BIOBRIEF
Mandibular Ridge Augmentation Using Customized Titanium Mesh

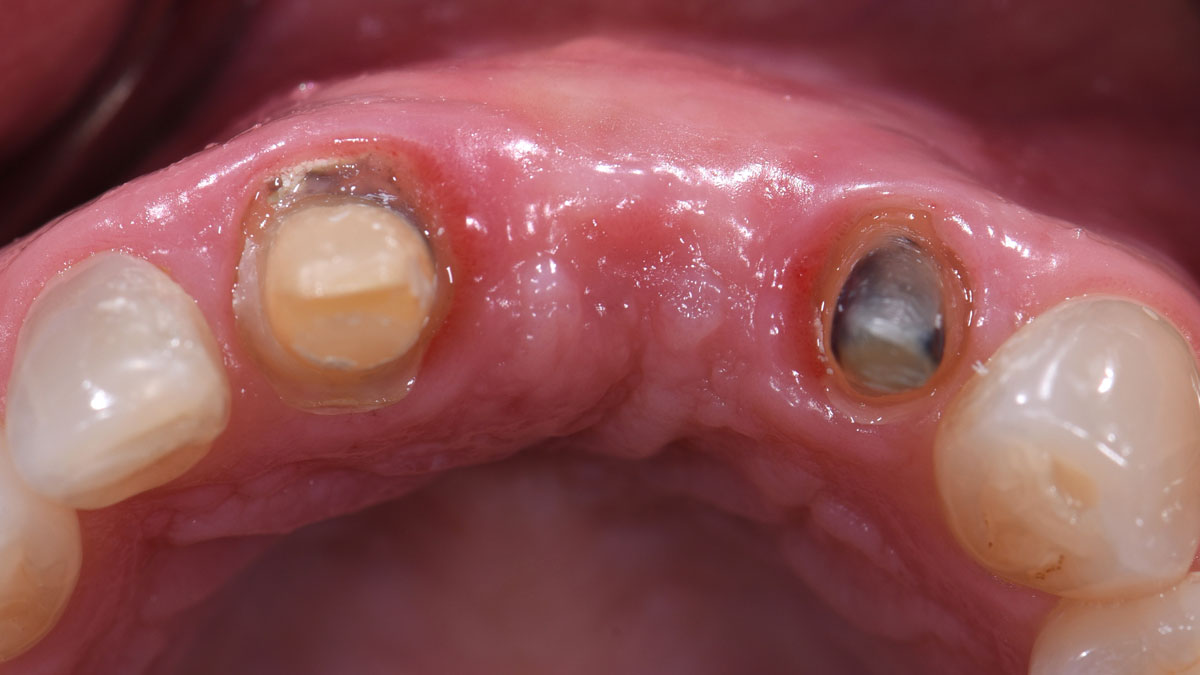
THE SITUATION
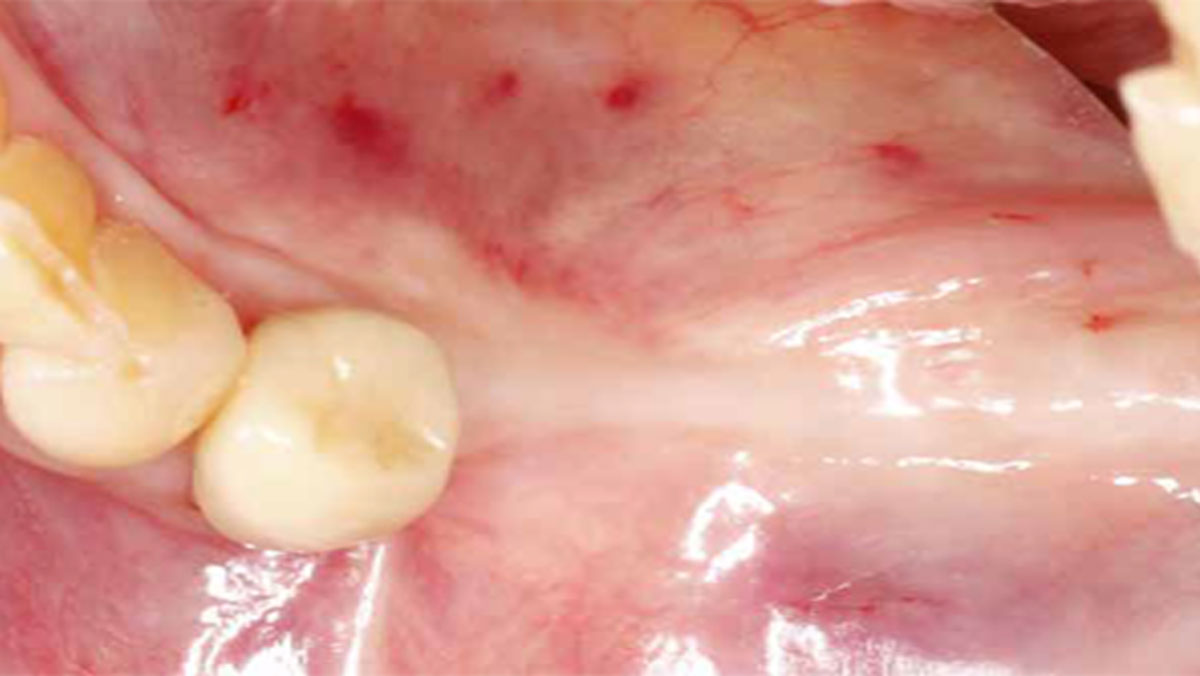
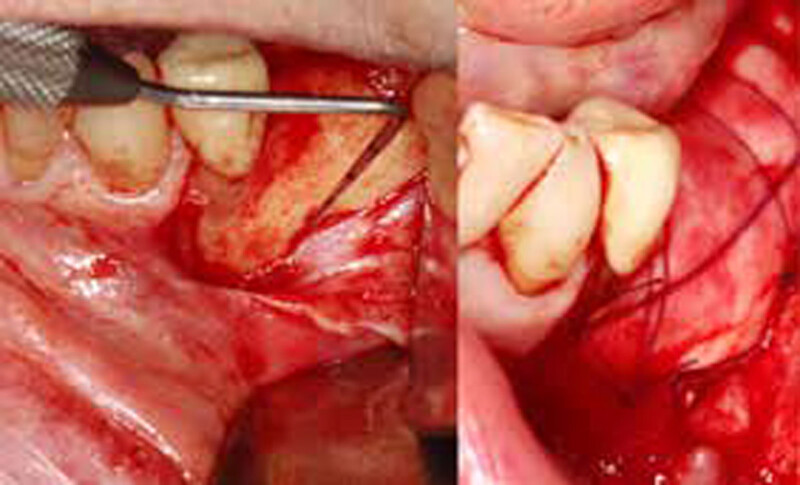
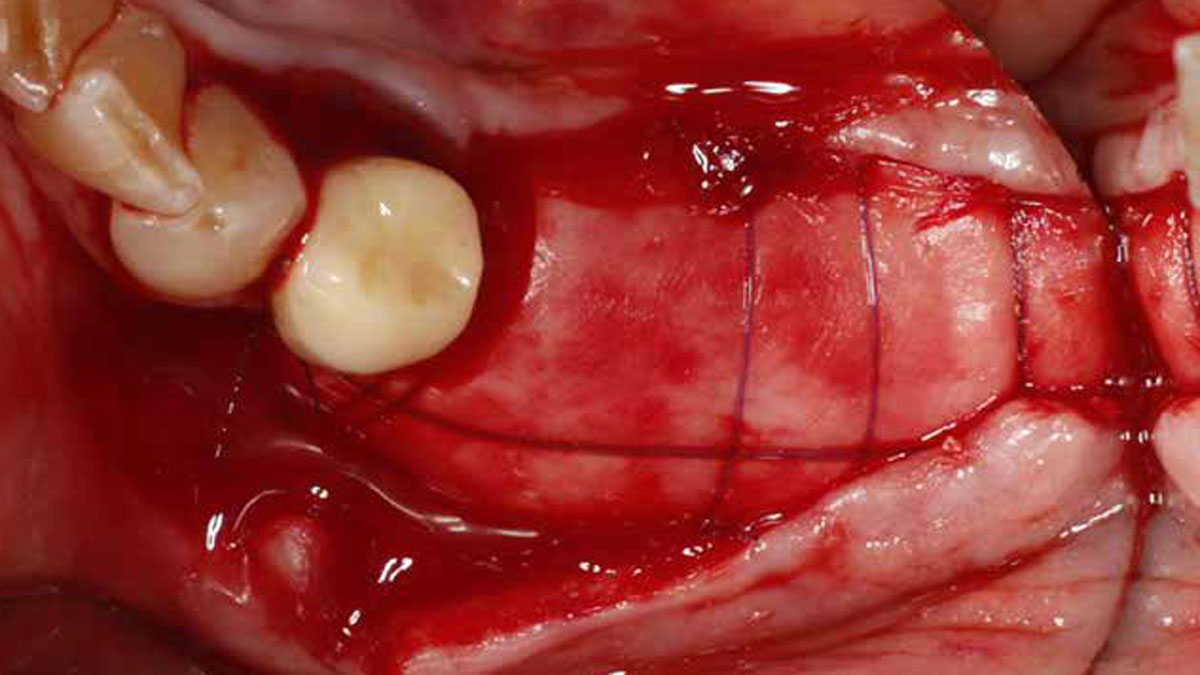
