





BIOBRIEF
Phenotype Conversion Using Geistlich Fibro-Gide® for Immediate Implants in the Esthetic Zone


THE SITUATION
A healthy non-smoking 50-year-old female patient who desires a single tooth solution to replace a non-restorable tooth, #12. A root fracture at the level of the palatal post was diagnosed in a root canaled tooth. Maintaining esthetics of the adjacent teeth is important as they are also restored with single full coverage porcelain crowns. Lastly, treatment time reduction and a minimally invasive surgical technique are desired by the patient for reduced downtime and post-operative morbidity.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system | Light smoker | Impaired immune system |
| Patient’s esthetic requirements | Low | Medium | High |
| Height of smile line | Low | Medium | High |
| Gingival biotype | Thick – “low scalloped” | Medium – “medium scalloped” | Thin – “high scalloped” |
| Shape of dental crowns | Rectangular | Triangular | |
| Infection at implant sight | None | Chronic | Acute |
| Bone height at adjacent tooth site | ≤ 5 mm from contact point | 5.5 – 6.5 mm from contact point | ≥ 7 mm from contact point |
| Restorative status of adjacent tooth | Intact | Restored | |
| Width of tooth gap | 1 tooth (≥ 7 mm) | 1 tooth (≤ 7 mm) | 2 teeth or more |
| Soft-tissue anatomy | Intact | Compromised | |
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
Facial Bone Wall Phenotype: High Risk (<1mm)
Esthetic Risk Profile (ERP) = Medium (summary of above)
THE APPROACH
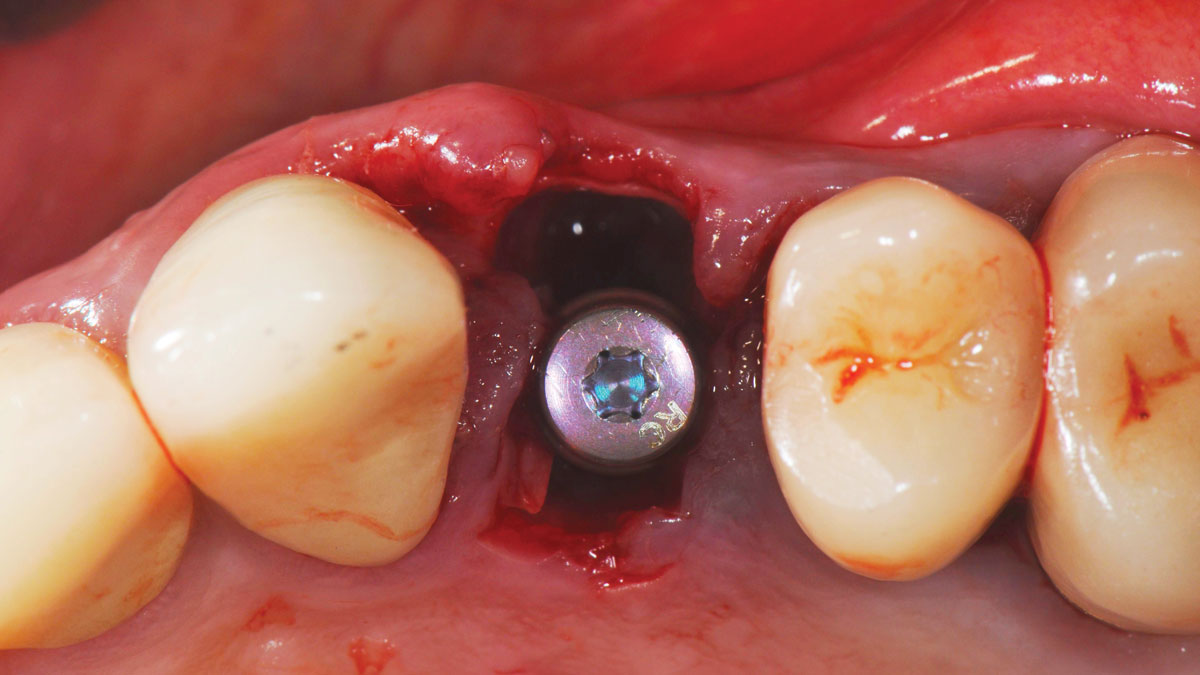
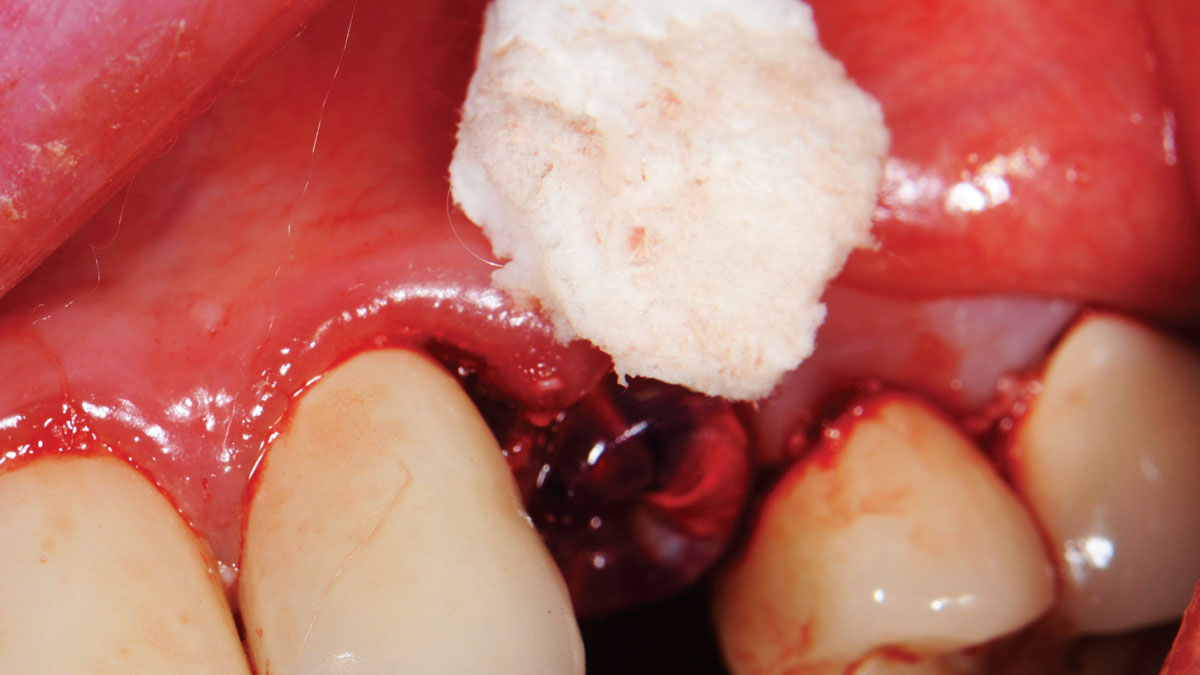
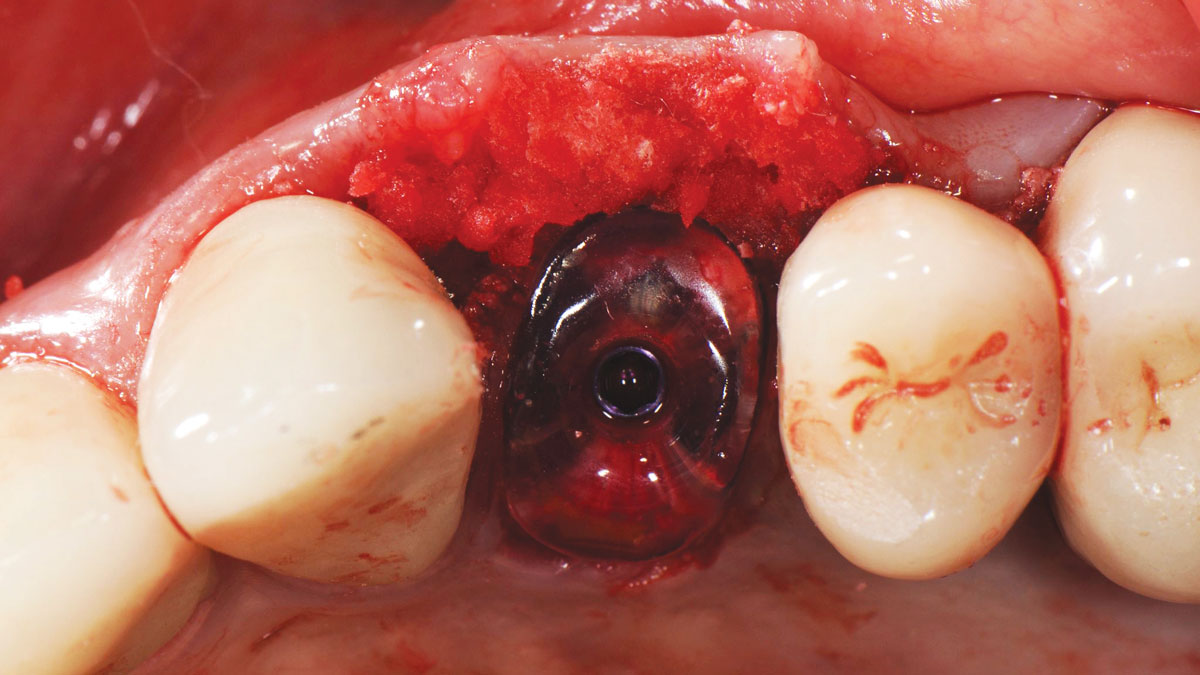
A minimally invasive surgical removal of tooth #12 with maintenance of the buccal plate and leaving a 3mm buccal gap. The implant will be placed one mm below the level of the intact buccal plate with an anatomically correct surgical guide template to provide for a screw-retained solution. The gap will be filled with Geistlich Bio-Oss Collagen® to maintain the bone buccal to the implant, and a palate free approach utilizing Geistlich Fibro-Gide® for soft tissue thickening to accomplish “phenotype conversion.” The long-term surgical goal is >2-3mm thickness of both hard and soft tissue buccal to the implant.

