CLINICAL CASE

THE SITUATION
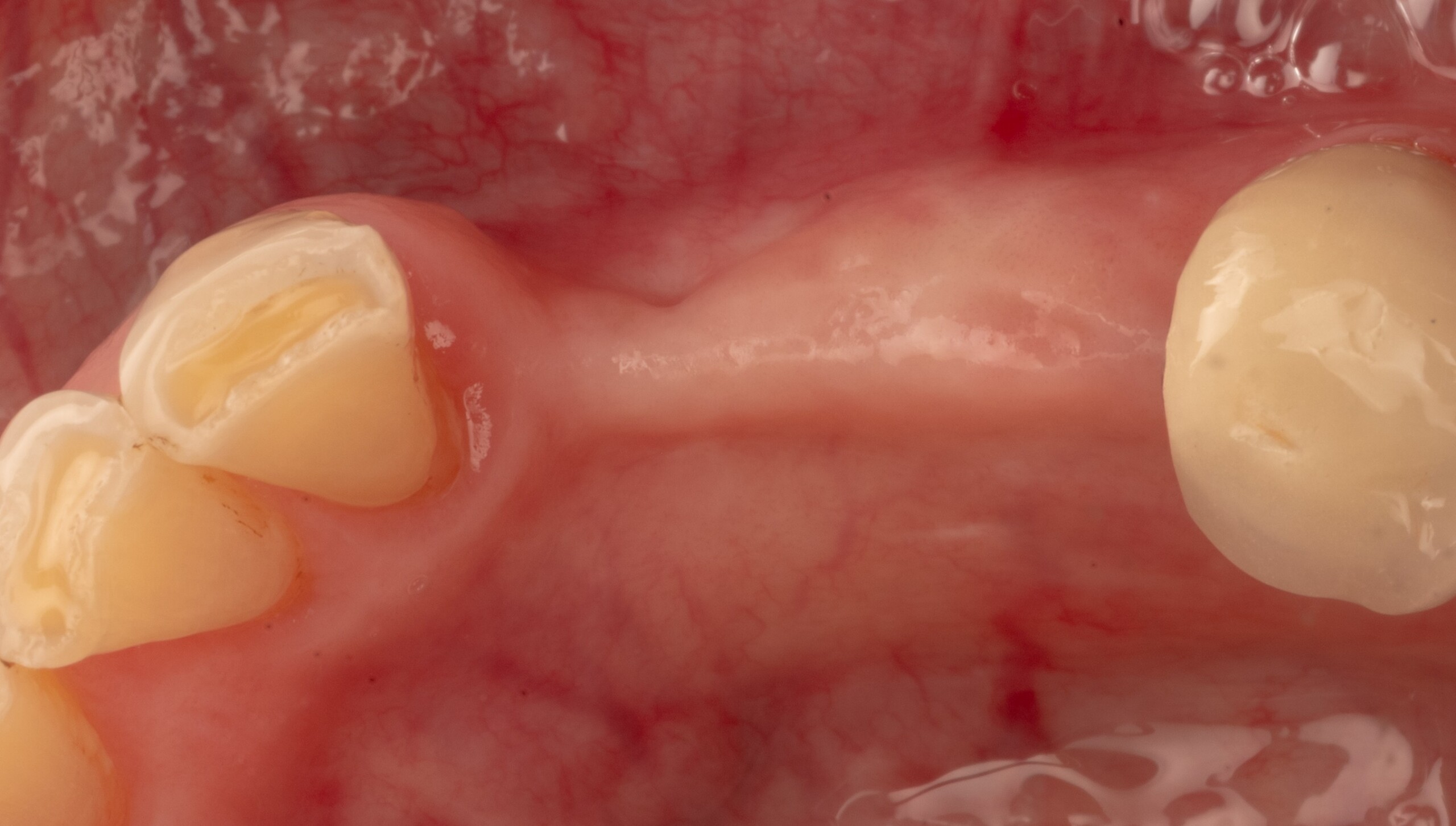
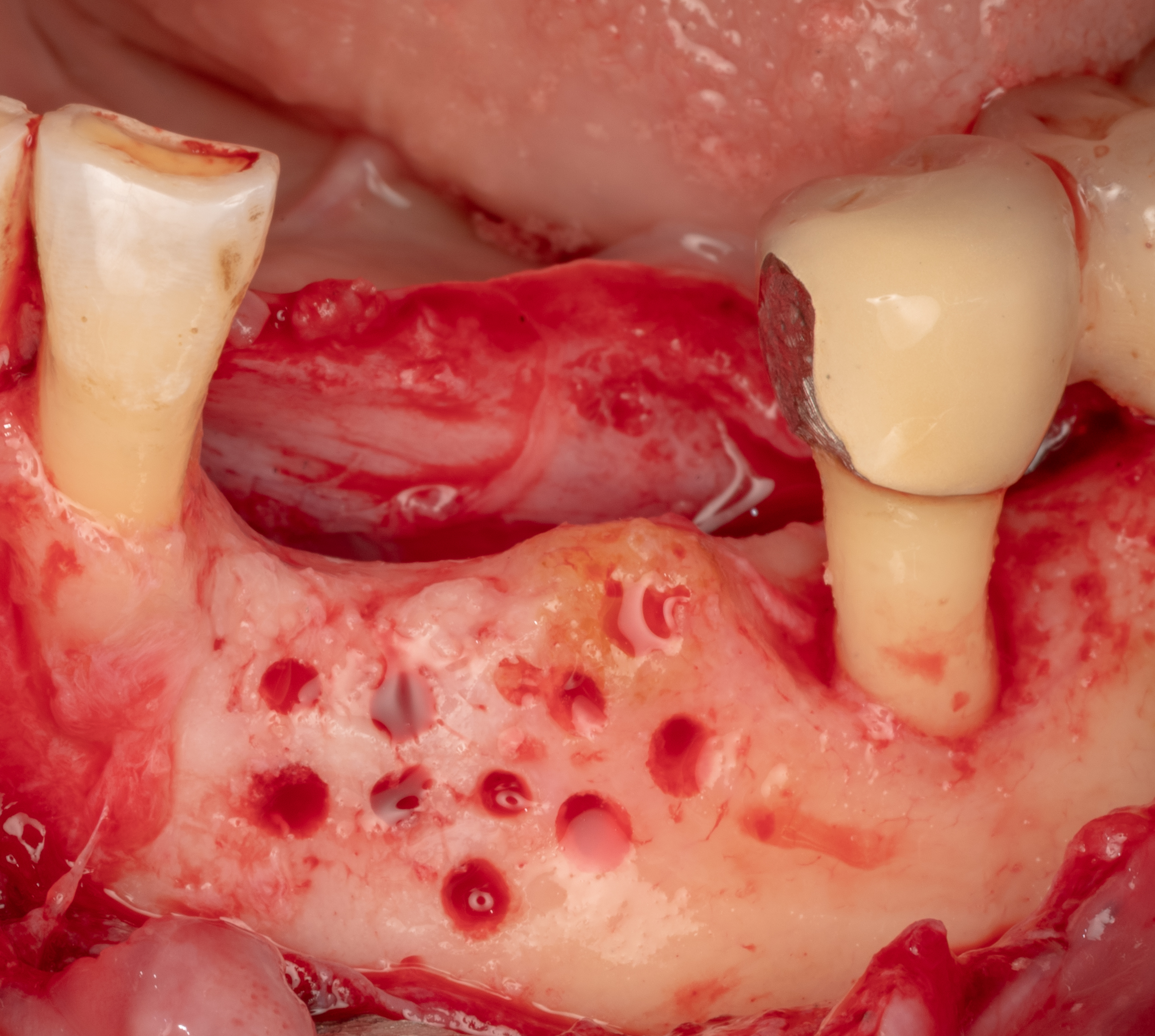
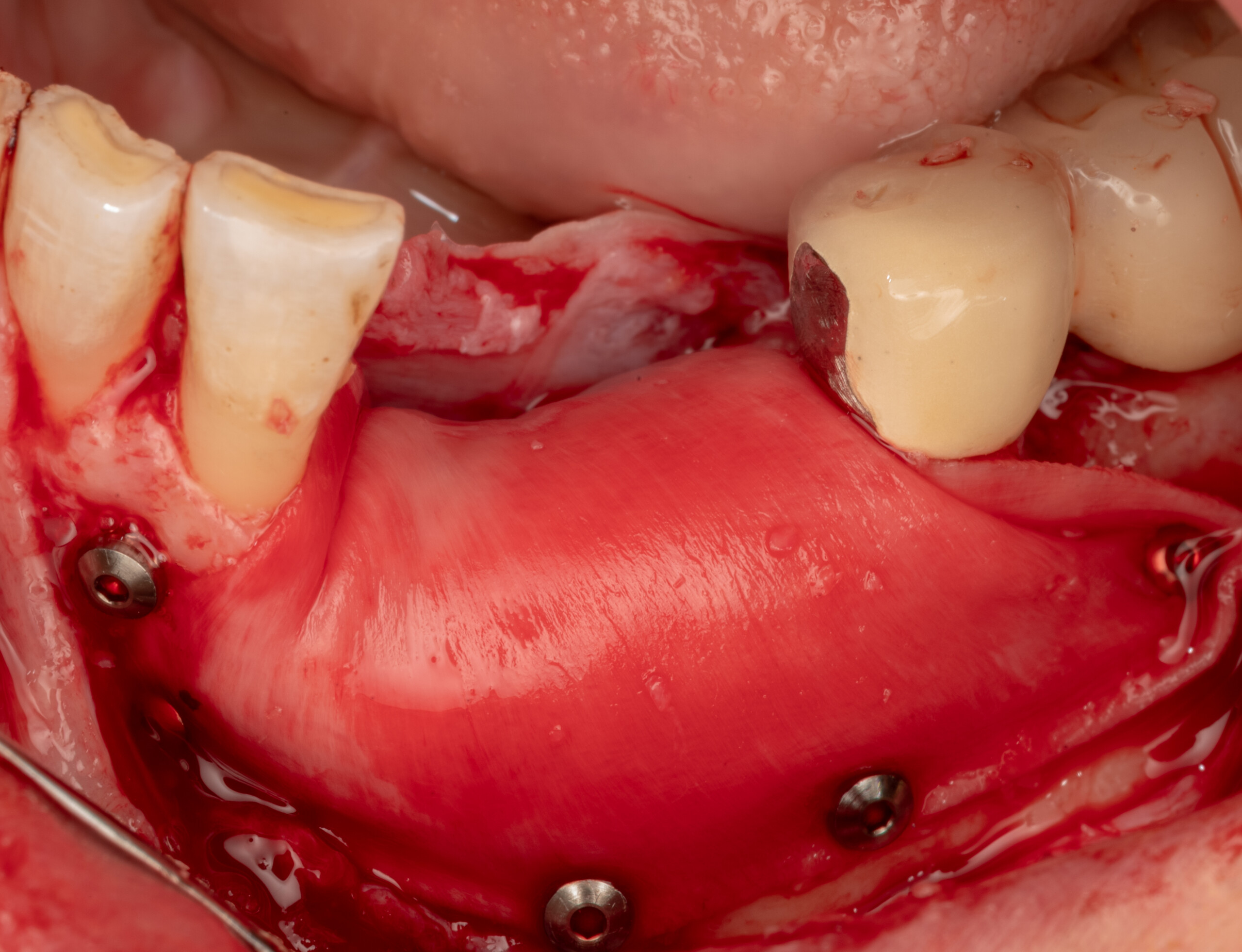
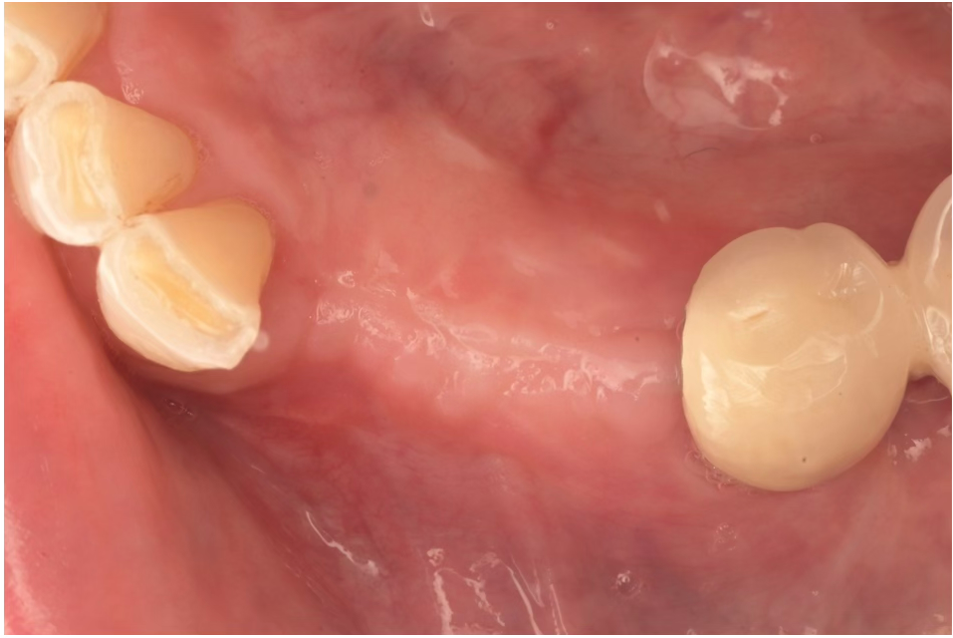
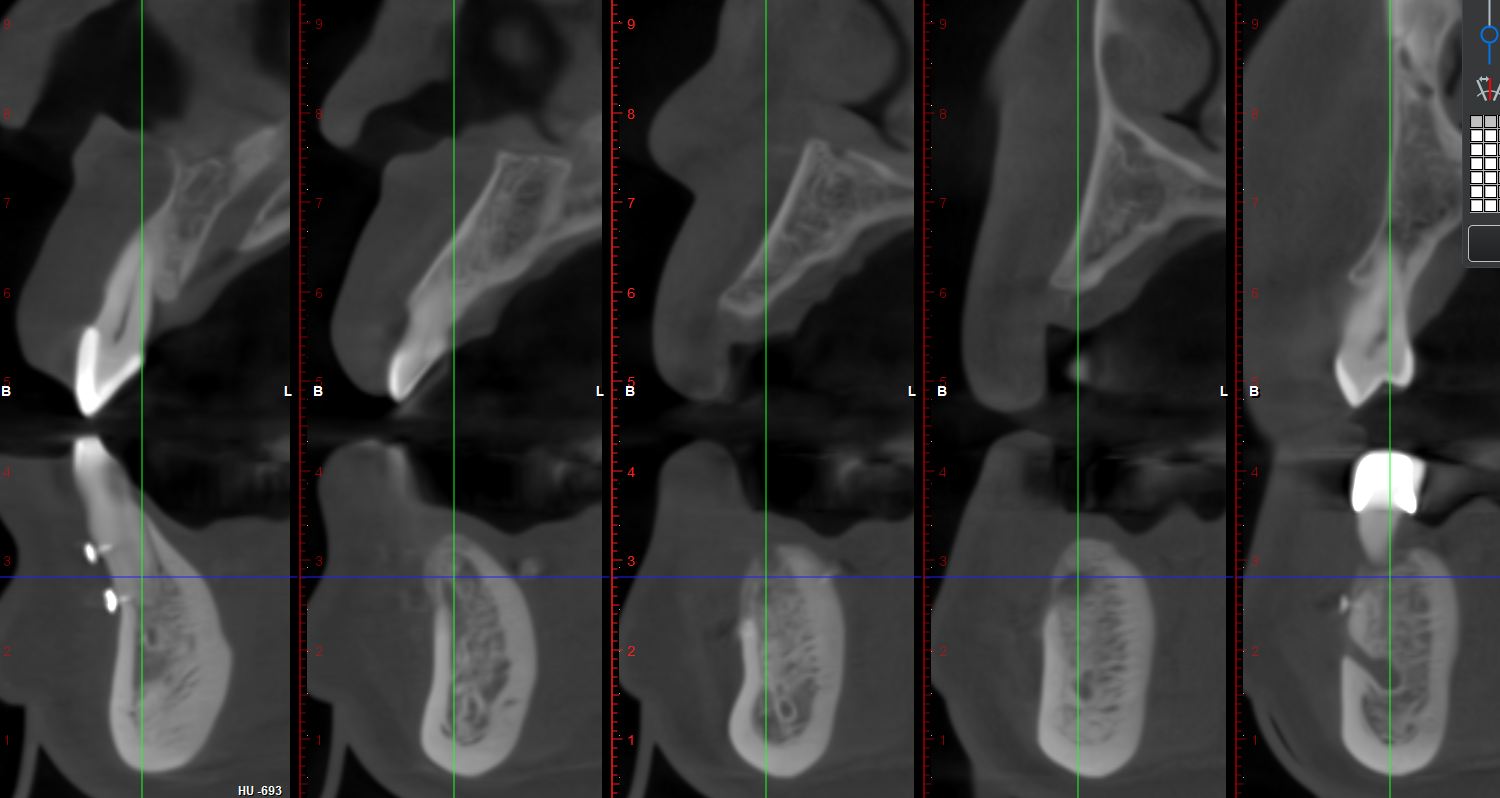
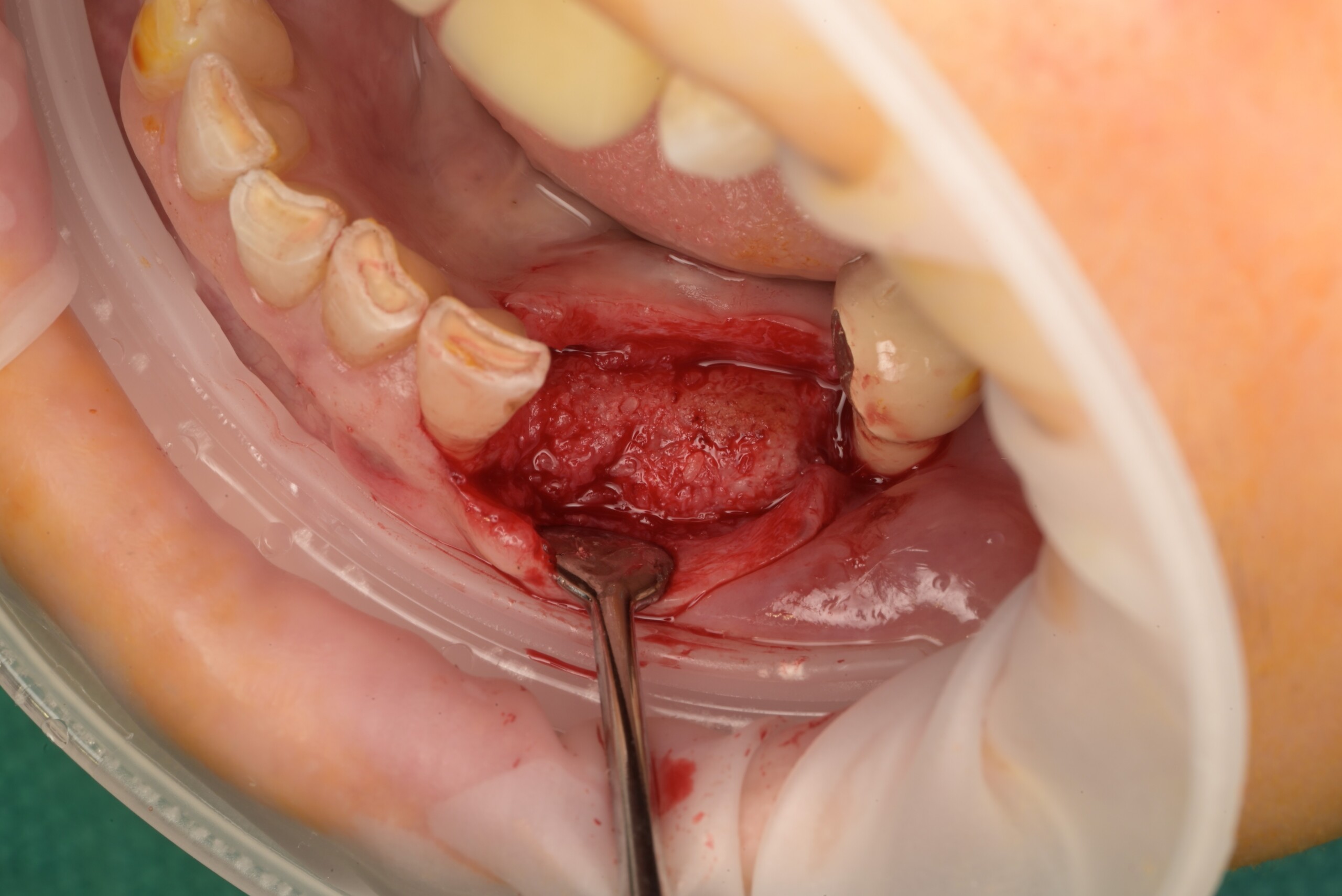
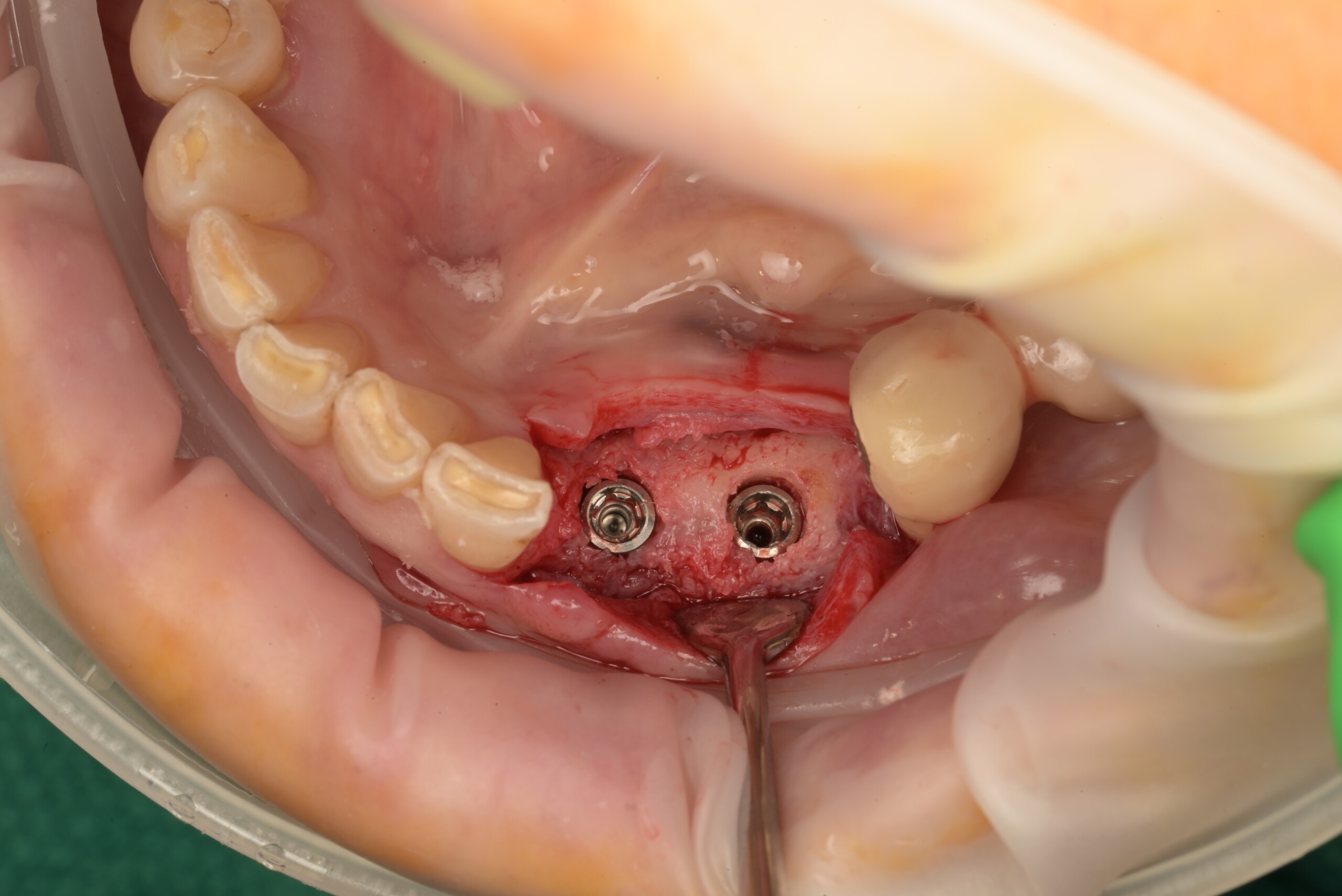
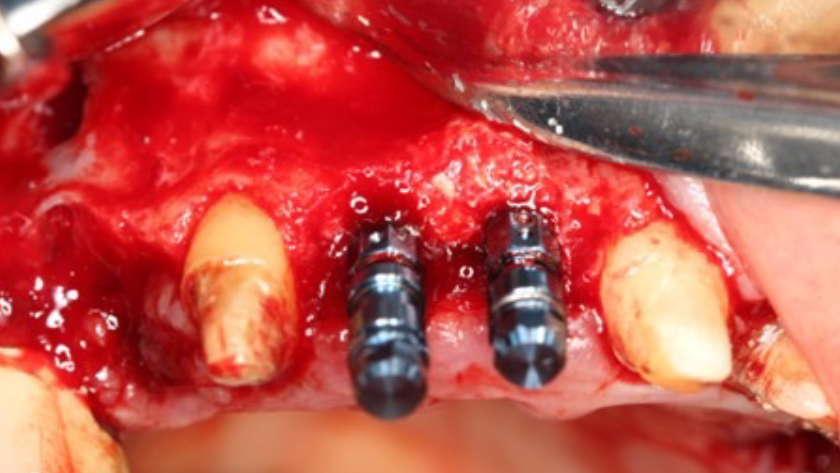
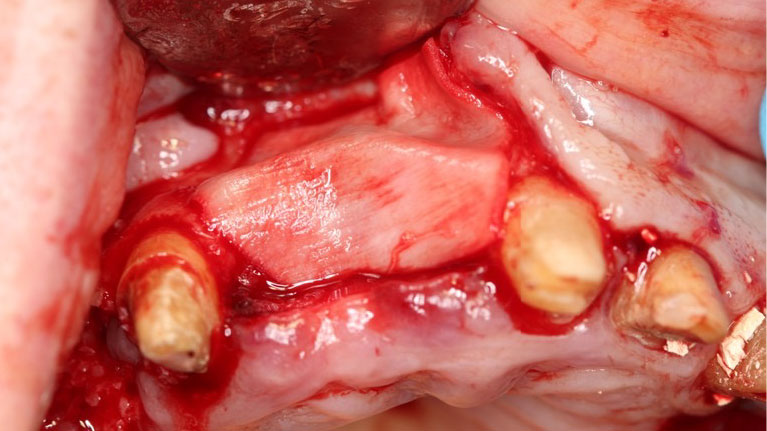
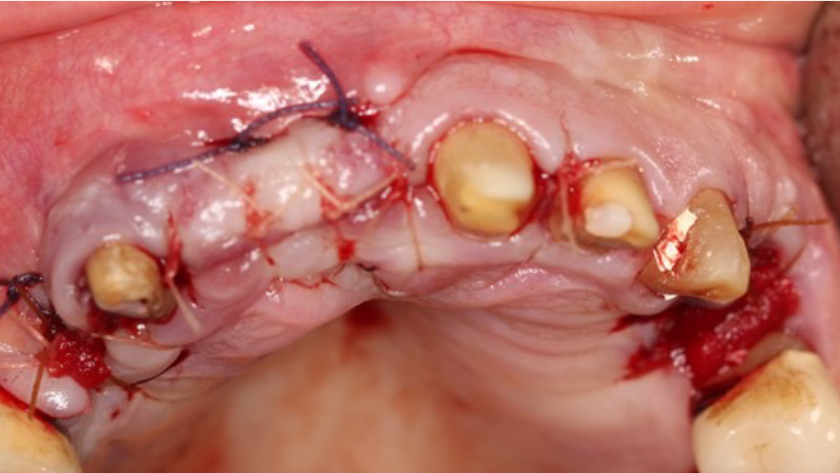
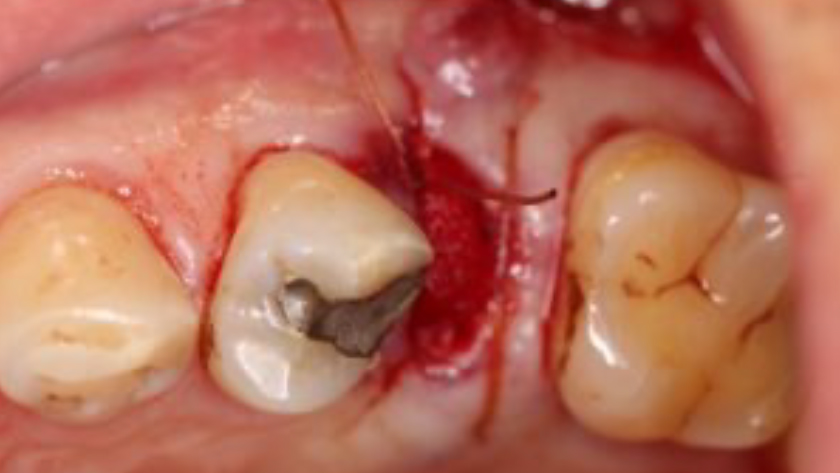
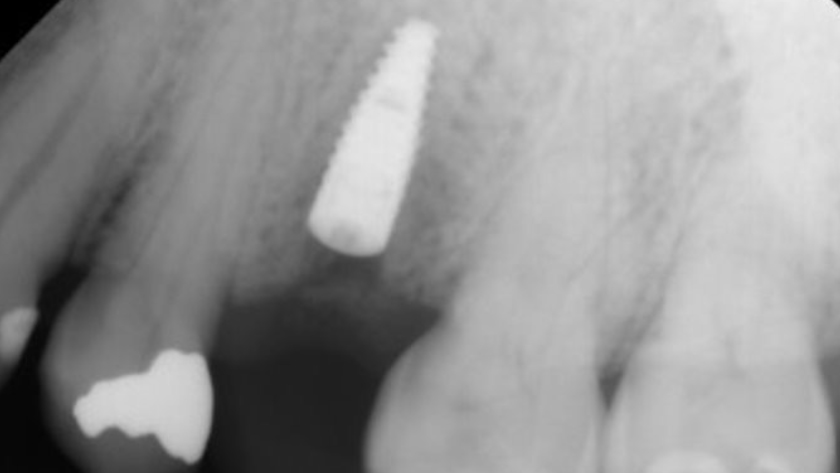
