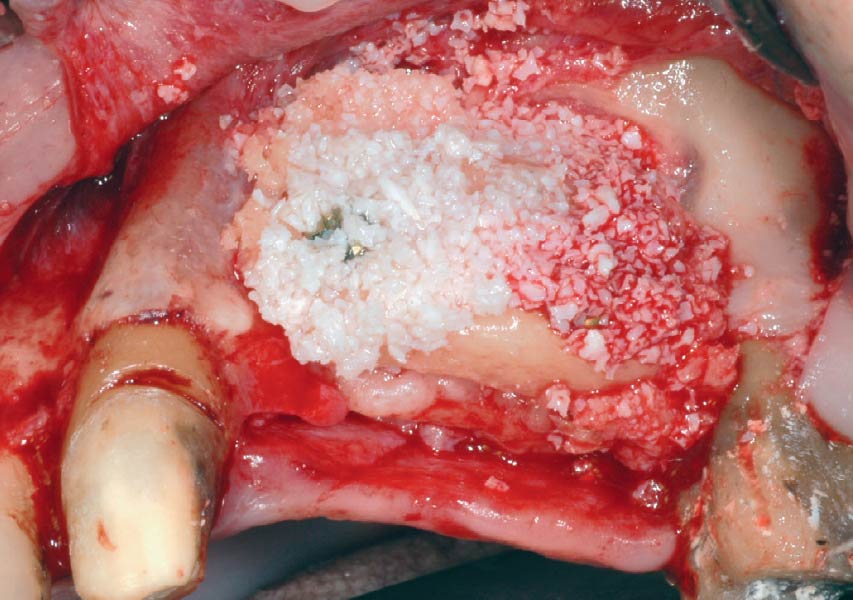
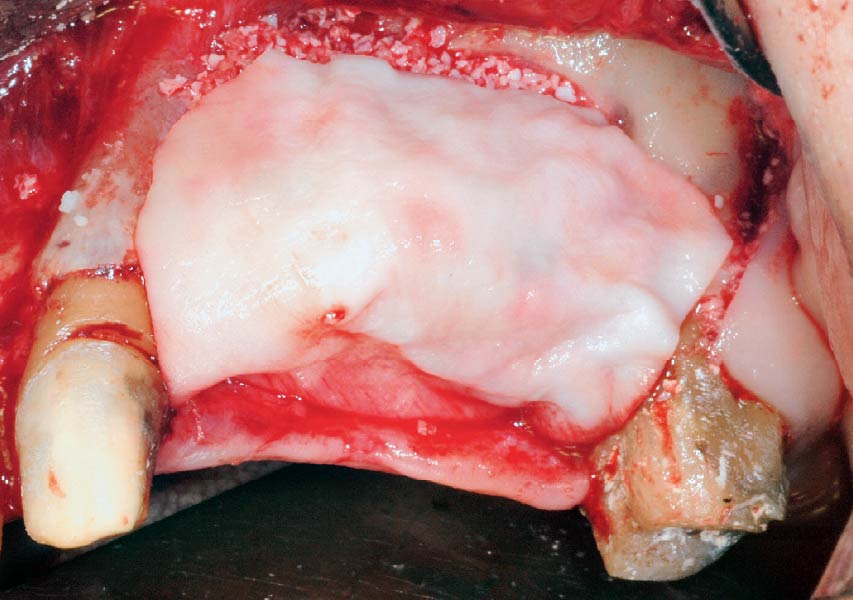
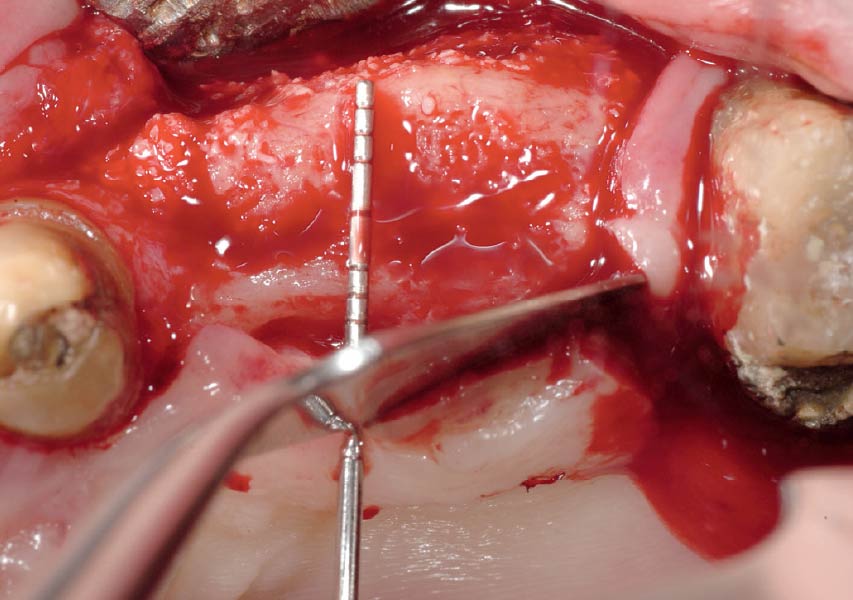
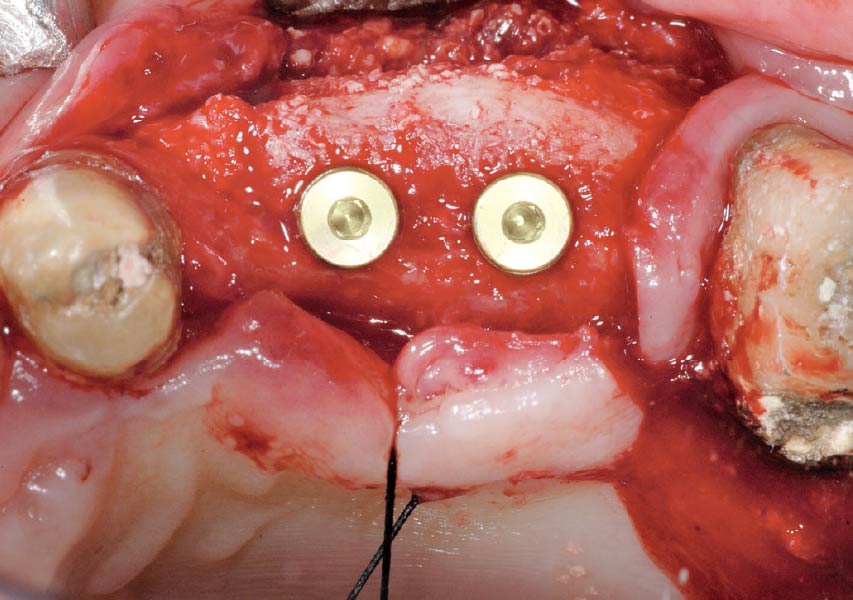
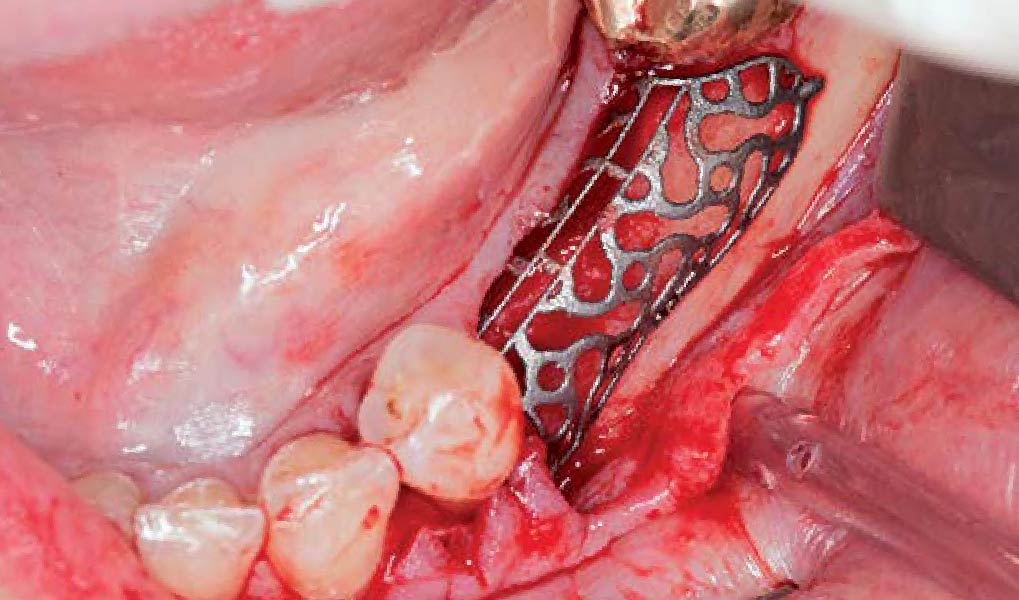
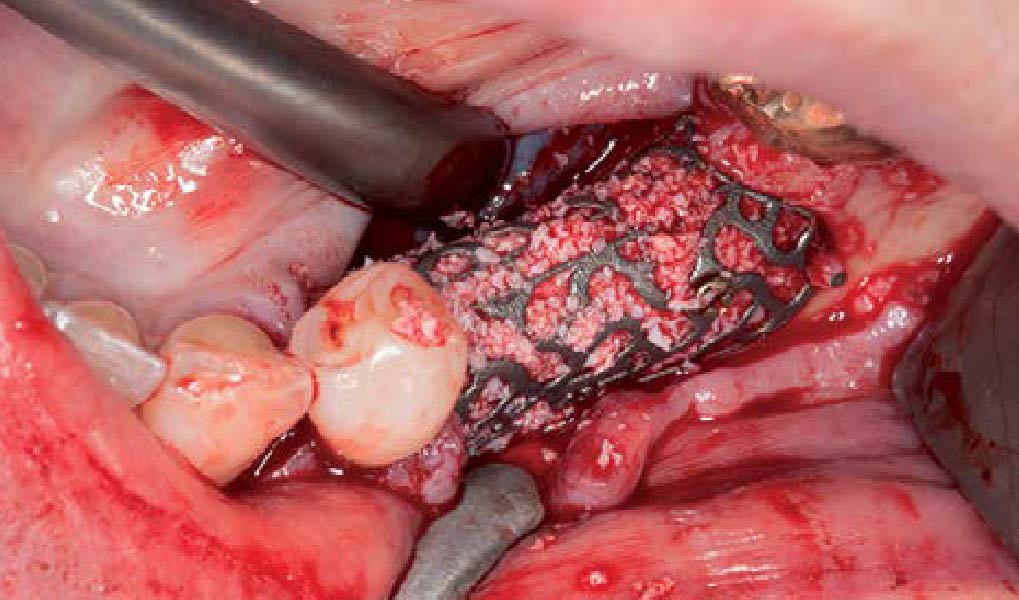
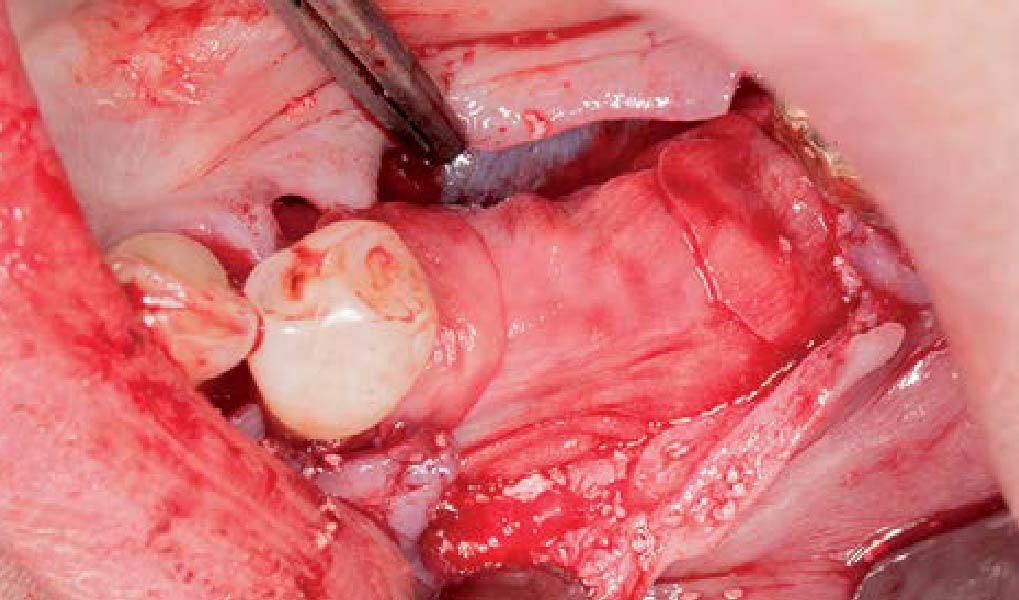
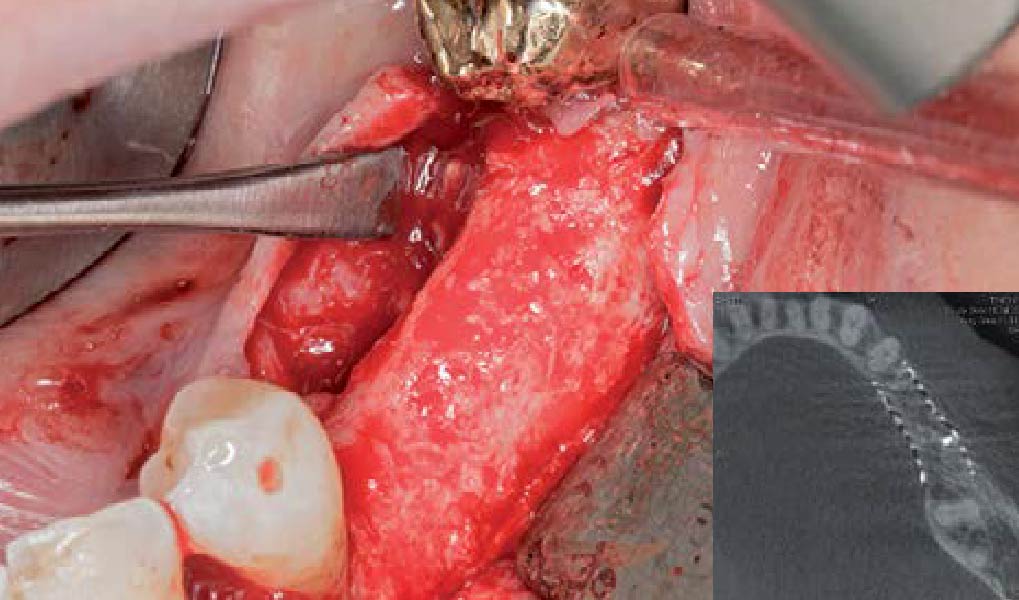
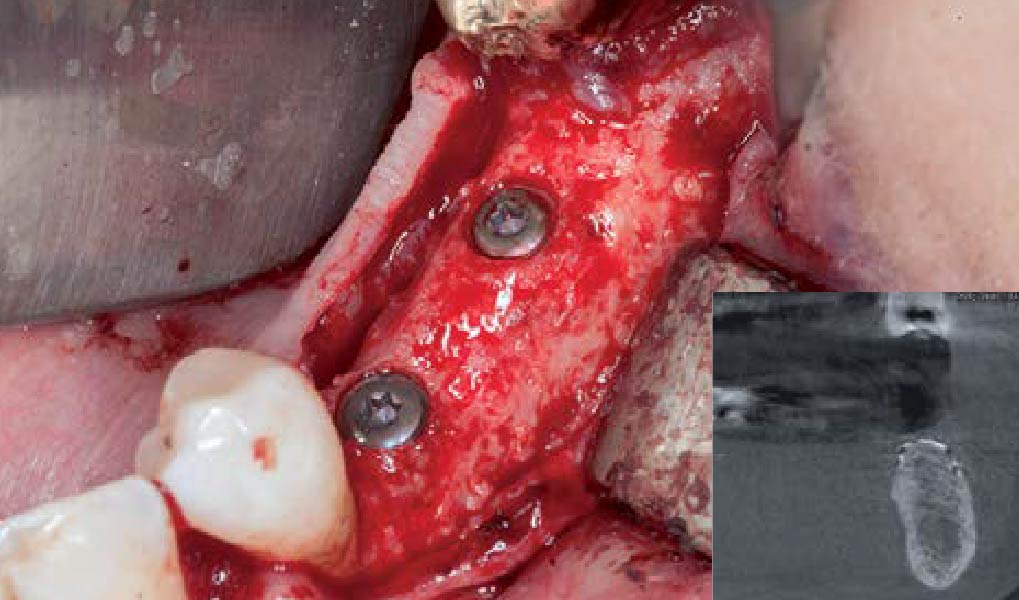
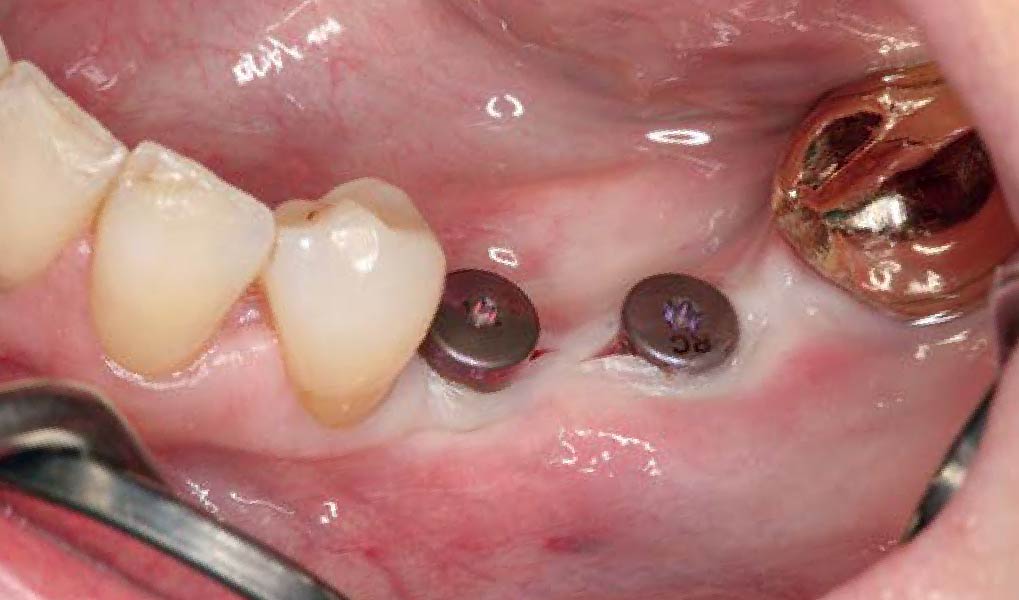
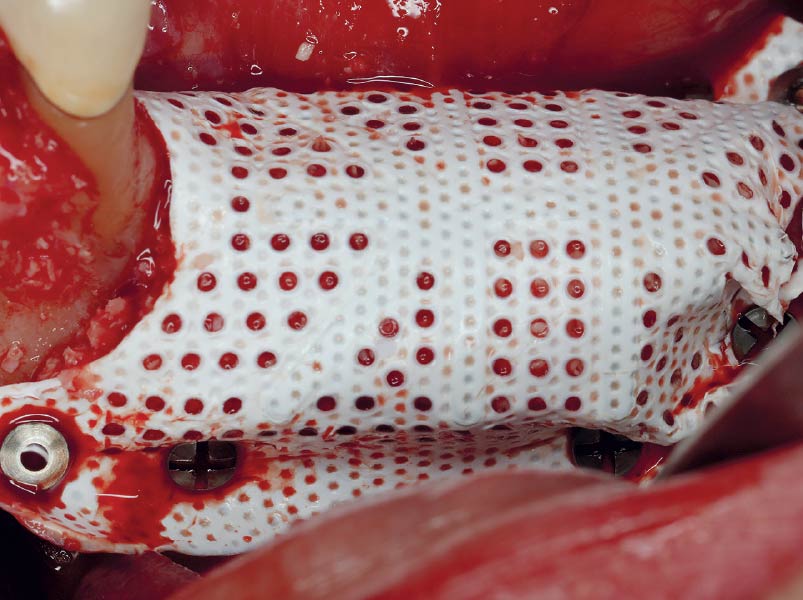
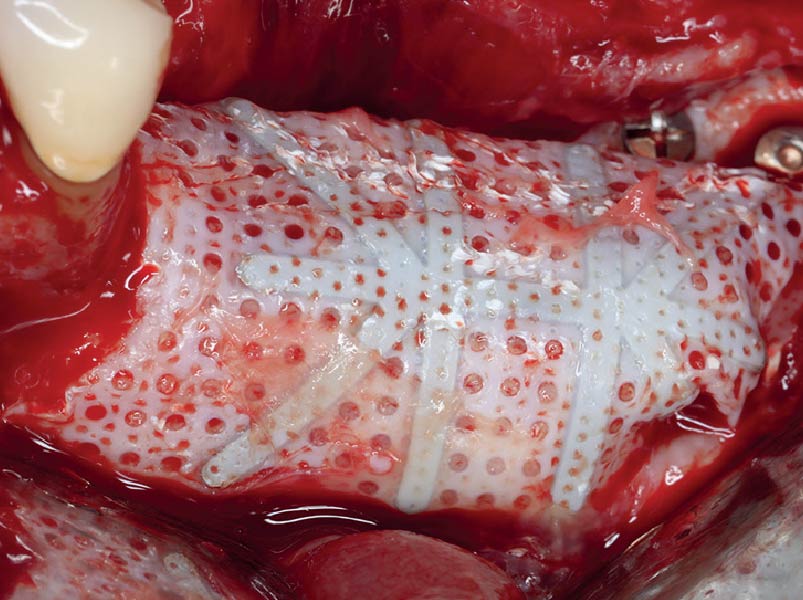
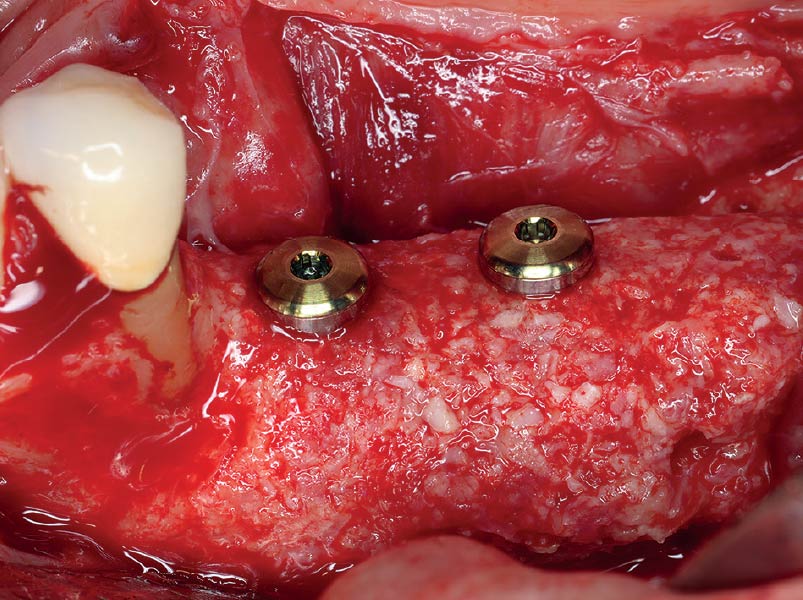
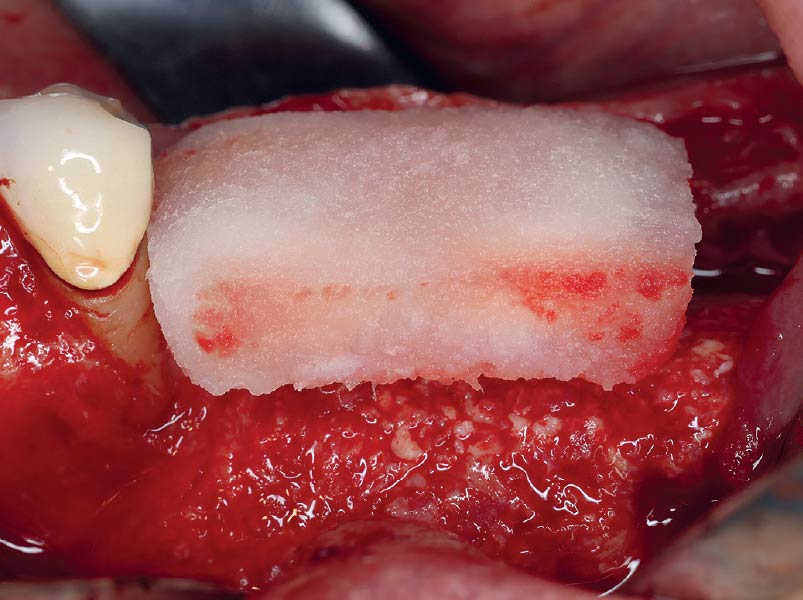
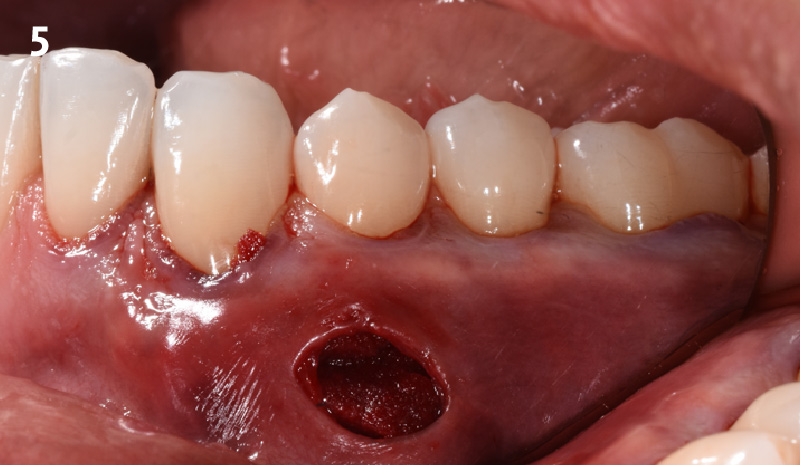
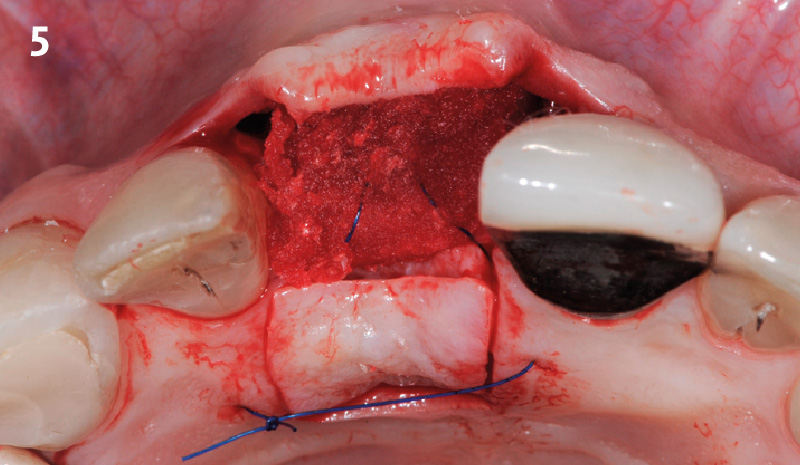