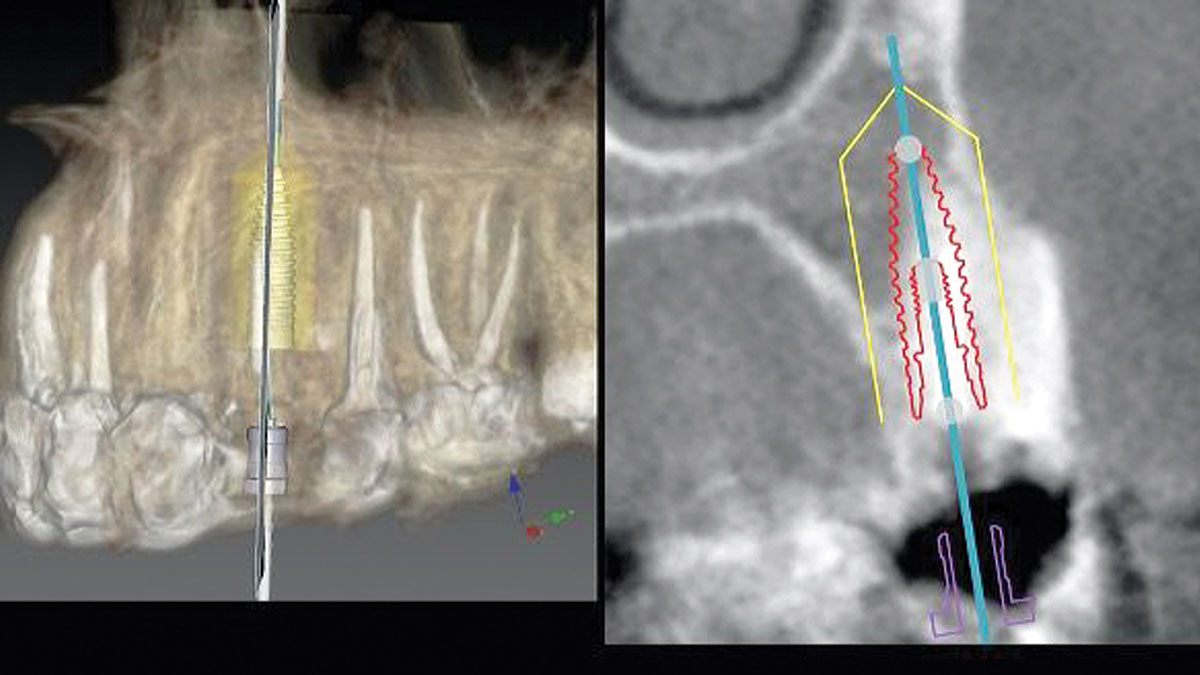
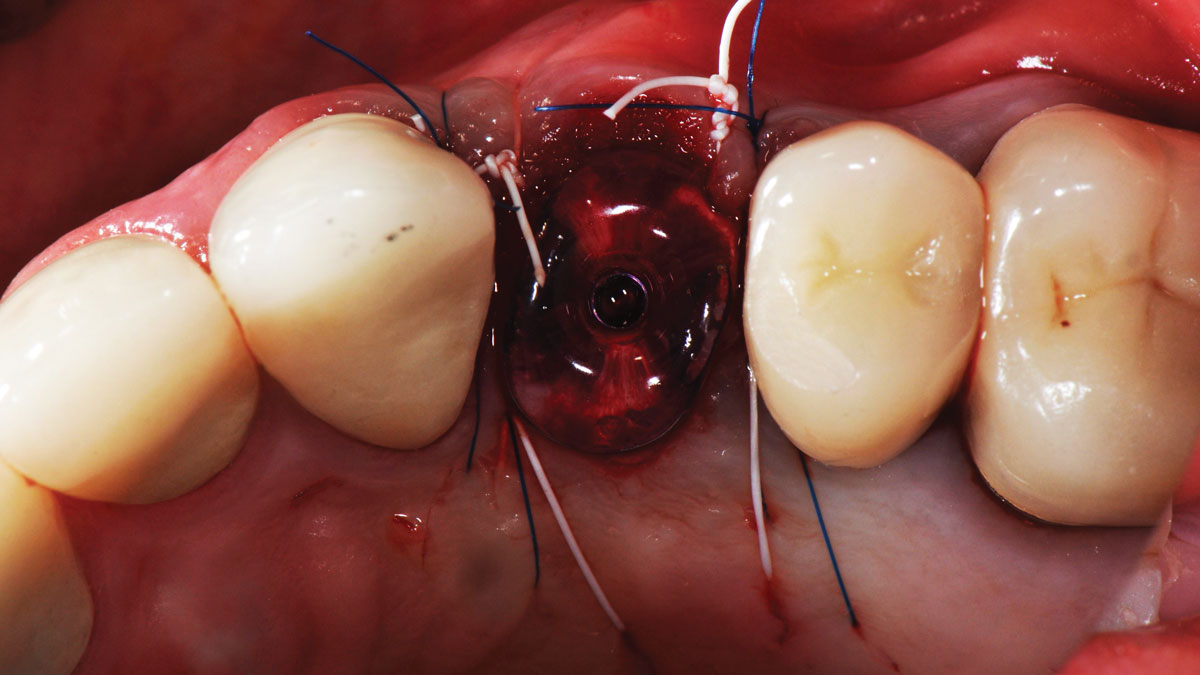

“High esthetic demands were the primary concern with this case. They were addressed with the diagnostic tools of clinical photos, a site specific CBCT to evaluate the buccal wall status, and summing the findings with patient expectations gathered using the Esthetic Risk Assessment (knee-to-knee; eye-to-eye) which is used along with our consent agreement to treatment.”