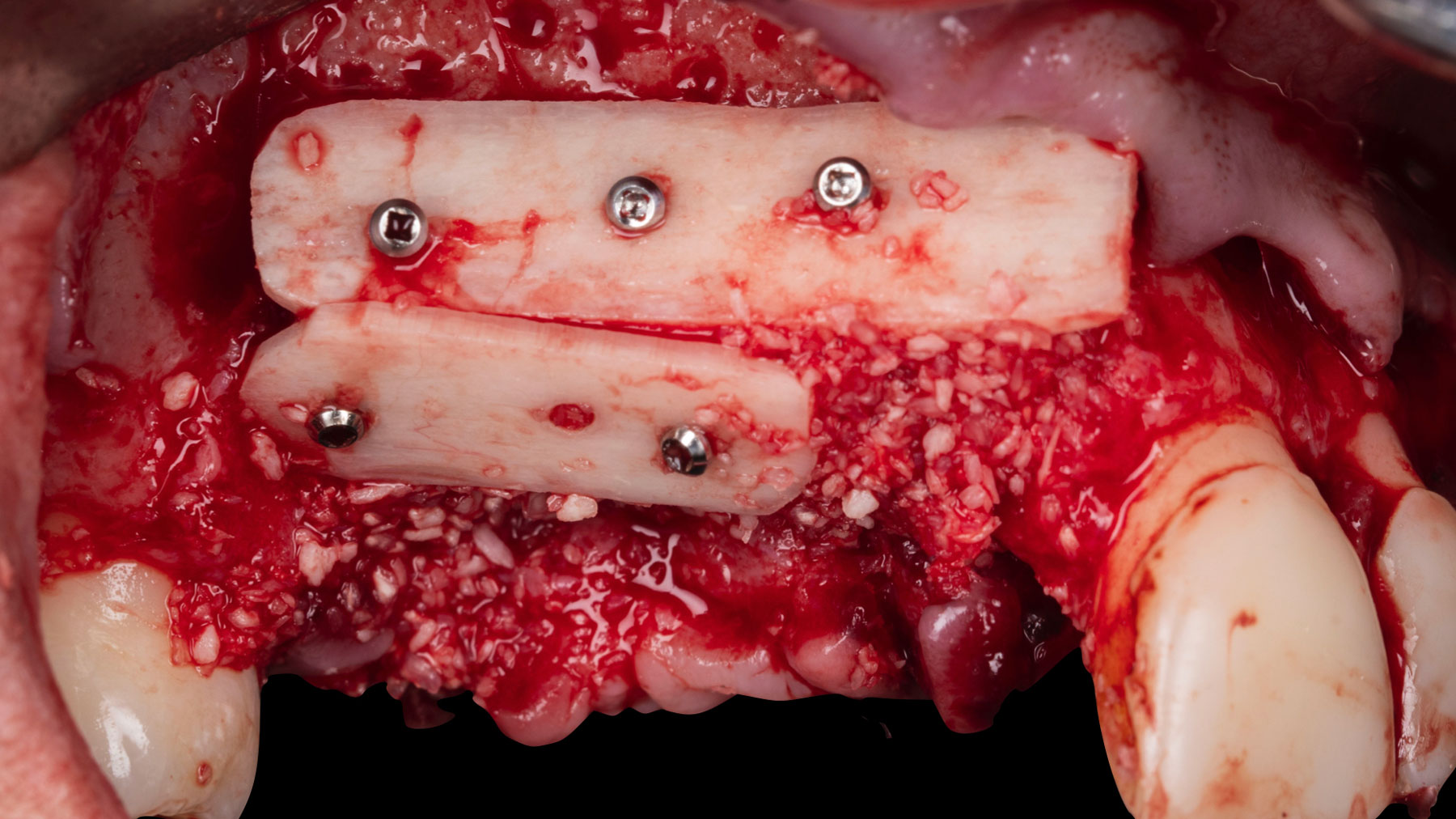
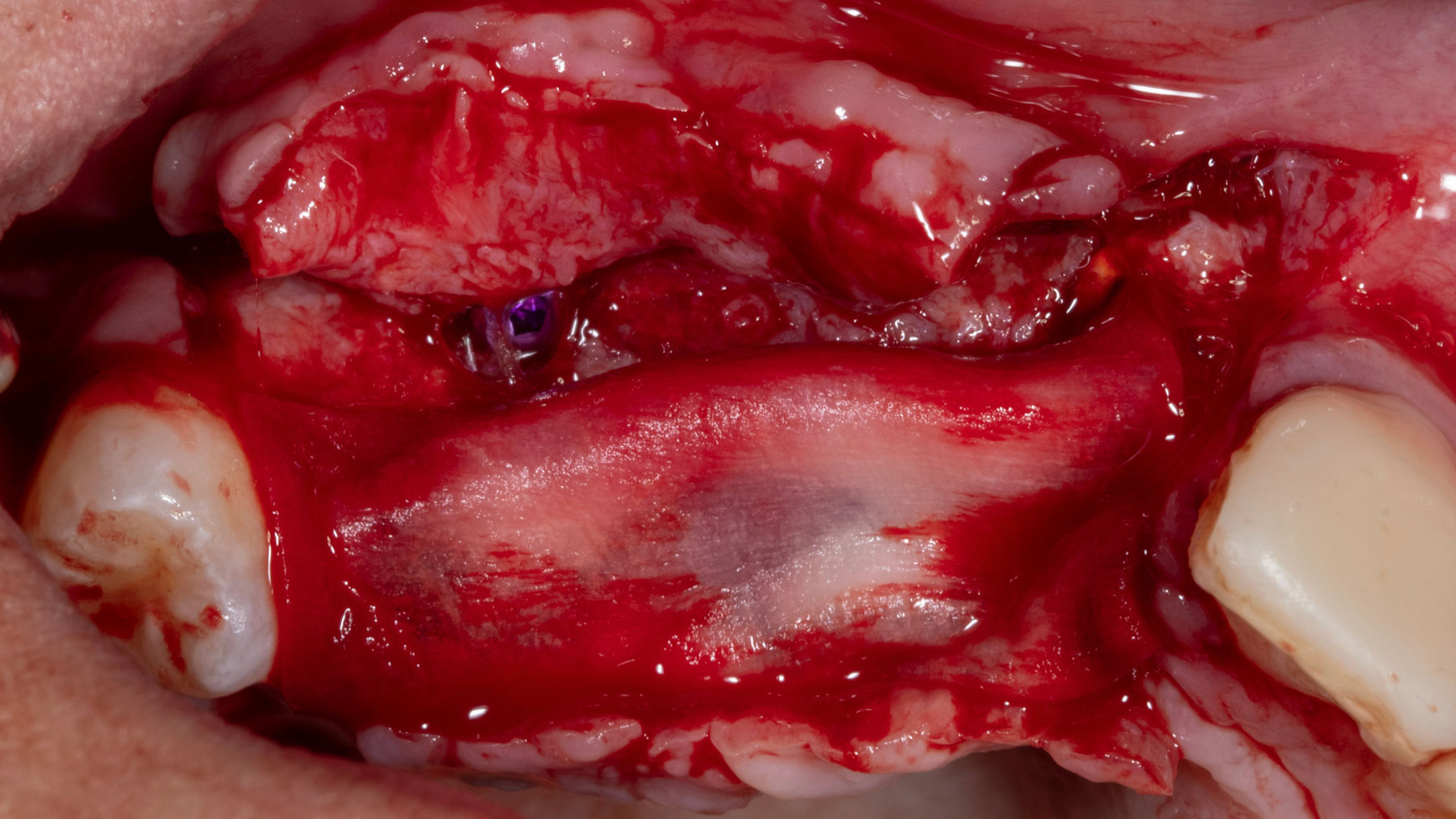
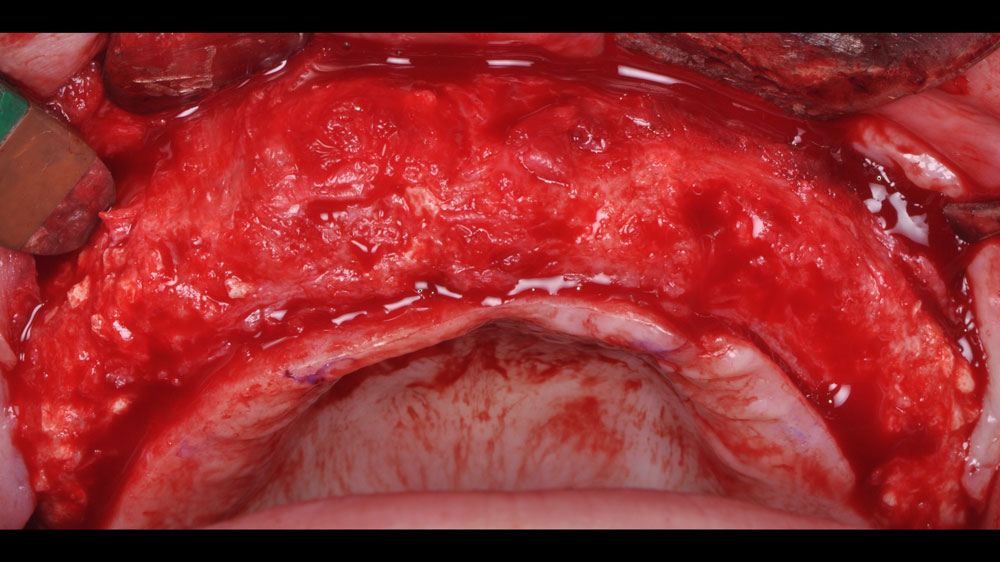
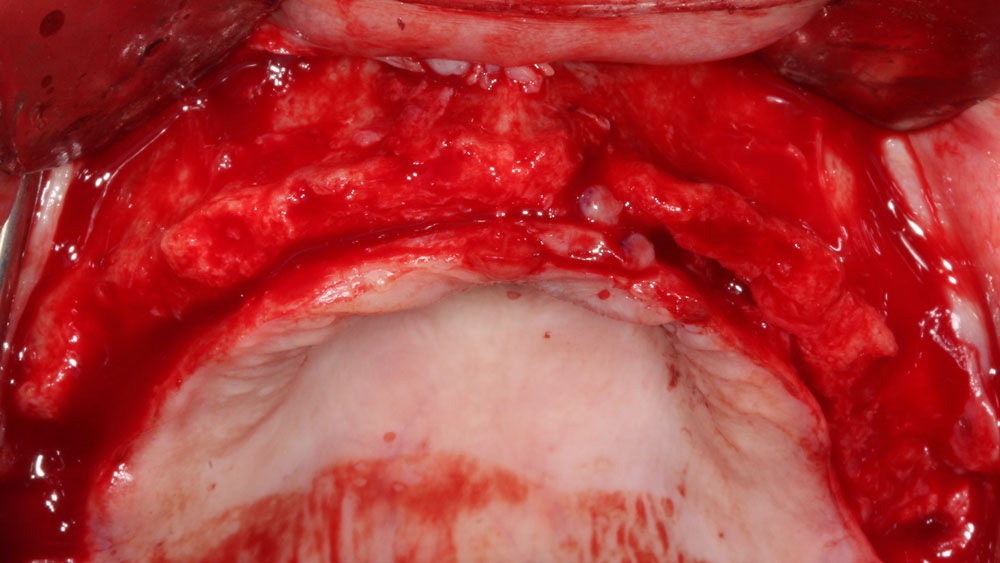
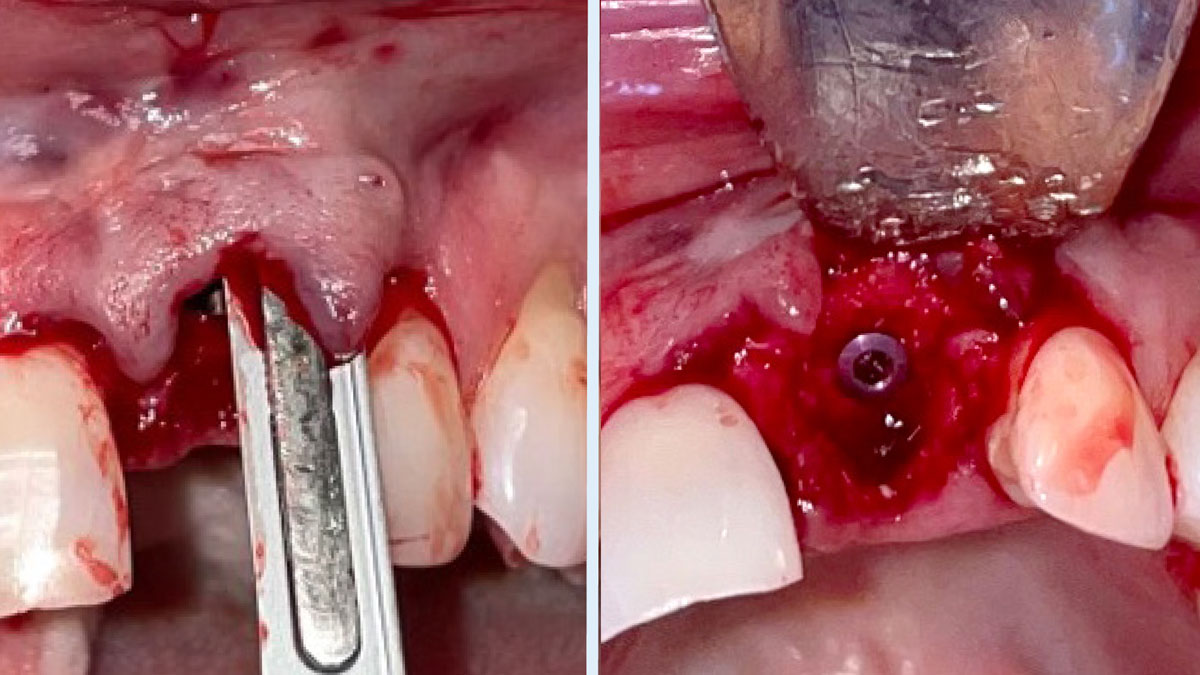
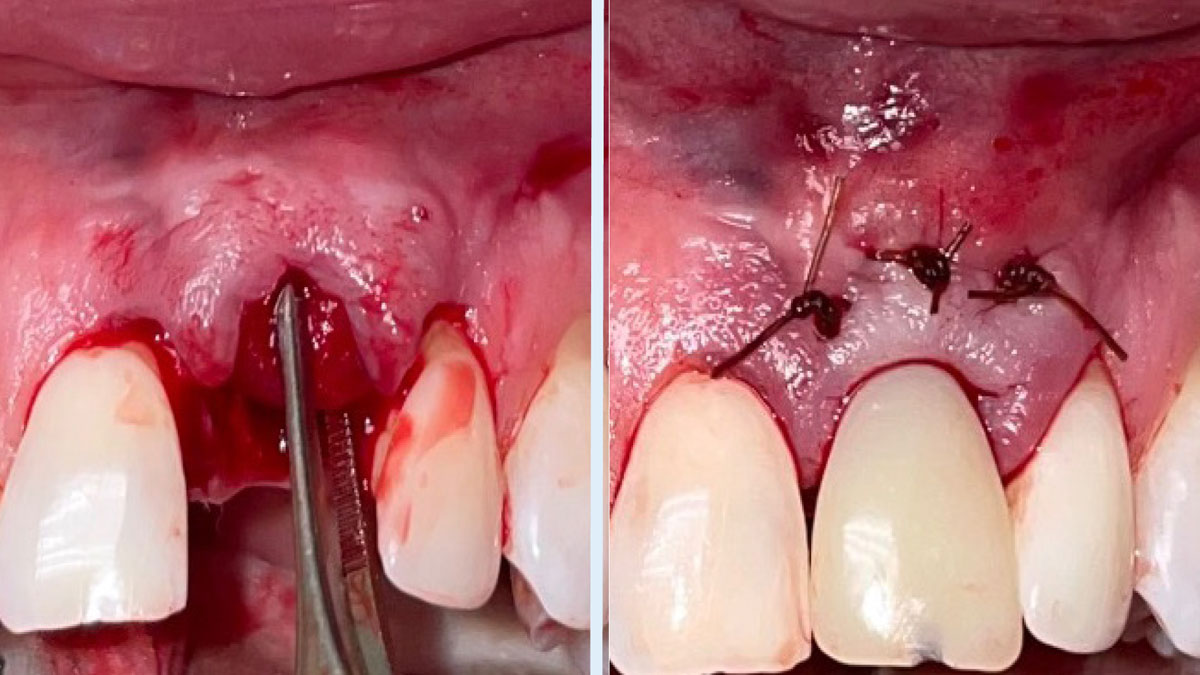
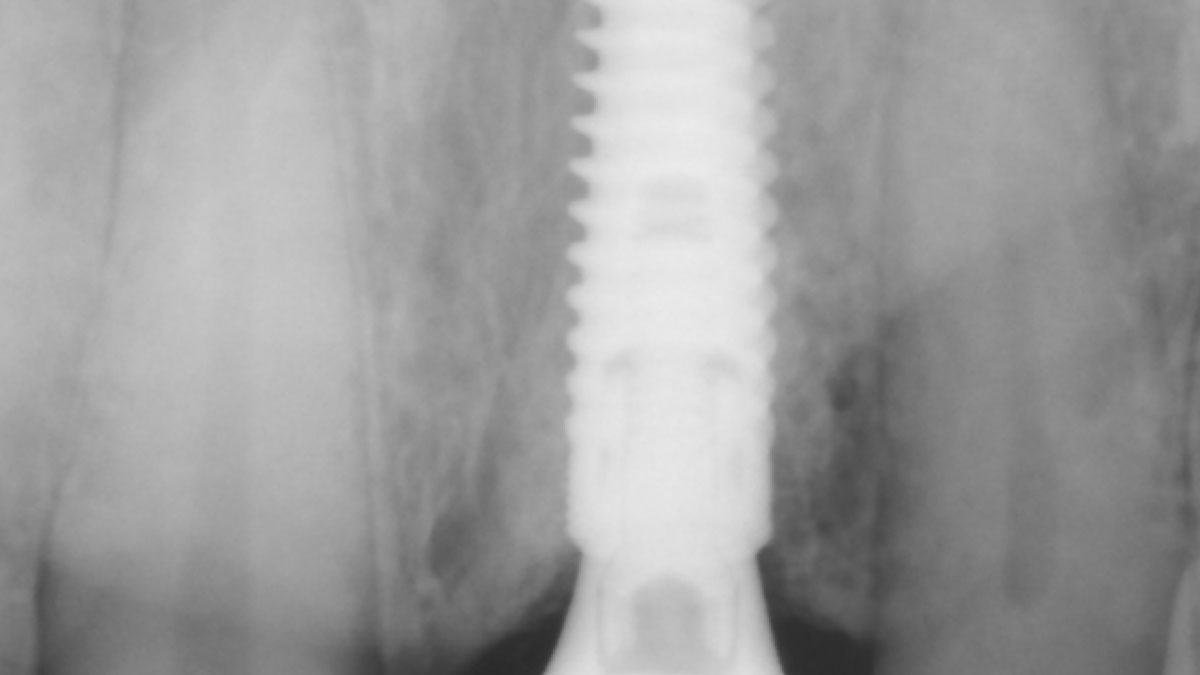
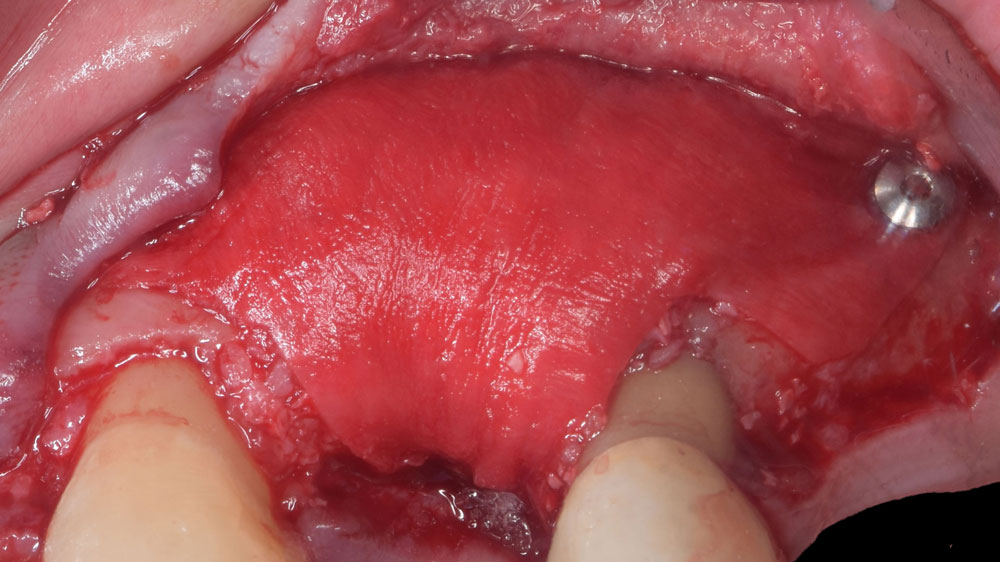
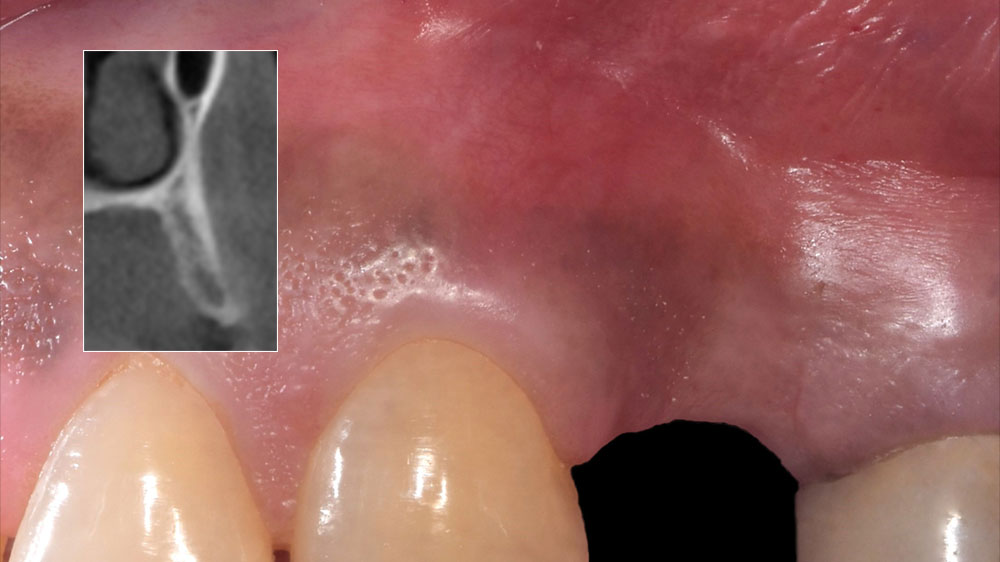
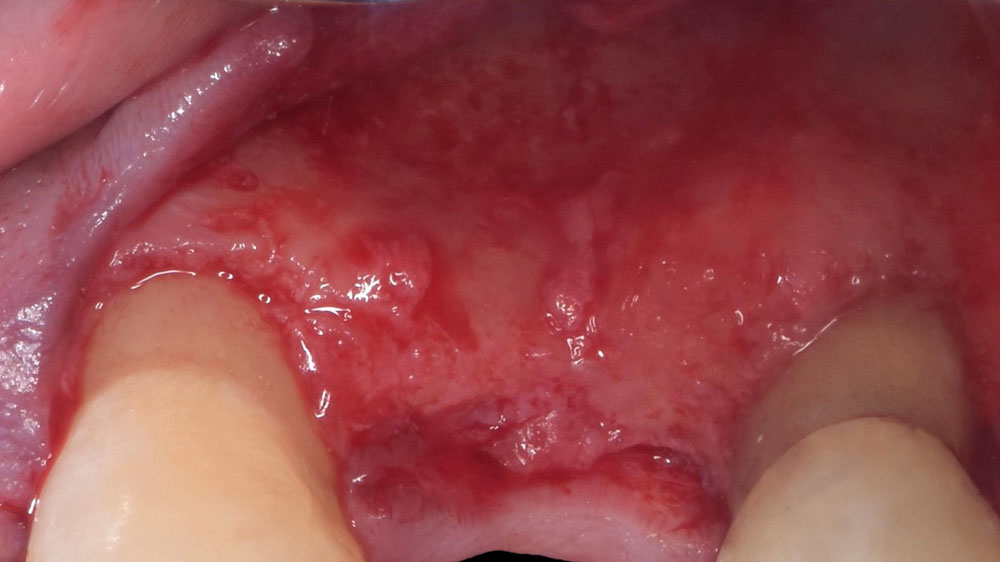
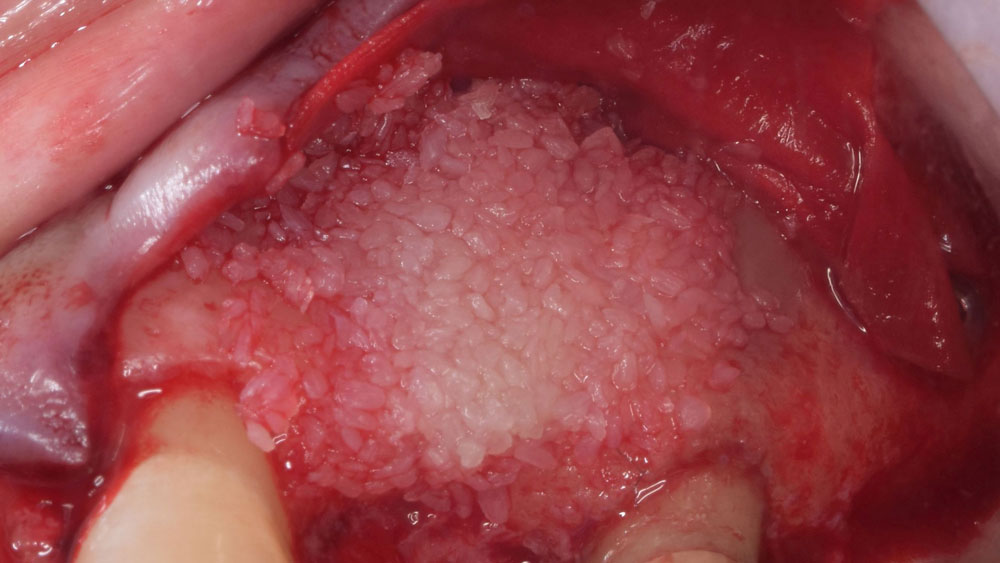
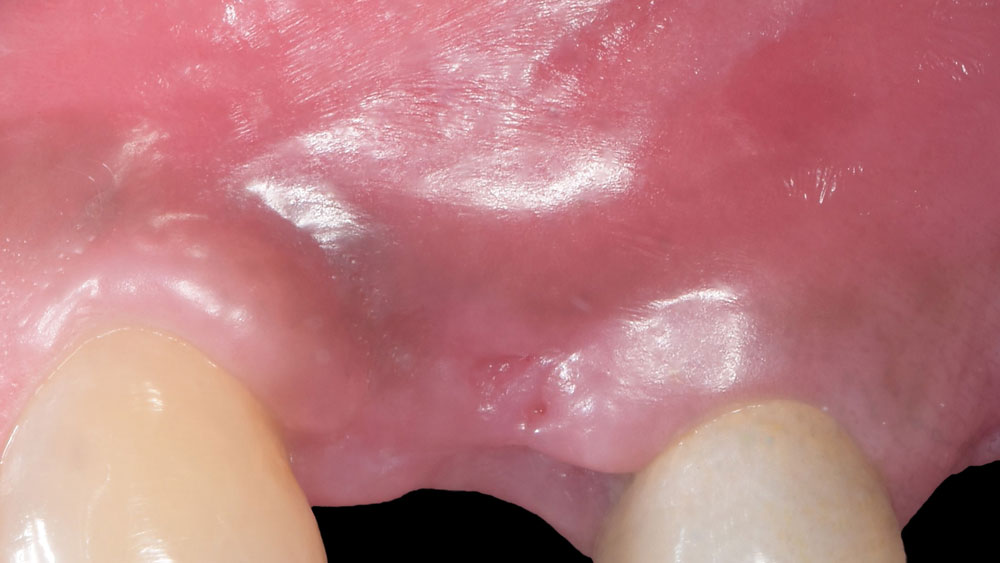