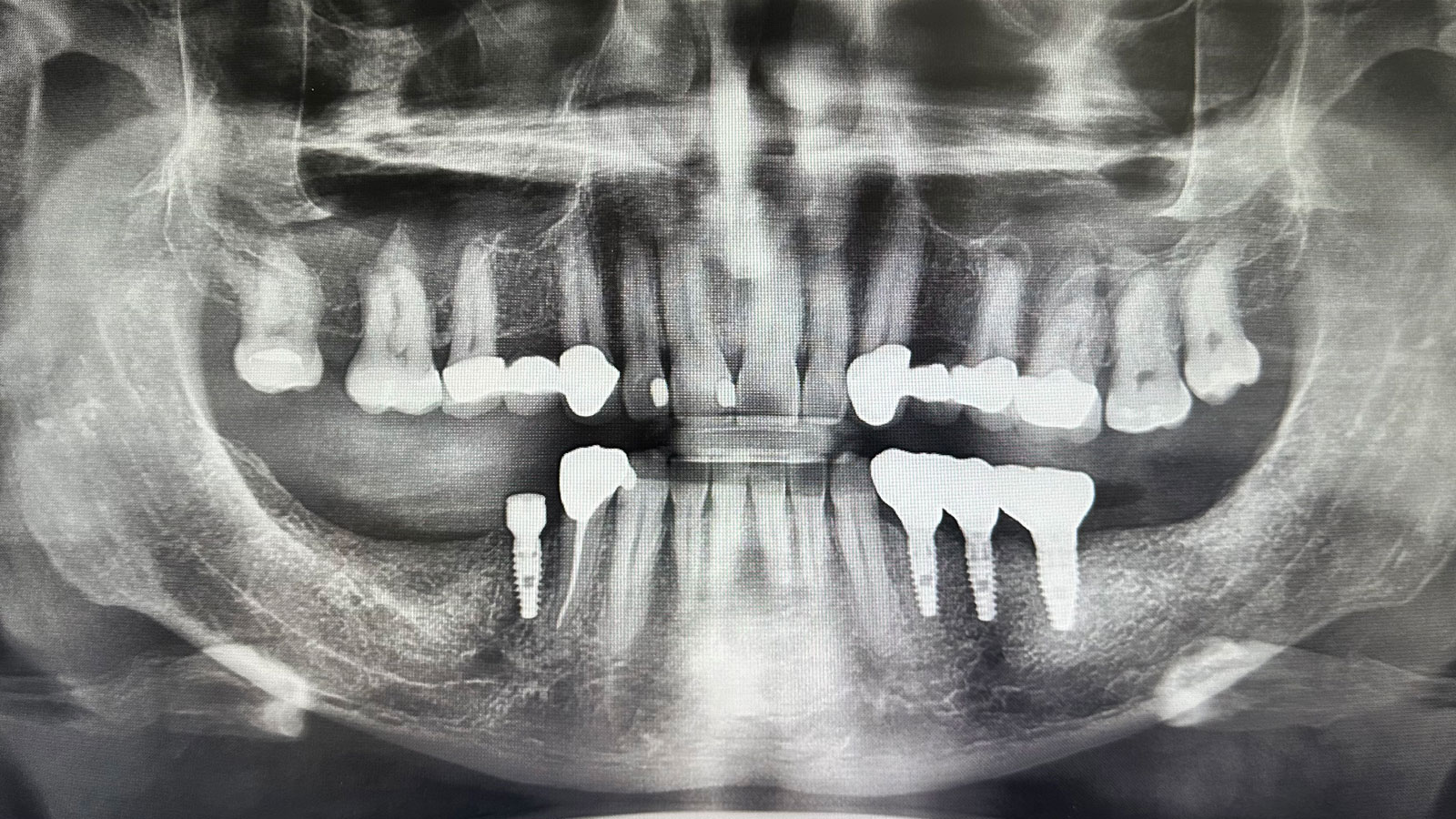
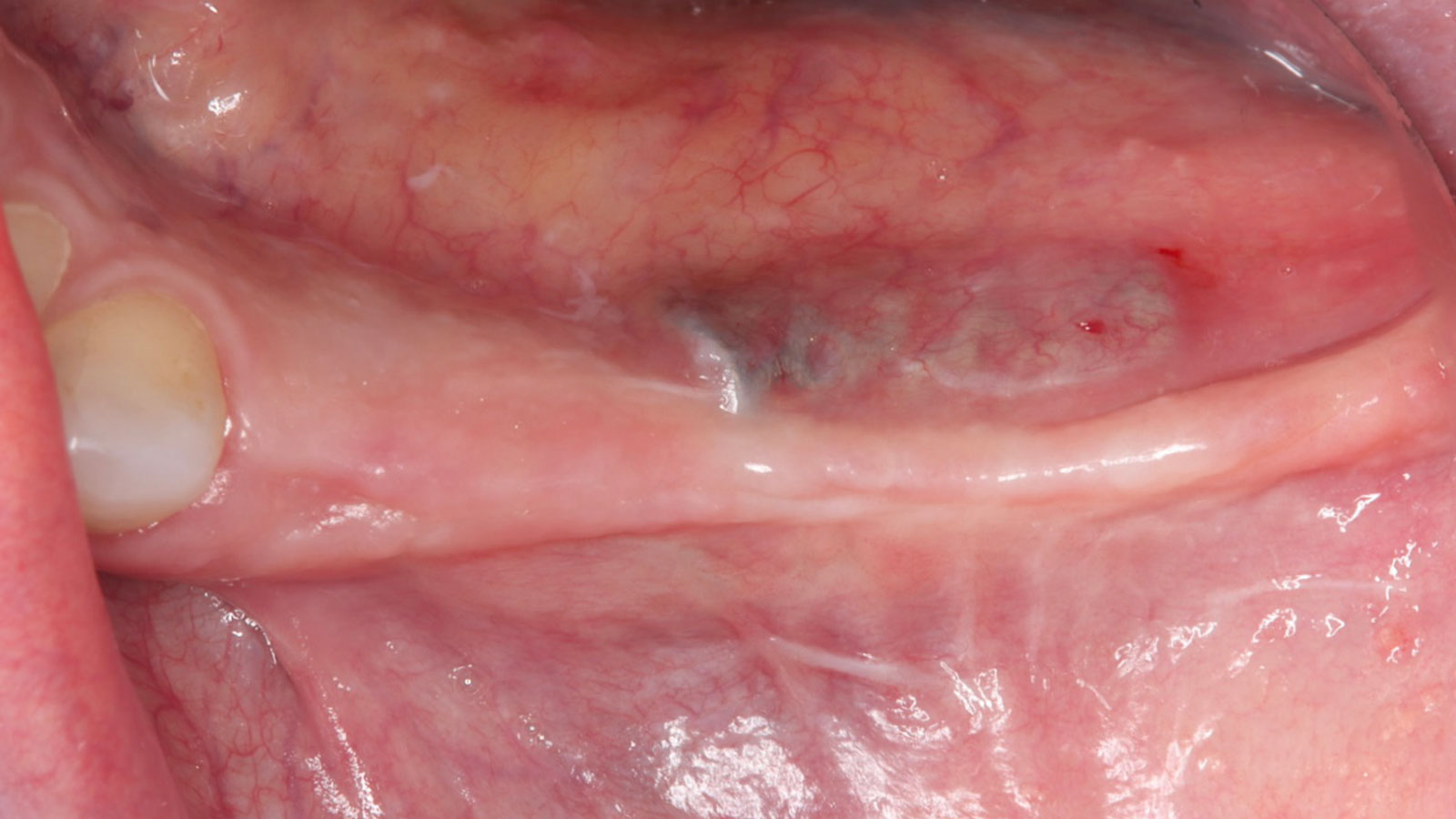
A 60-year-old healthy male presented with a failing lower left bridge. Due to a long history of missing teeth, he had a significantly atrophic mandibular ridge. We decided to use a customized