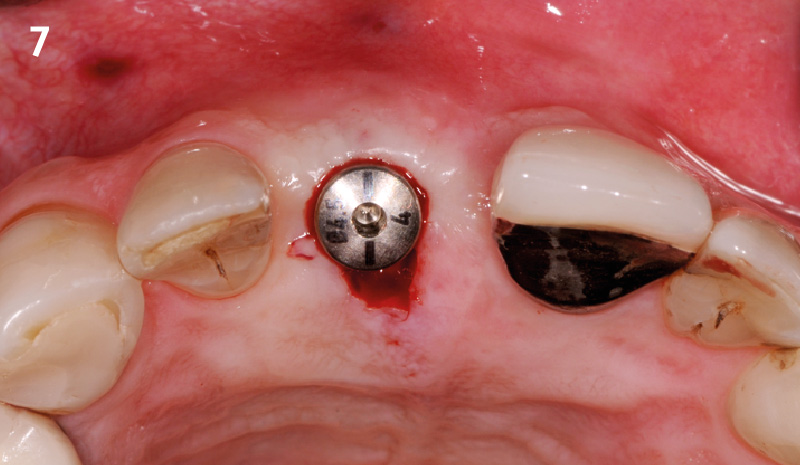
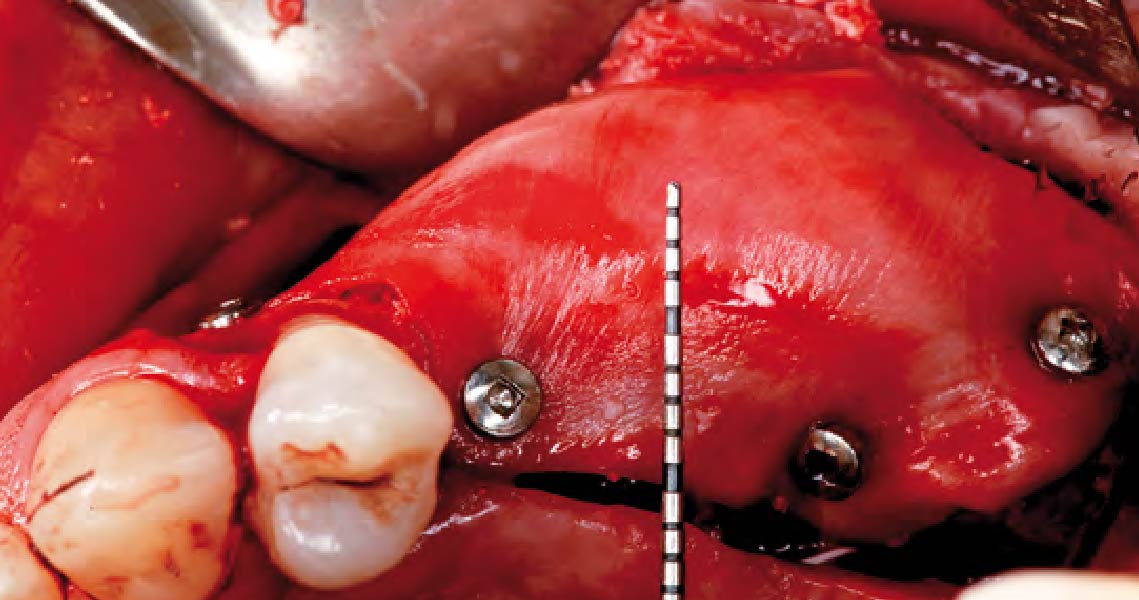
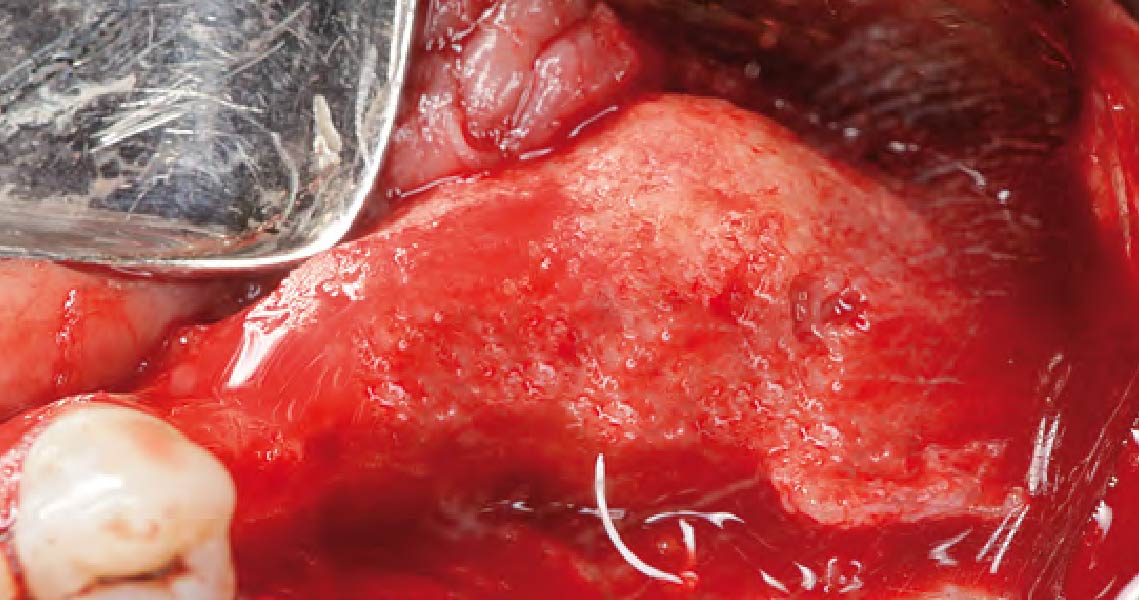
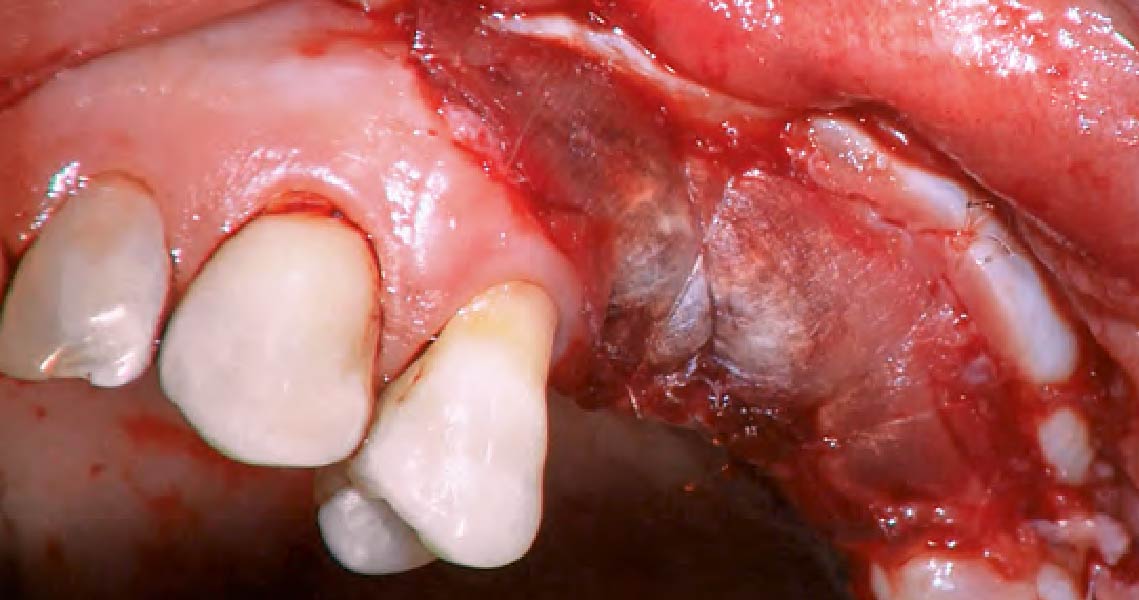
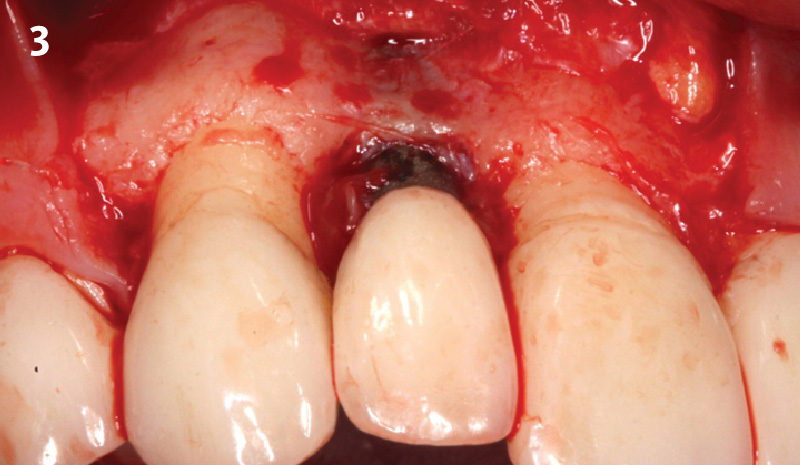
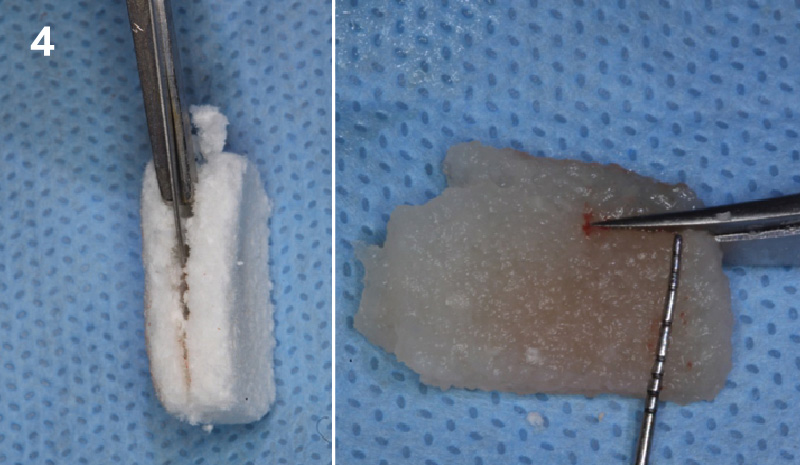
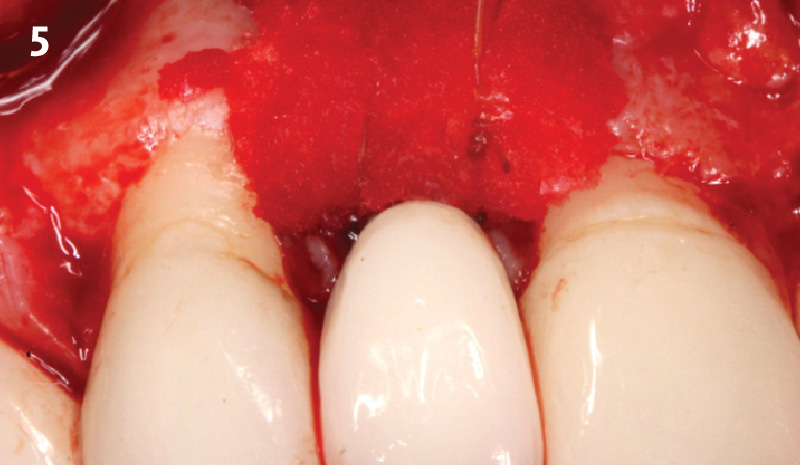
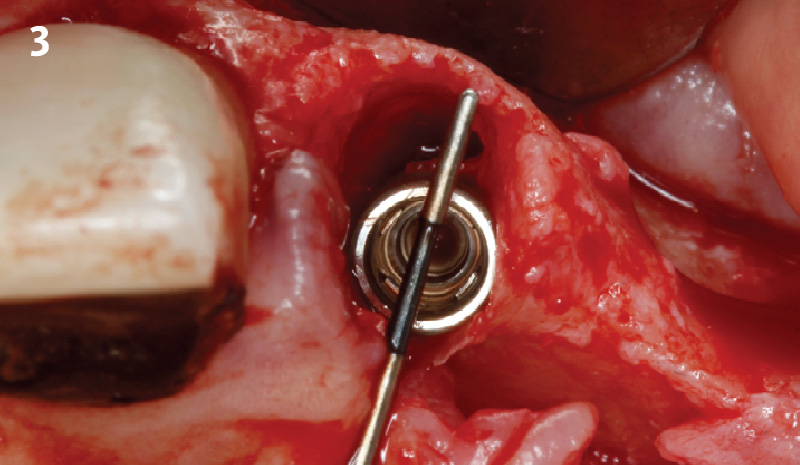
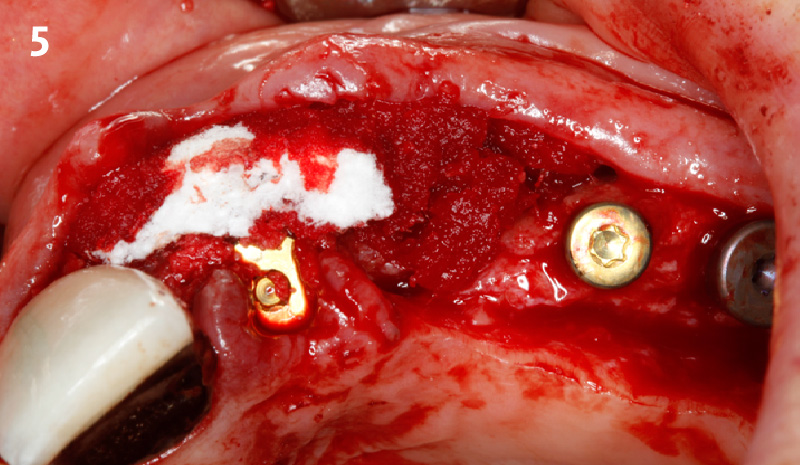
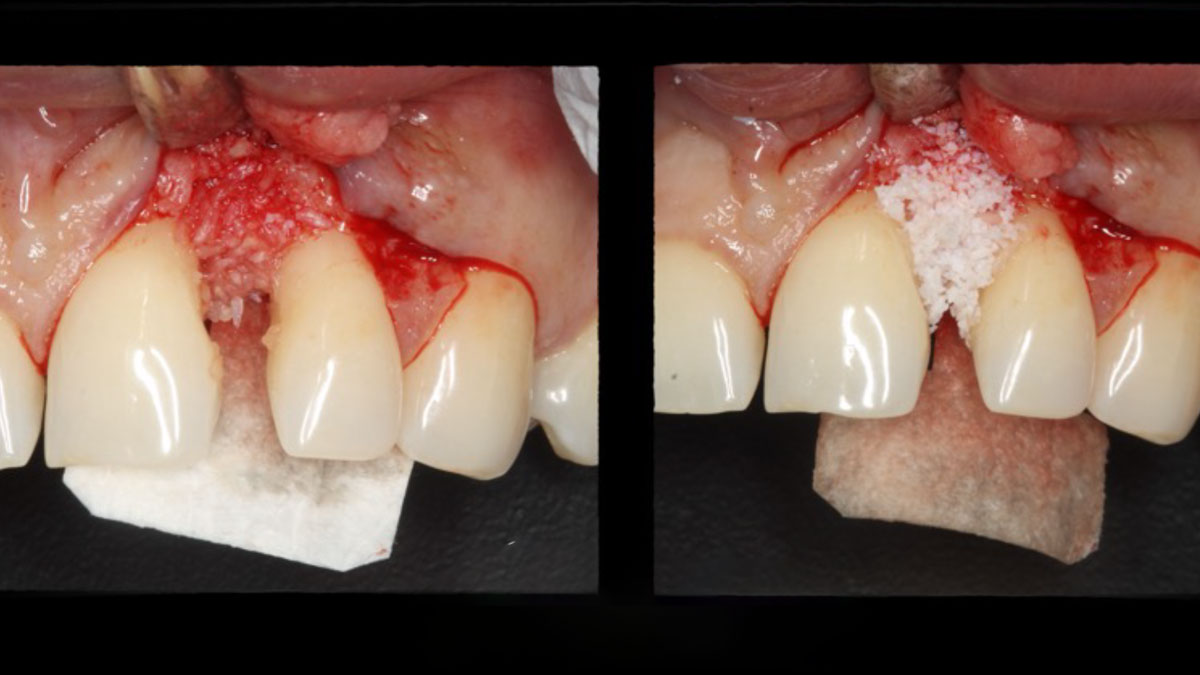
Area #9-10 was debrided and showed a wide 1-2 wall defect measuring ~7mm vertical bone loss. GTR procedure using Geistlich vallomix™ bone graft (allograft + xenograft) and a collagen membrane were employed and primary closure obtained. Healing at 2 and 4 weeks and 6 months showed proper bone fill with stable periodontium.