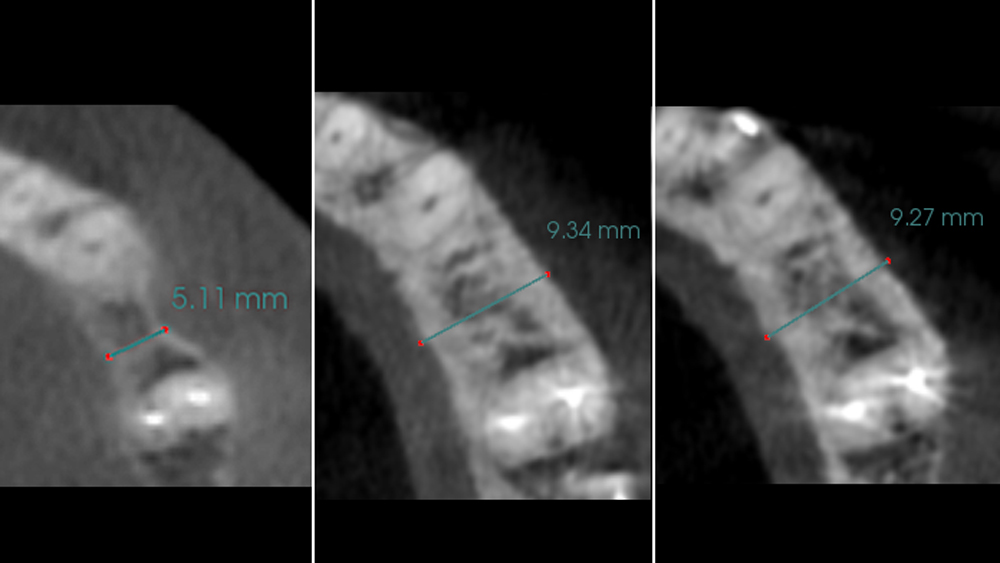
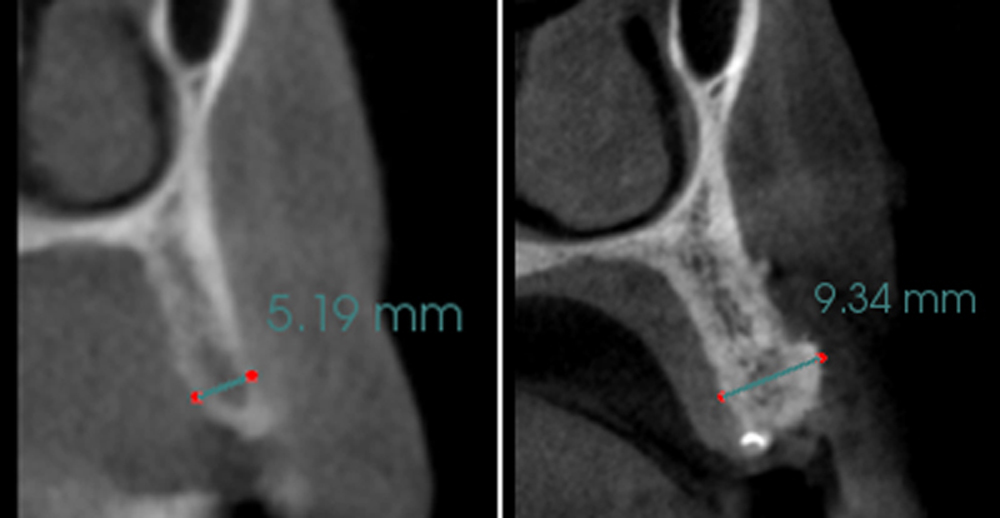
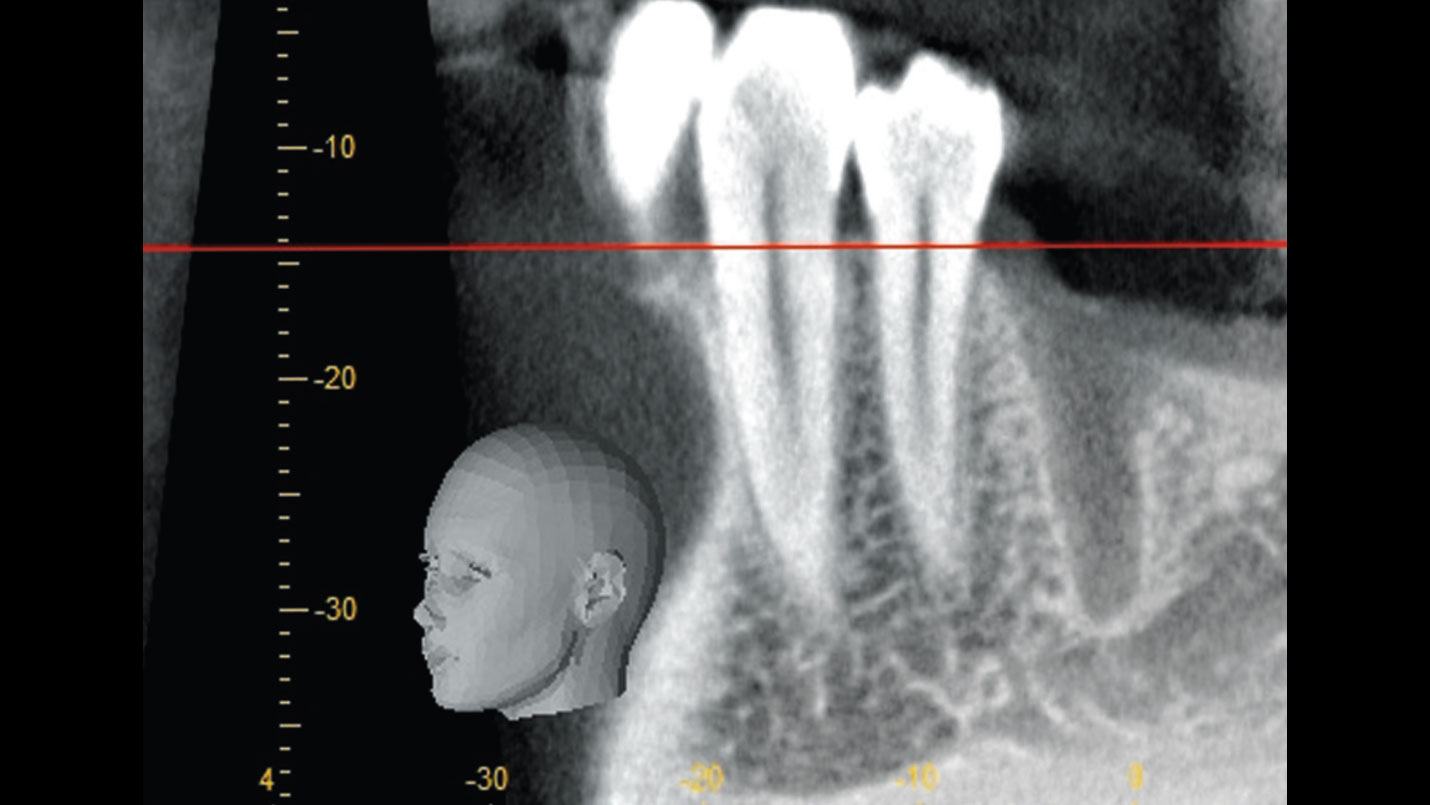
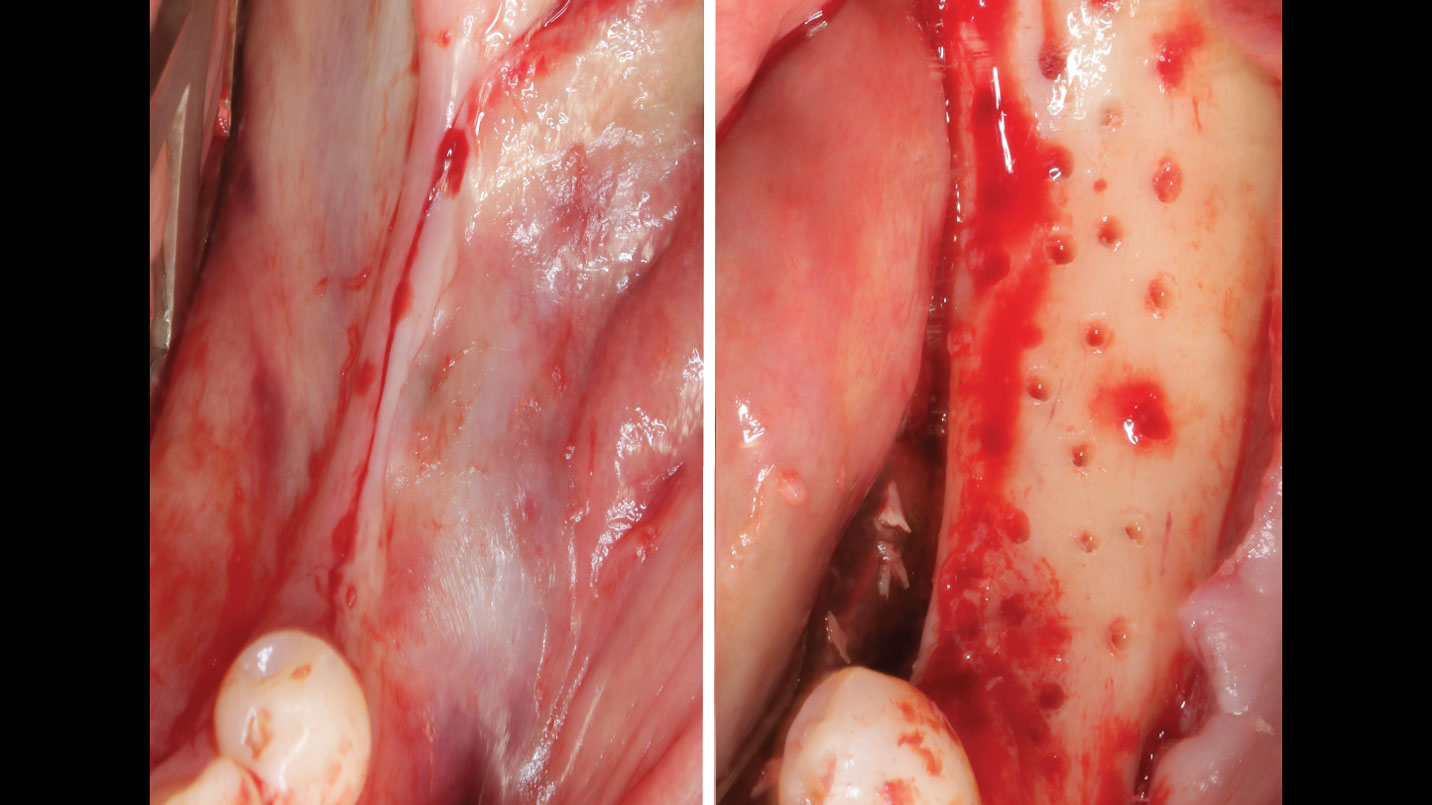
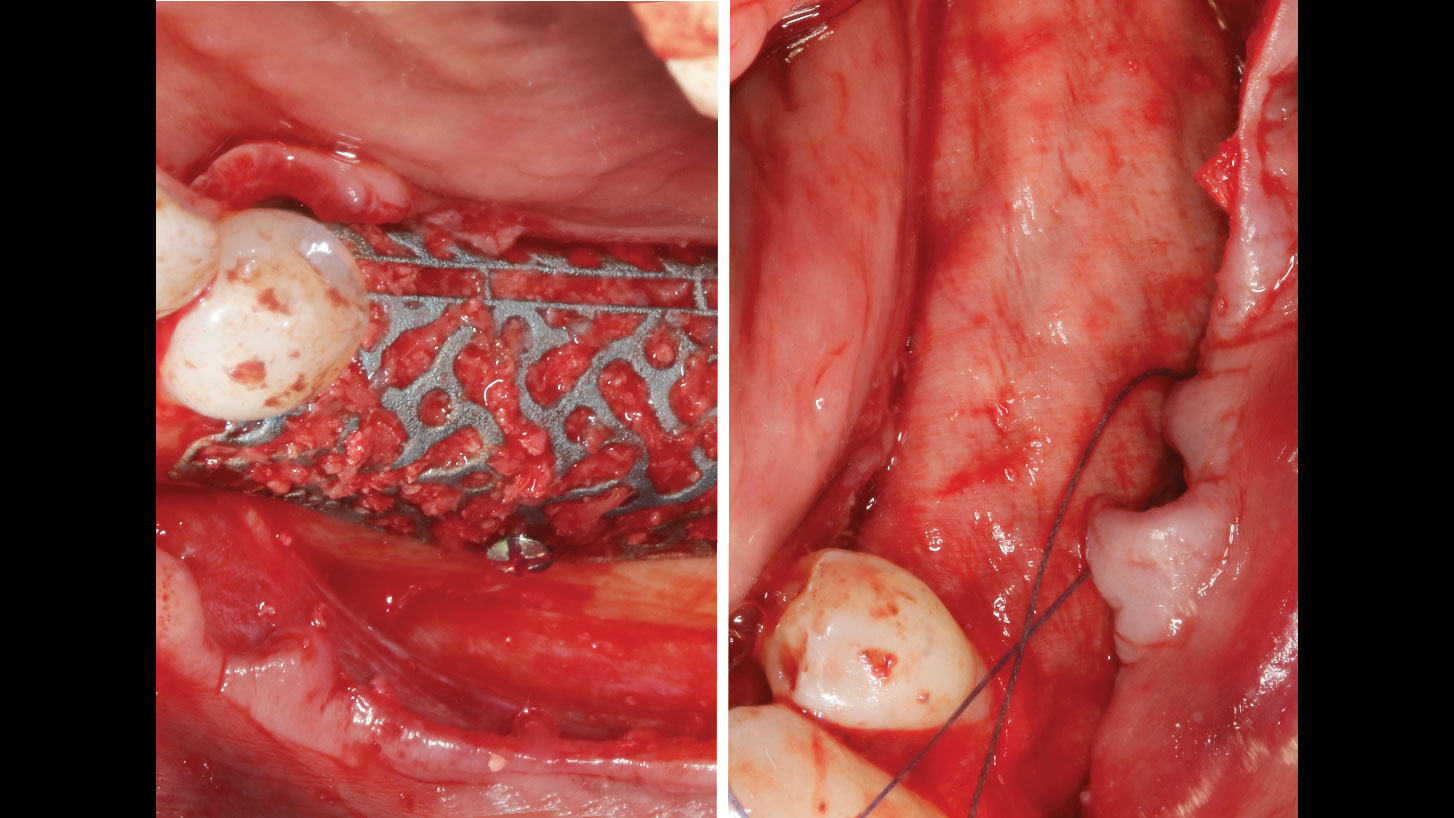
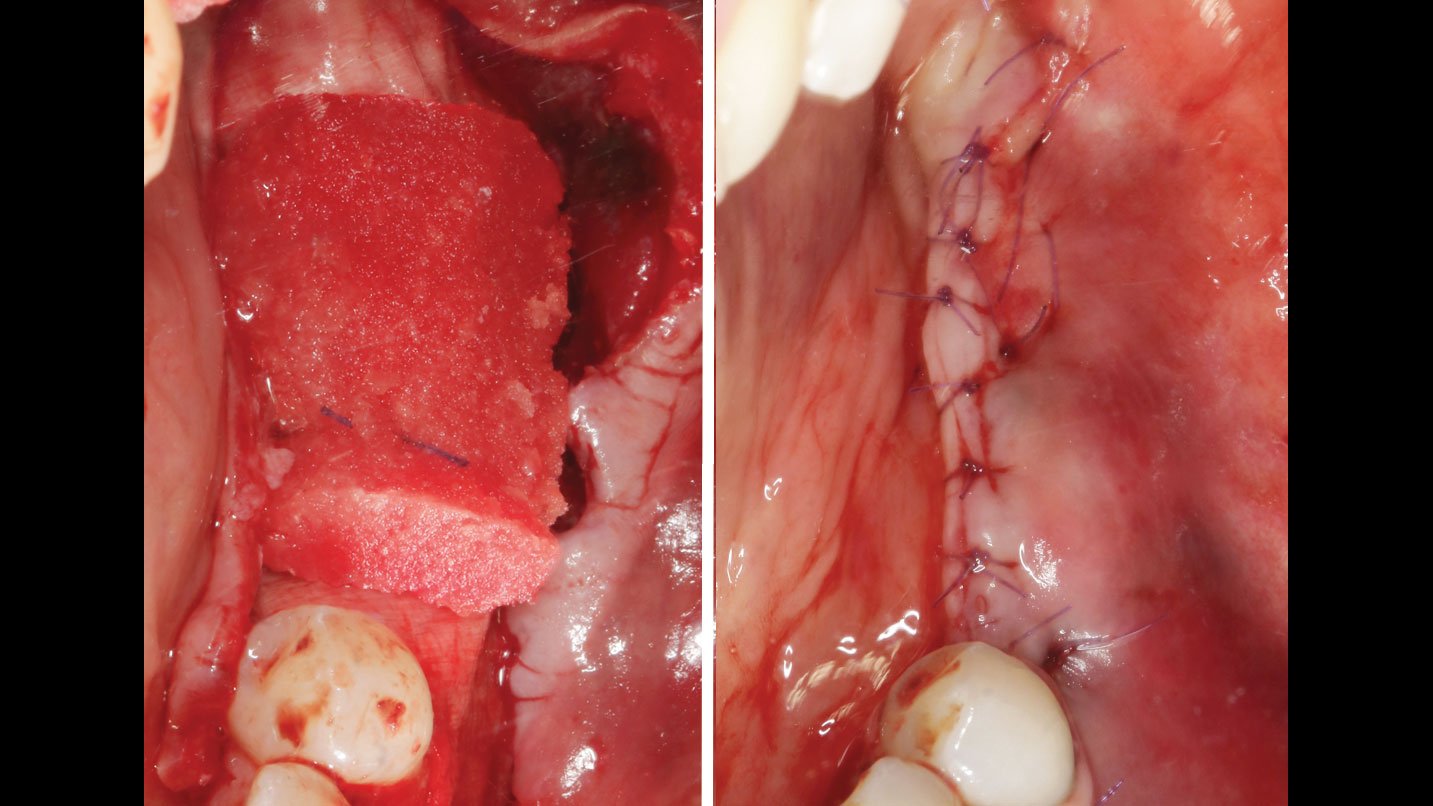
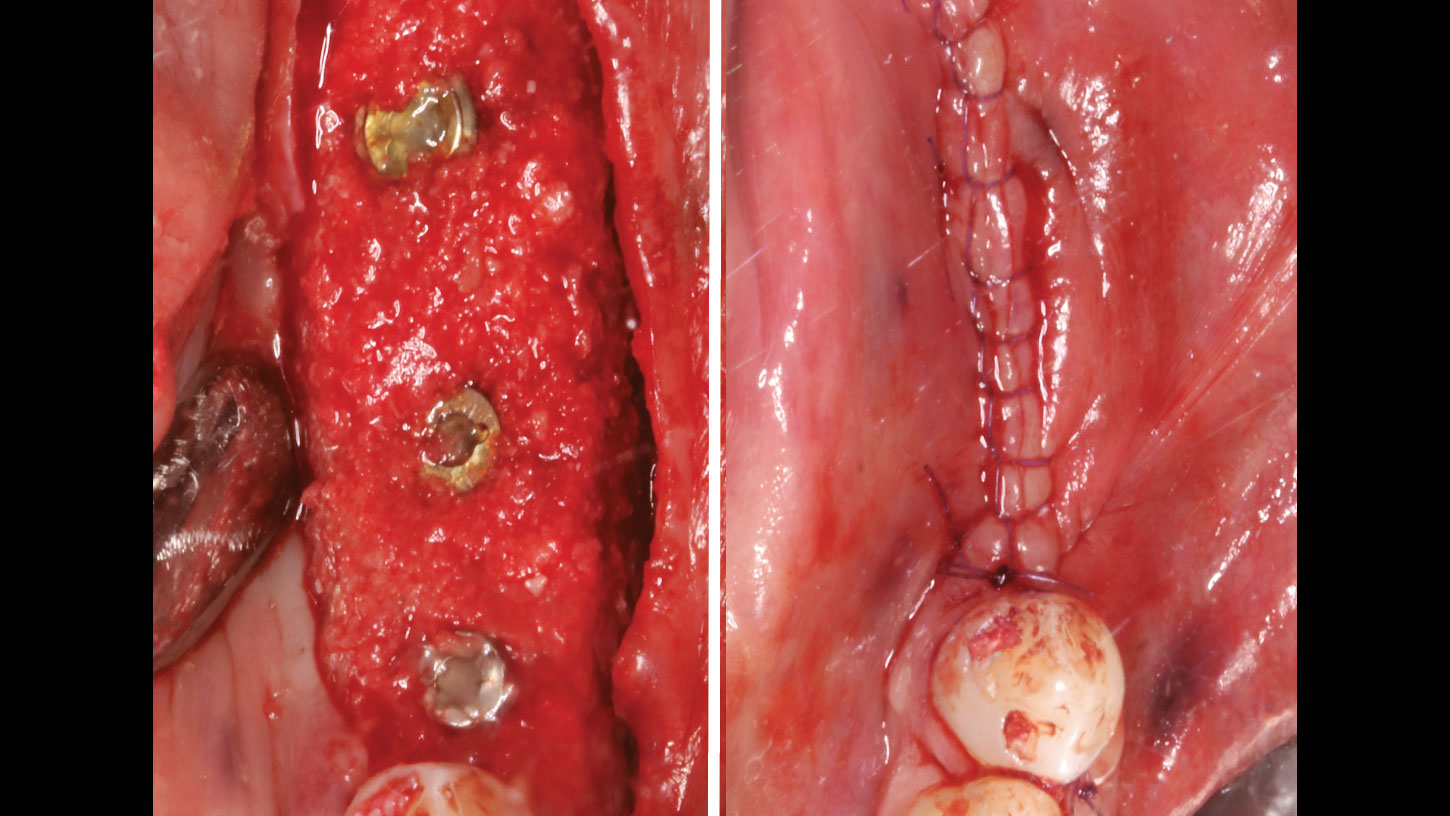
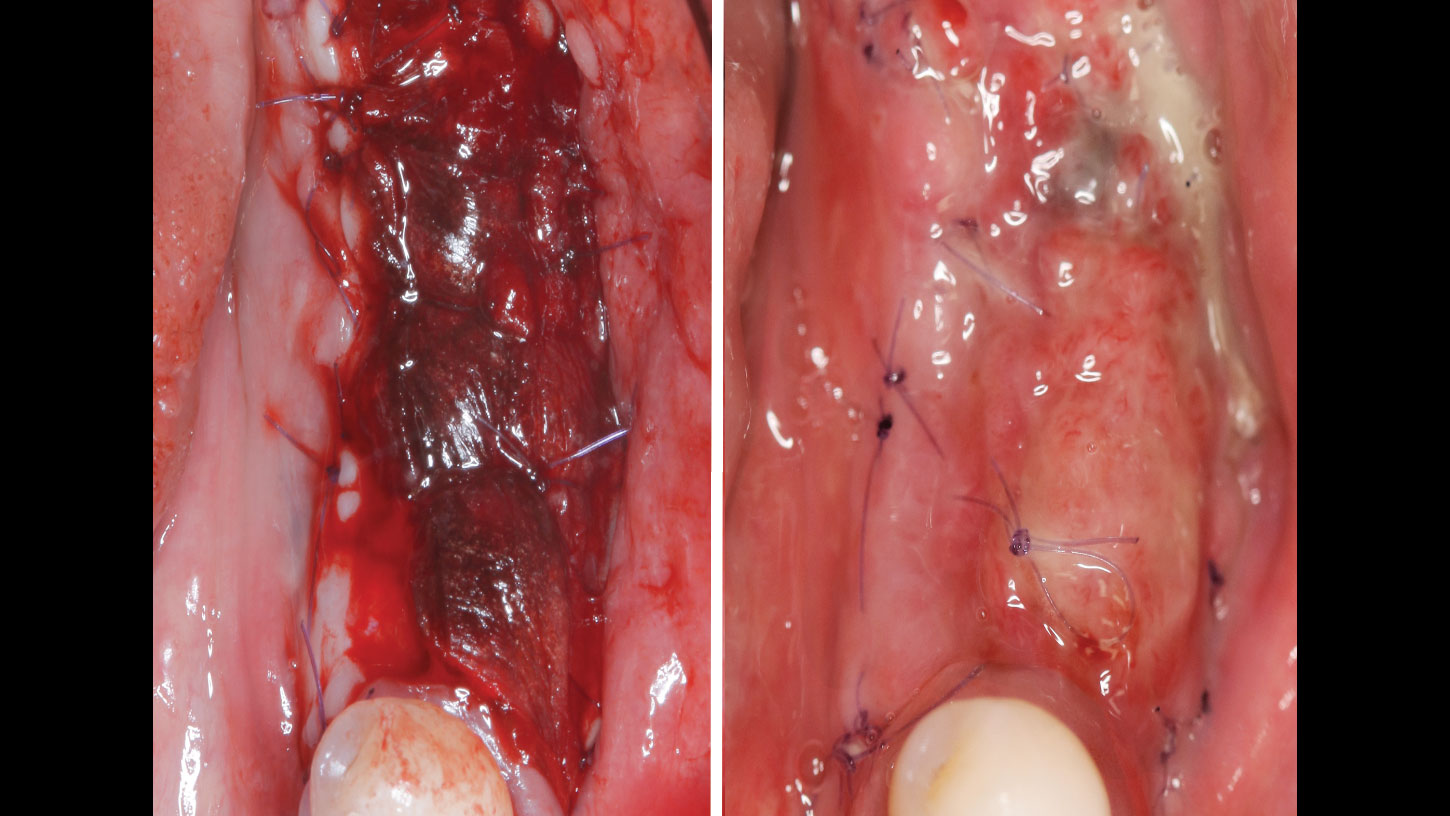
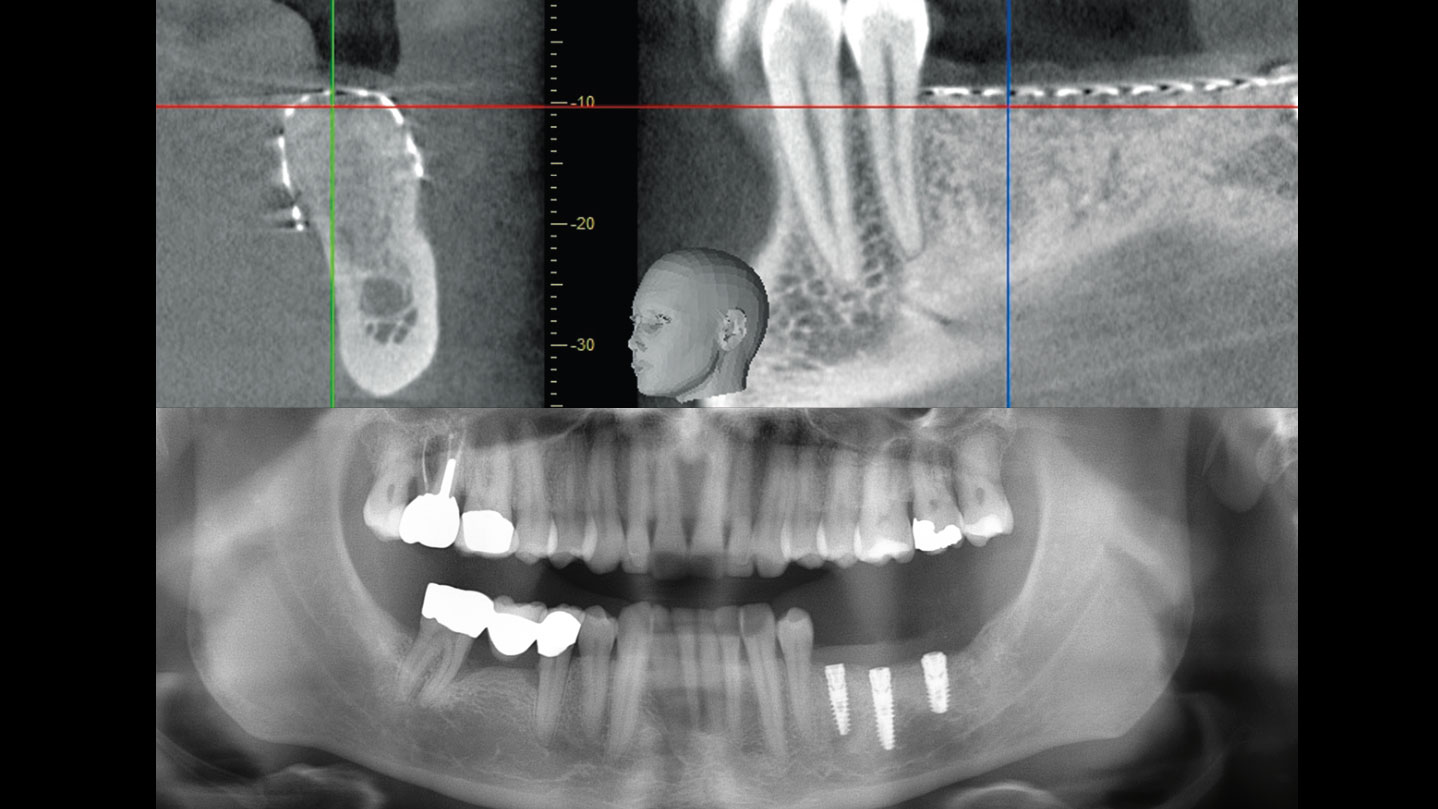
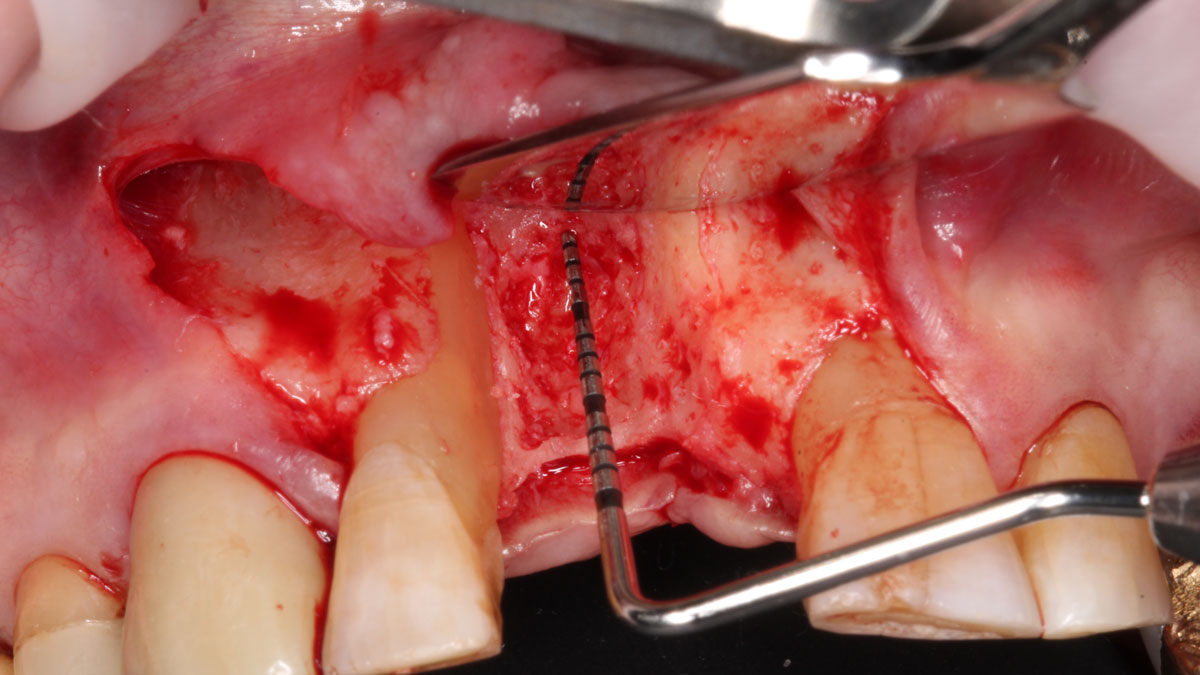
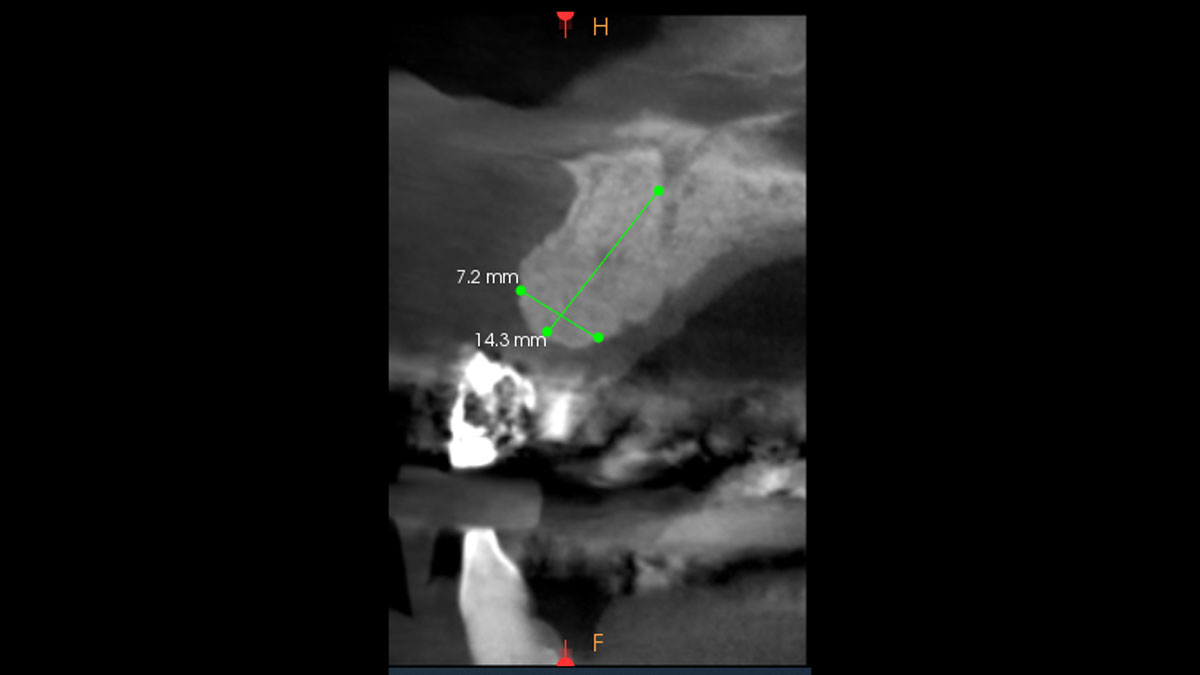
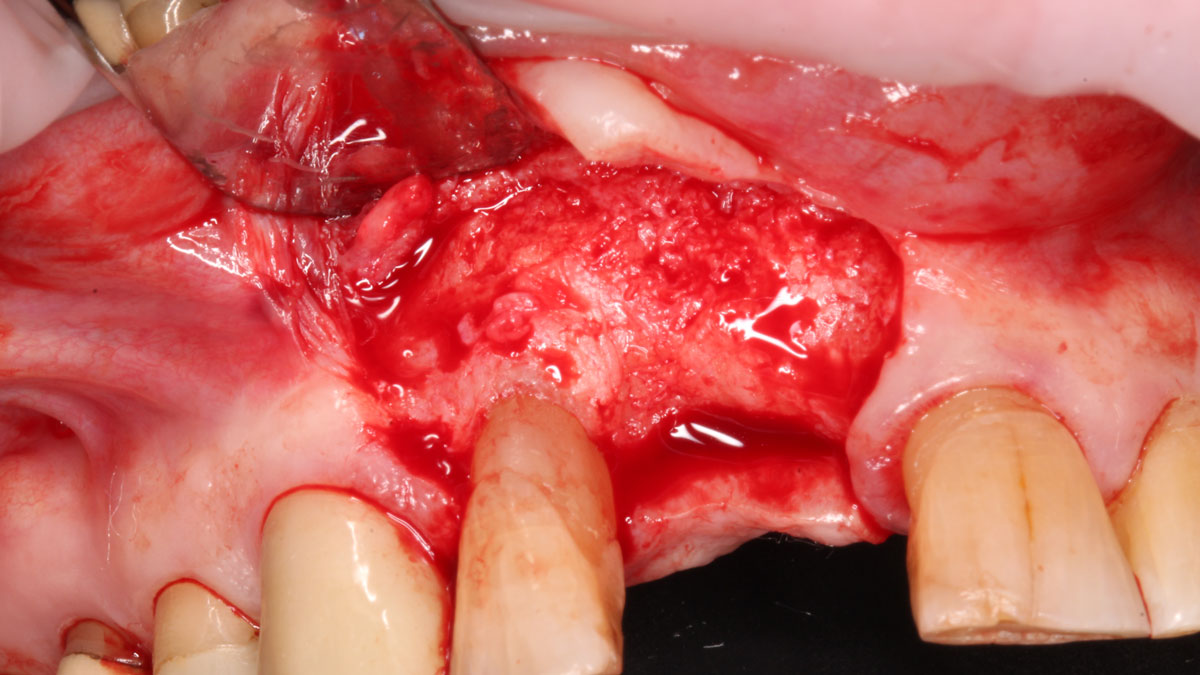