titanium mesh to achieve the necessary vertical and horizontal bone augmentation for dental implant rehabilitation.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system | Light smoker | Impaired immune system |
| Patient’s esthetic requirements | Low | Medium | High |
| Restorative status of adjacent tooth | Intact | Restored | |
| Width of tooth gap | 1 tooth (≥ 7 mm) | 1 tooth (≤ 7 mm) | 2 teeth or more |
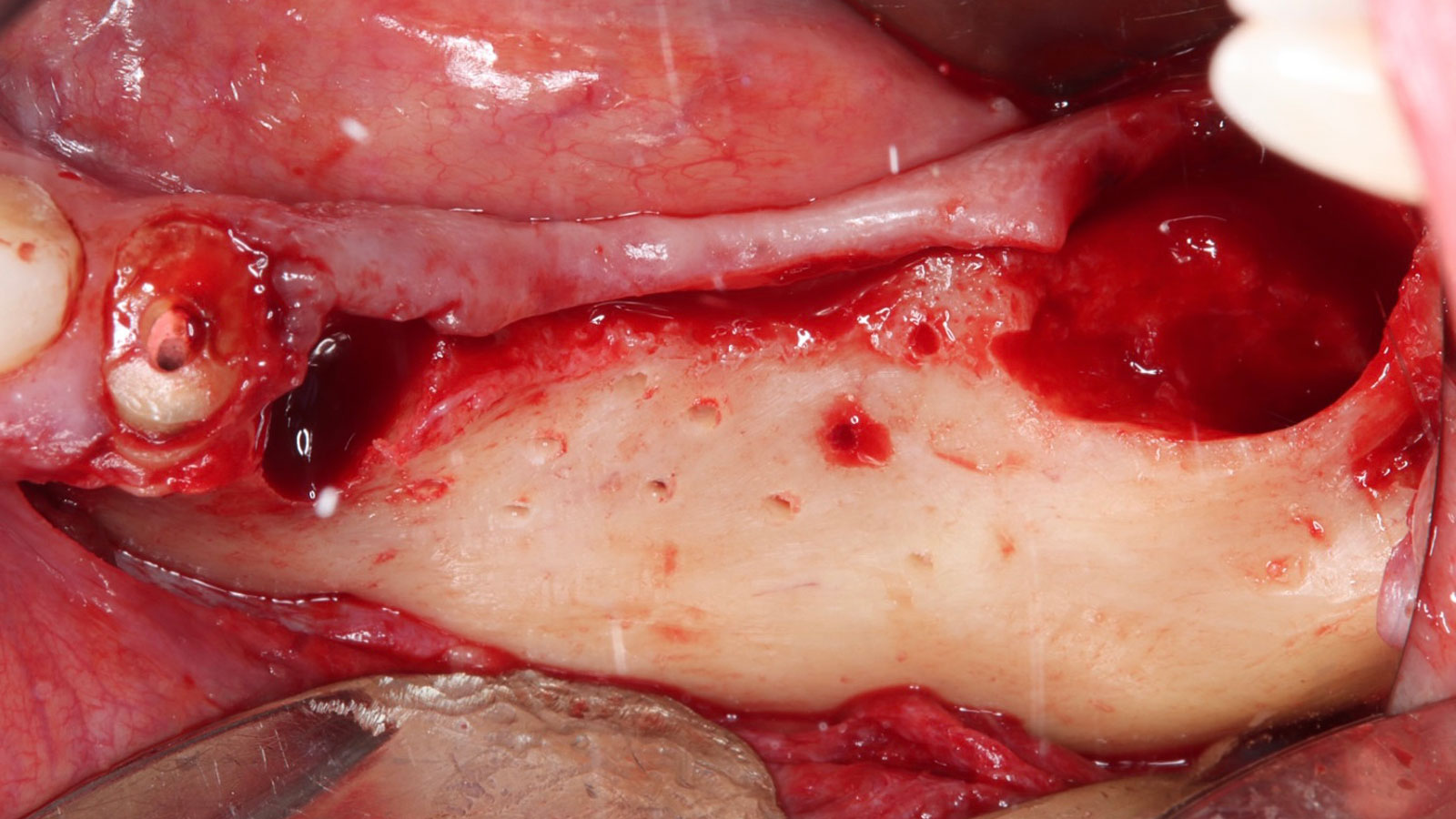
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
THE APPROACH