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system | Light smoker | Impaired immune system |
| Patient’s esthetic requirements | Low | Medium | High |
| Height of smile line | Low | Medium | High |
| Gingival biotype | Thick – “low scalloped” | Medium – “medium scalloped” | Thin – “high scalloped” |
| Shape of dental crowns | Rectangular | Triangular | |
| Infection at implant sight | None | Chronic | Acute |
| Bone height at adjacent tooth site | ≤ 5 mm from contact point | 5.5 – 6.5 mm from contact point | ≥ 7 mm from contact point |
| Restorative status of adjacent tooth | Intact | Restored | |
| Width of tooth gap | 1 tooth (≥ 7 mm) | 1 tooth (≤ 7 mm) | 2 teeth or more |
| Soft-tissue anatomy | Intact | Compromised | |
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
THE APPROACH
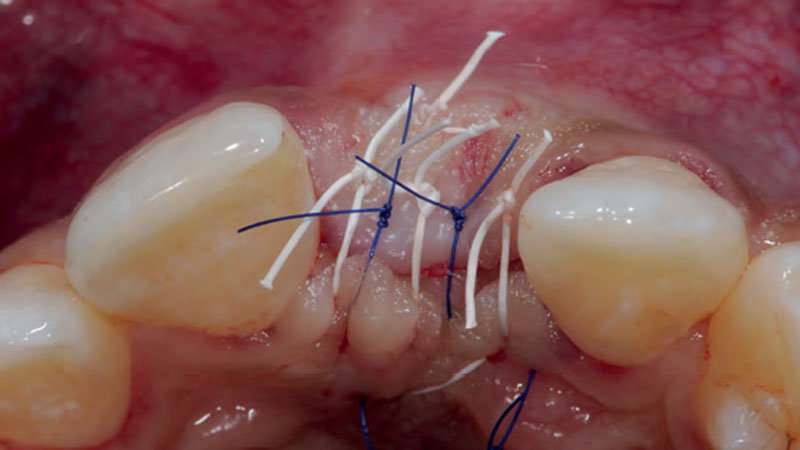
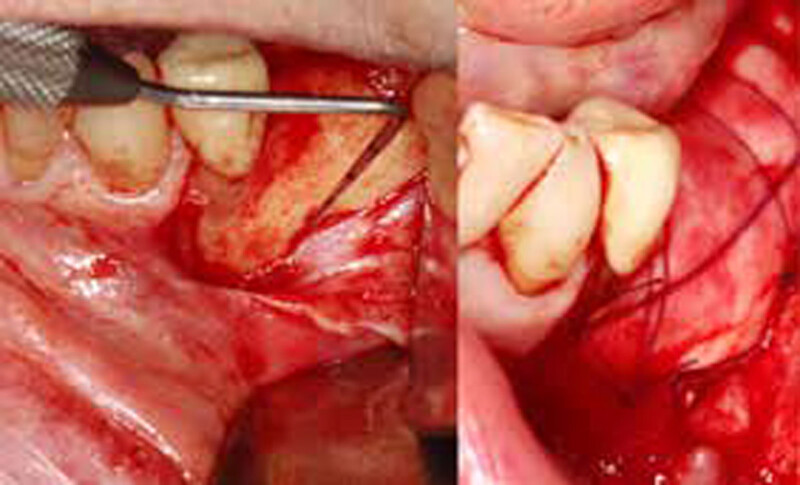
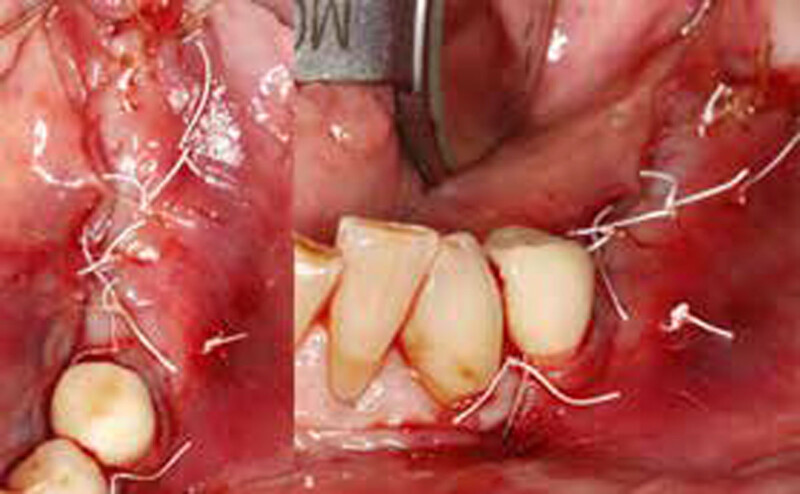
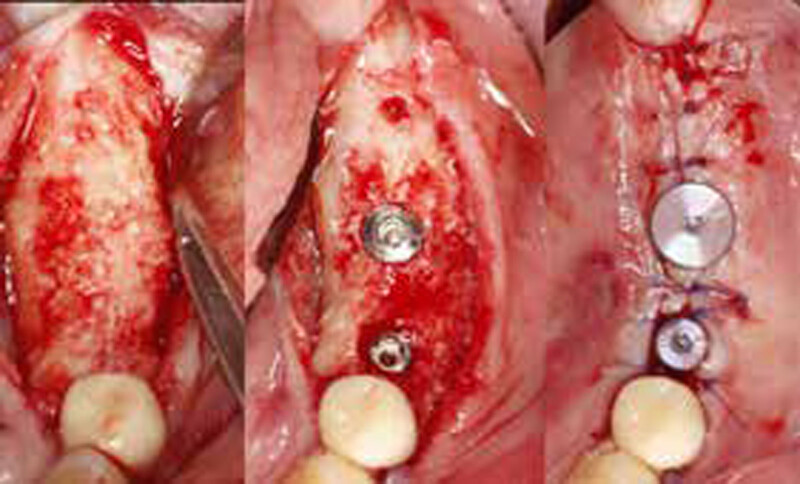
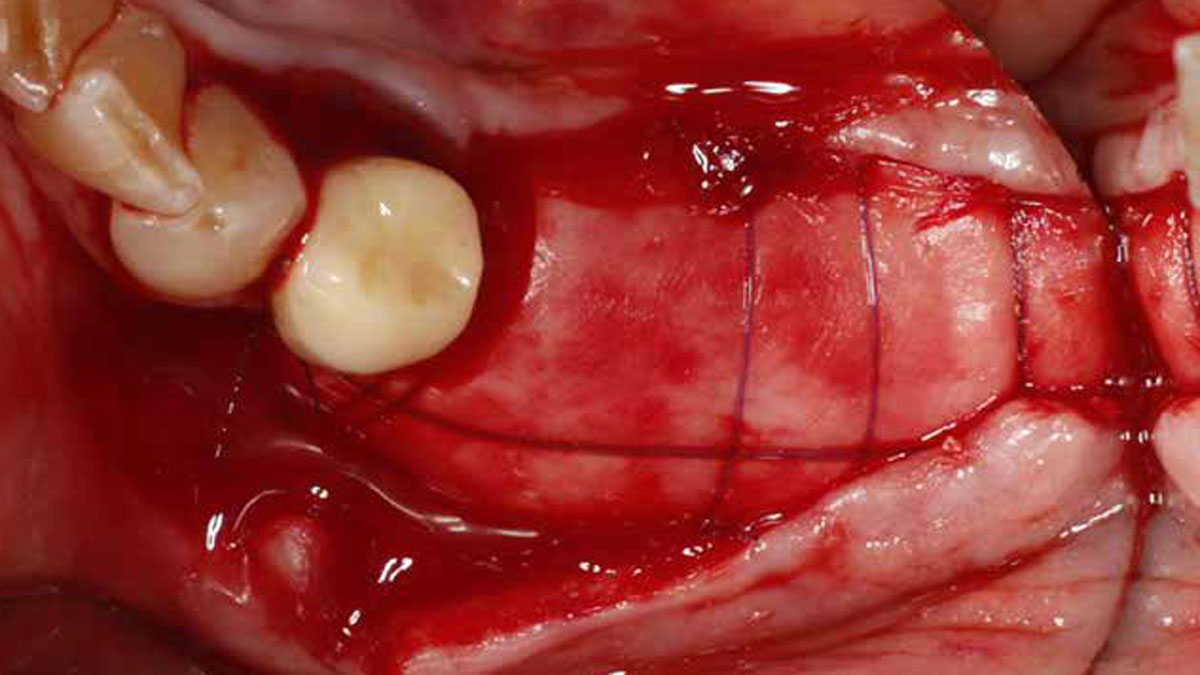
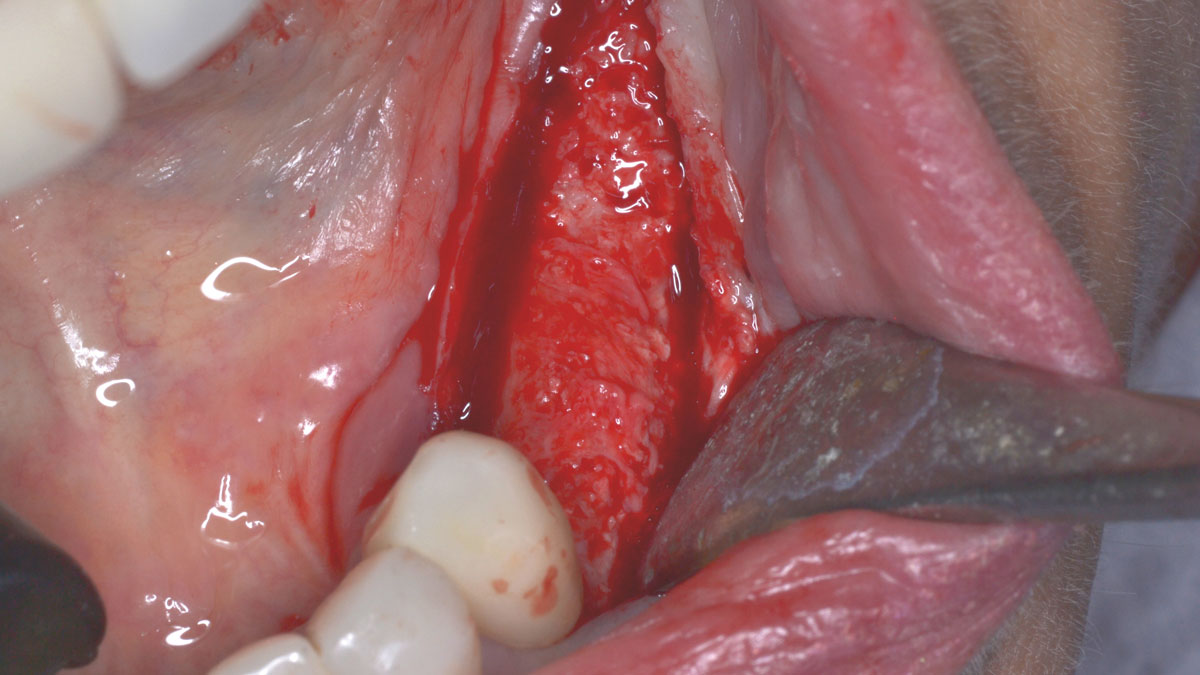
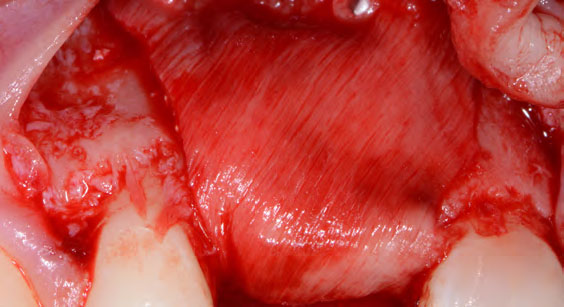
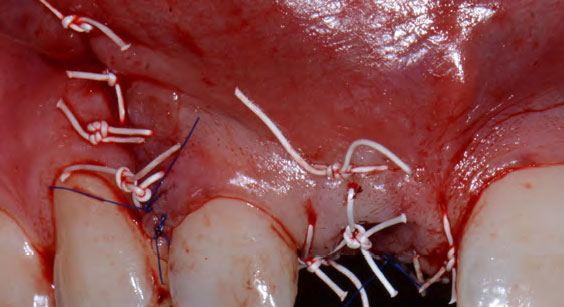
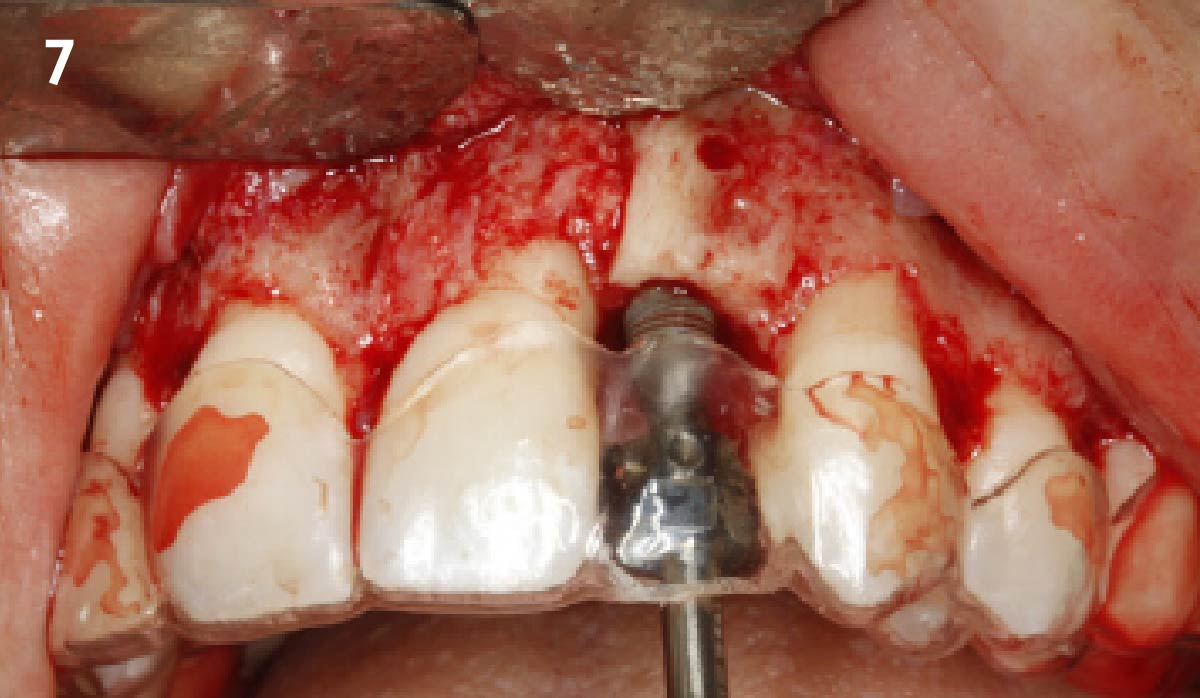
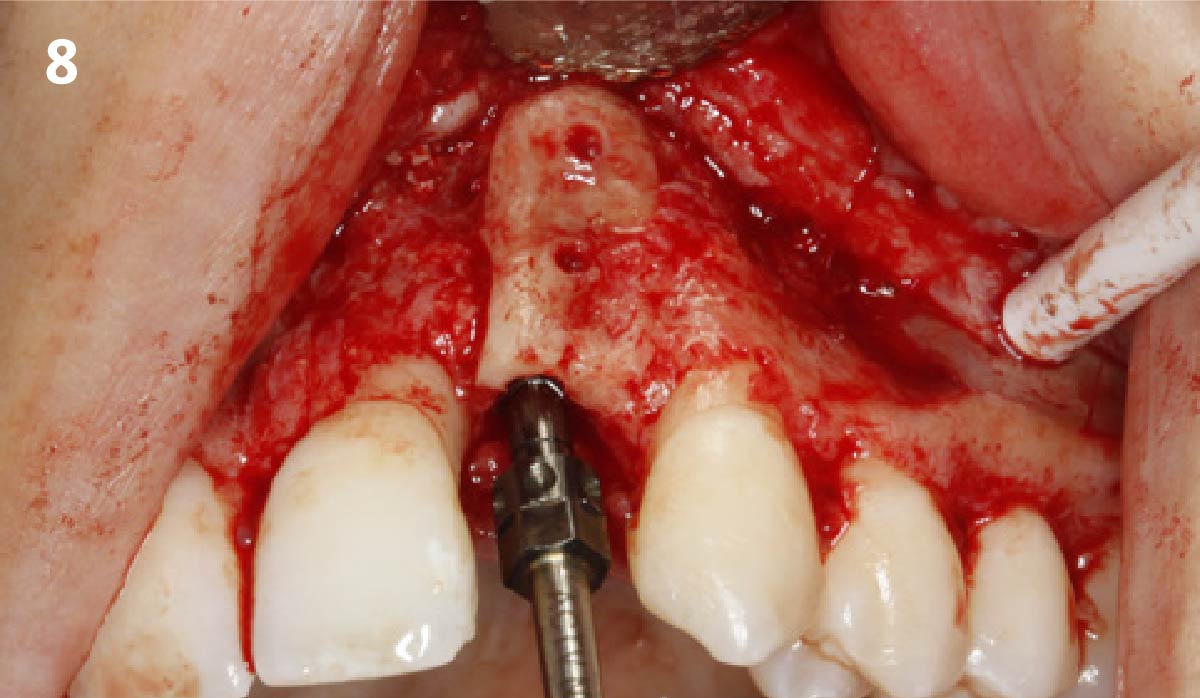
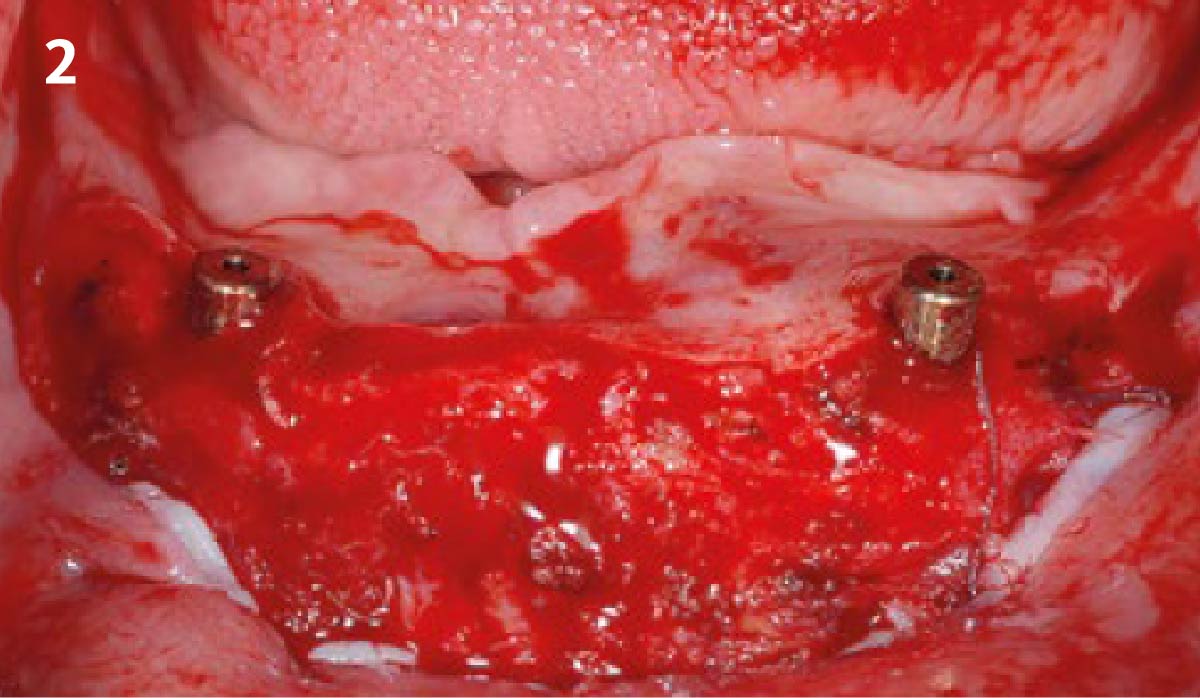
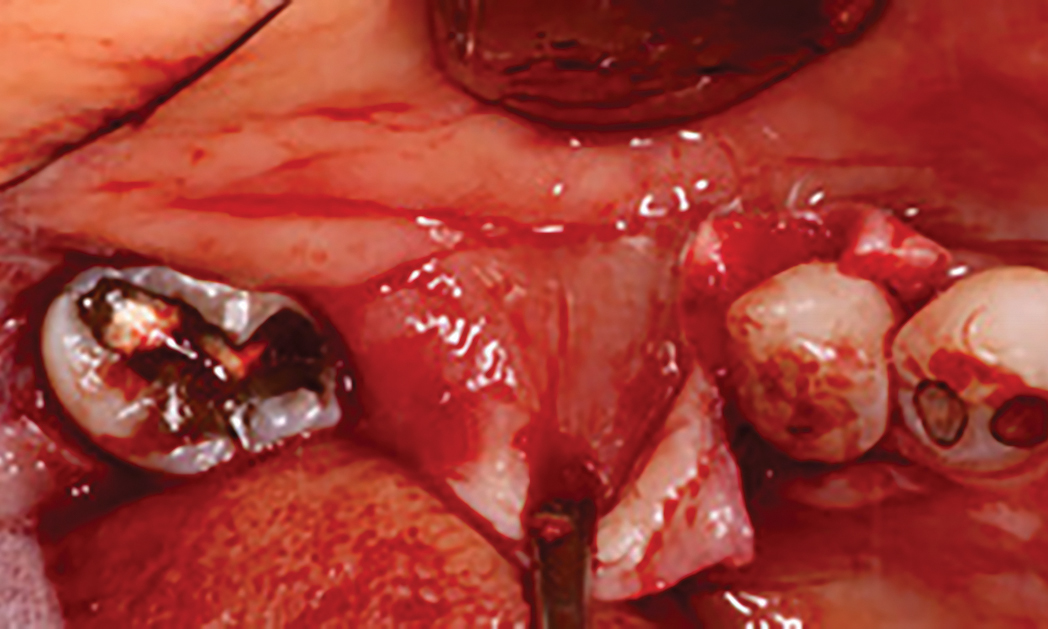