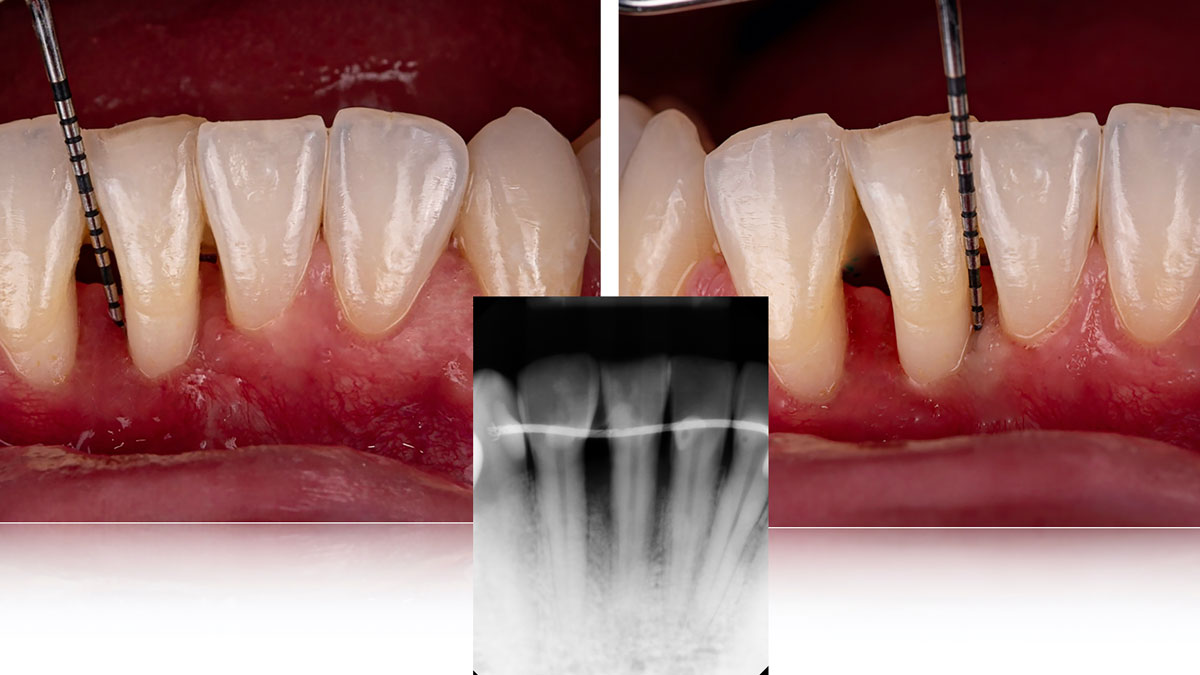
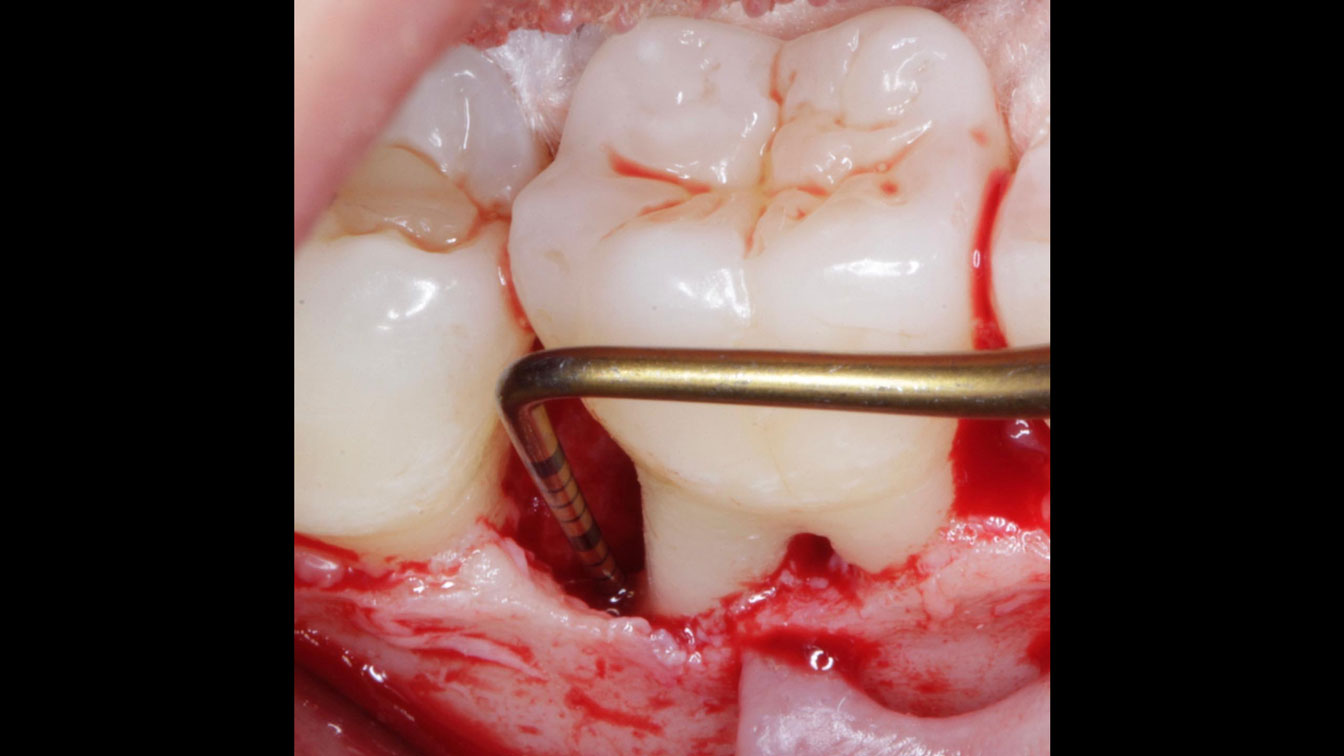
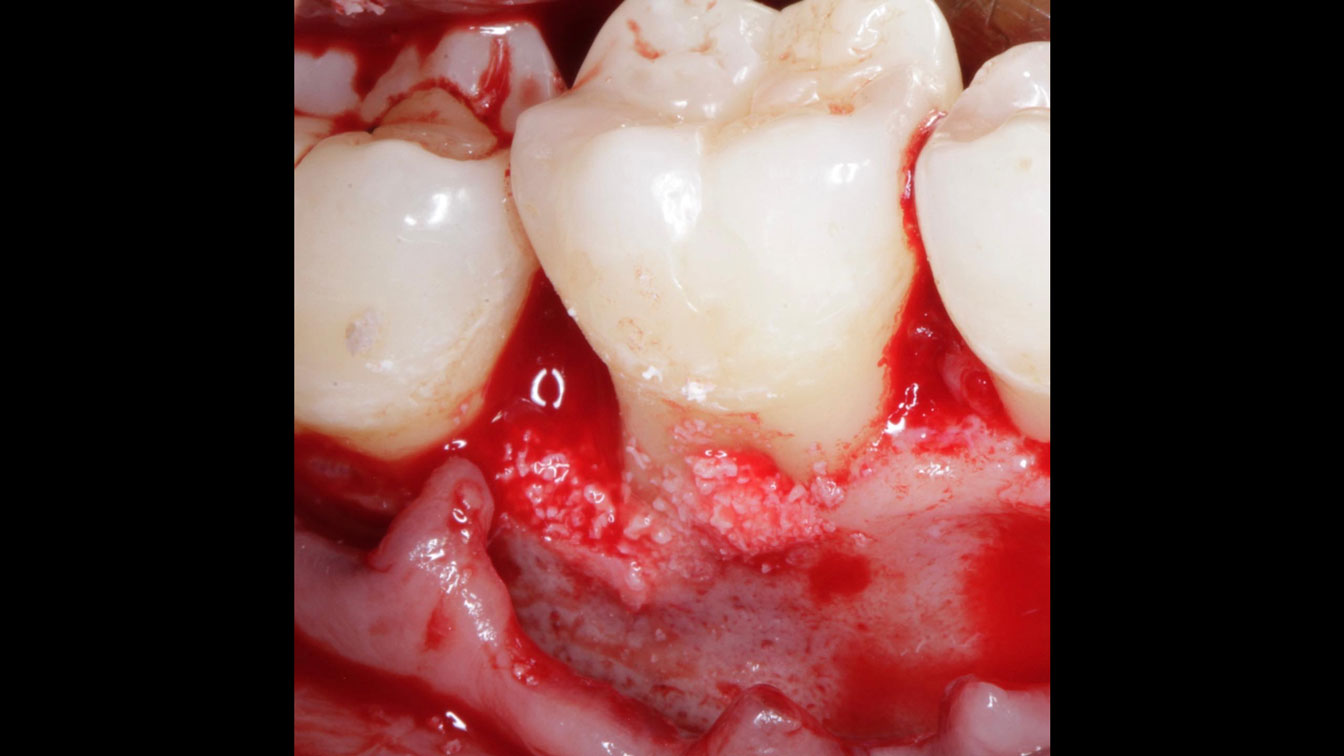
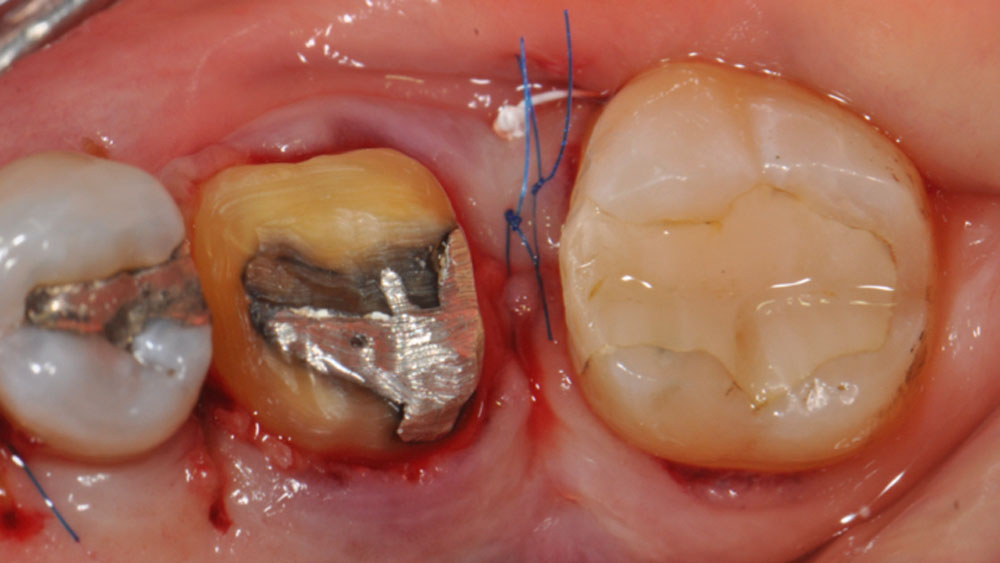
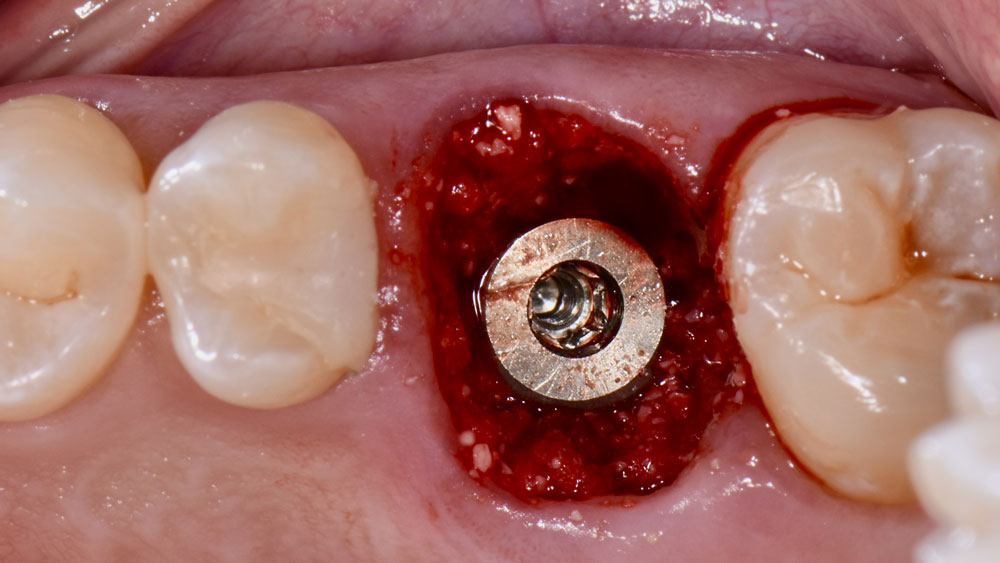
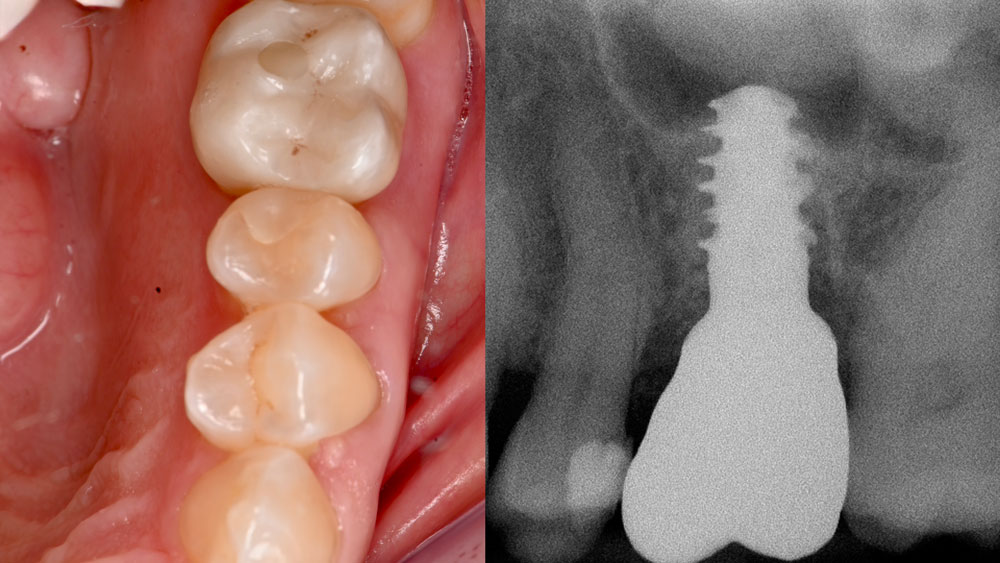
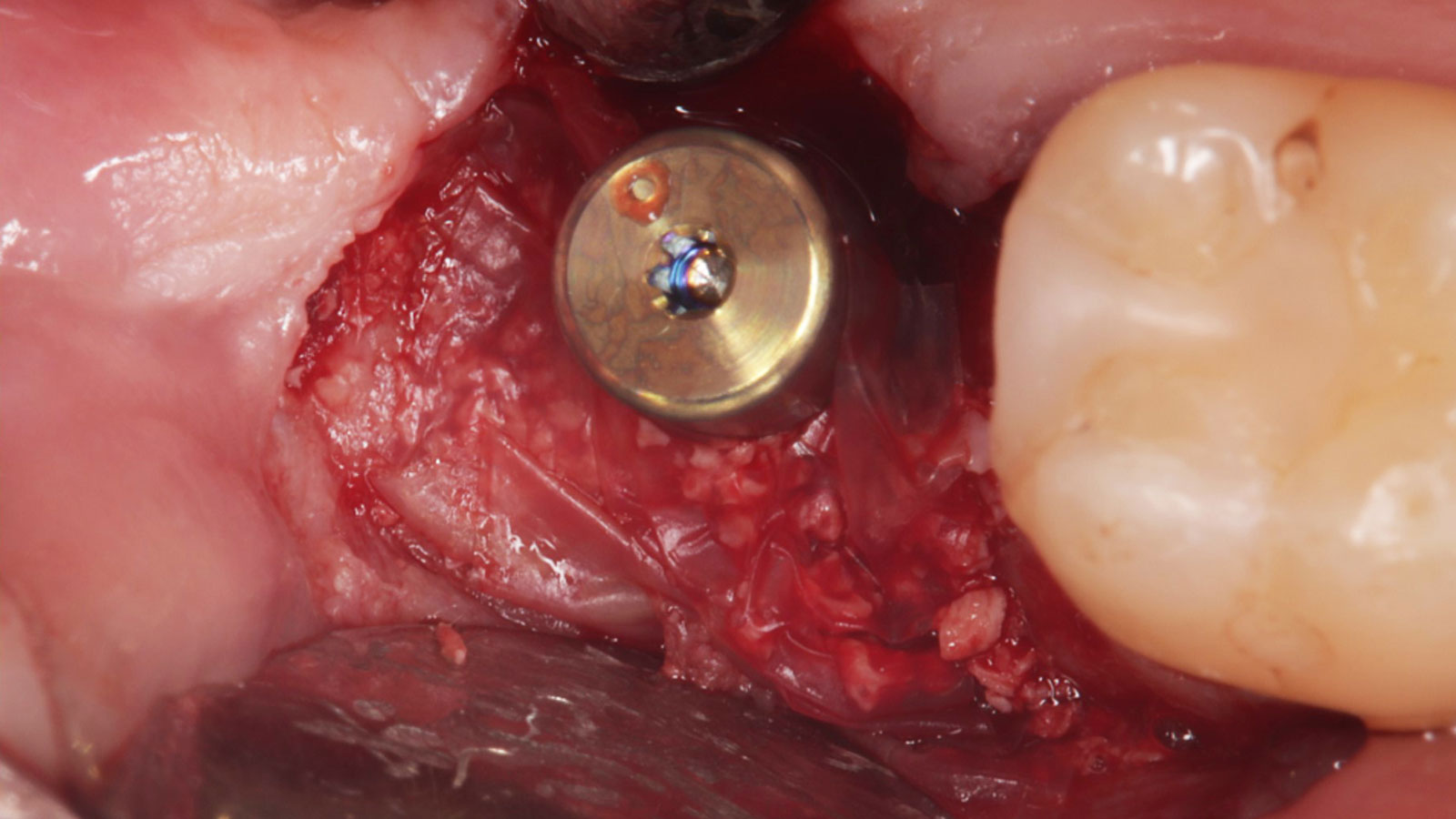
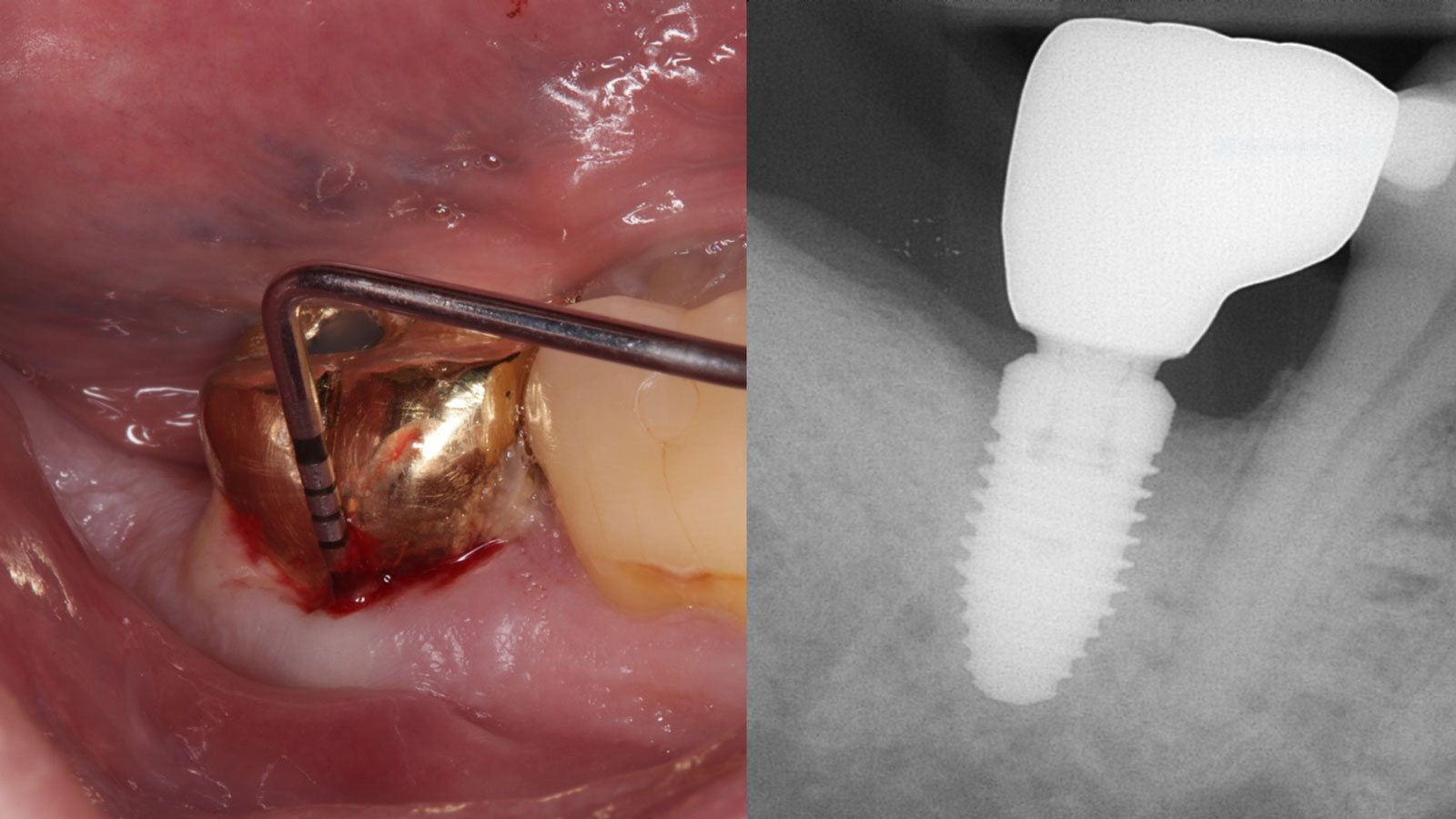
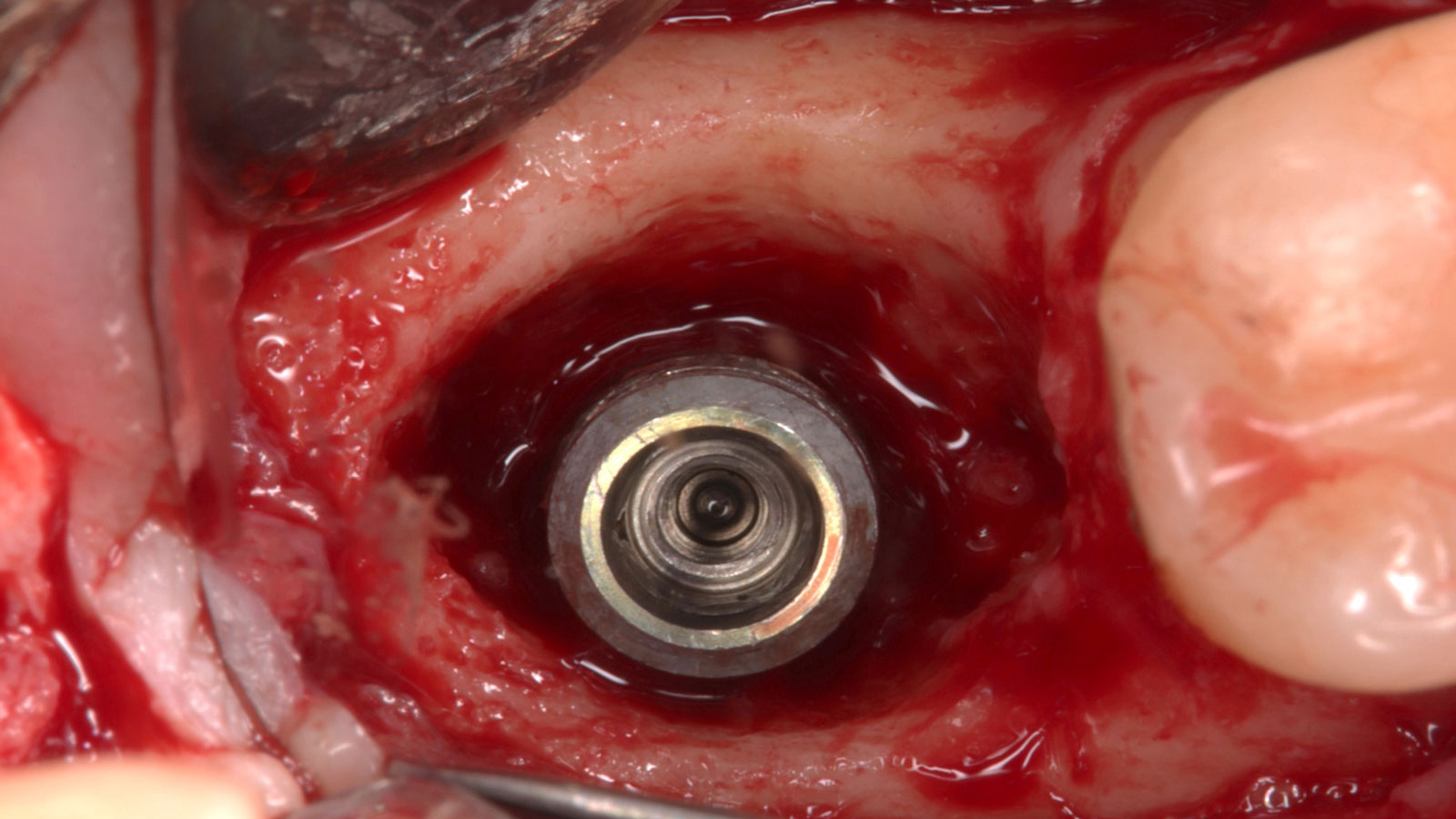
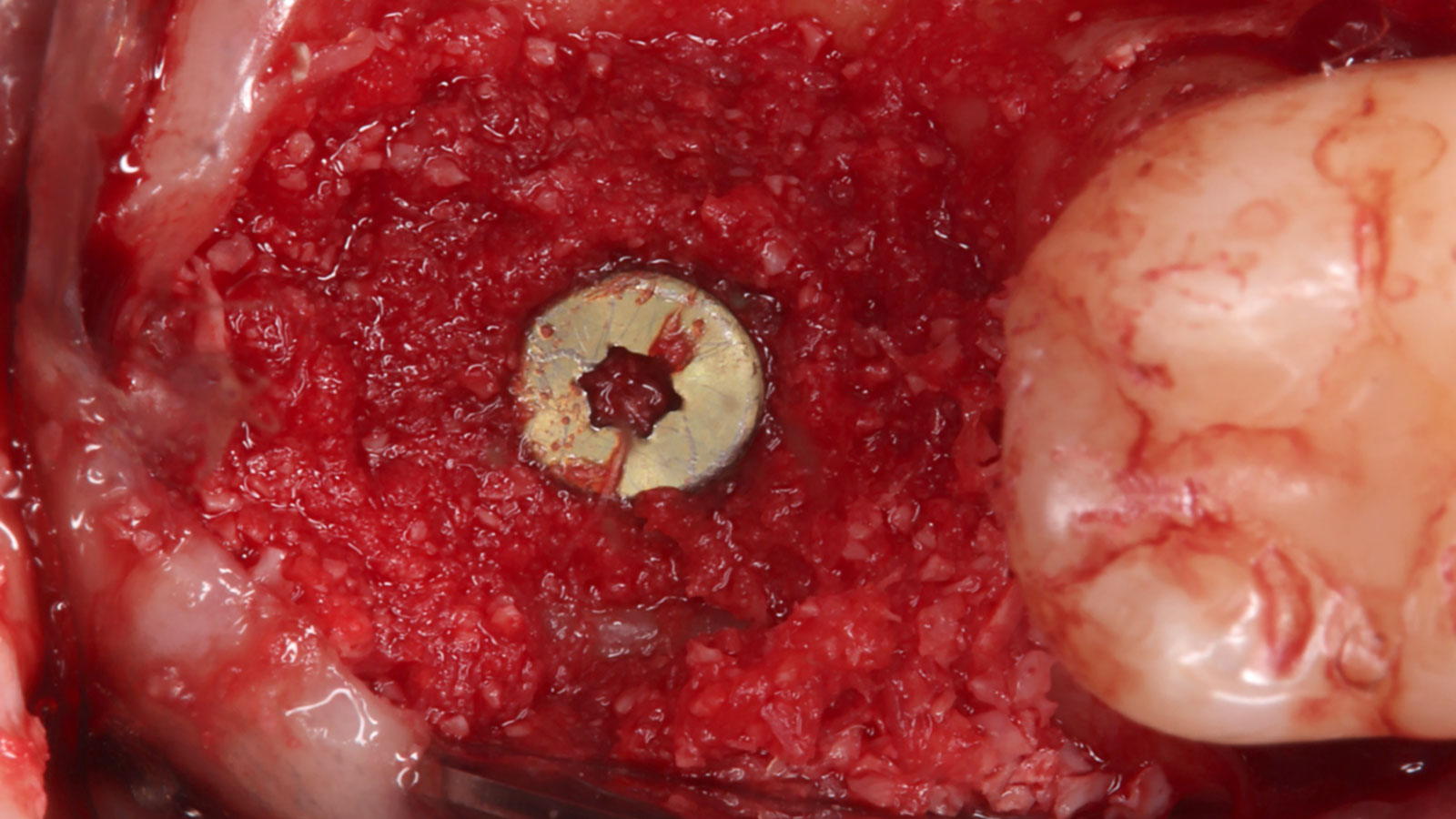
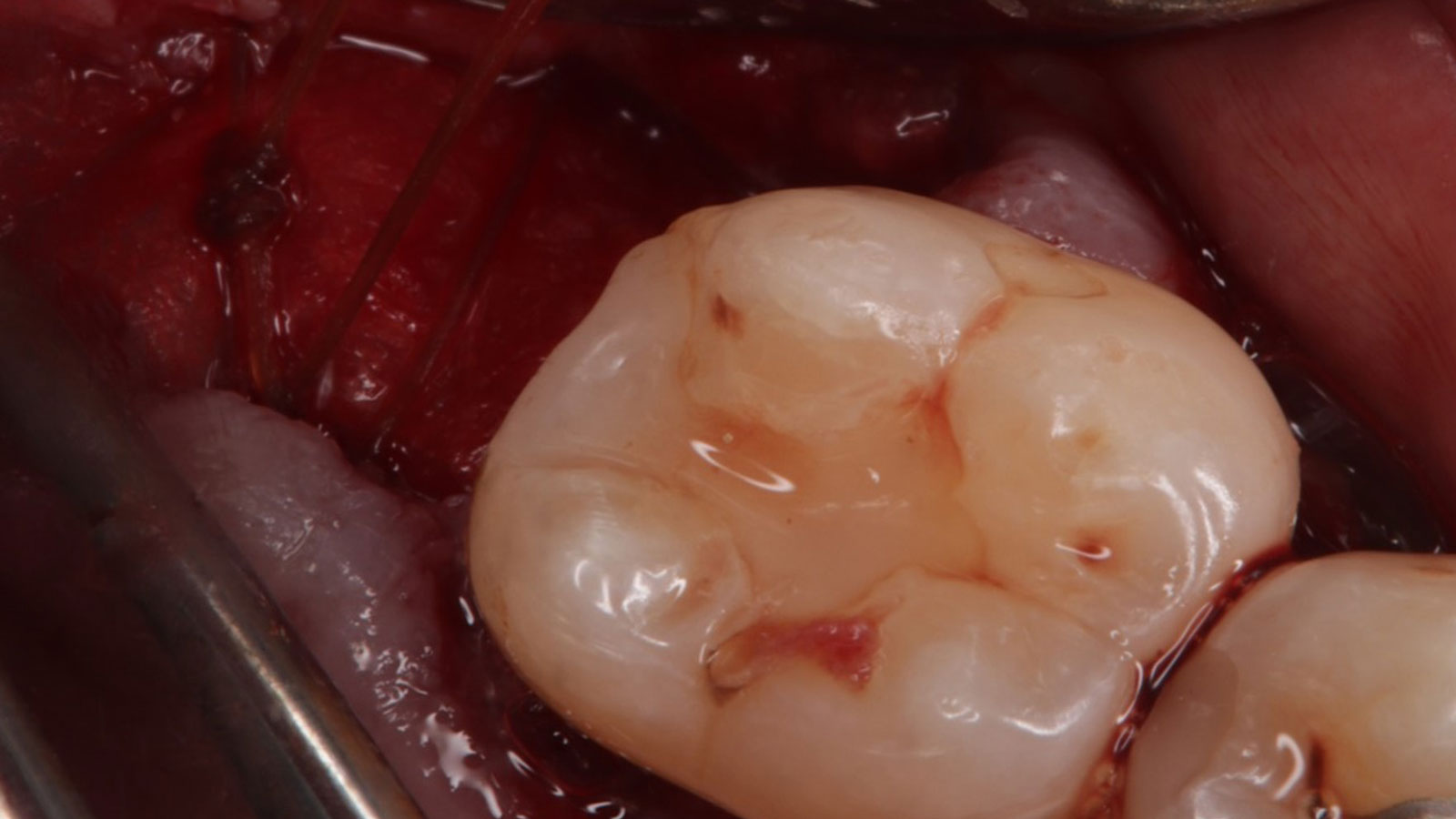
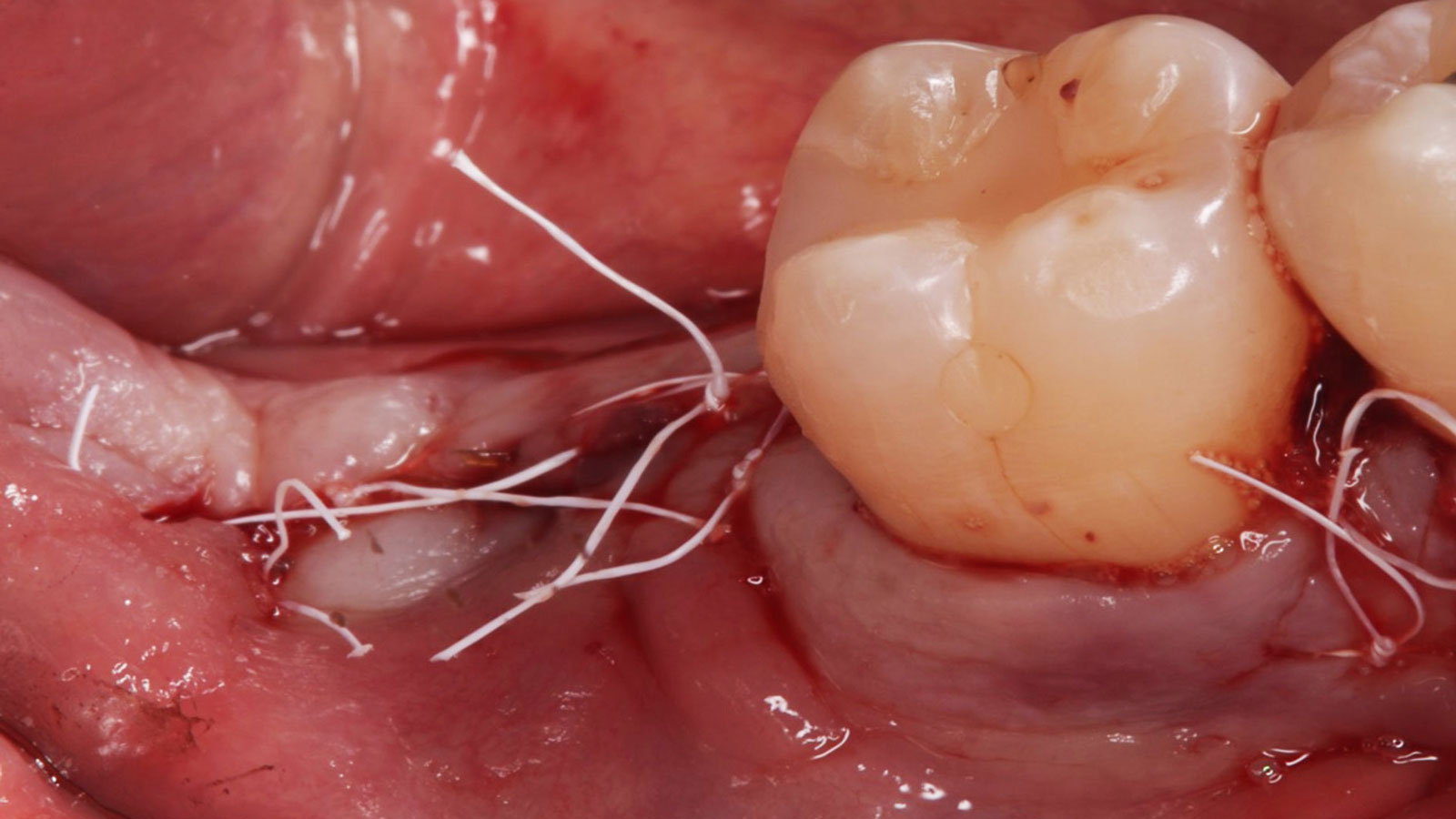
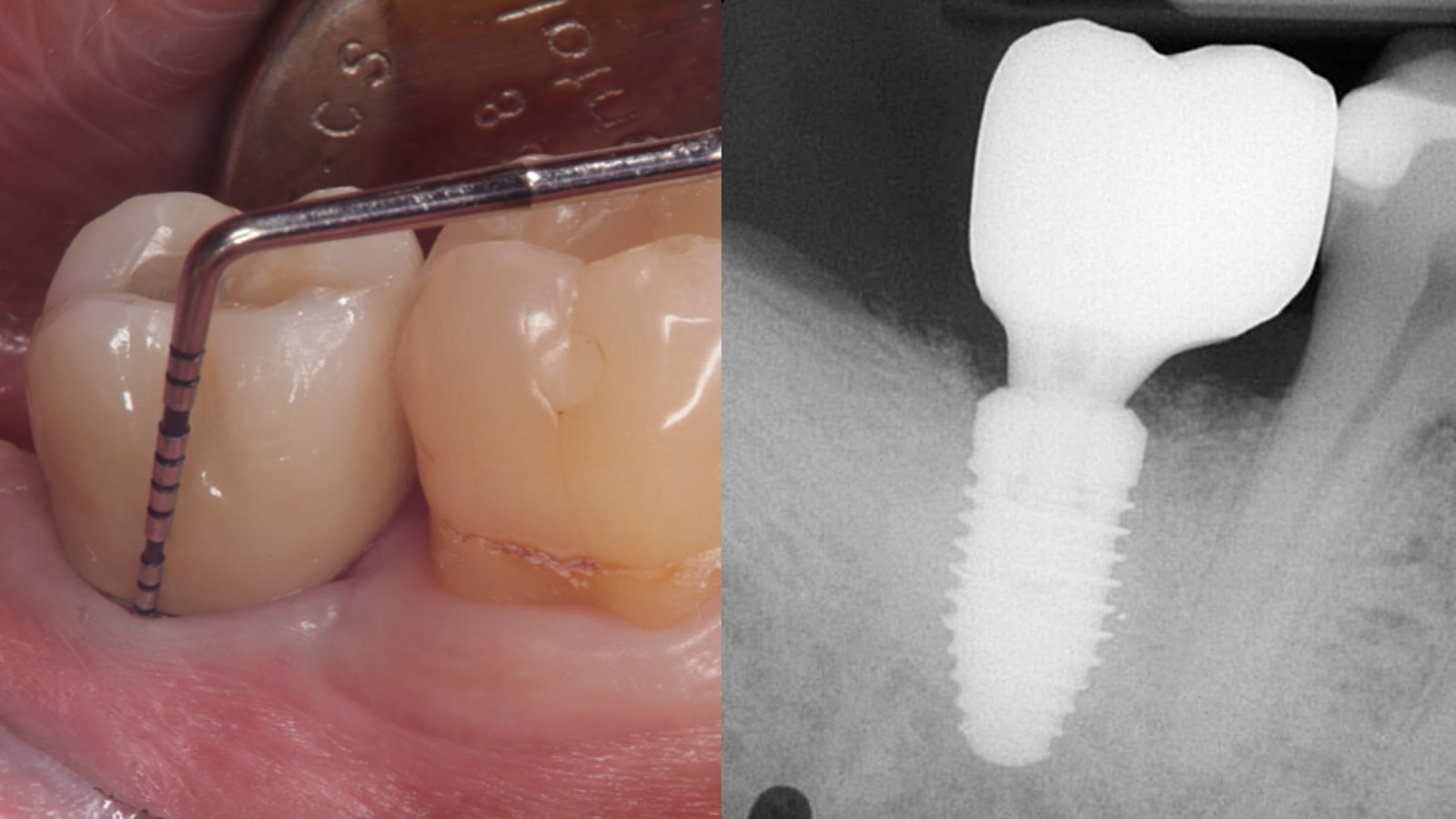
