






BIOBRIEF
Ramal Bone Graft for Congenitally Missing Maxillary Lateral Incisor

THE SITUATION
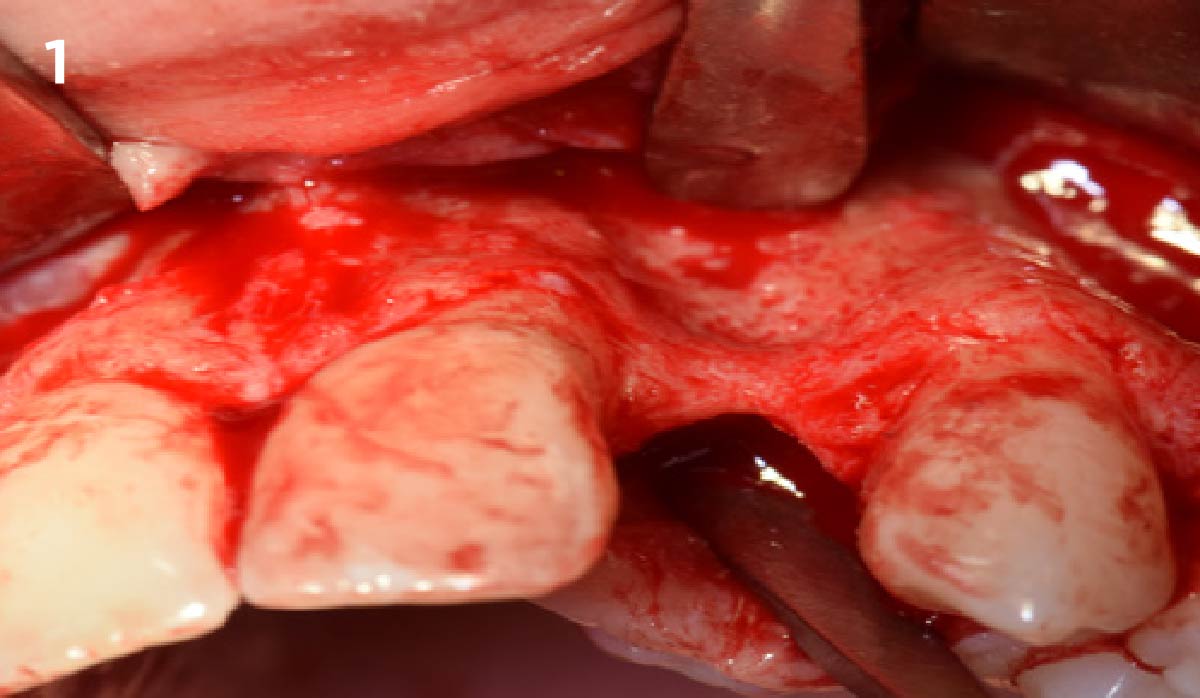
An 18-year-old female presented with a congenitally missing tooth #10. The patient previously sought care by another provider and had undergone guided bone regeneration with allograft and subsequent implant placement with additional grafting at the time of implant placement. The implant ultimately failed and was removed prior to my initial consultation. An examination revealed maximal incisal opening, within normal limits, missing #10 with 6 mm ridge width. In addition there was a significant palpable cleft-like depression on the facial aspect of the ridge, adequate attached tissue but reduced vertical height in relation to adjacent dentition and attached tissue. Previous surgeries resulted in extensive fibrous tissue with scarring at site #10. Plan: A ramal bone