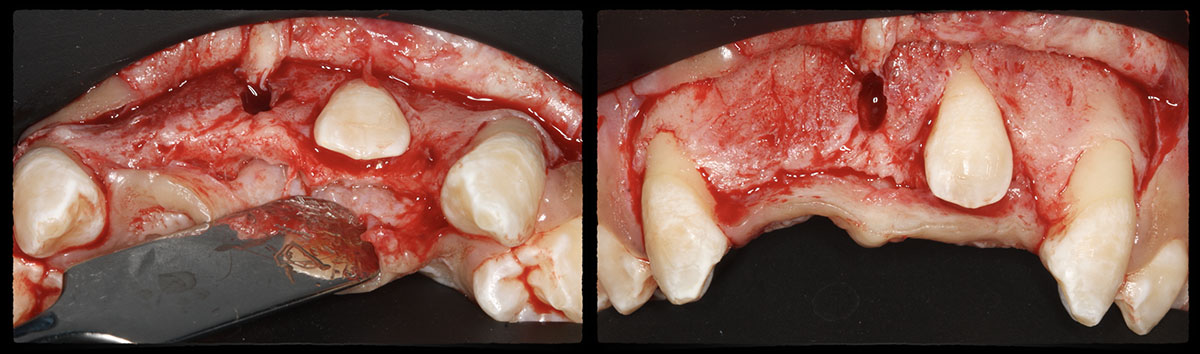
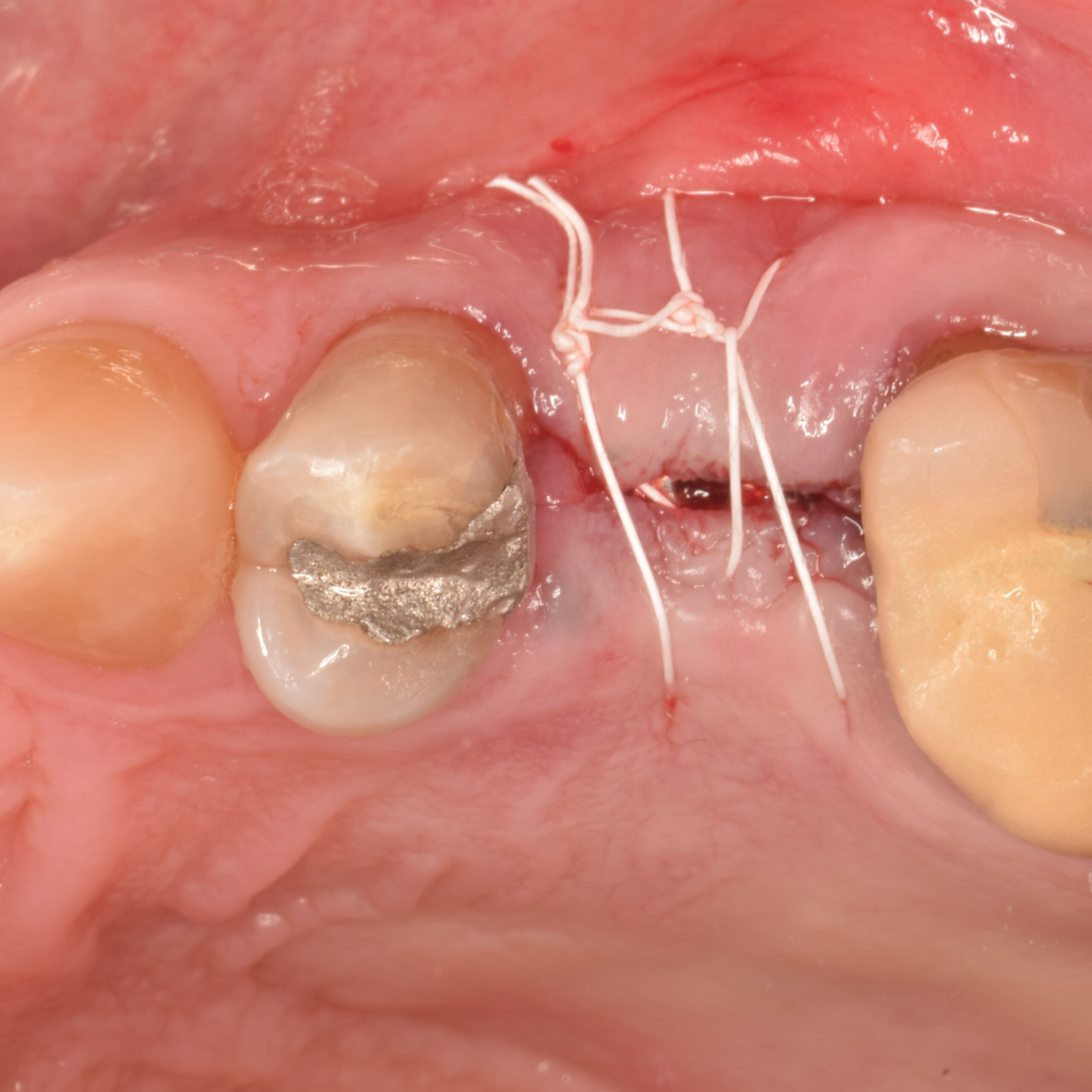
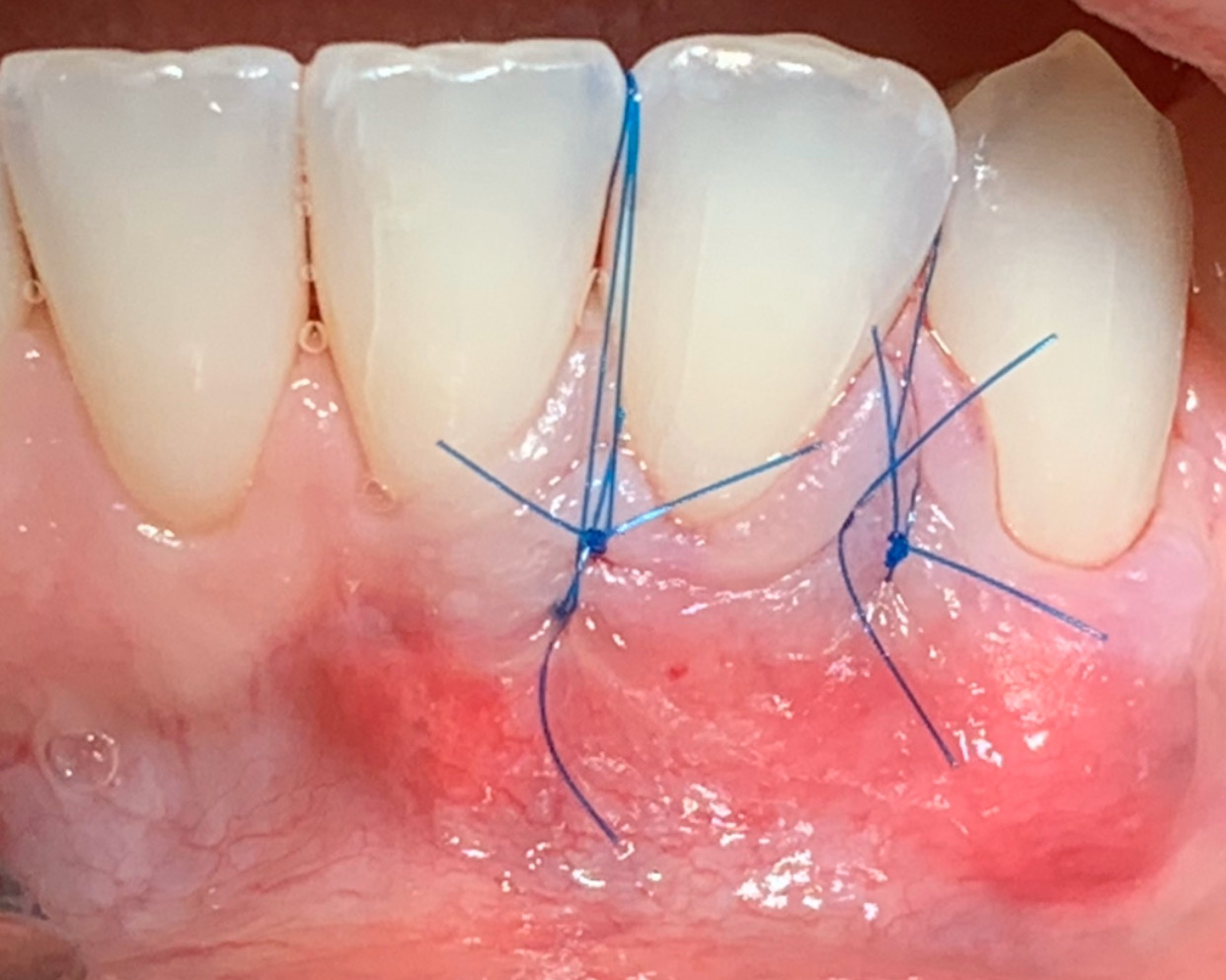
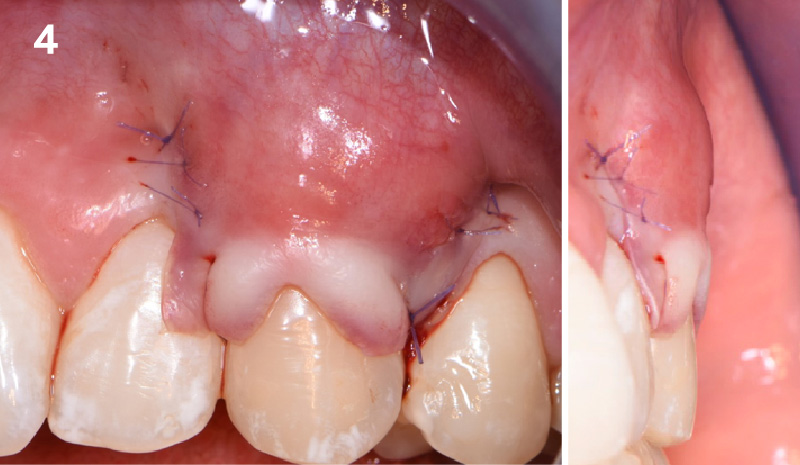
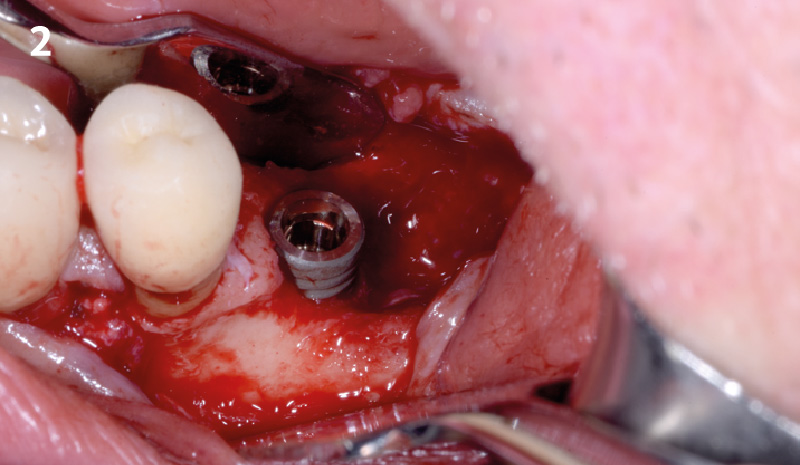
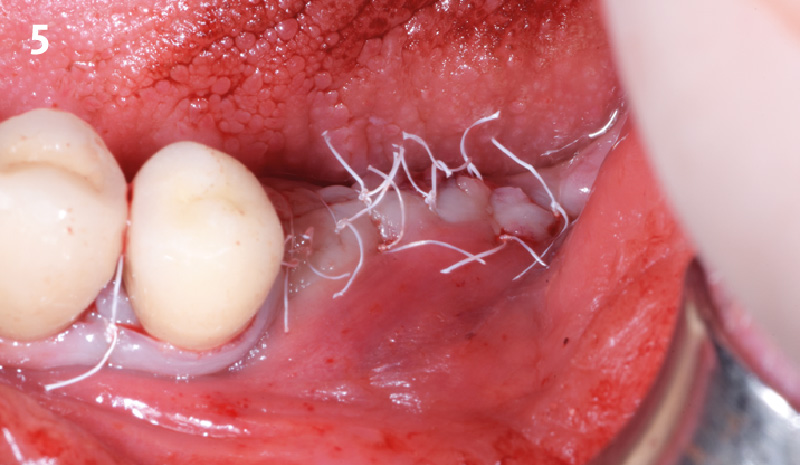
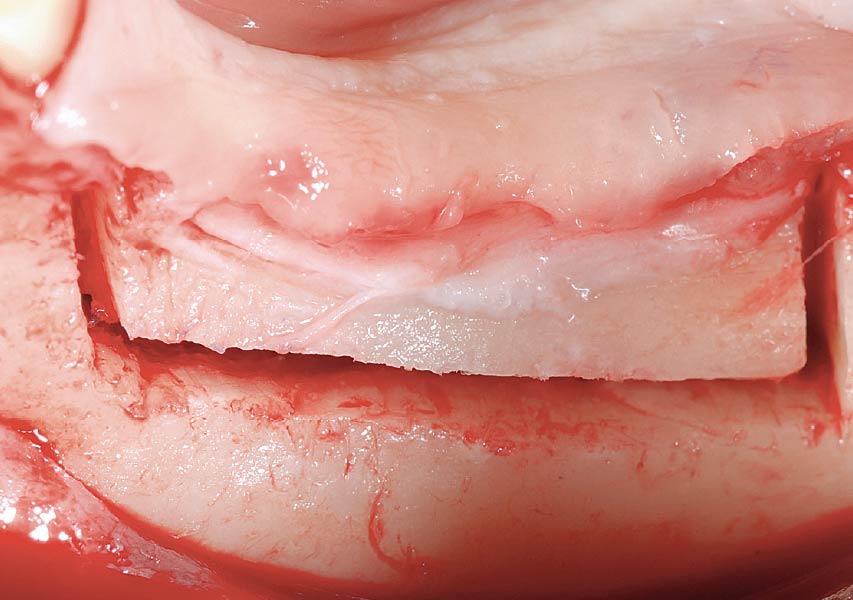
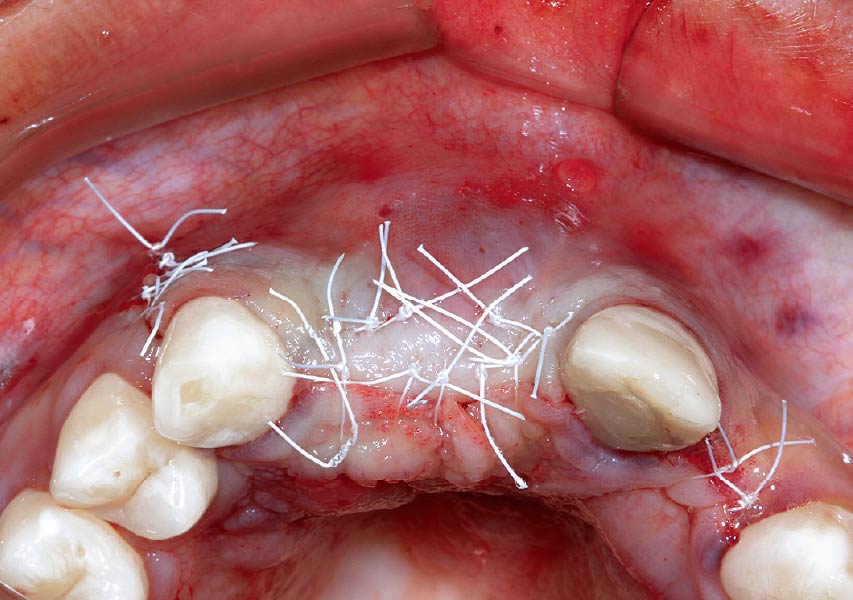
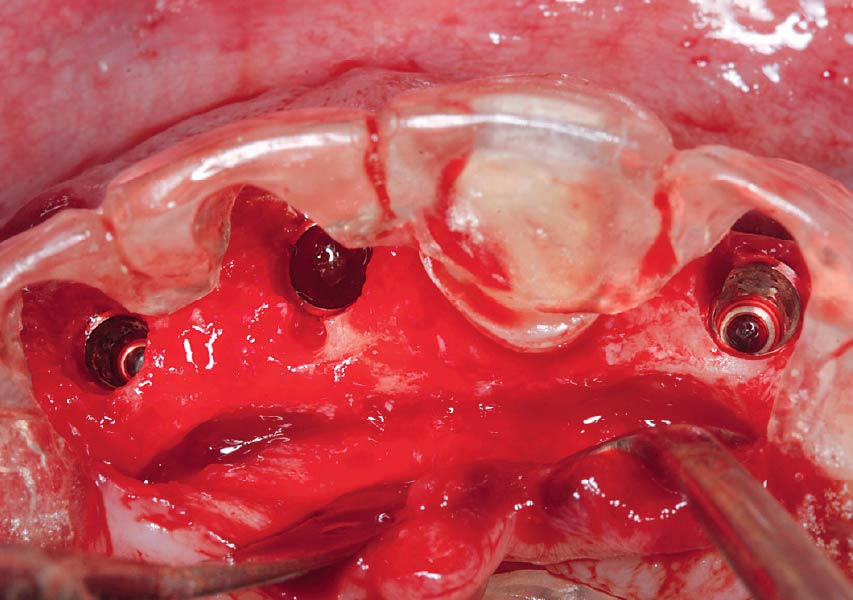
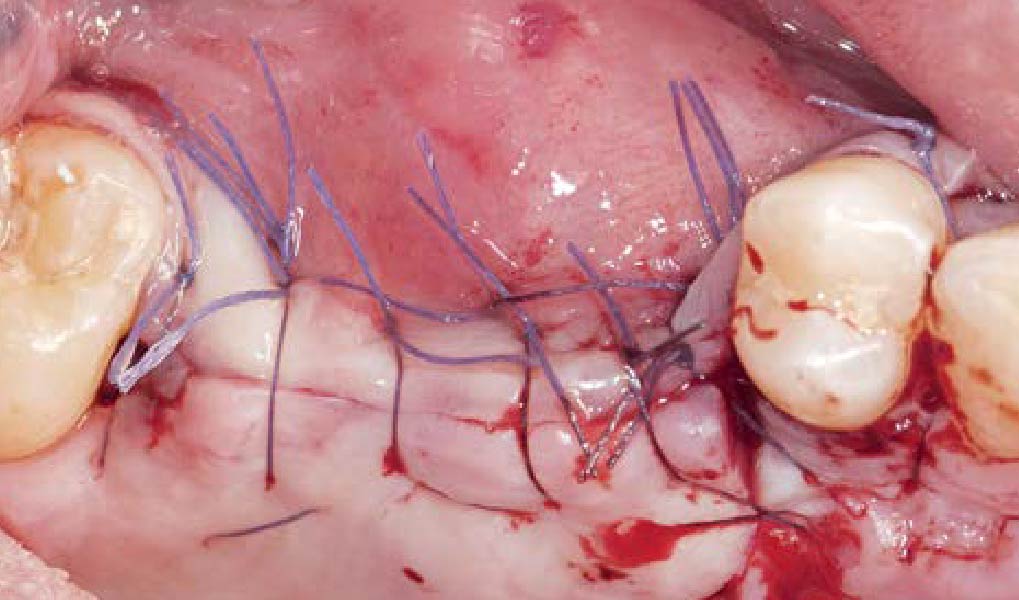
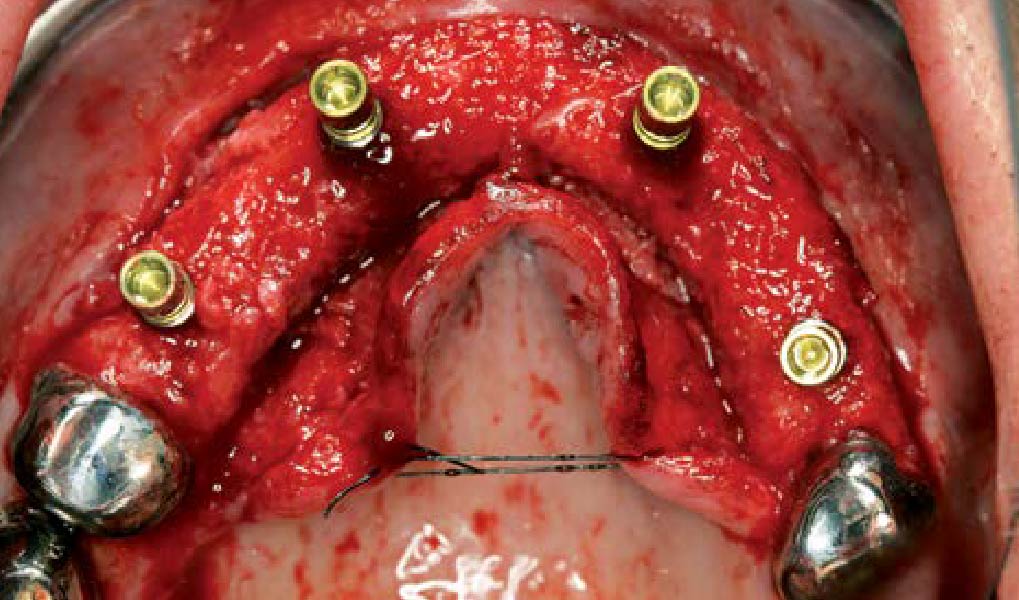
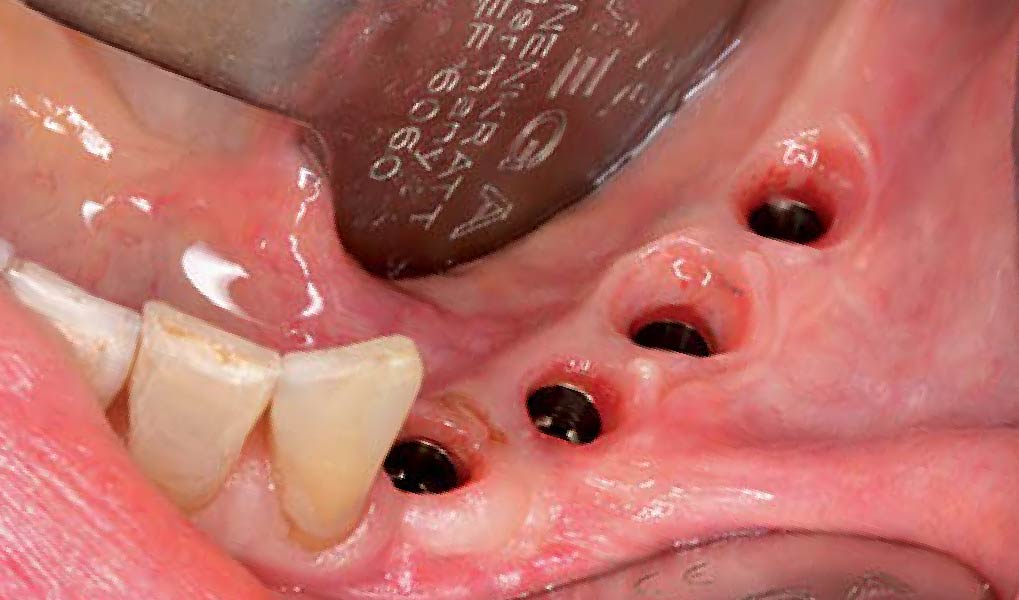
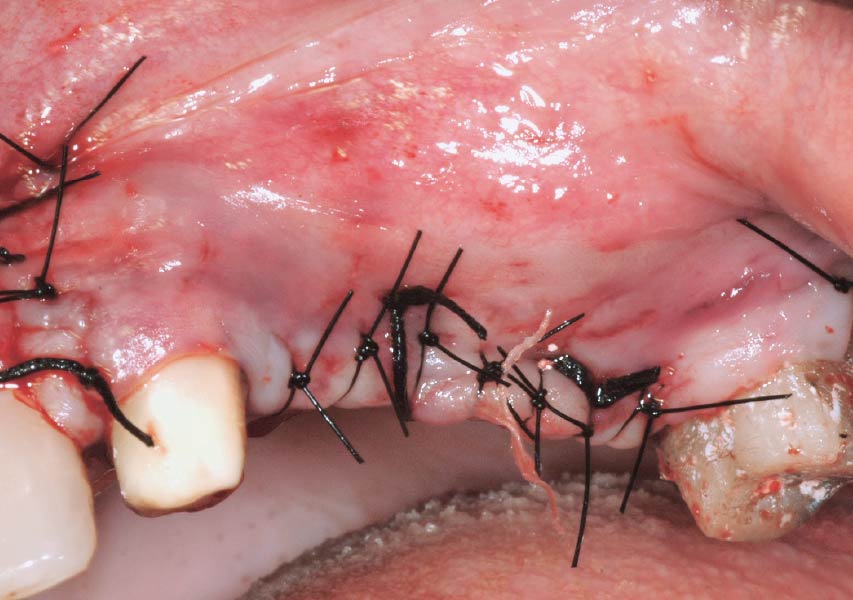
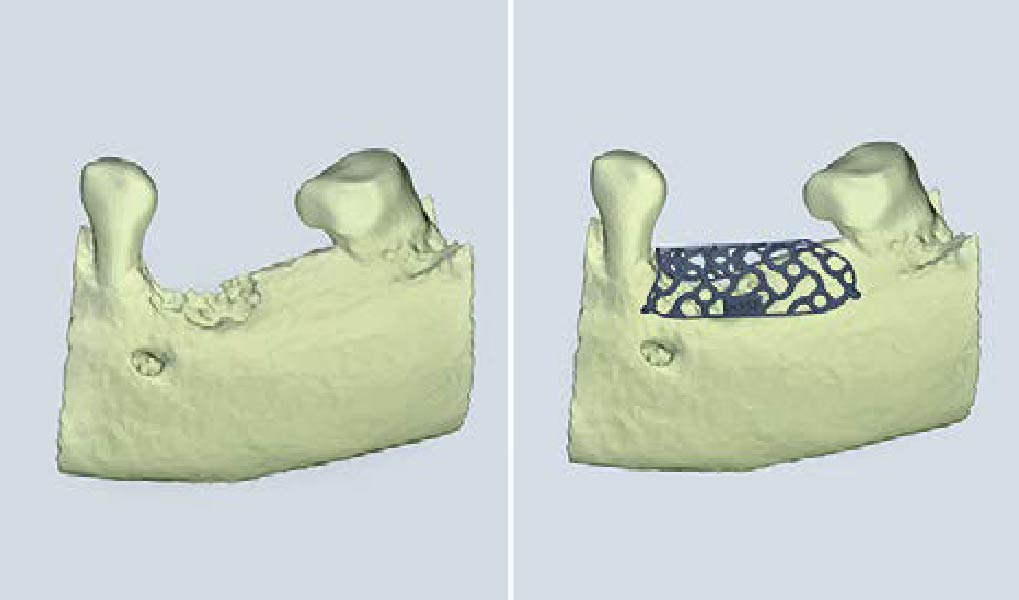
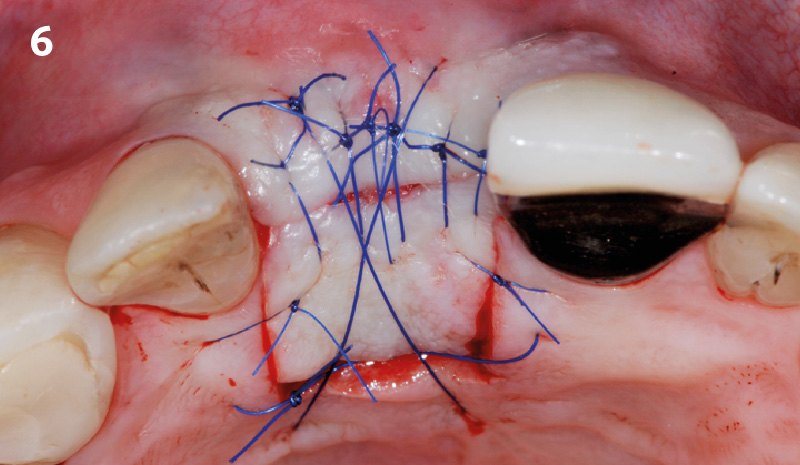
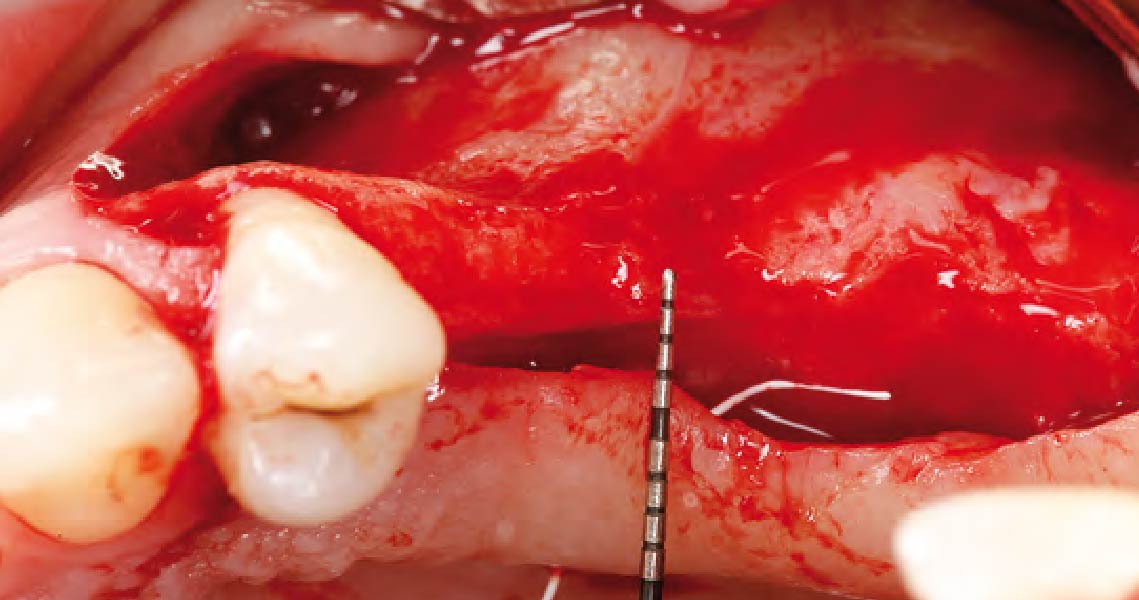
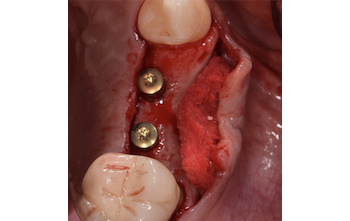