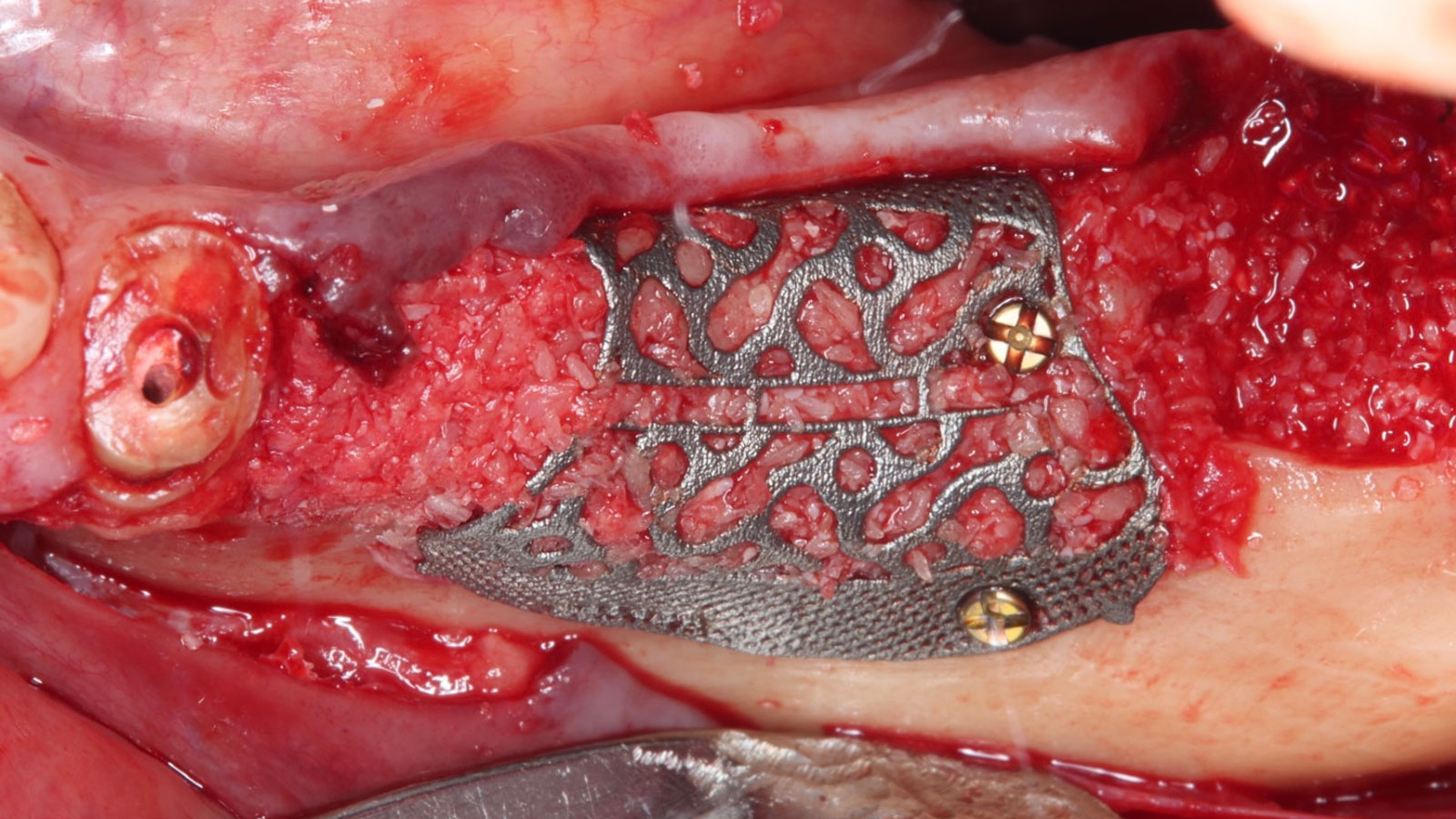
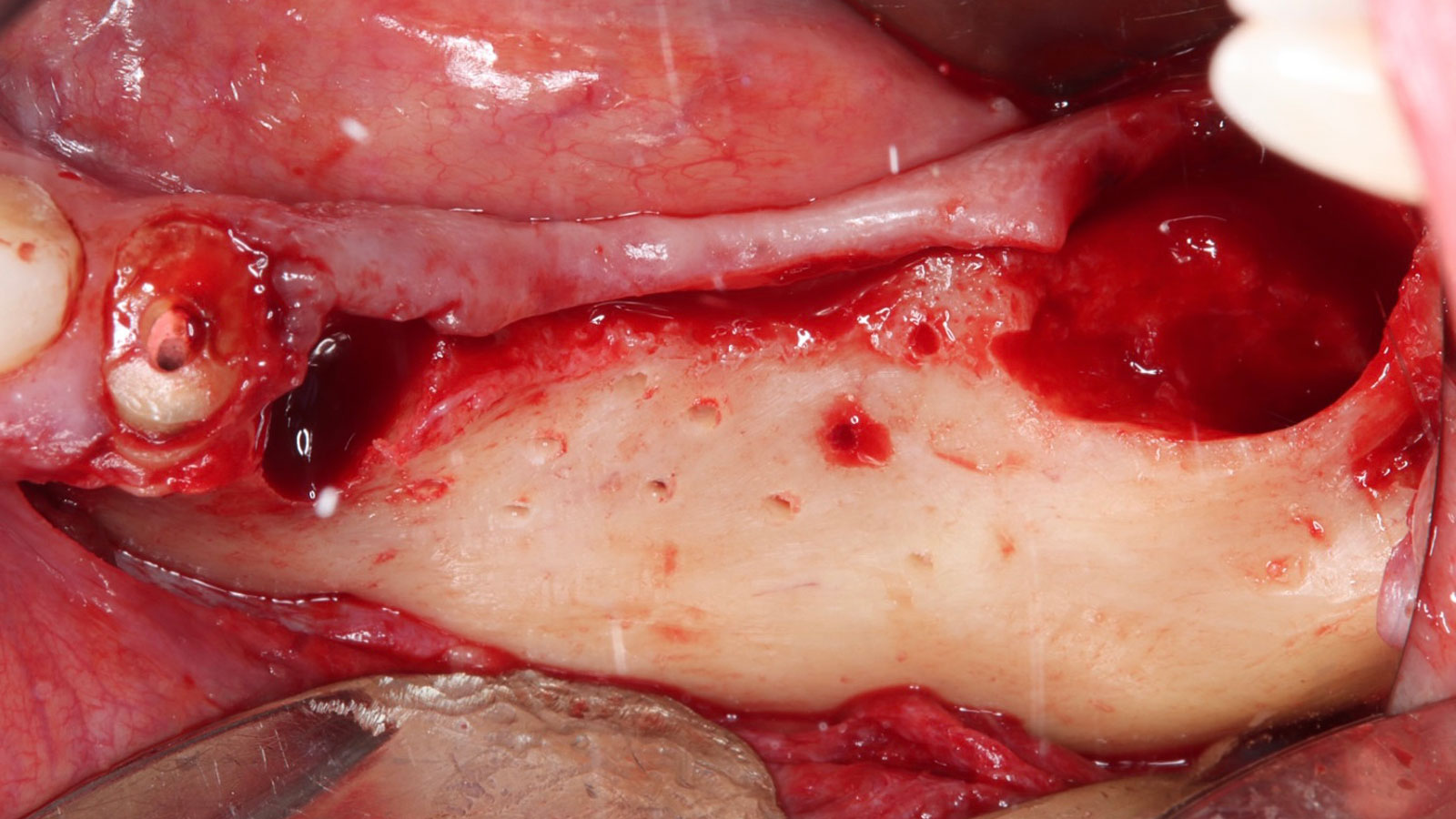
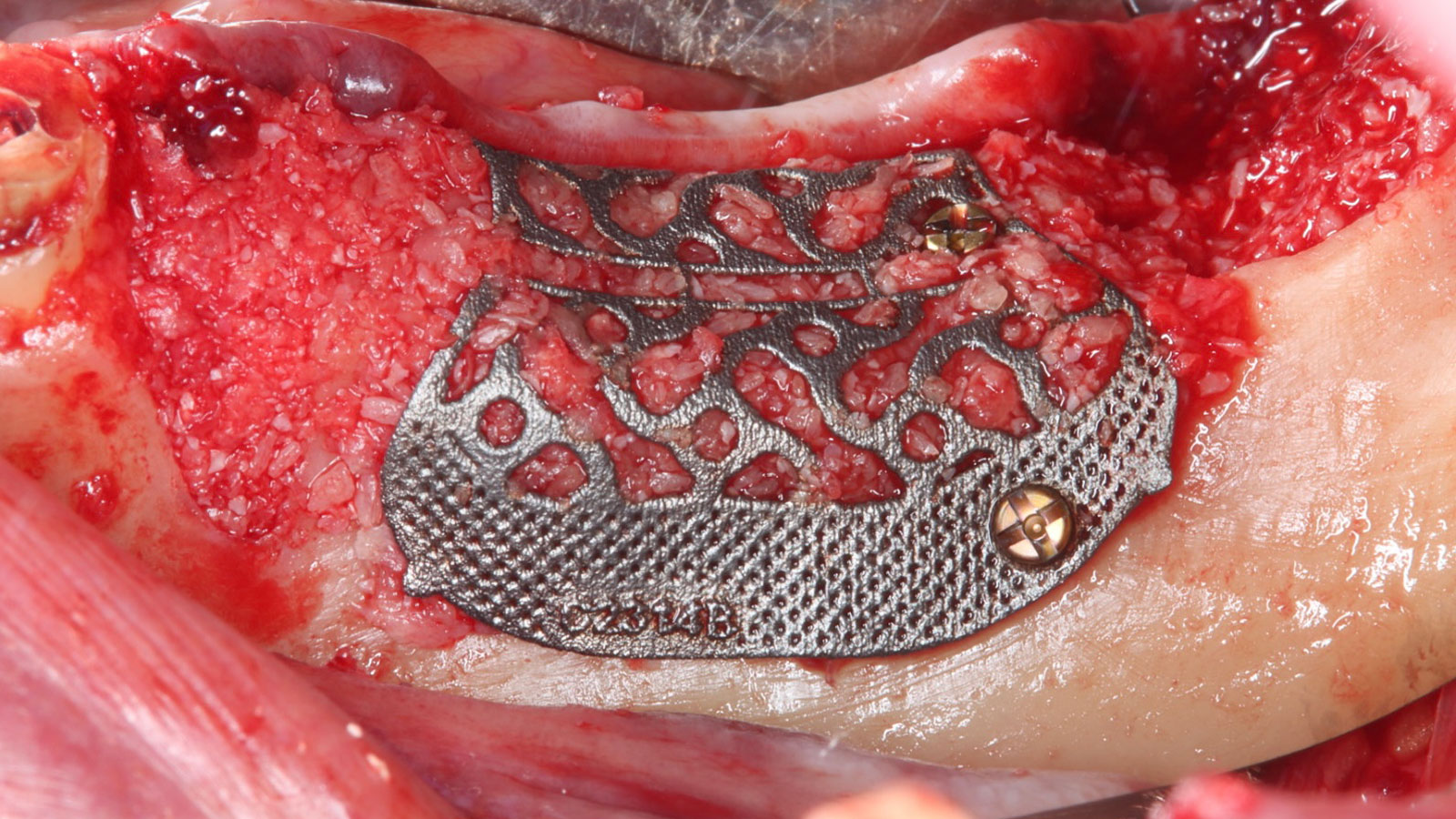
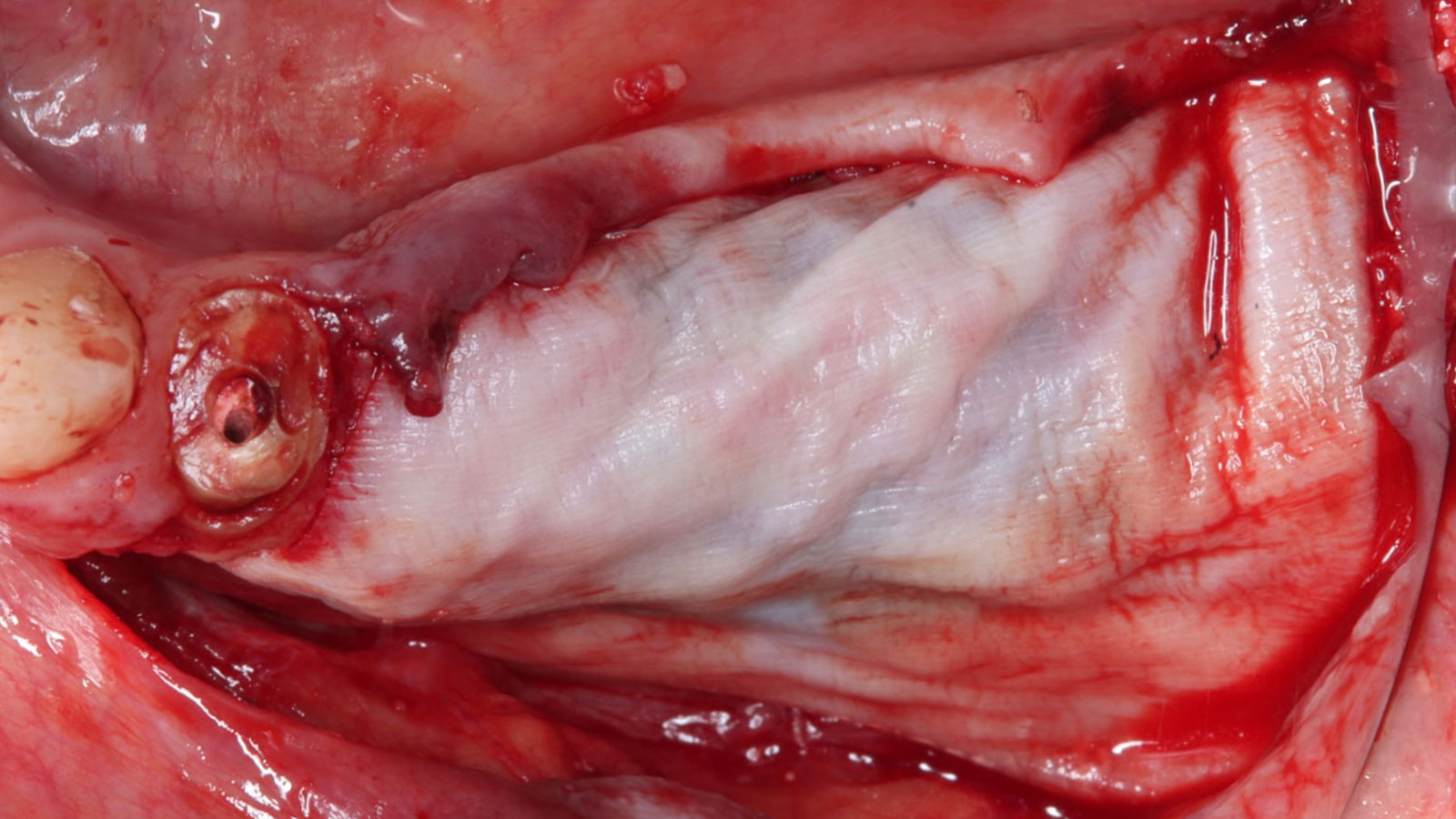
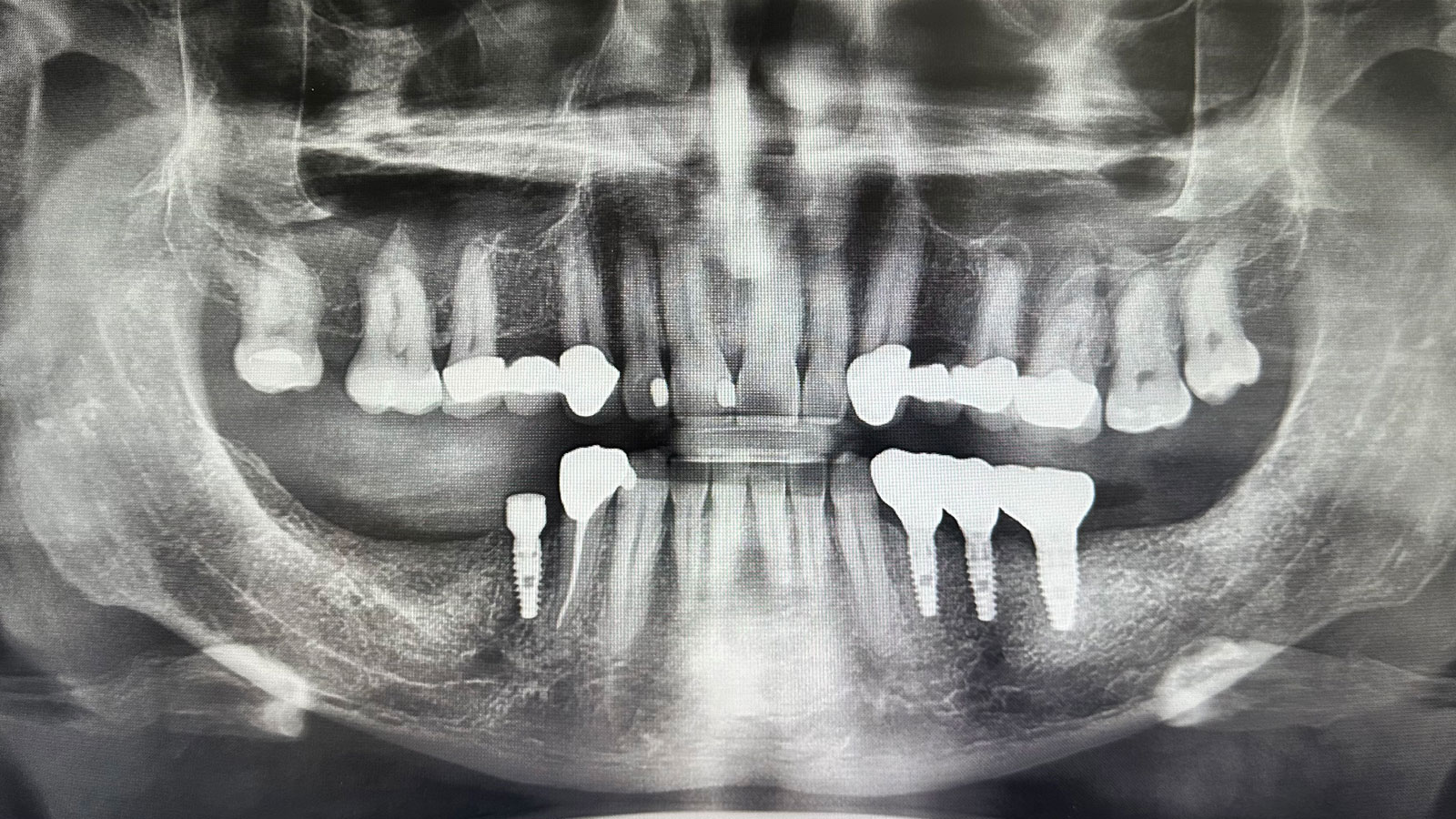
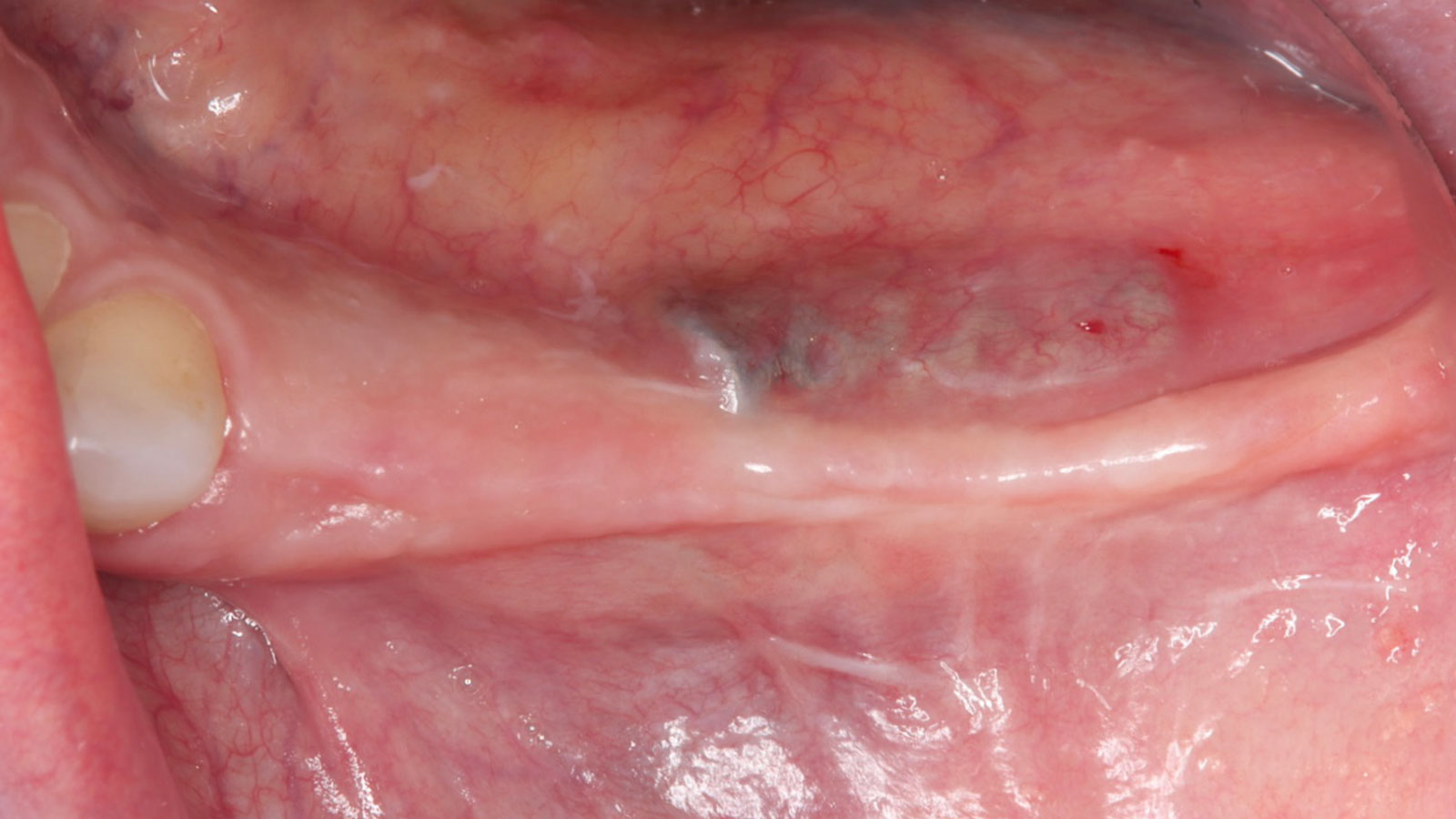
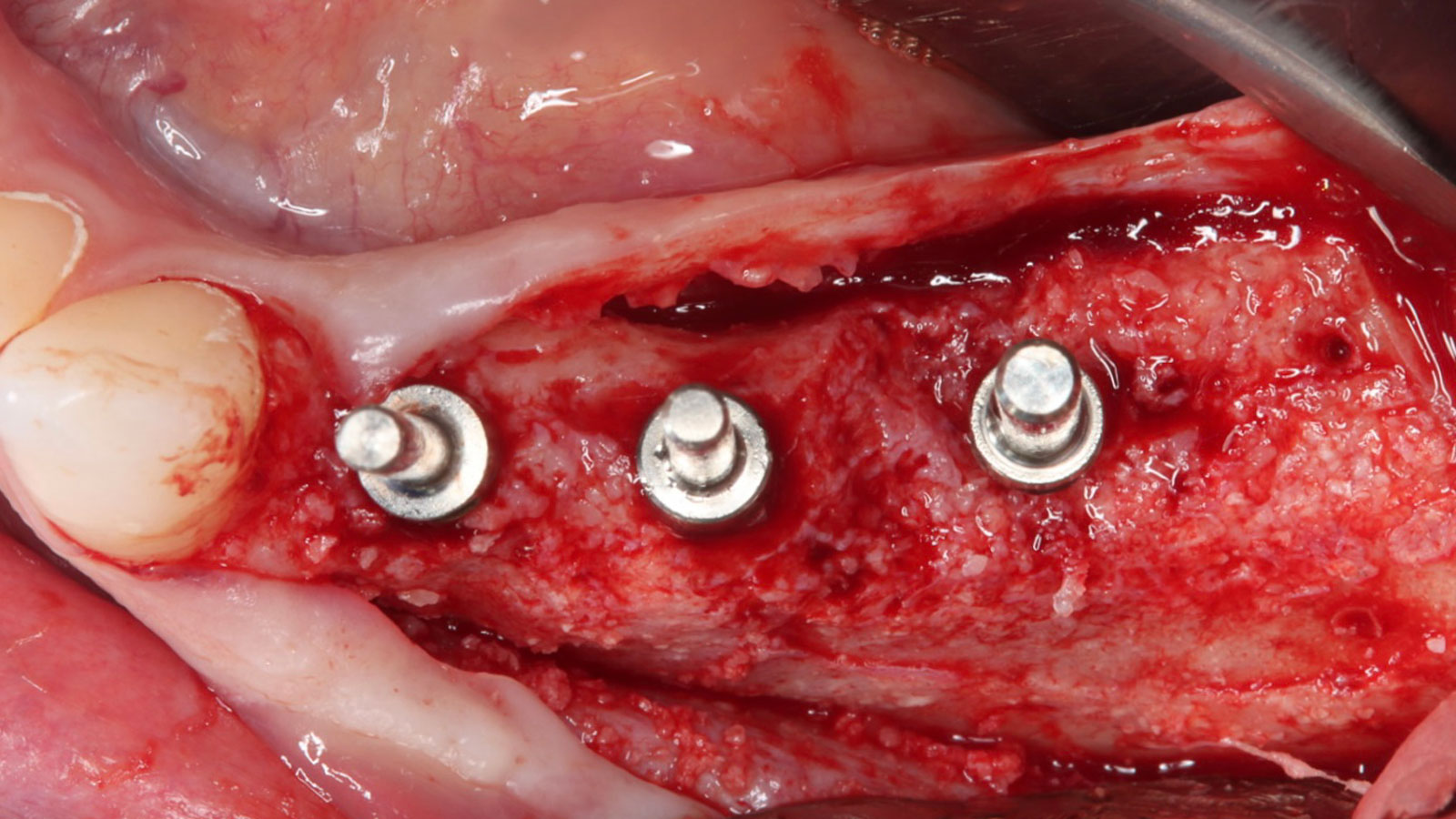
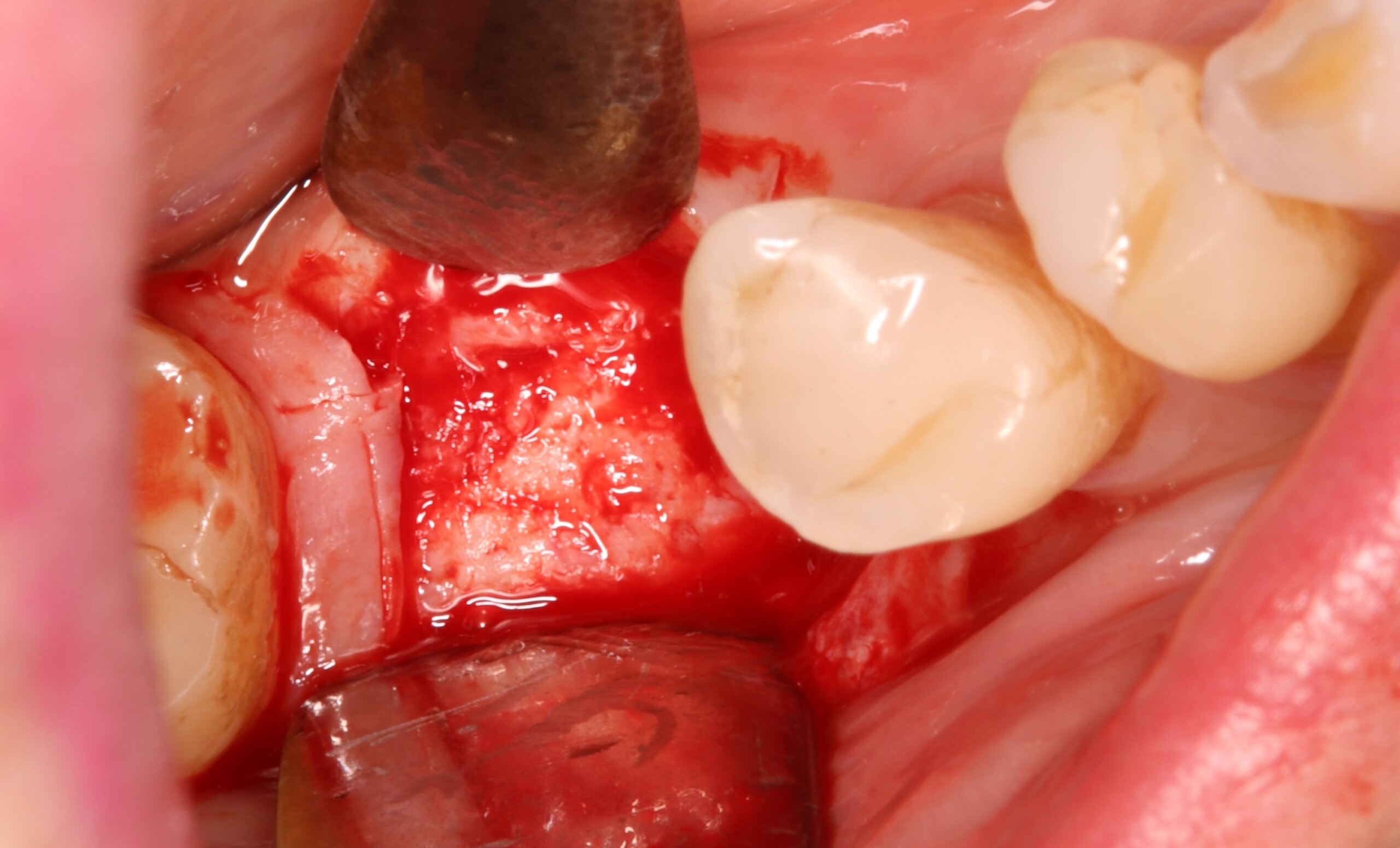
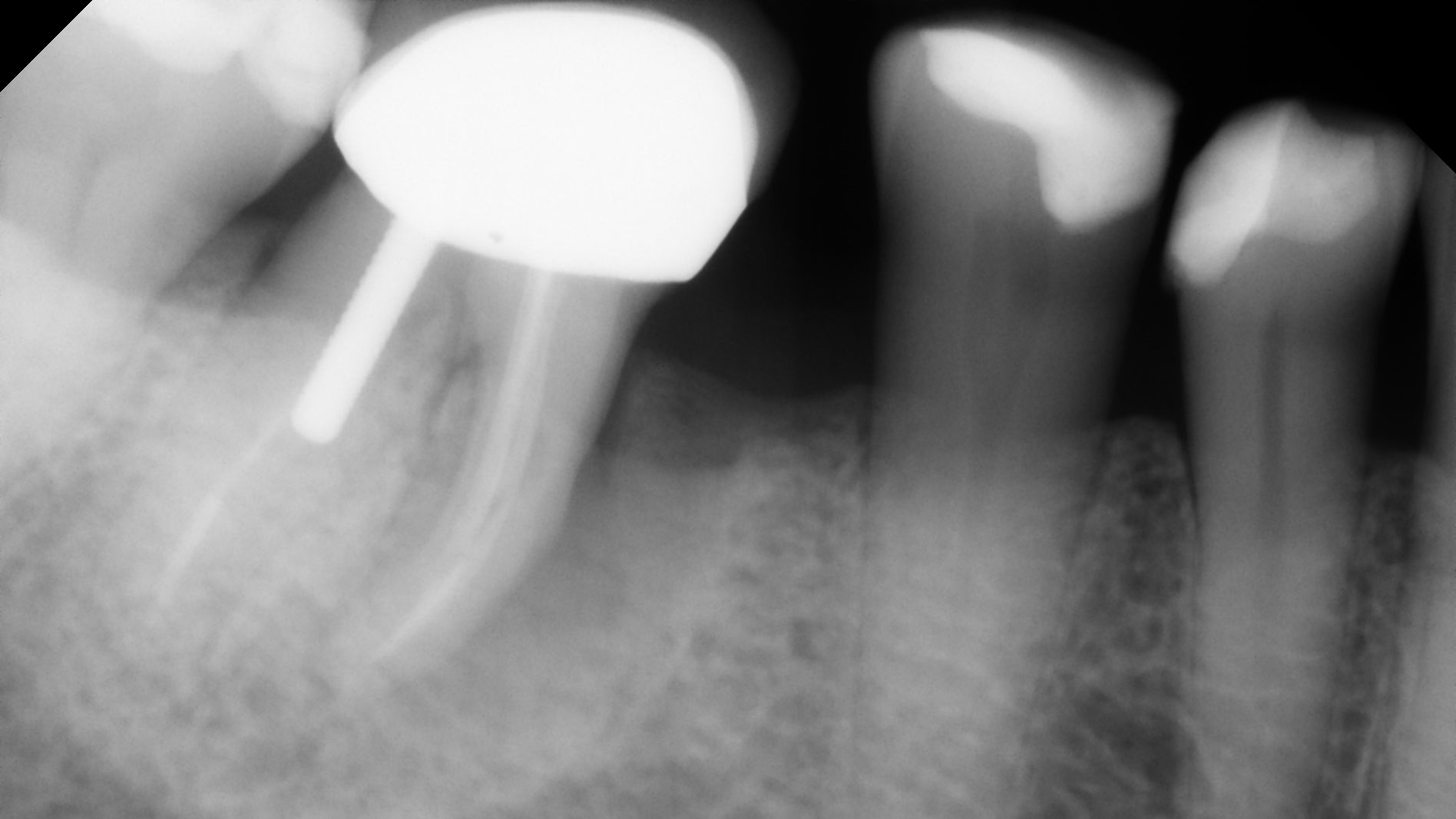
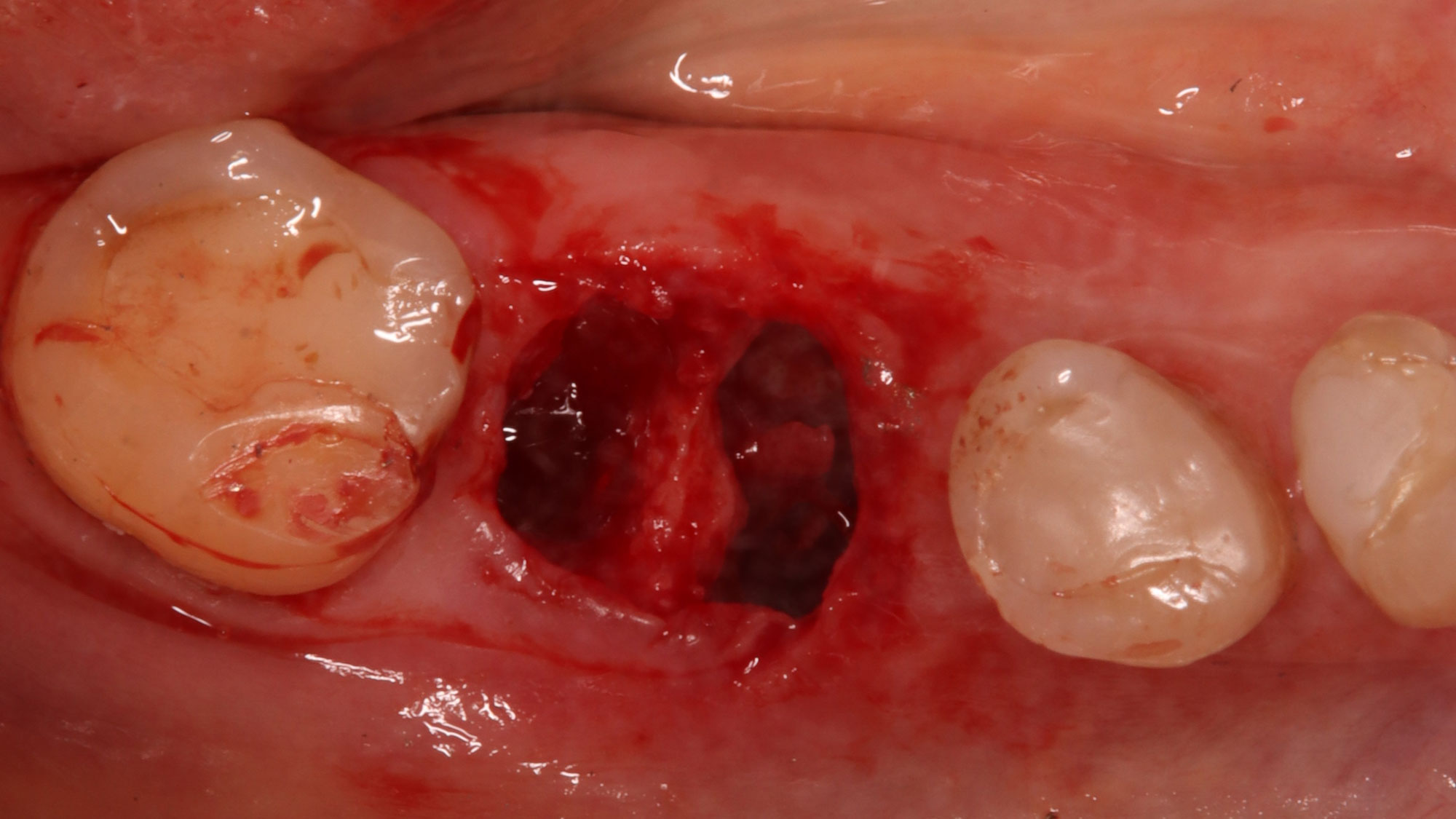
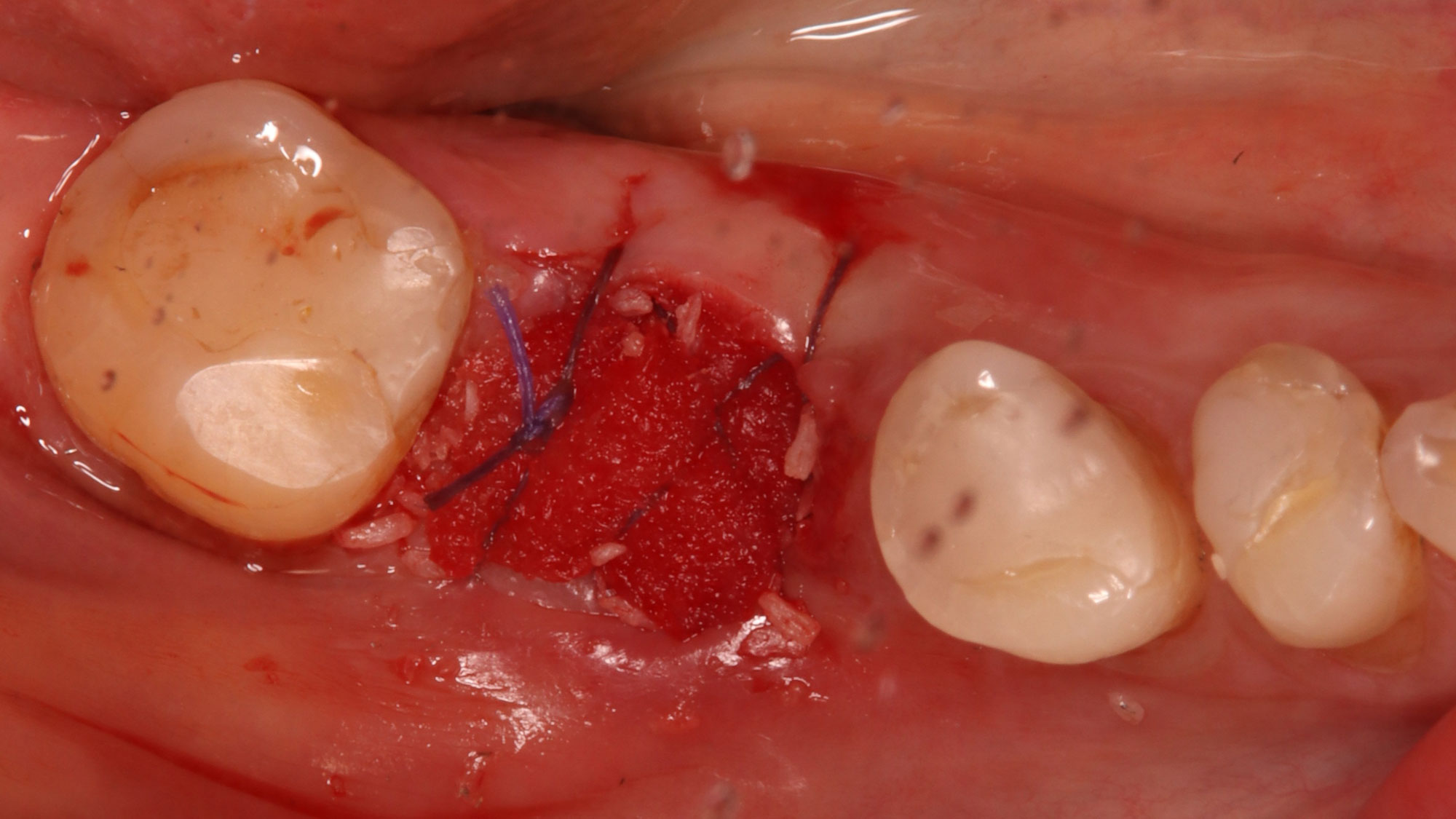
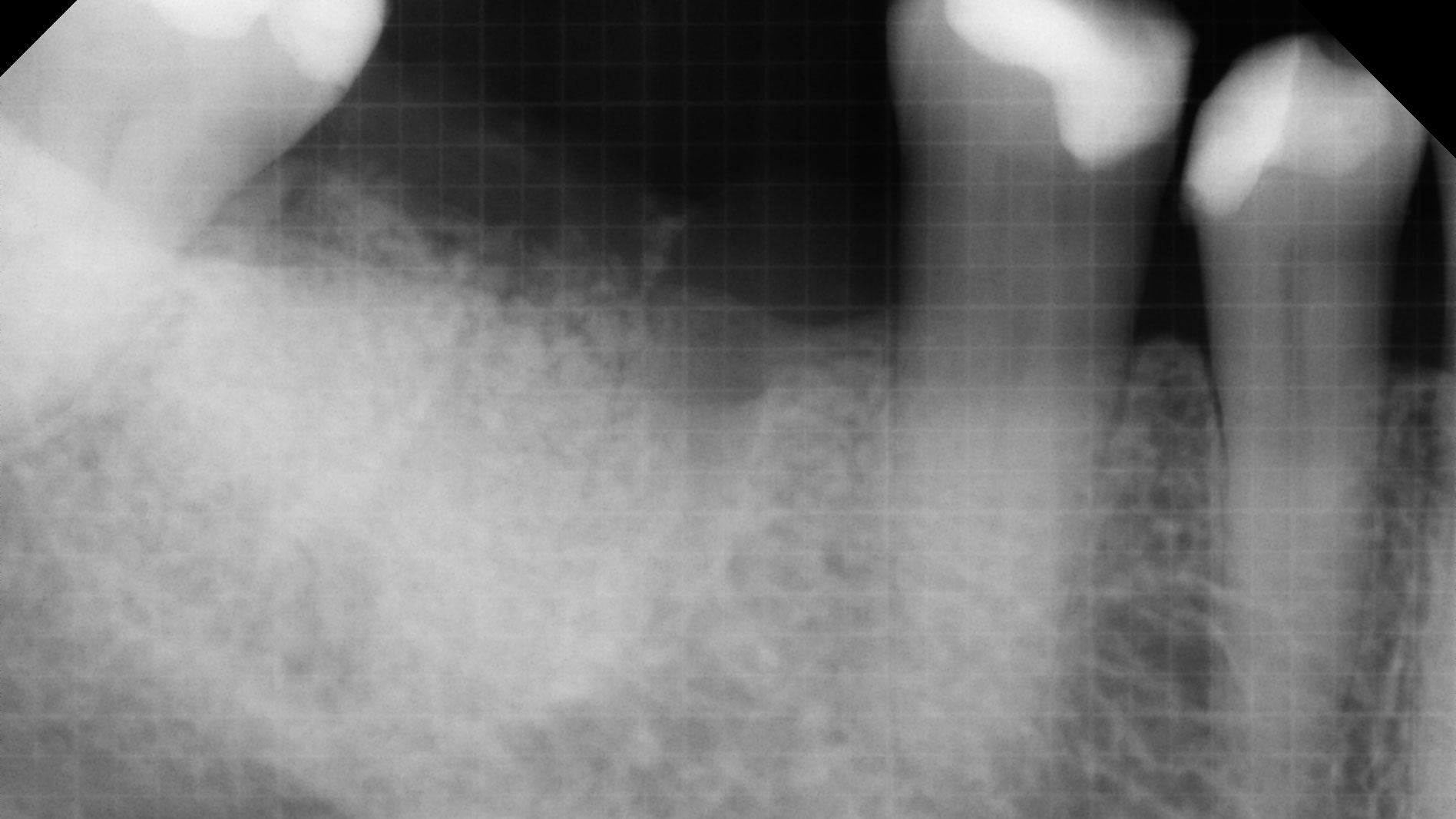