graft is indicated at the congenitally missing site #10 with Geistlich Bio-Oss® and Geistlich Mucograft® matrix utilized for ridge augmentation prior to secondary implant placement.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system Non-smoker | Light smoker | Impaired immune system |
| Patient’s esthetic requirements | Low | Medium | High |
| Height of smile line | Low | Medium | High |
| Gingival biotype | Thick – “low scalloped” | Medium – “medium scalloped” | Thin – “high scalloped” |
| Shape of dental crowns | Rectangular | Triangular | |
| Infection at implant sight | None | Chronic | Acute |
| Bone height at adjacent tooth site | ≤ 5 mm from contact point | 5.5 – 6.5 mm from contact point | ≥ 7 mm from contact point |
| Restorative status of adjacent tooth | Intact | Restored | |
| Width of tooth gap | 1 tooth (≥ 7 mm) | 1 tooth (≤ 7 mm) | 2 teeth or more |
| Soft-tissue anatomy | Intact | Compromised | |
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
THE APPROACH
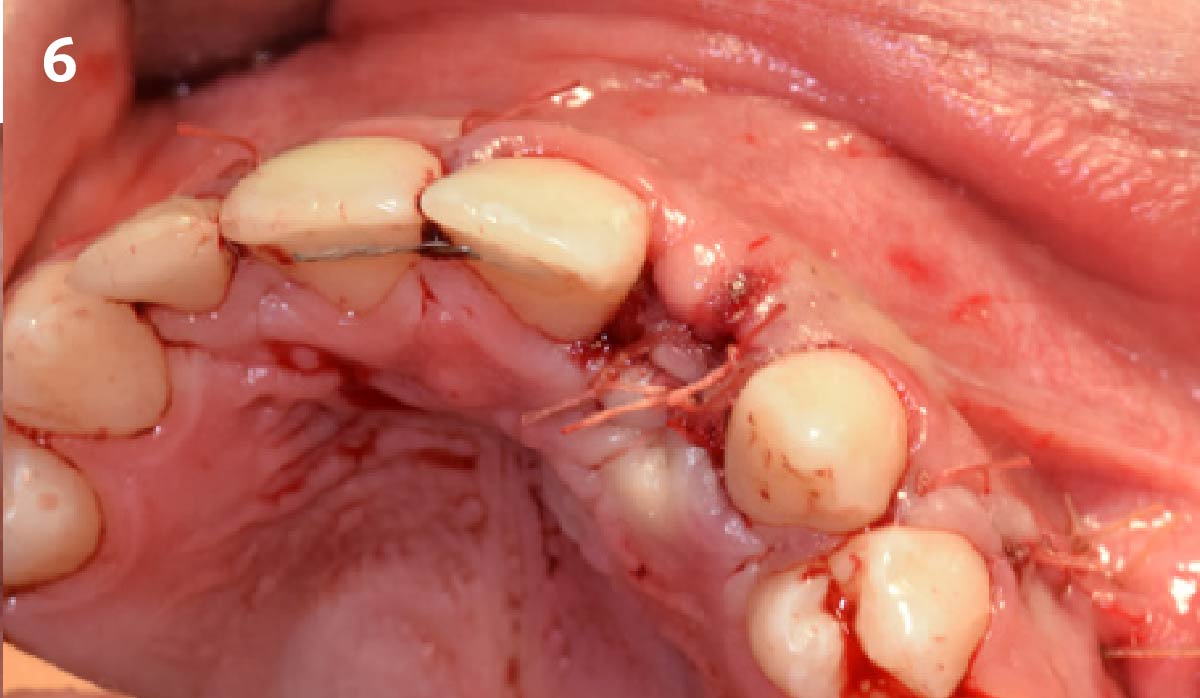
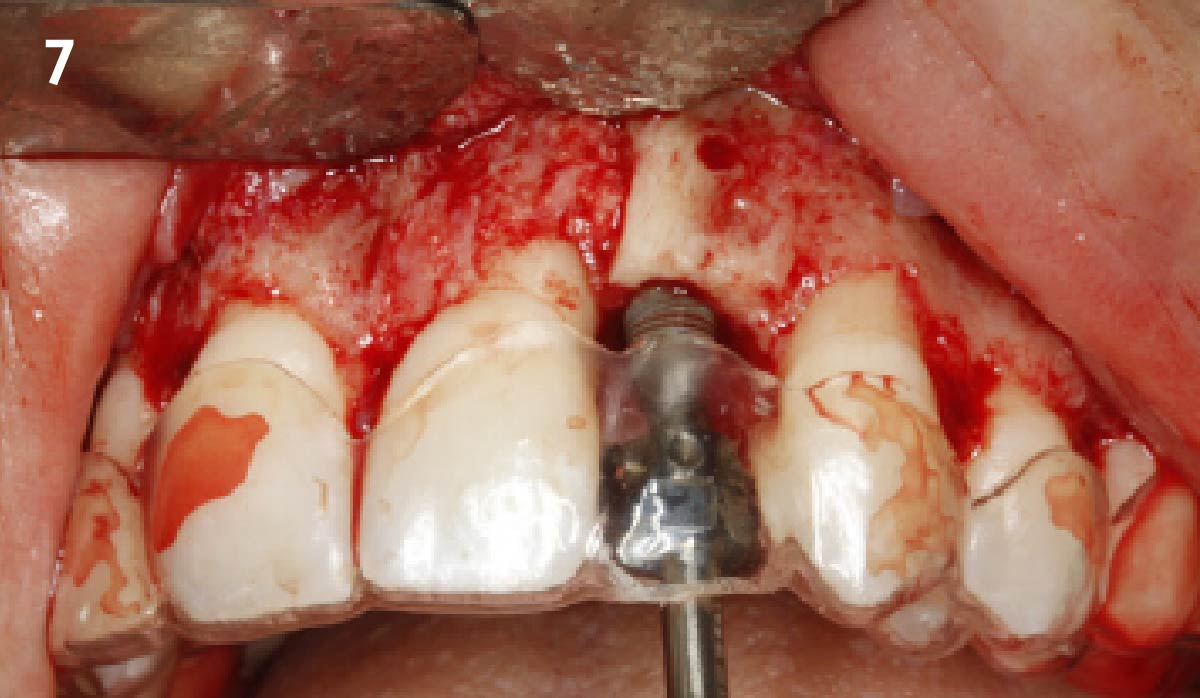
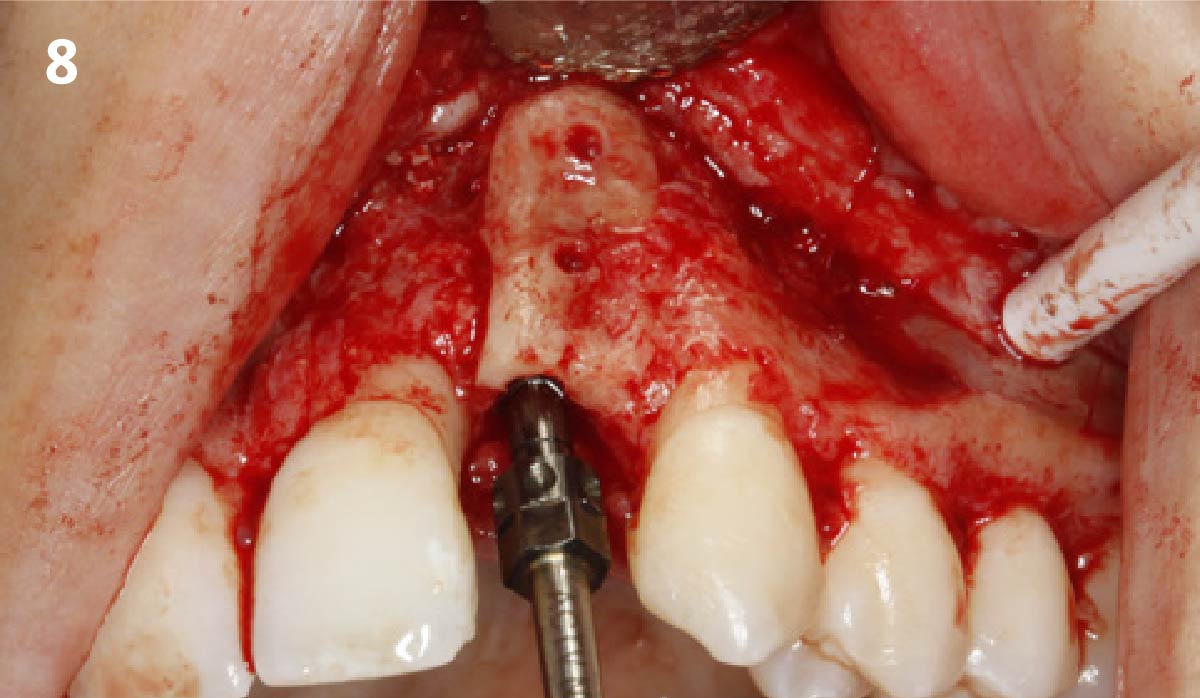
The goals for this patient are to reconstruct the osseous foundation and provide a matrix for improvement with the overlying soft tissue. Specifically, a coordinated multidisciplinary plan was established with the restoring dentist, periodontist and oral surgeon. A plan for idealized anterior cosmetic prosthetic restoration was established. Sequencing of treatment was established. Surgical phase one included a ramal bone graft to site #10 and Essix type temporary prosthesis for immediate post-operative phase followed by a temporary Maryland bridge. Surgical phase two included implant placement and simultaneous crown lengthening and osteoplasty. This stage was done with immediate provisionalization.