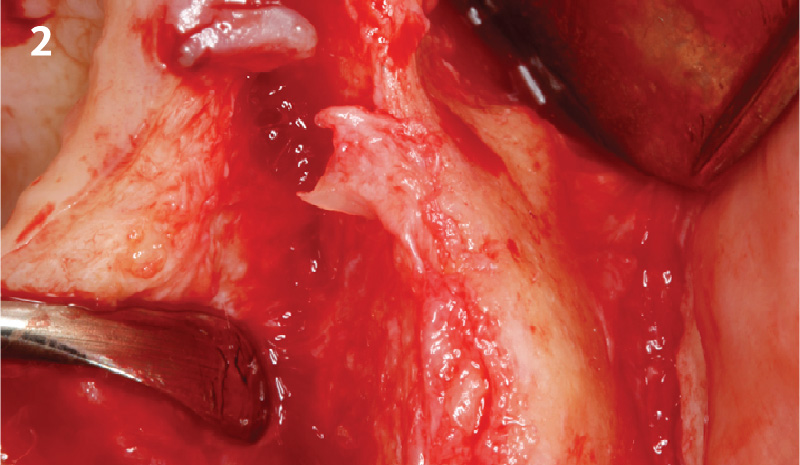
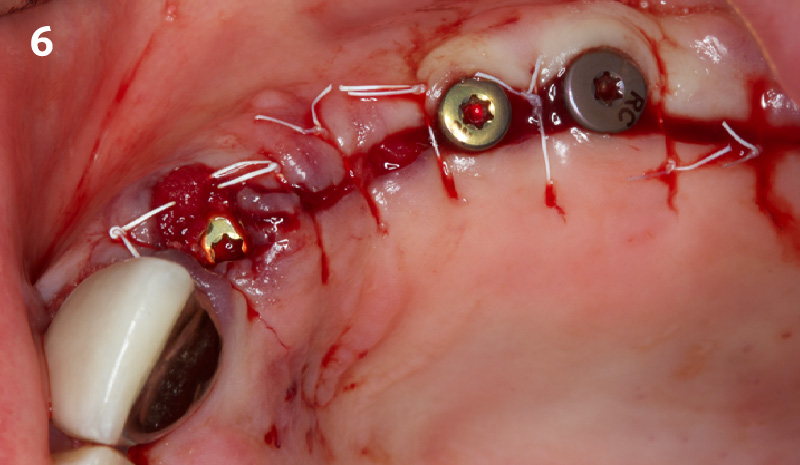
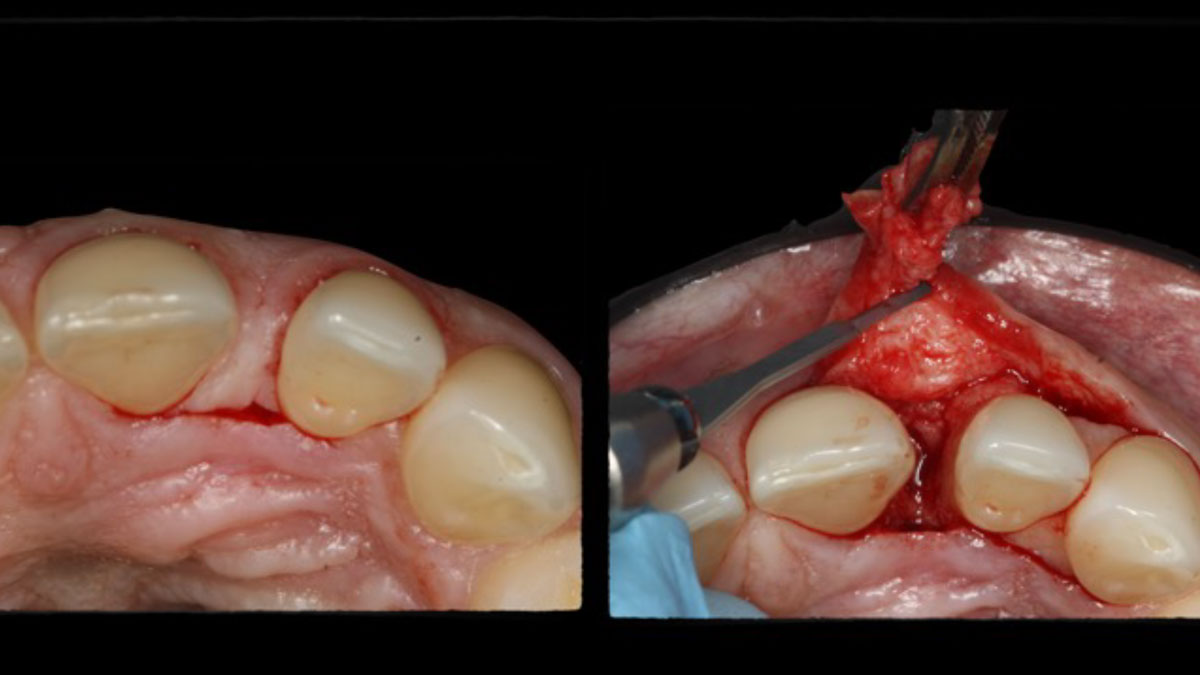
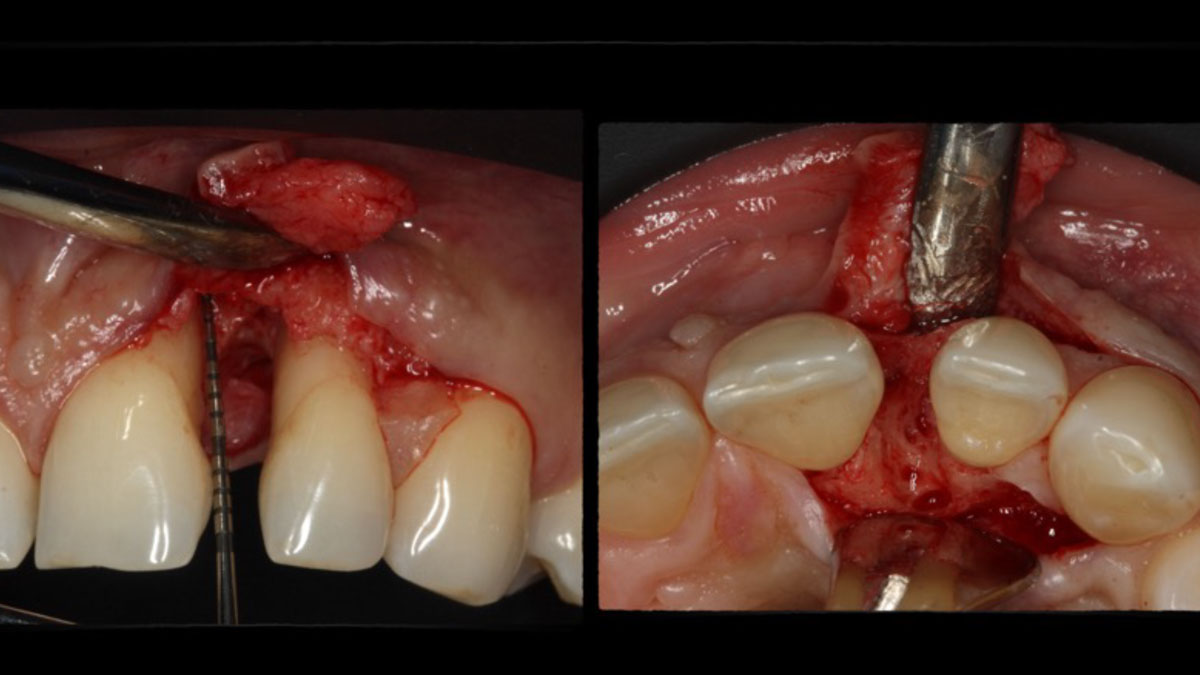
Correct the vertical bone loss around #9-10 and save the dentition. Sulcular incisions with a paracrestal incision around #9-10 were performed. The area was debrided showing a wide 1-2 bony wall defect (measuring ~7mm vertical bone loss). Primary closure was obtained using 6-0 prolene sutures.




“Guided tissue regeneration is indicated to correct the vertical bone loss around the #9-10 area and stabilize the periodontium.”
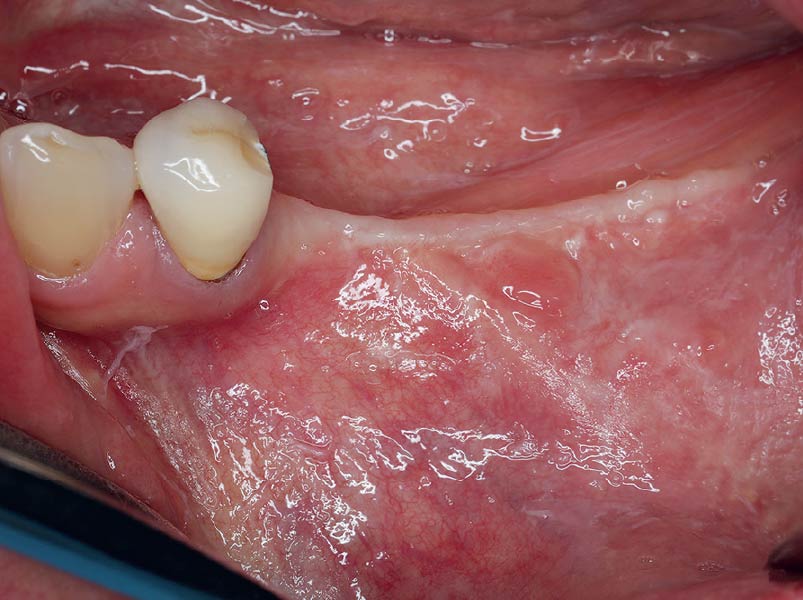
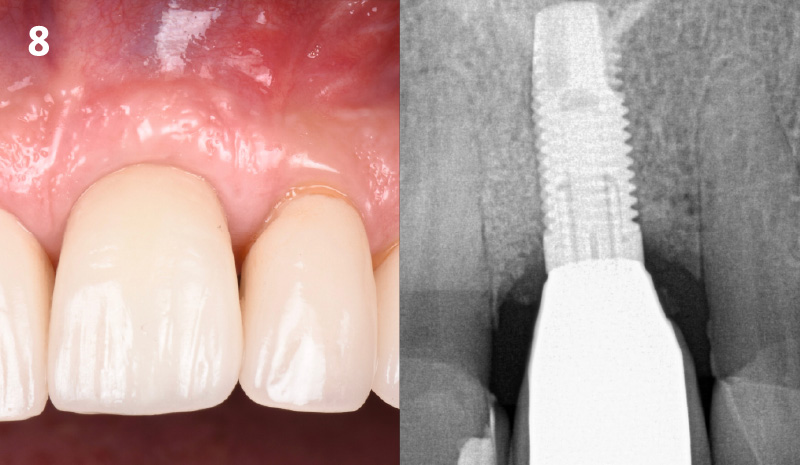