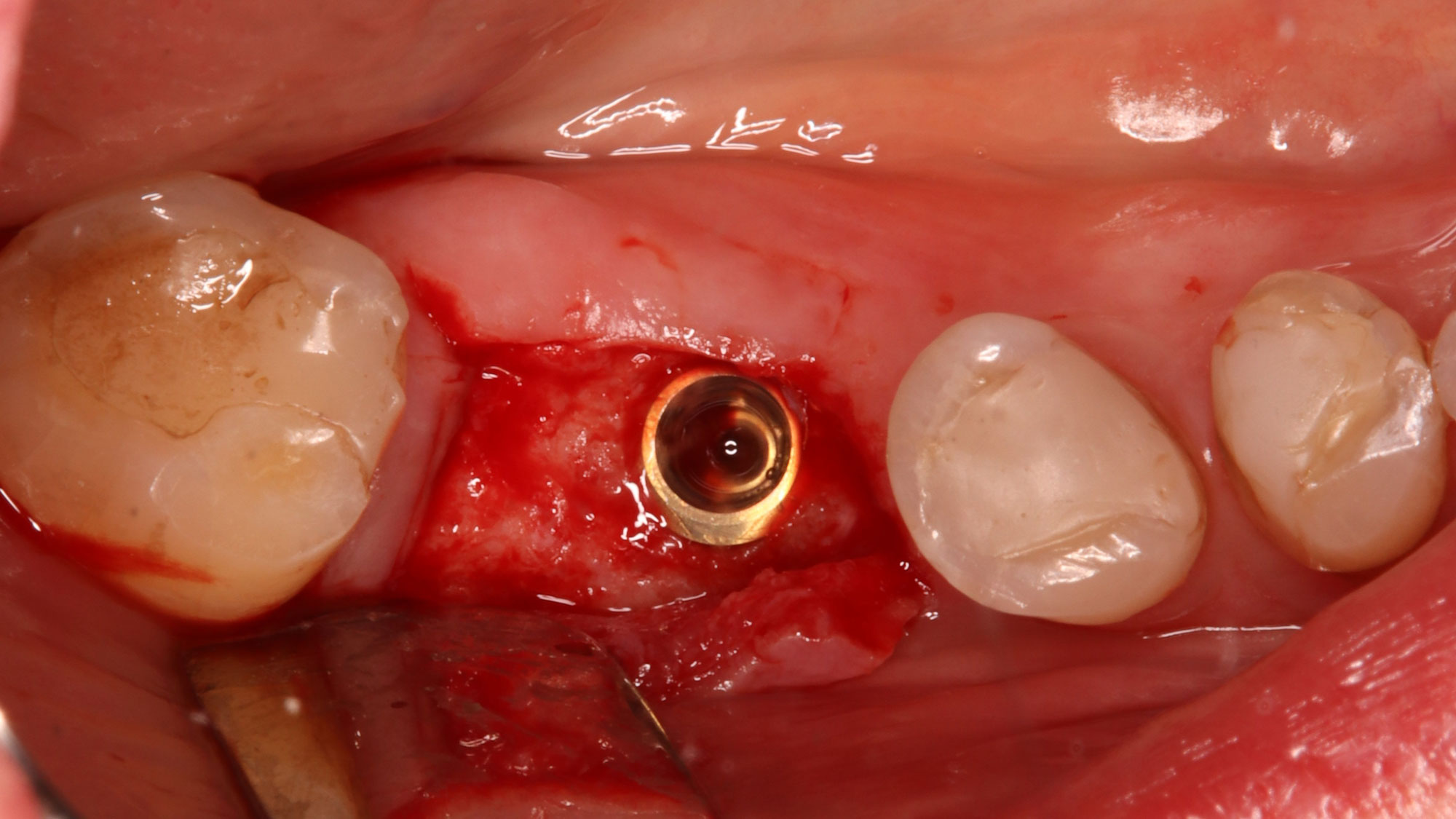
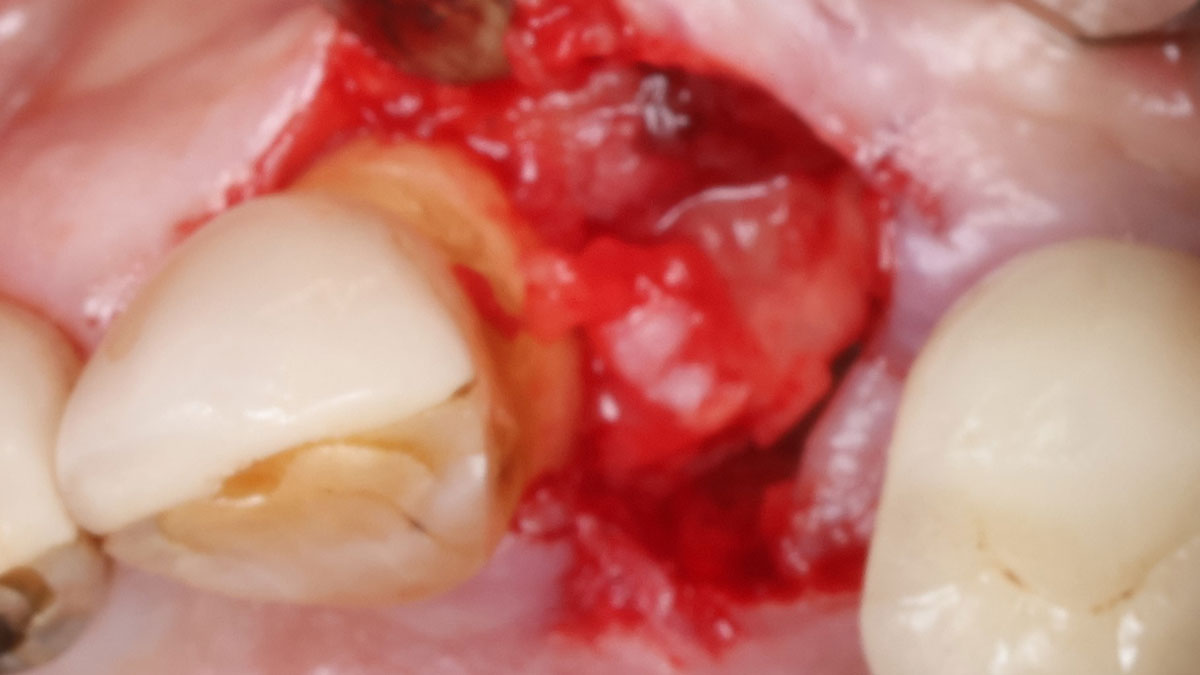
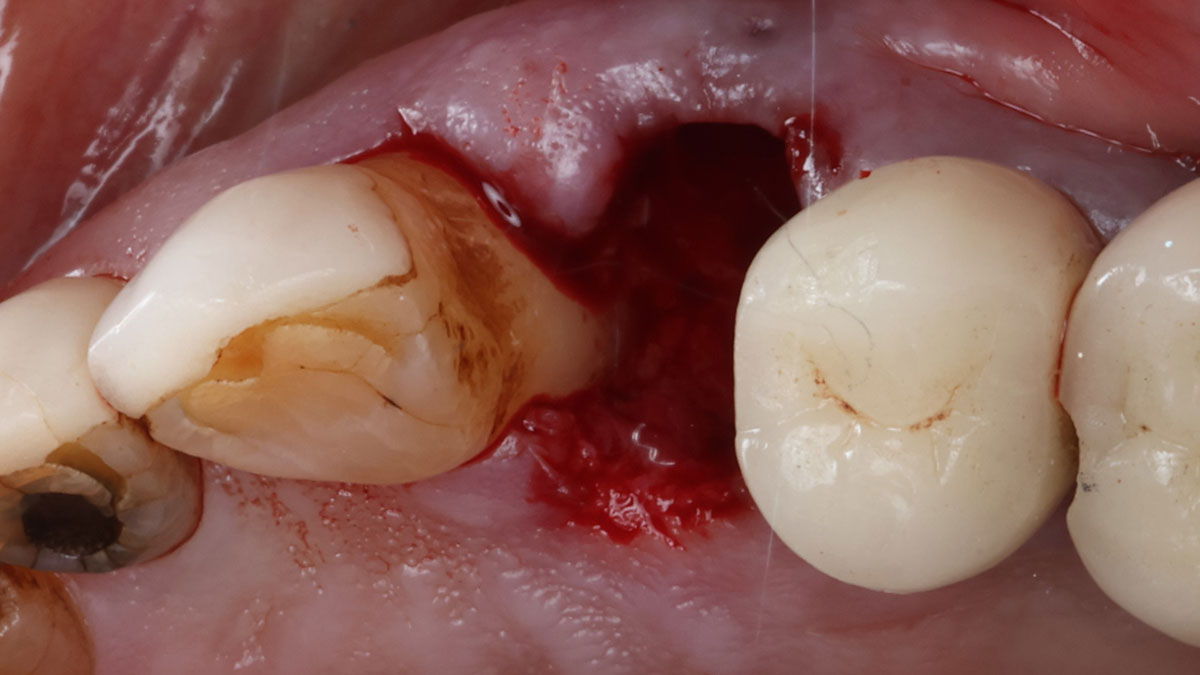
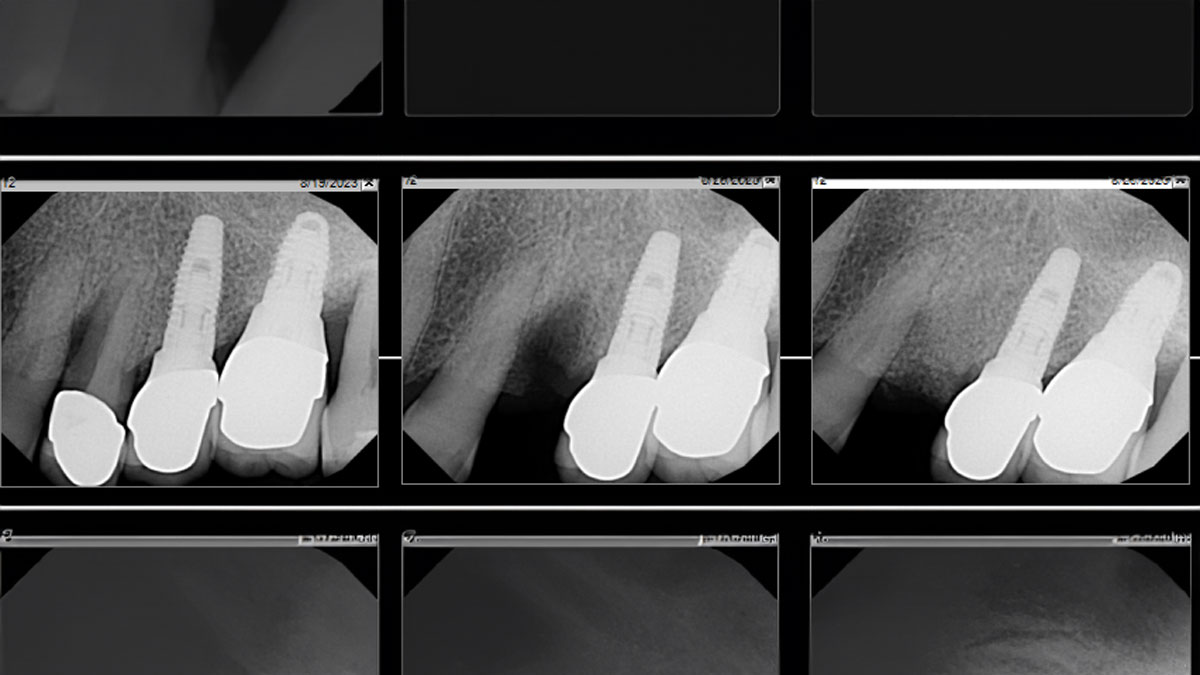
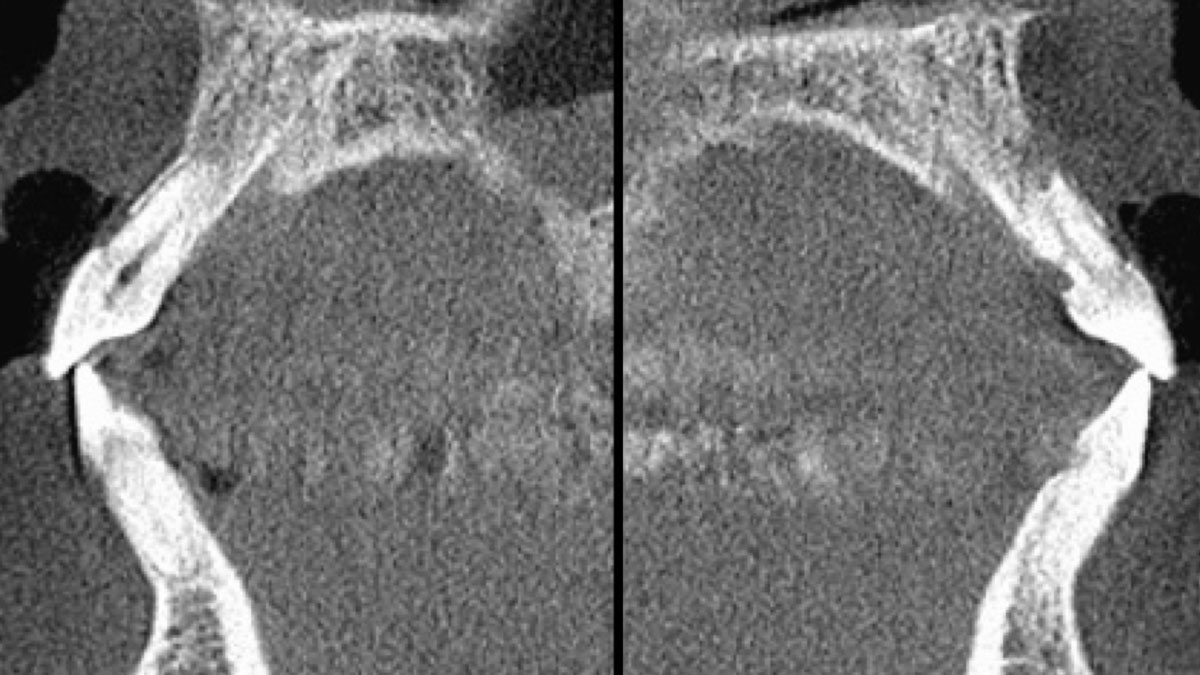
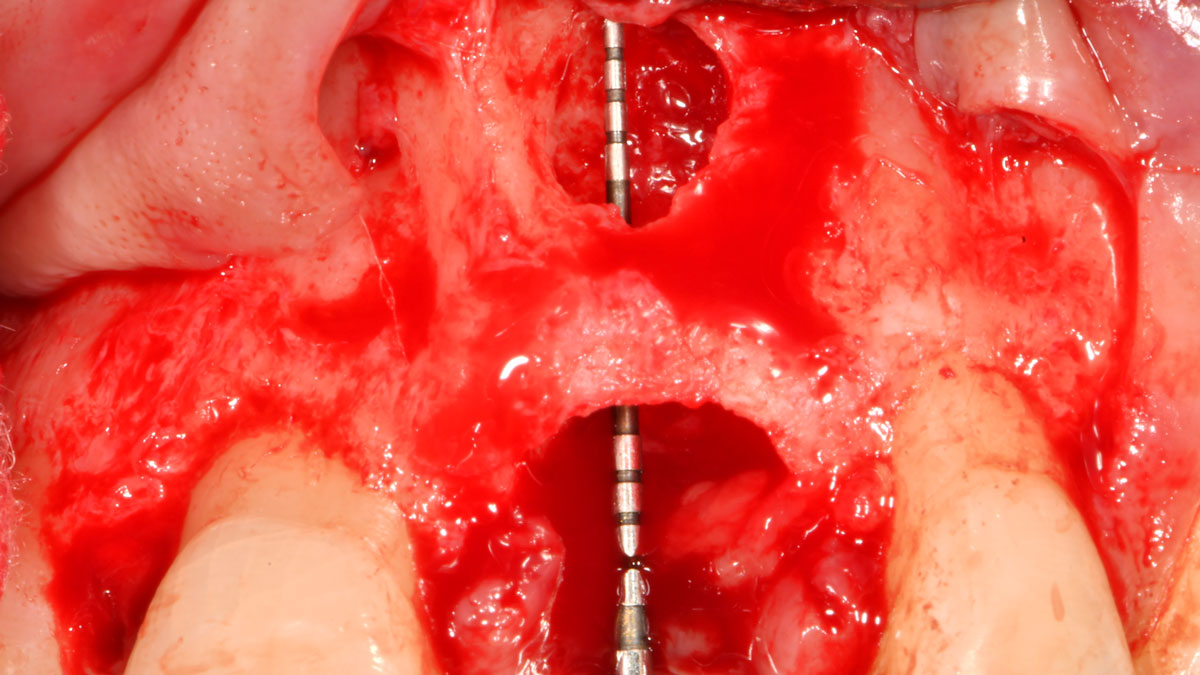
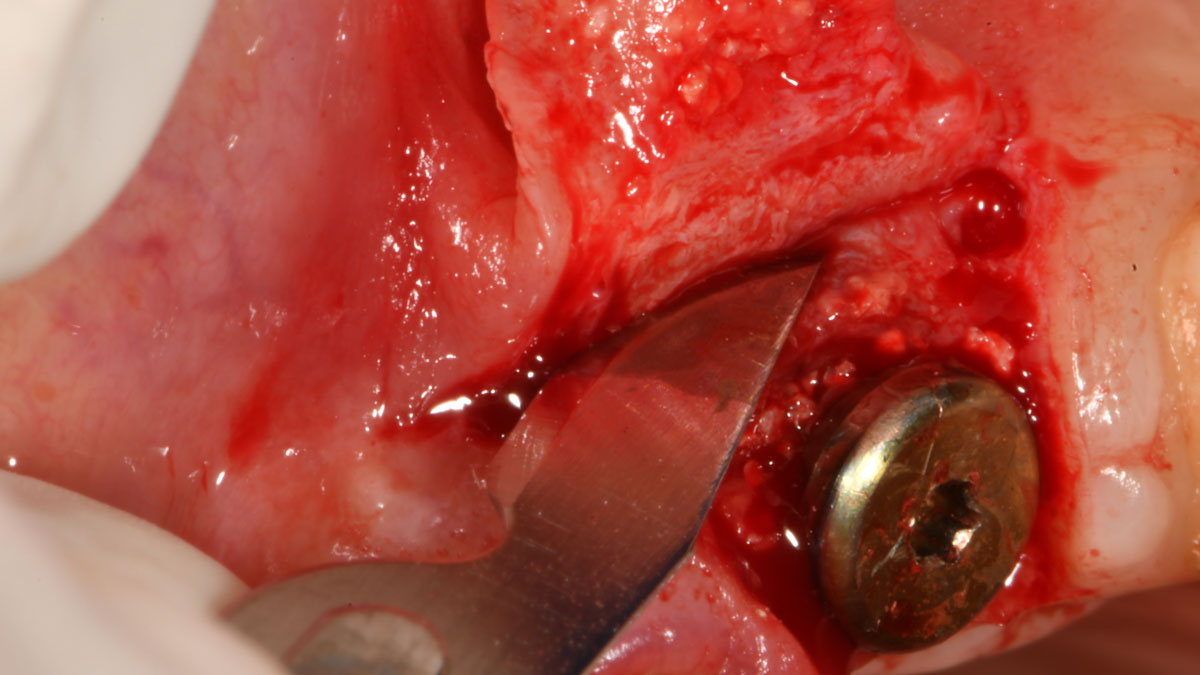
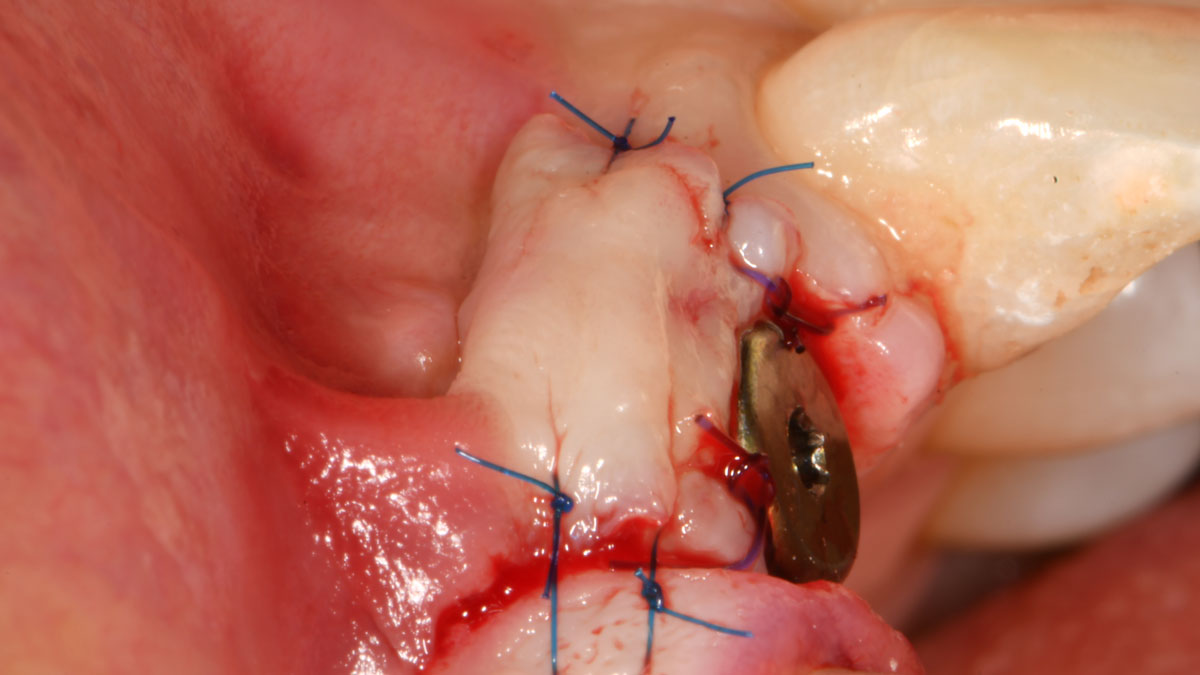
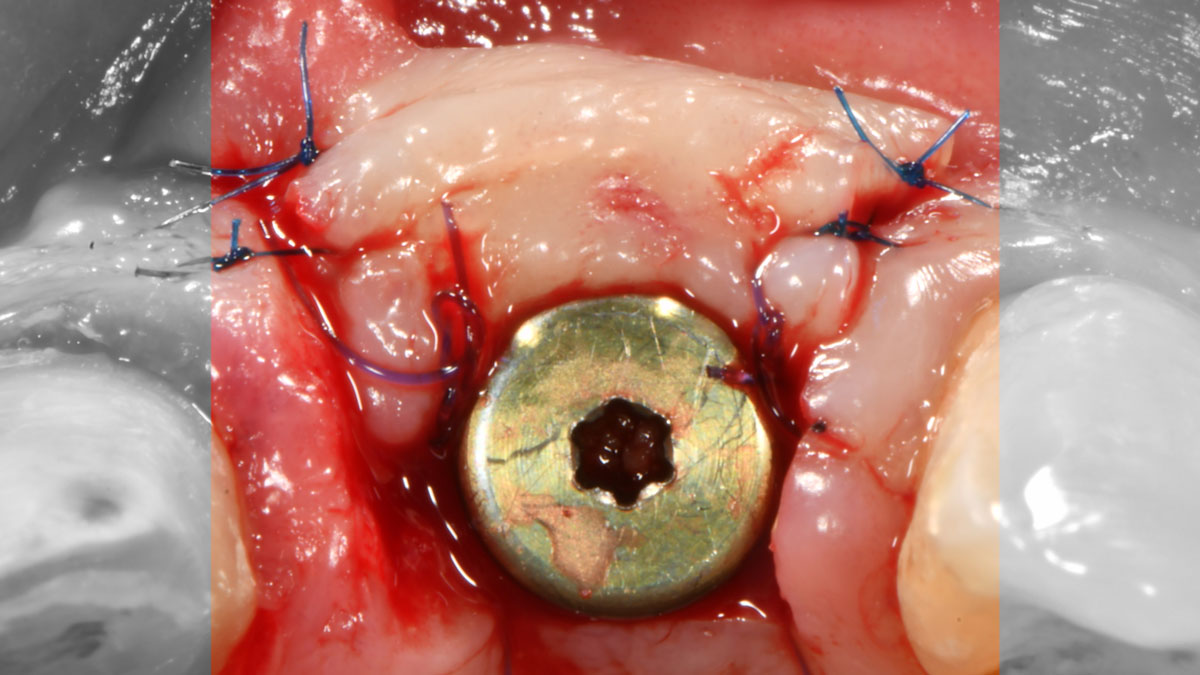
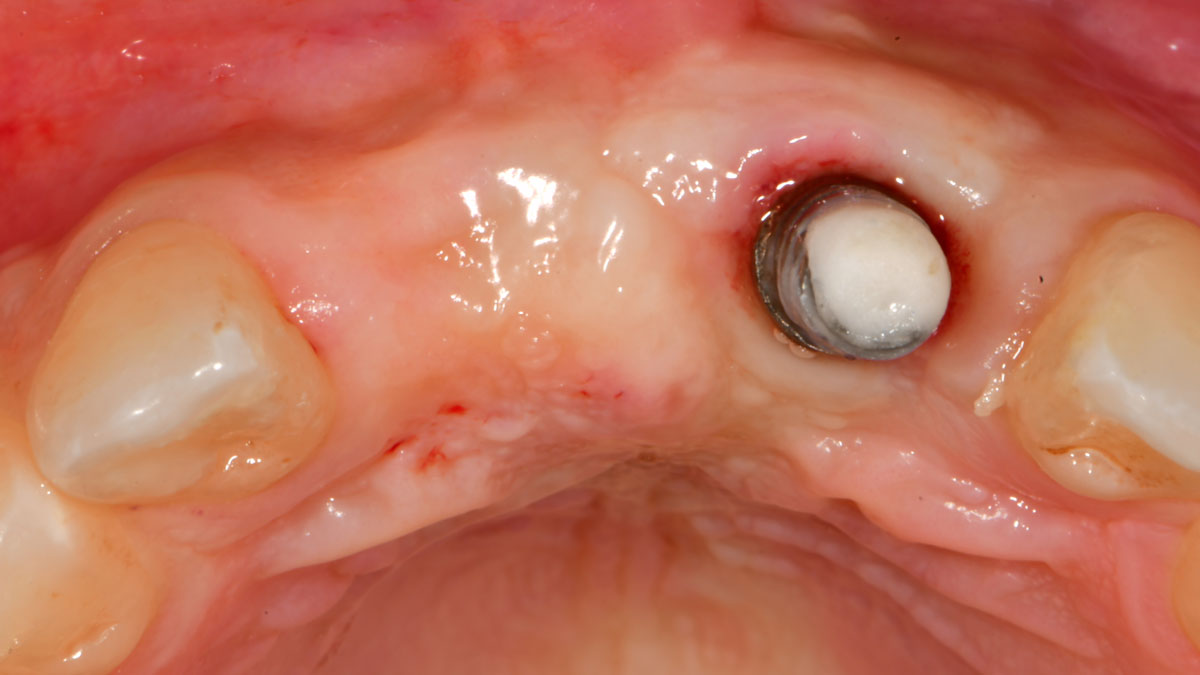
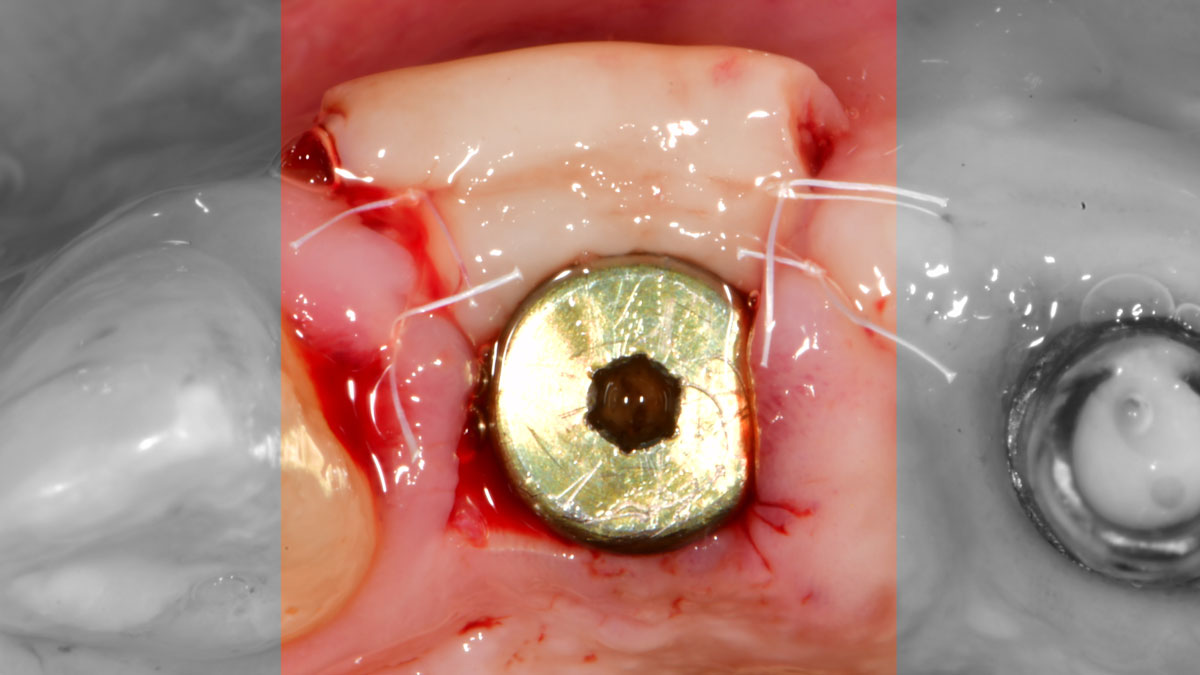
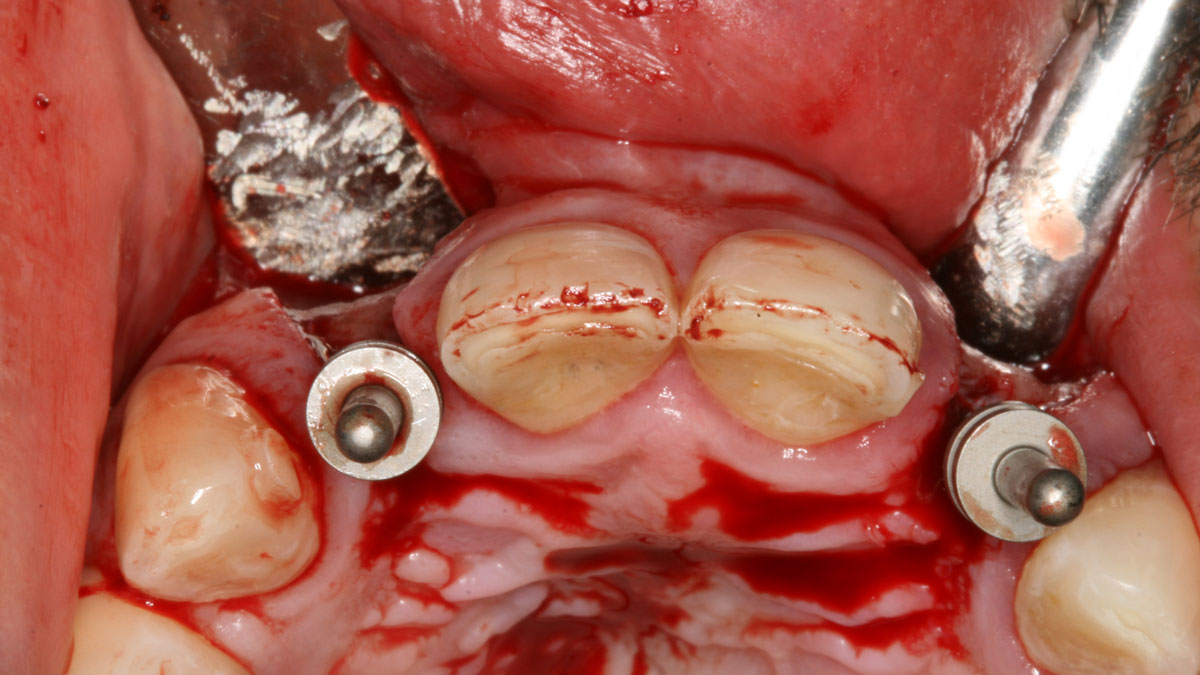