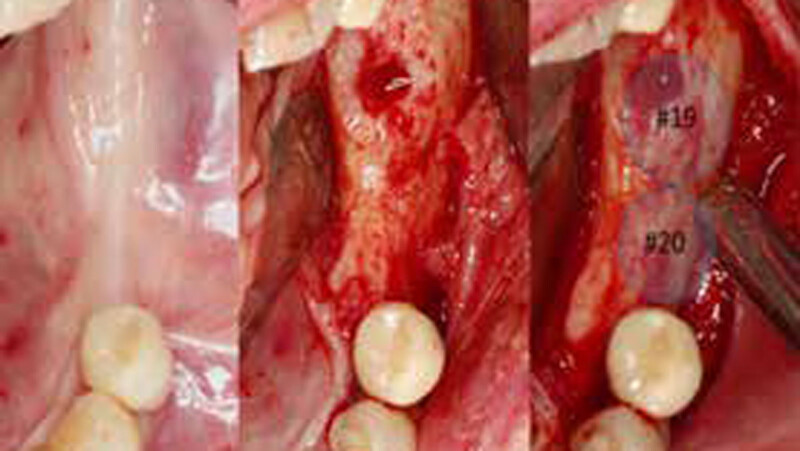
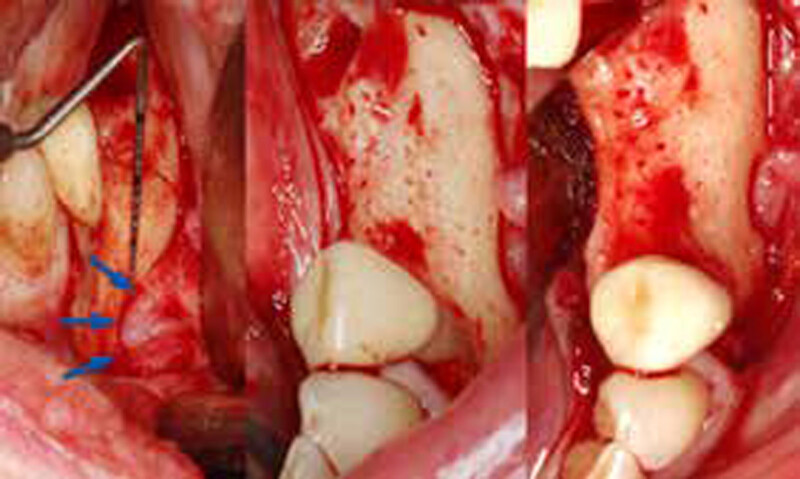
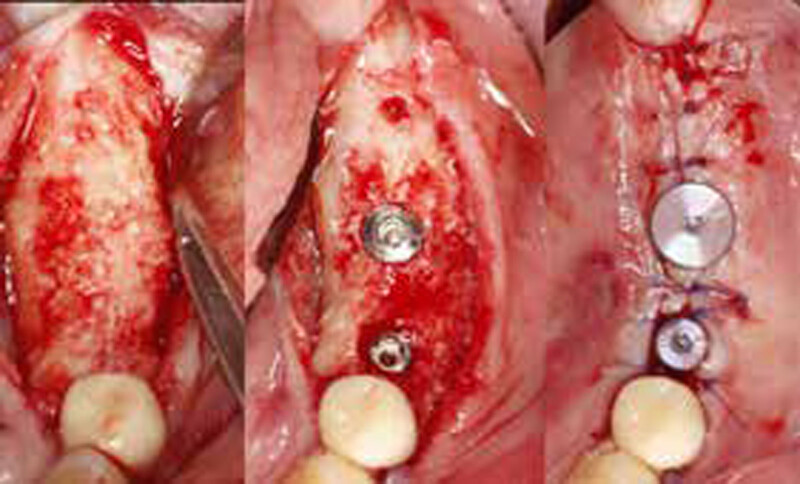
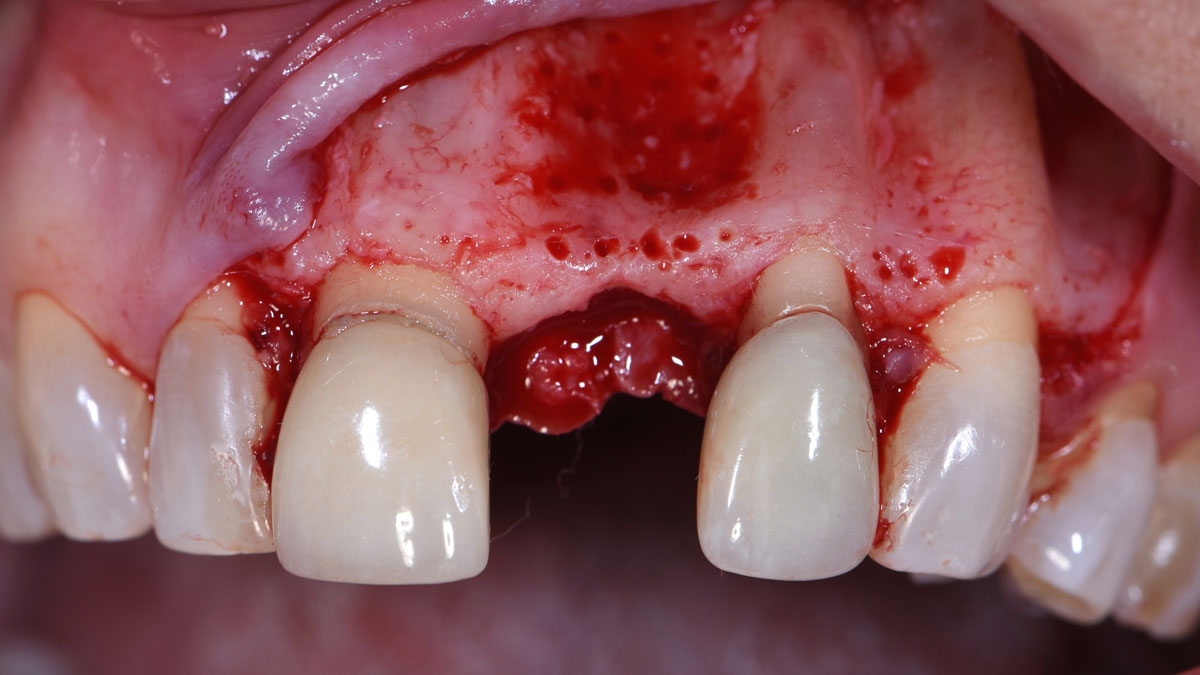
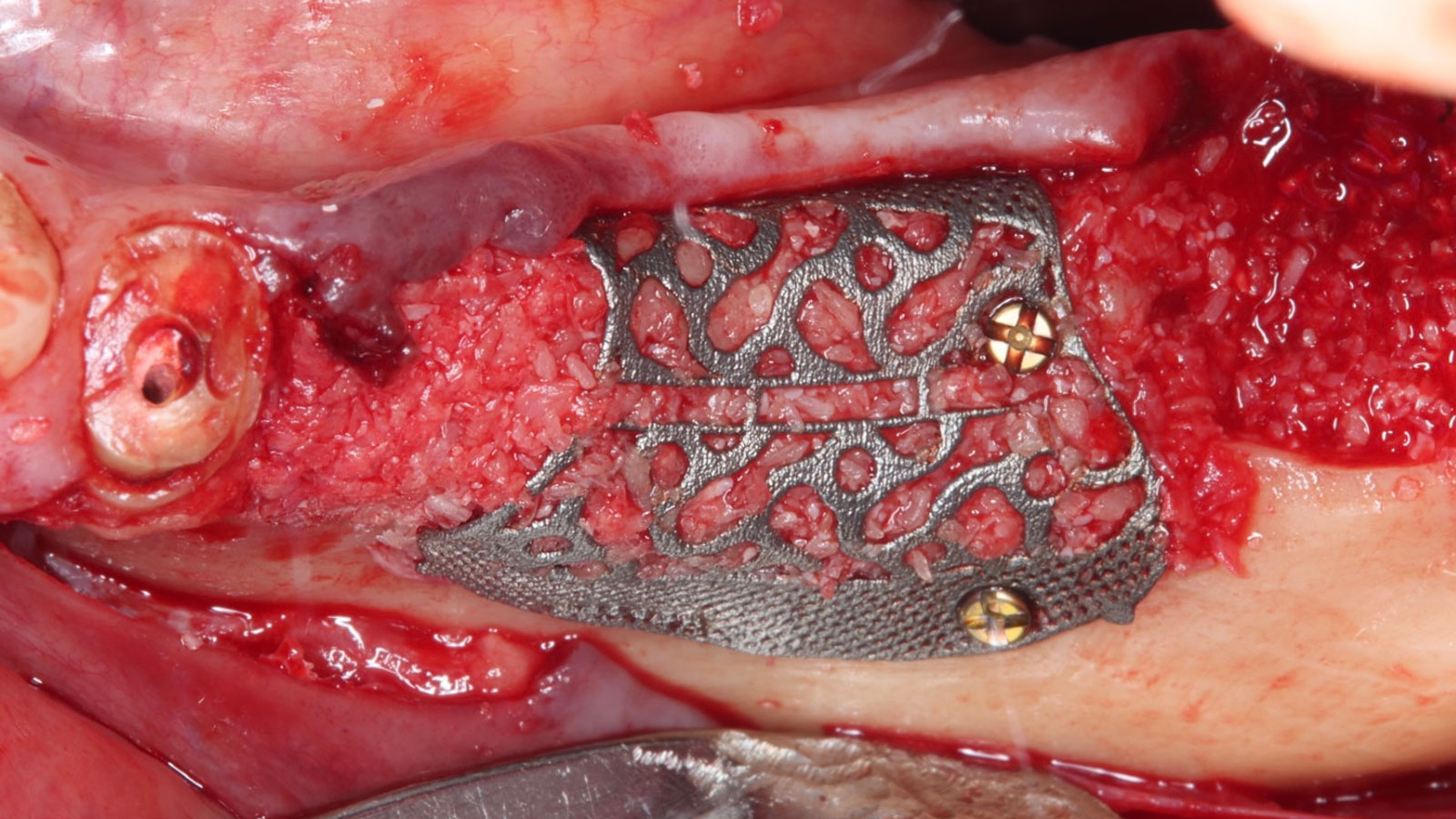
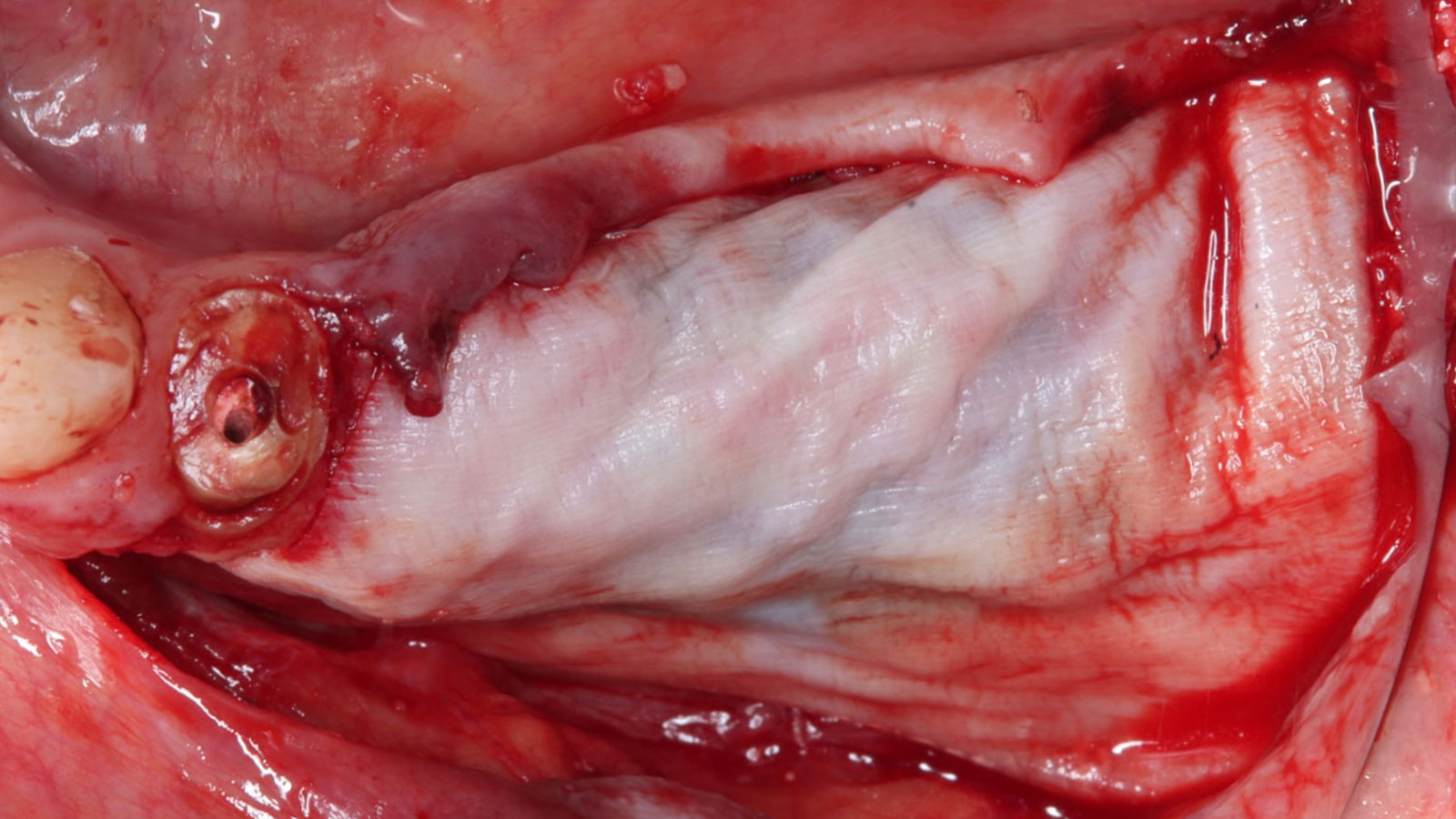