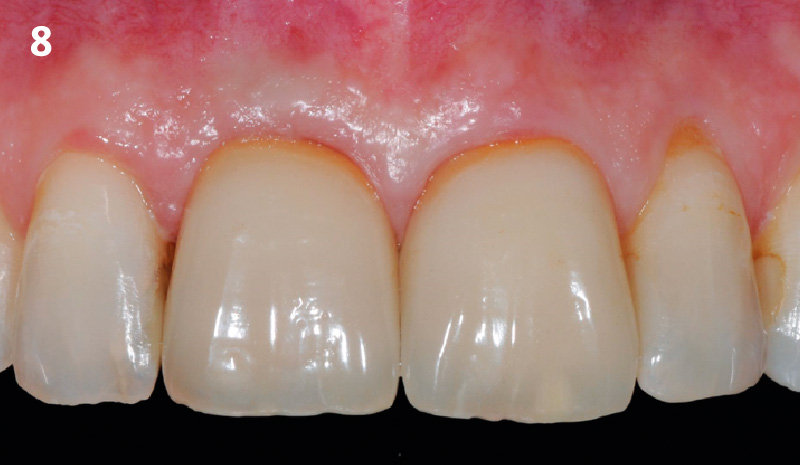
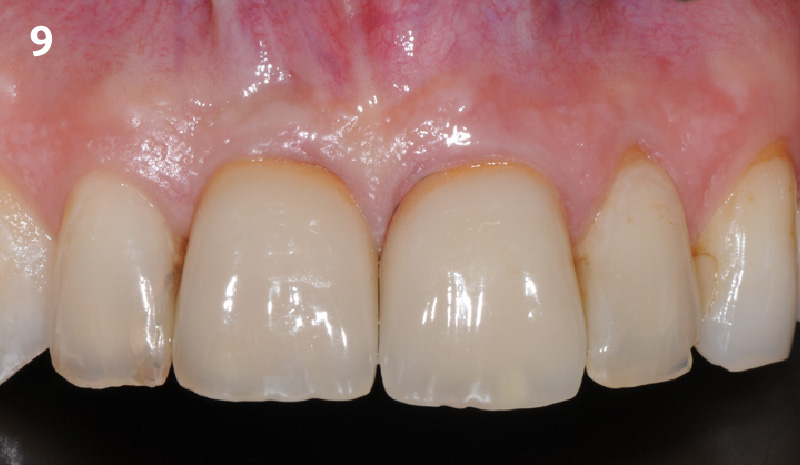
THE OUTCOME
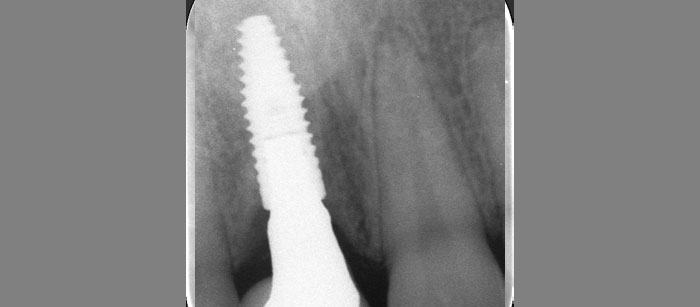
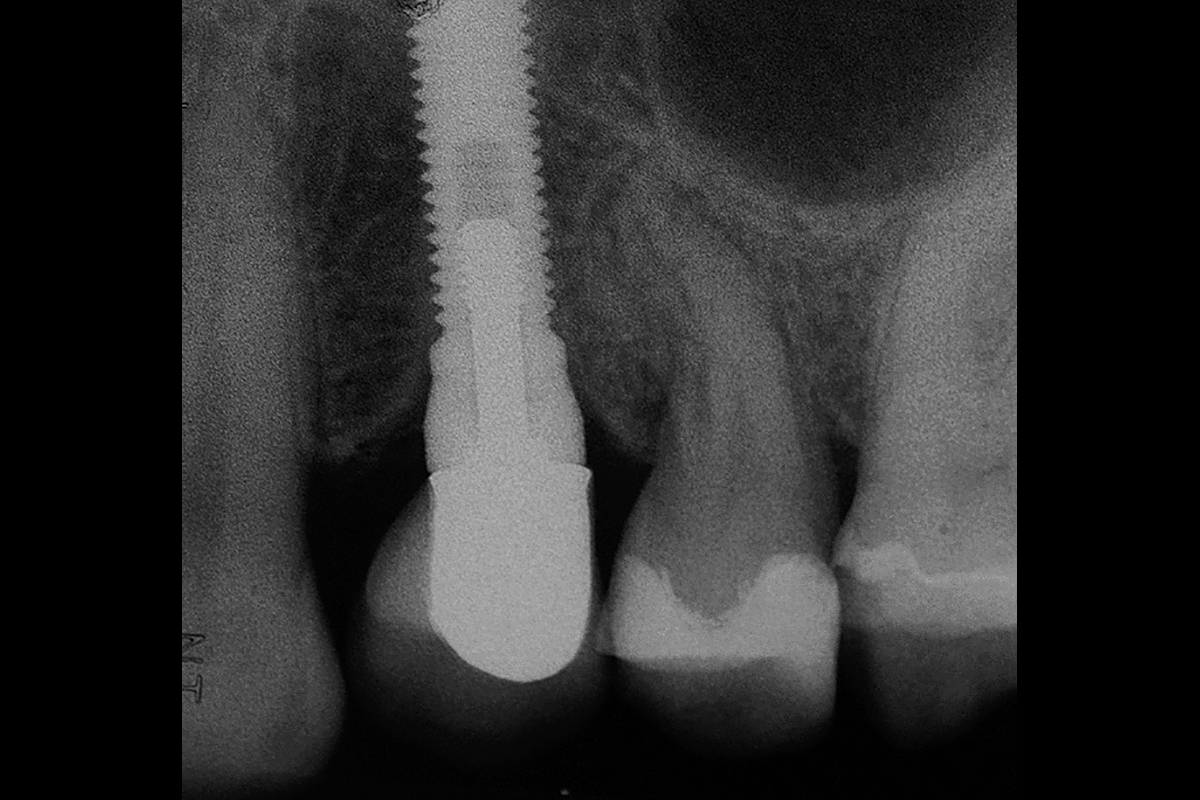
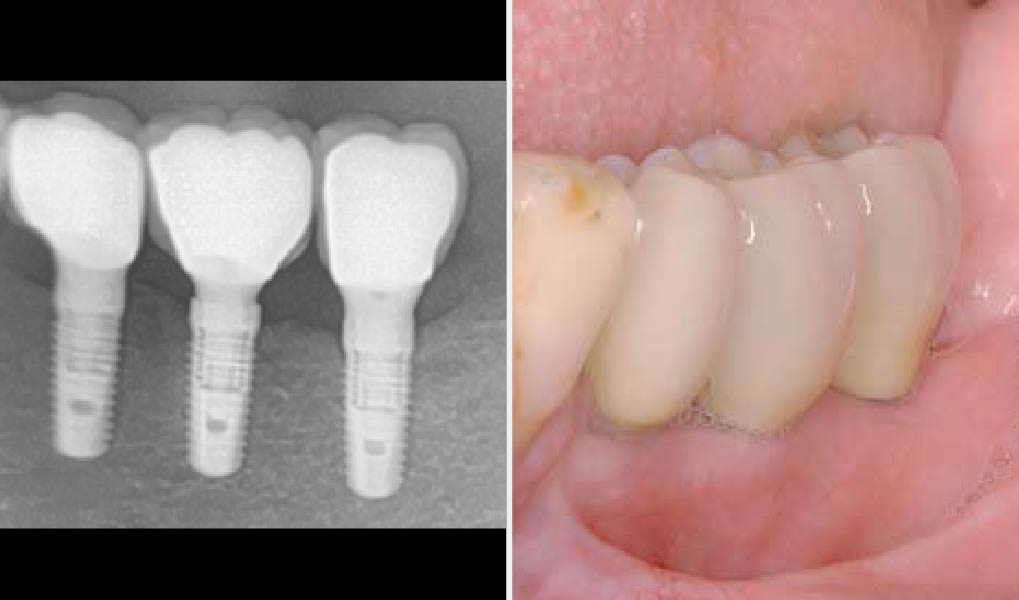
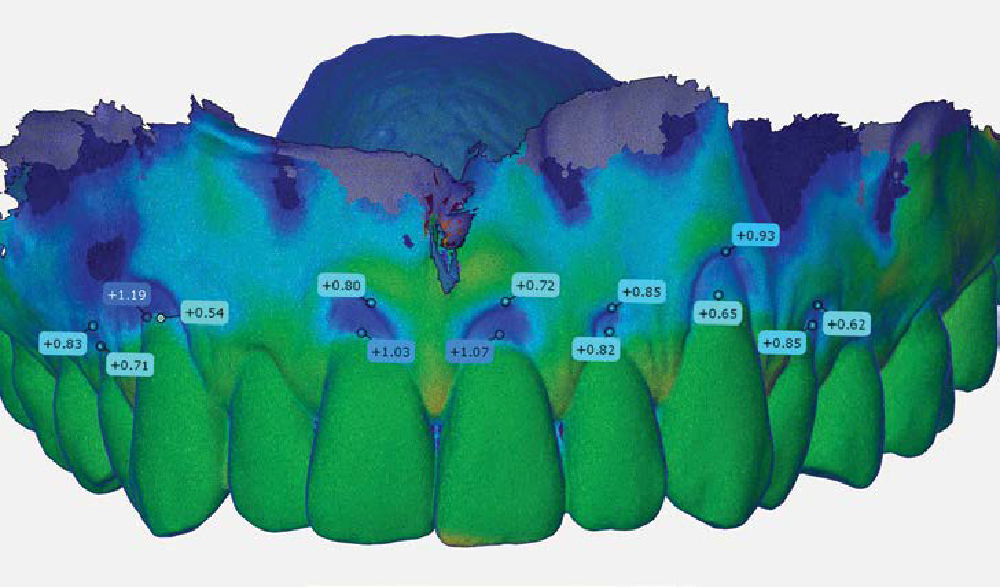
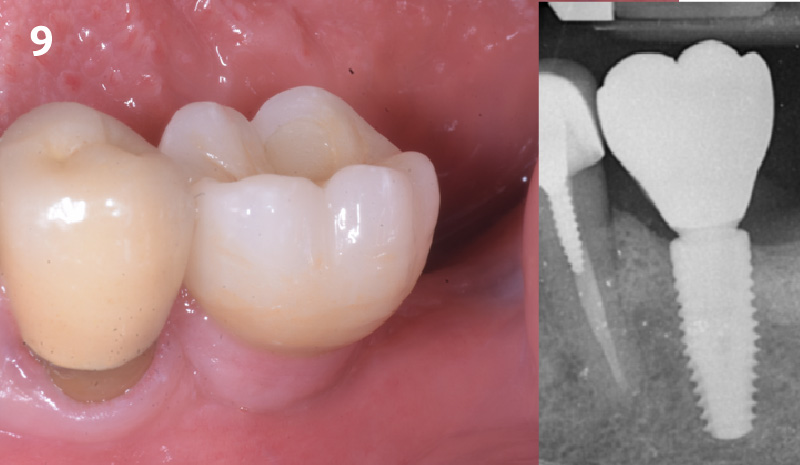
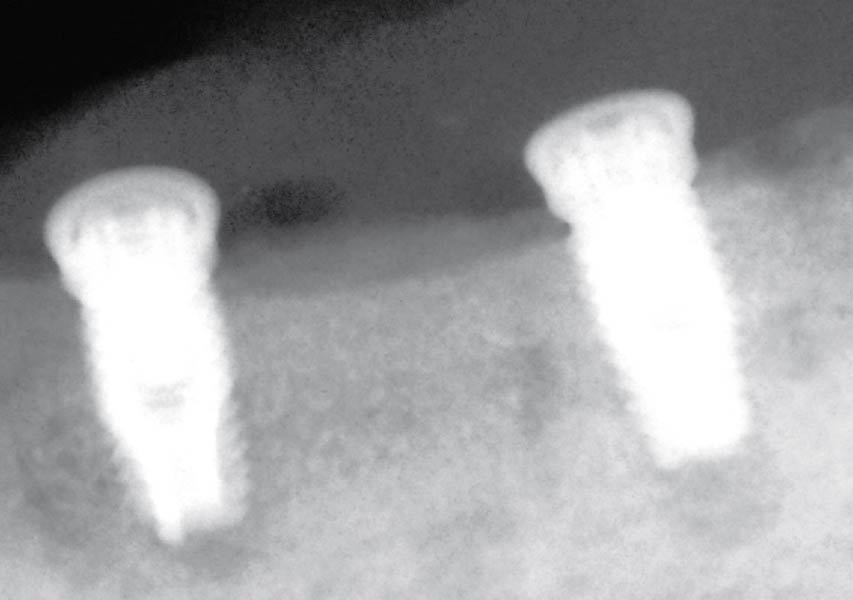
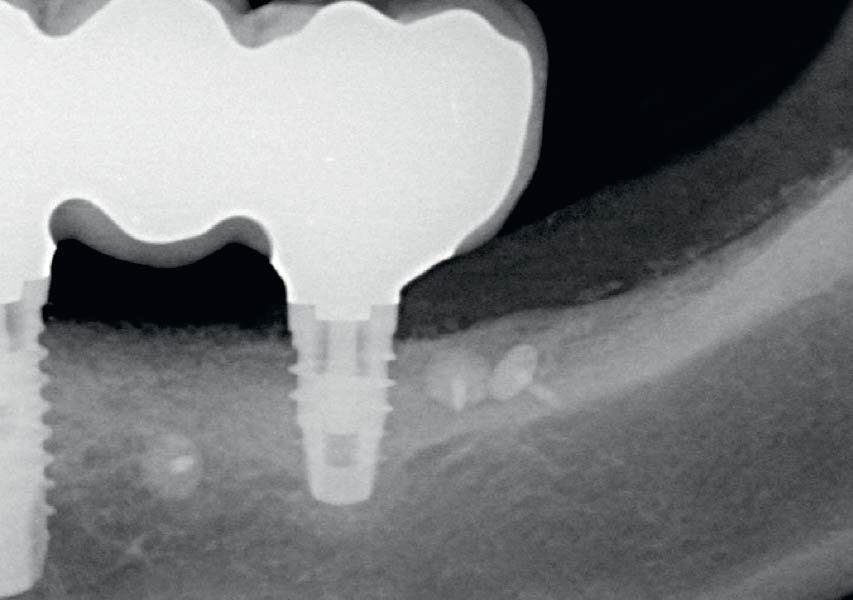
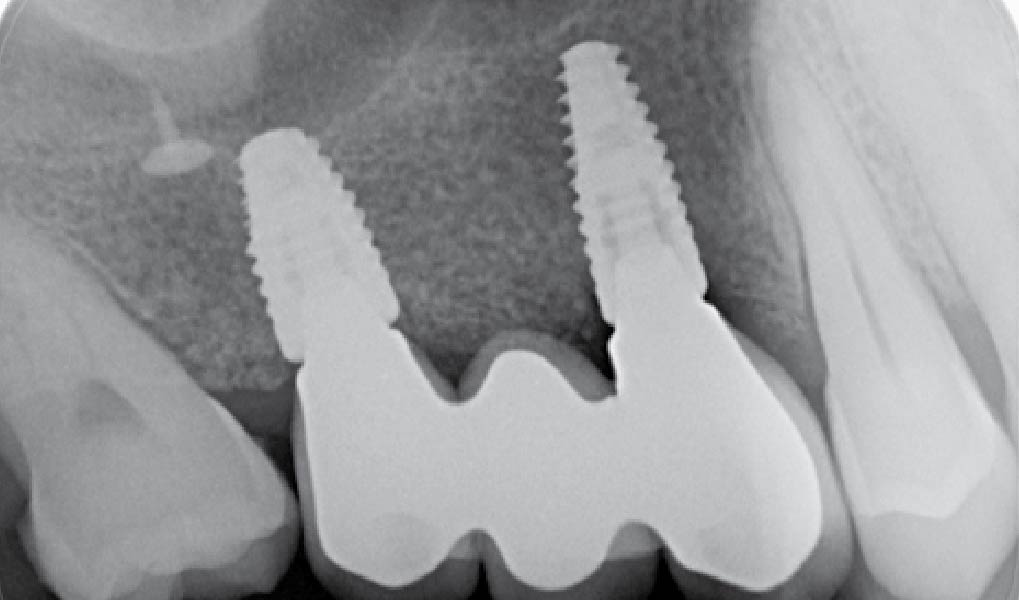
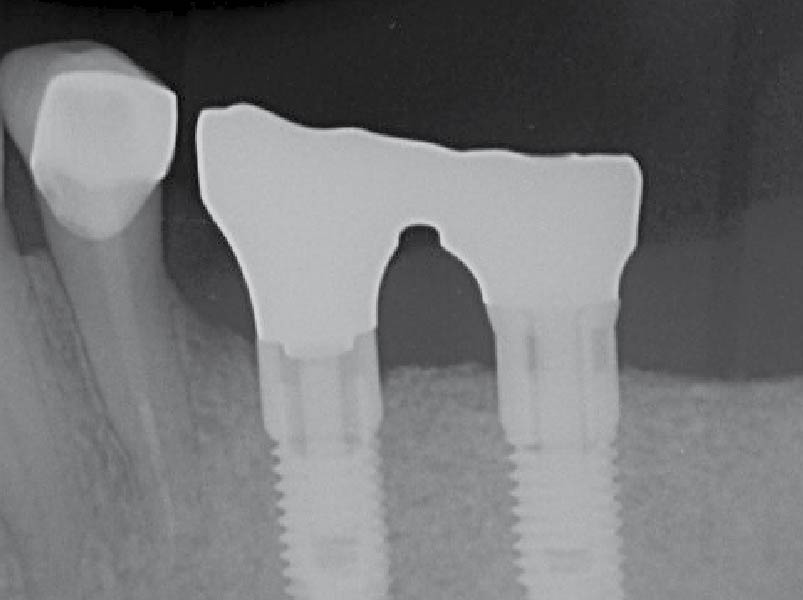
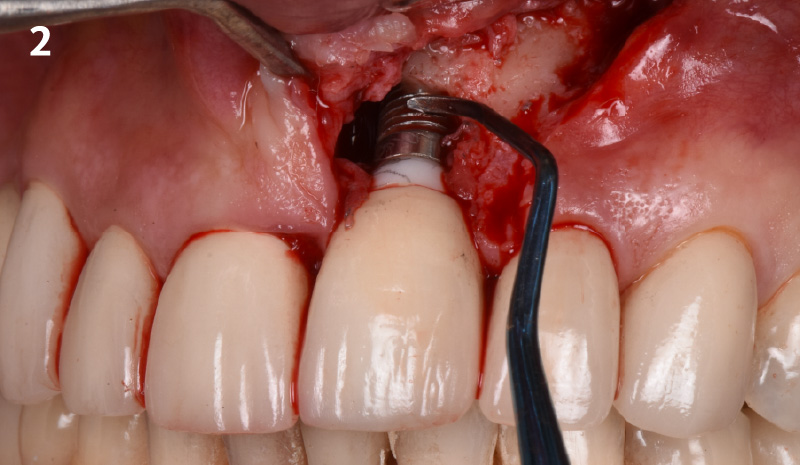
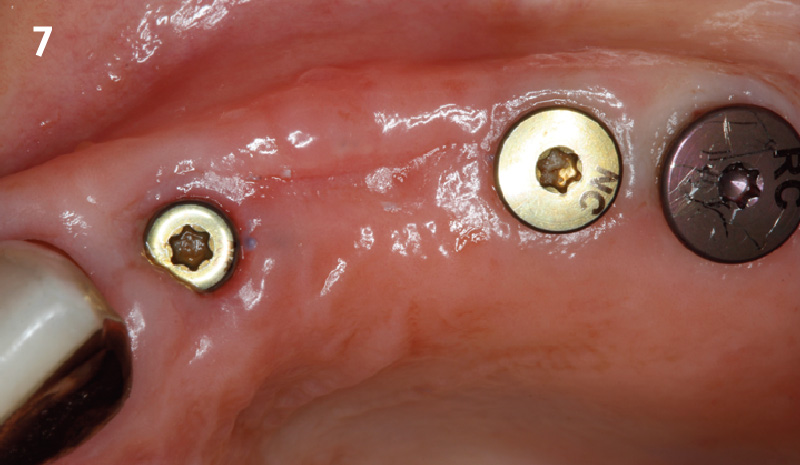
The use of a minimally invasive surgical GTR approach showed excellent radiographic bone fill and reduction in probing depths from 8mm to 3mm at 6 months follow-up. Treatment outcome revealed stable periodontium and the patient was happy with the healthy stable teeth.

Bassam Kinaia, DDS, MS, DICOI
Dr. Kinaia is the Associate Director of the Graduate Periodontology Program at the University of Detroit Mercy (UDM). He is also the former Director of the Periodontology Program at UDM in Michigan and Boston University Institute for Dental Research and Education in Dubai. He is a Diplomate of the American Acade- my of Periodontology (AAP) and International Congress of Oral Implantology (ICOI). He received a certificate of Excellence from the AAP in recognition of teaching-research fellowship.