“This is a young patient with a congenitally missing incisor that has high esthetic concerns and has had multiple failed surgical attempts that is now presenting for definitive management.”
THE OUTCOME
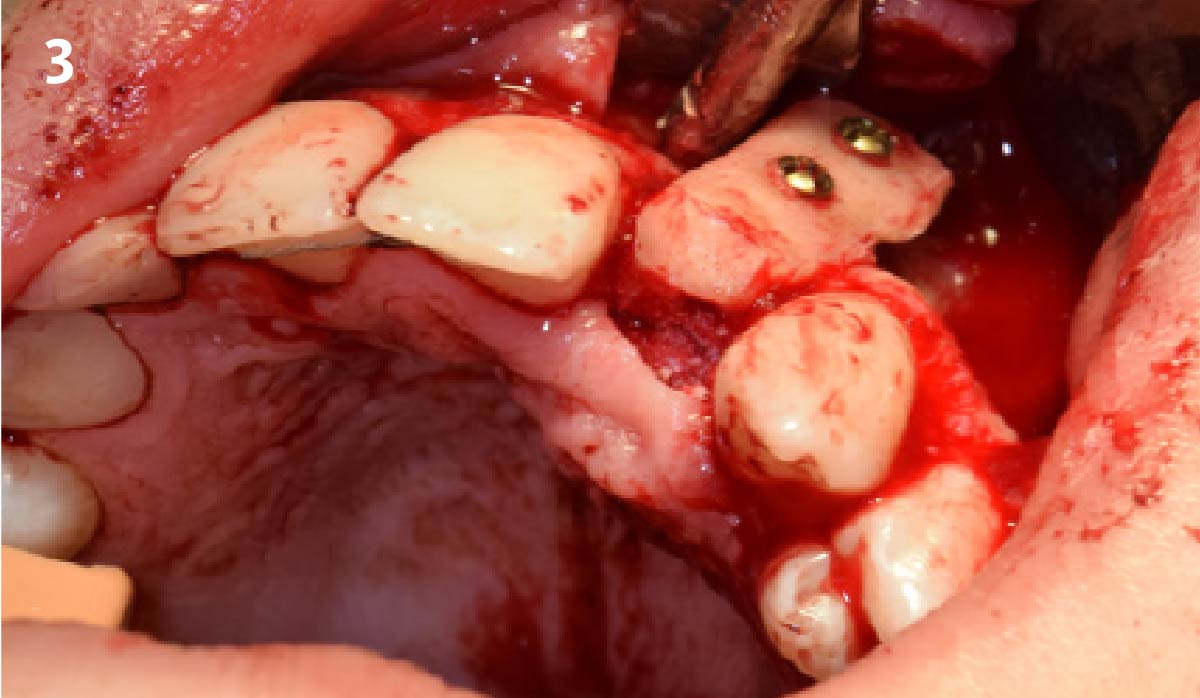
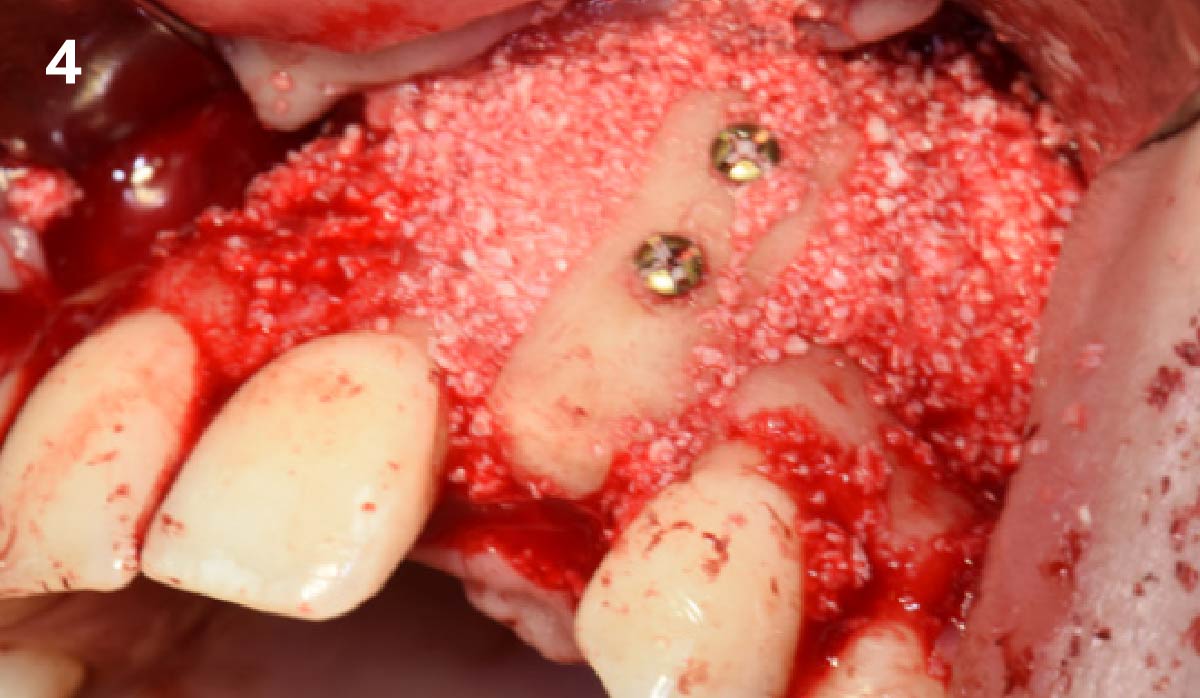
This case was dependent upon adequate hard-tissue reconstruction combined with soft-tissue manipulation to eliminate scar tissue and provide esthetic recontouring. Obtaining an adequate autogenous graft combined with Geistlich Bio-Oss® at the periphery of the onlay graft is essential for anterior-posterior and vertical augmentation. Utilizing a Geistlich Mucograft® matrix at the ridge crest to help contain the particulate graft and improve the soft-tissue profile for subsequent immediate provisionalization and re-contouring of the surrounding soft tissue played a significant role in the esthetic success.
Dr. Richard E. Bauer, III
Oral and Maxillofacial Surgeon – University of Pittsburgh
Richard E. Bauer, III, DMD, MD is a graduate of the University of Pittsburgh Schools of Dental Medicine and Medicine. Dr. Bauer completed his residency training in Oral and Maxillofacial Surgery at the University of Pittsburgh Medical Center. Dr. Bauer has served on multiple committees for the American Association of Oral and Maxillofacial Surgery (AAOMS). He is a full-time faculty member and Residency Program Director at the University of Pittsburgh in the department of Oral and Maxillofacial Surgery and his practice is focused on dental implants and corrective jaw surgery. He has been active in research with focus on bone regeneration and virtual applications for computer assisted planning and surgery.