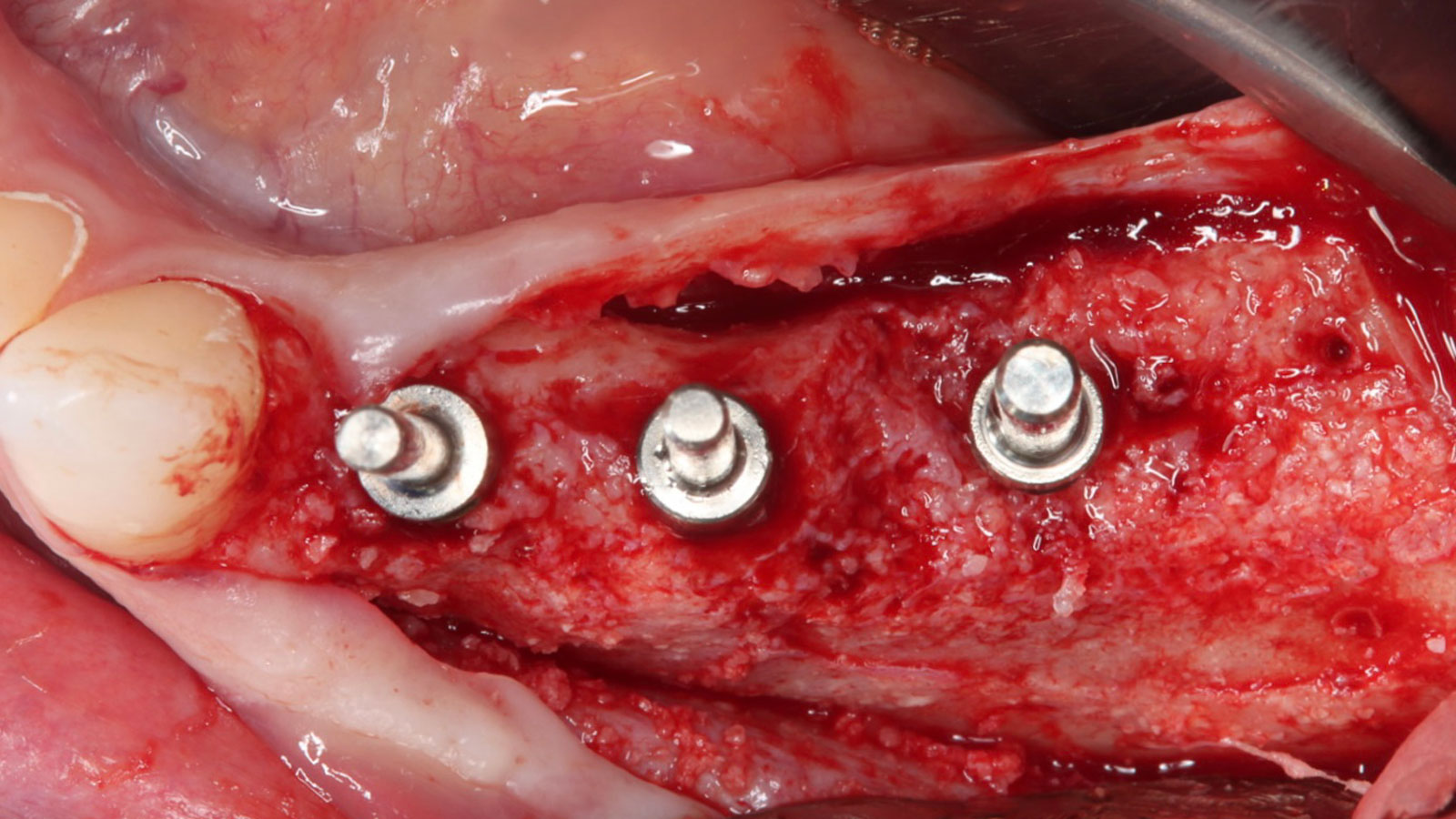
The goal of this procedure was to regenerate sufficient bone to place restoratively driven dental implants. Due to the horizontal and vertical ridge deficiency, we used a customized titanium mesh to predictably achieve this outcome.