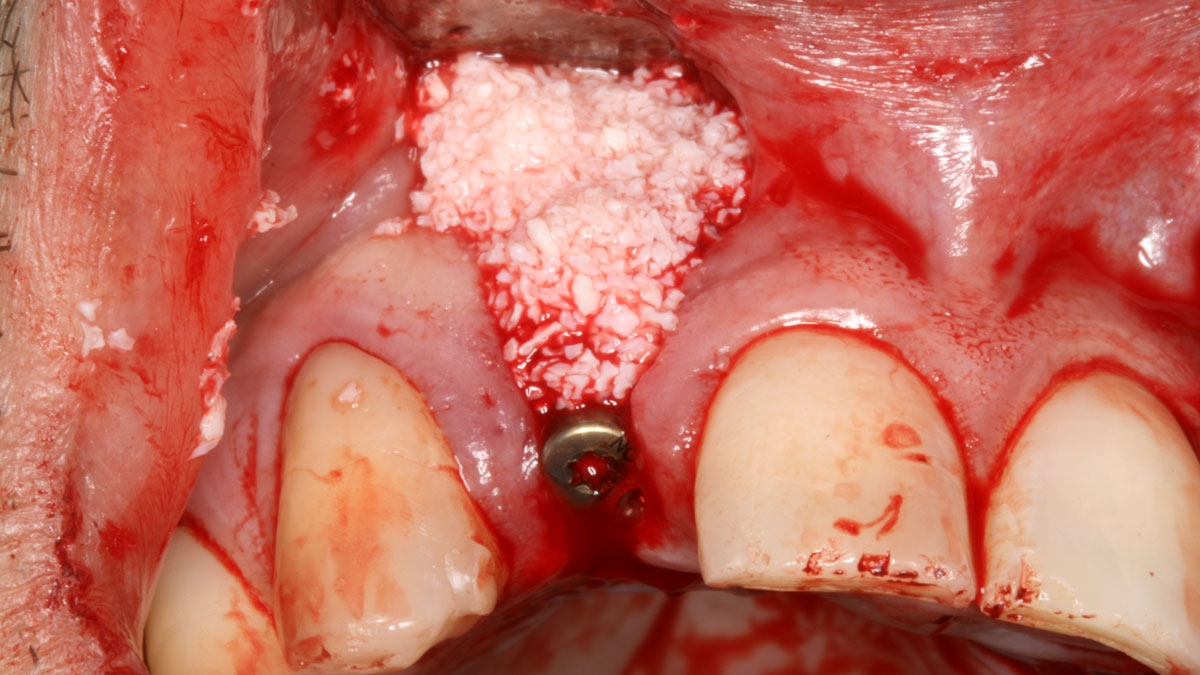
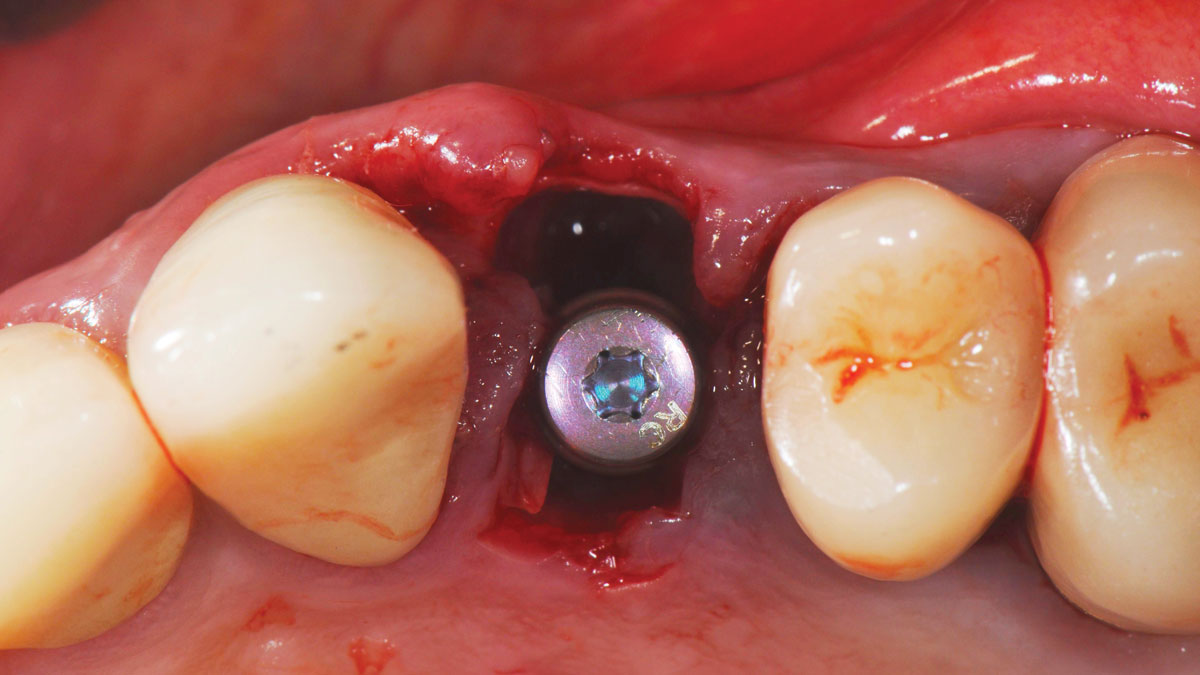
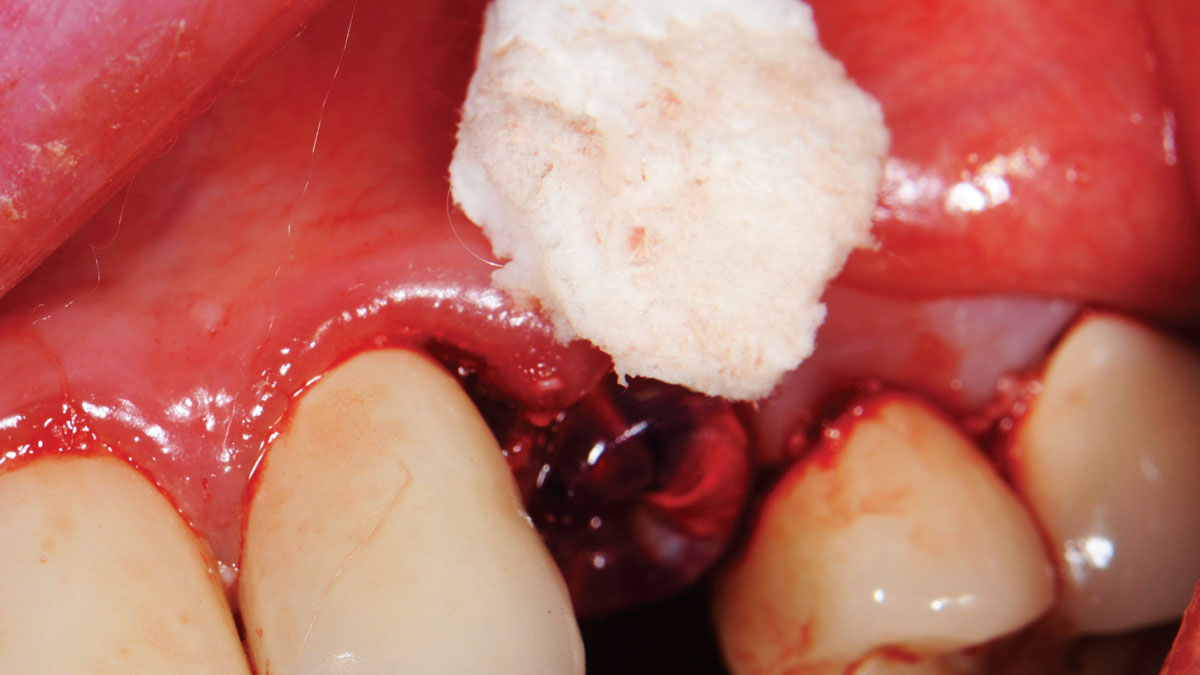
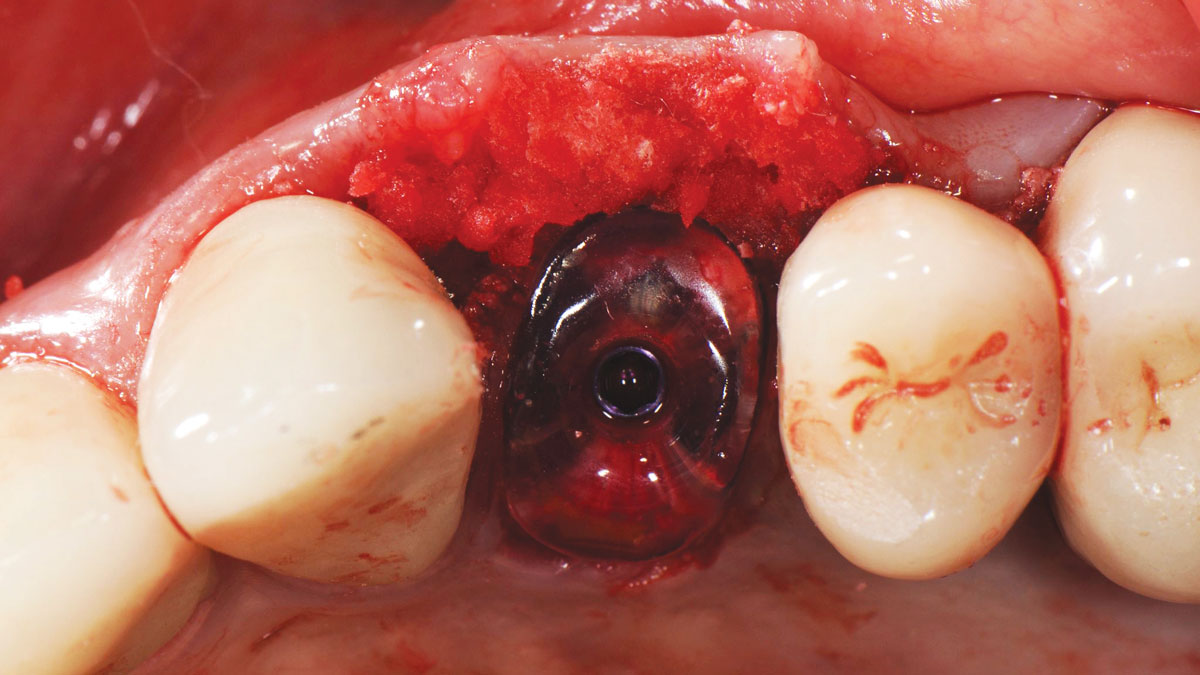
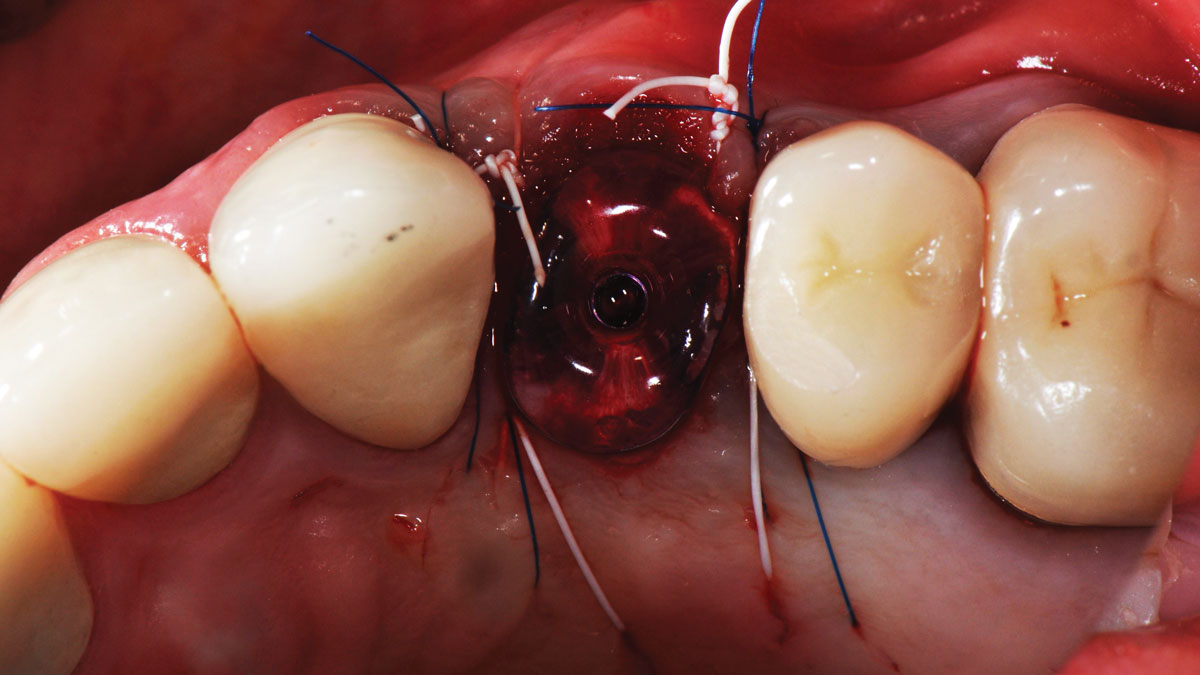
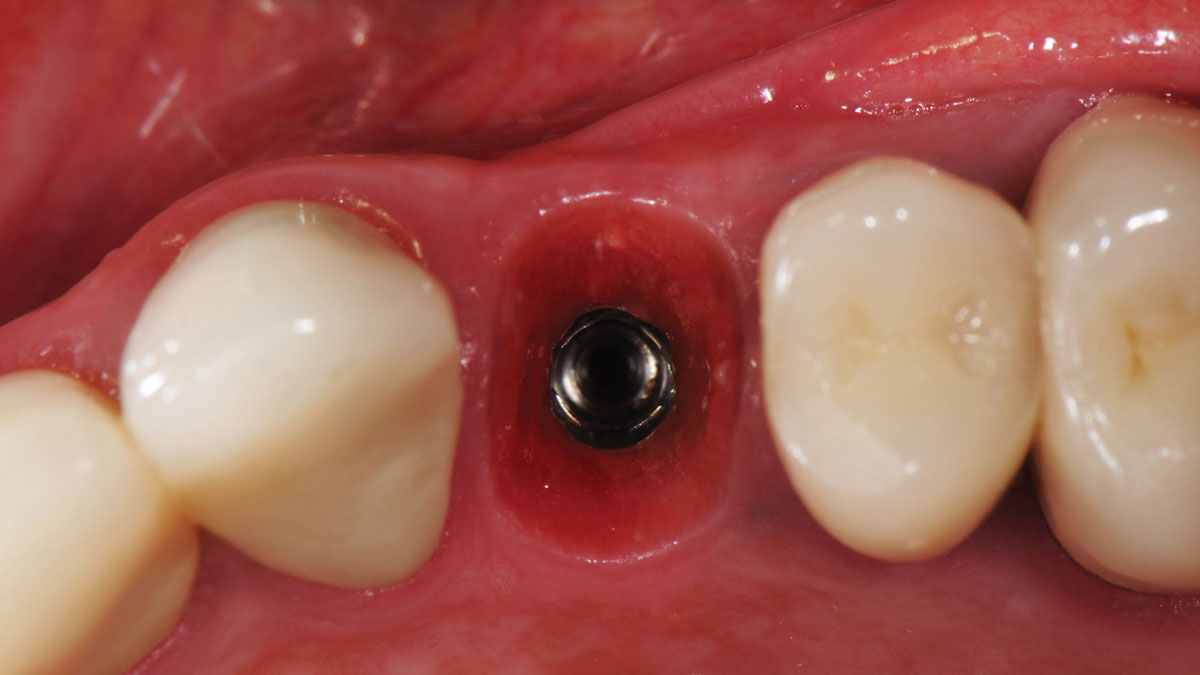
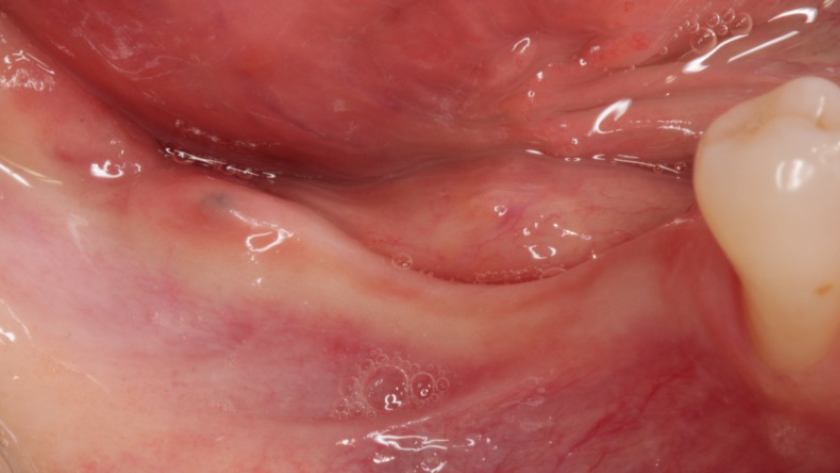
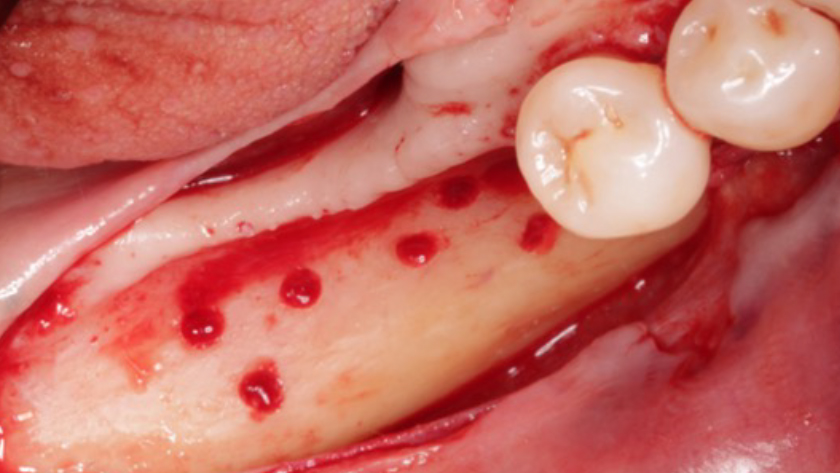
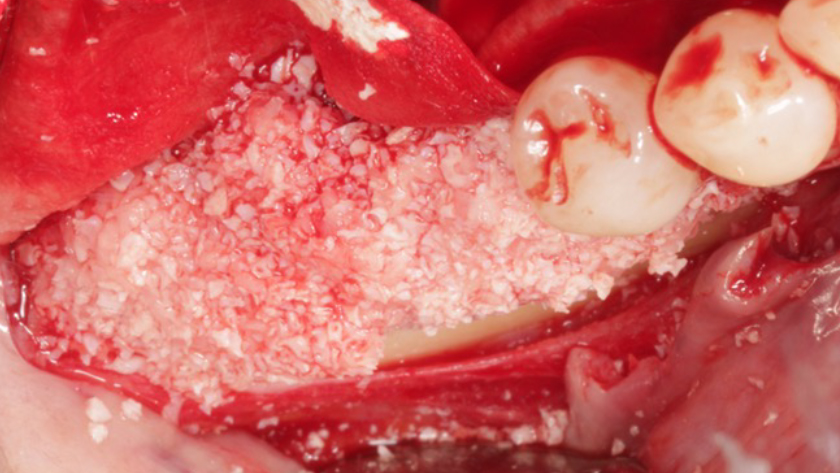
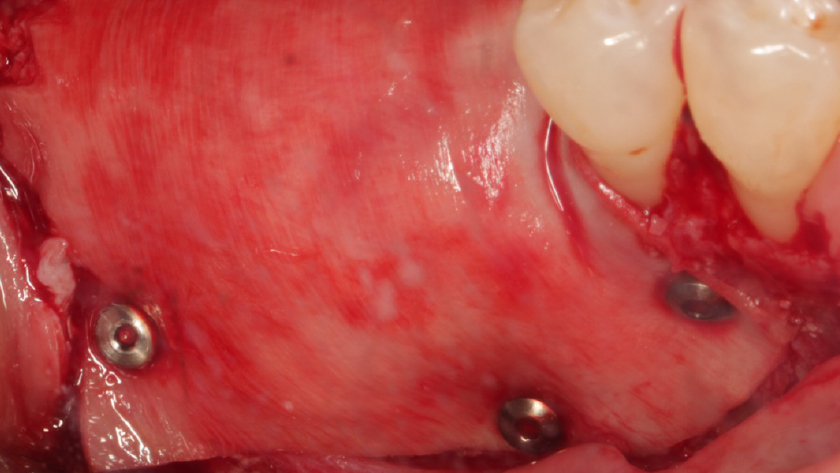
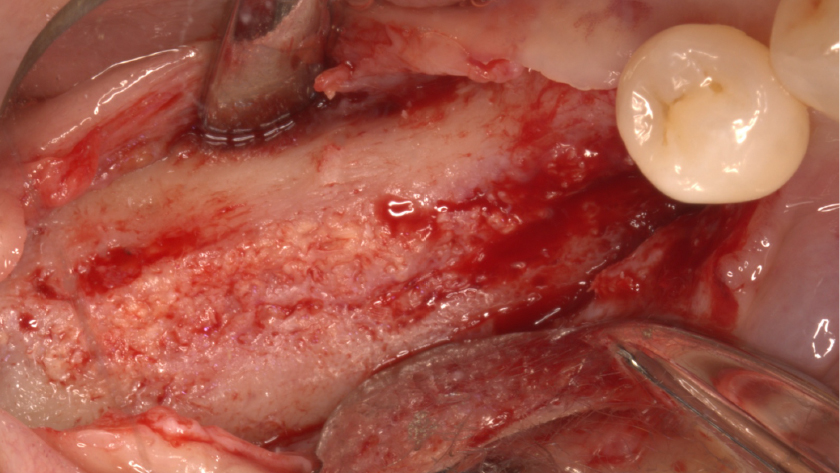
Teeth 30* and 31* had been previously extracted without alveolar ridge preservation. The site demonstrated approximately 1–2 mm of residual ridge width. The goal was to restore the site with implants.
*Universal Numbering System
Disclaimer: These results are not guaranteed; individual outcomes may vary depending on patient circumstances. This information is for informational purposes only and may not reflect Geistlich’s official position, opinion, or recommendation. Treatment decisions are made at the physician’s discretion, based on the unique needs of each patient.