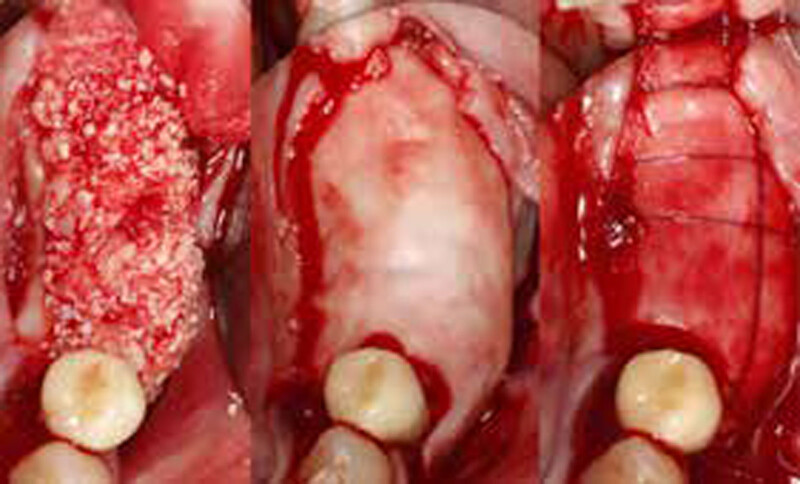
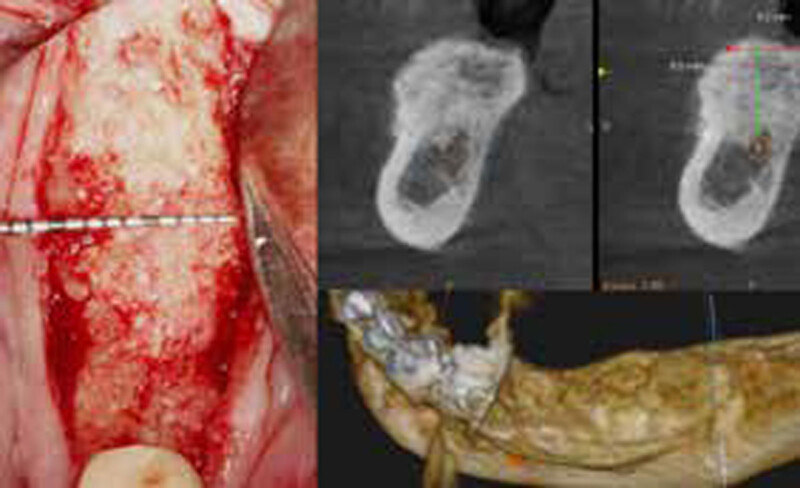
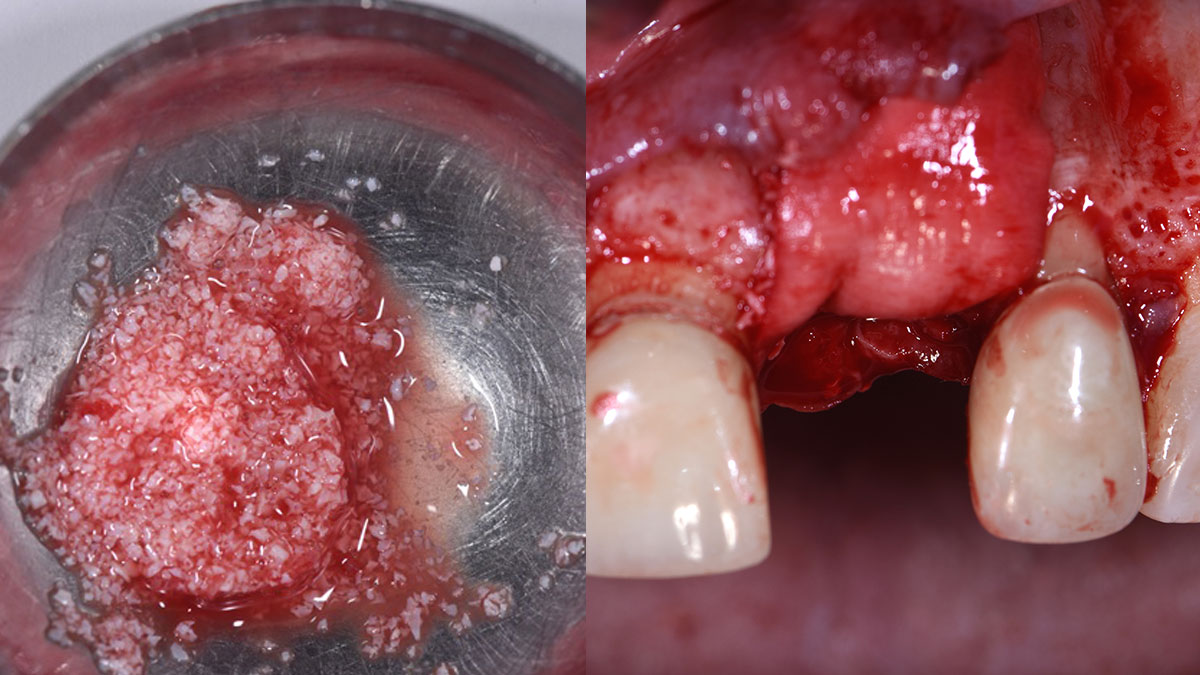
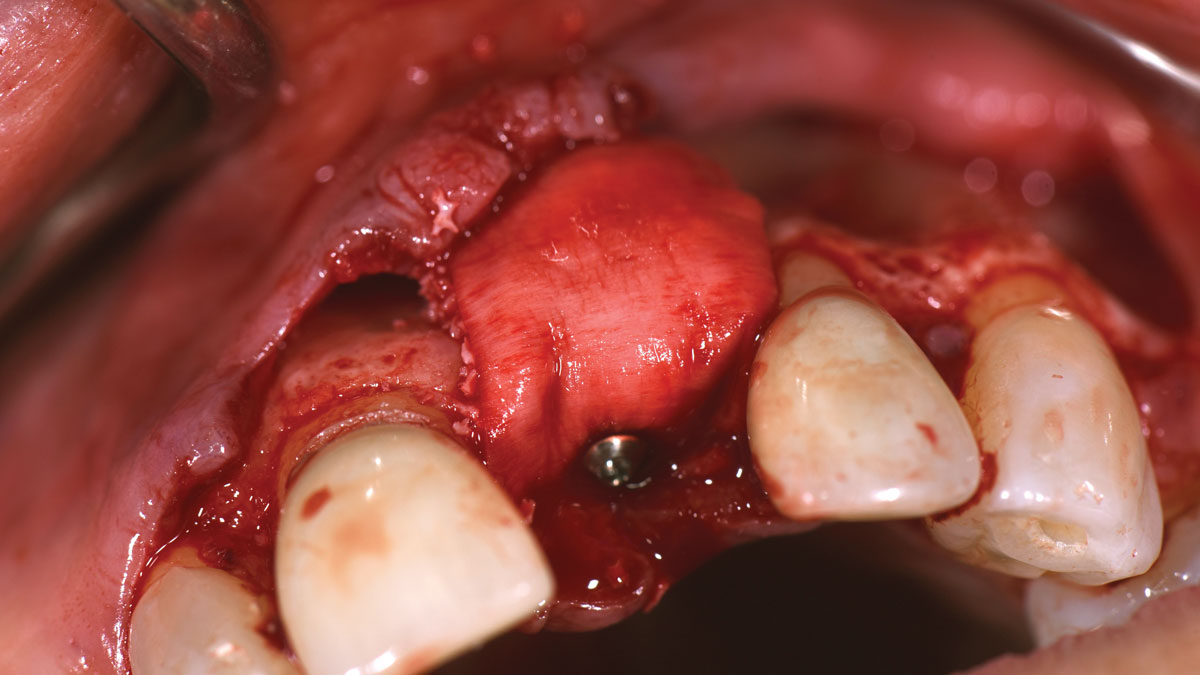
Autogenous bone collected with SafeScraper Twist and Geistlich Bio-Oss® filled the Yxoss CBR® Protect and a Geistlich Bio-Gide® collagen membrane covered the mesh.
.
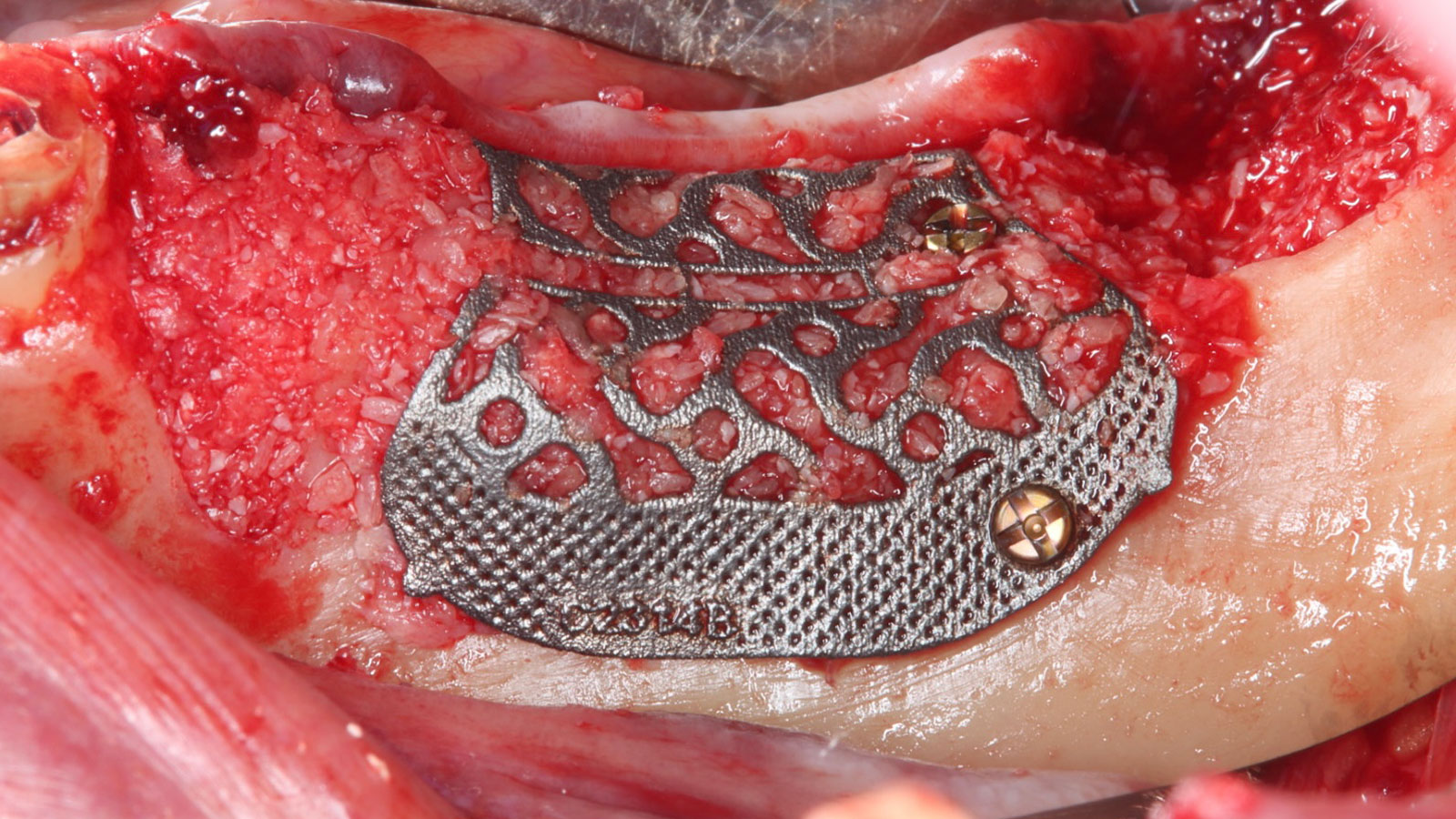

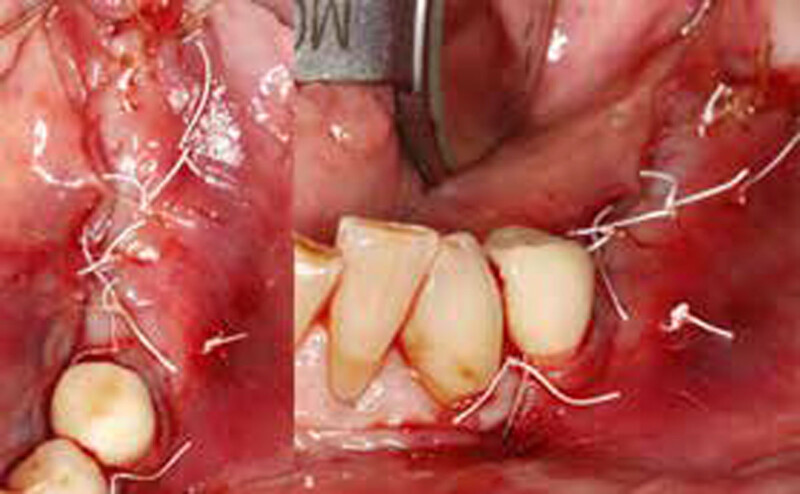
“Success in these cases primarily depends on proper mesh design and careful handling of soft tissue to ensure zero-tension primary closure.”
— Shaun R. Young, DMD
THE OUTCOME
A left mandibular ridge deficiency was corrected using a Yxoss CBR® Protect Customized Bone Regeneration Titanium Mesh, designed from the patient’s CBCT scan.
Shaun R. Young, DMD
Dr. Shaun Young, an Oral and Maxillofacial Surgeon based in Tampa, Florida, specializes in complex ridge augmentation, immediate implants, and All-on-X full arch rehabilitation. He earned his Doctor of Dental Medicine degree from the University of Florida and completed his OMFS residency at Emory University in Atlanta, Georgia, where he served as Administrative Chief Resident. Dr. Young brings his expertise to a full-scope group practice, serving Tampa, Clearwater, and New Port Richey, Florida.