THE OUTCOME
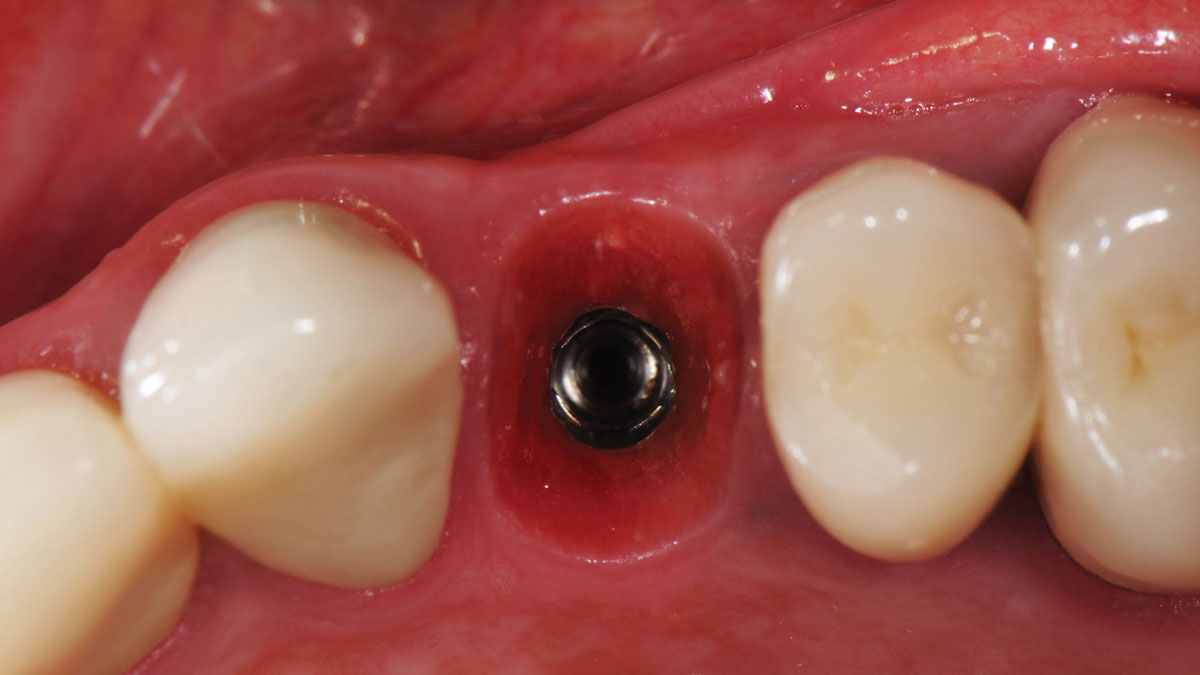
Minimally invasive surgery for buccal wall maintenance, virtually planning the buccal gap and implant width, using a xenograft in the buccal gap with phenotype conversion using a volume stable collagen matrix in conjuction with immediate contour management, allows for the best chance for papillae fill interproximally and maintenance of the mid-buccal gingival margin long-term.
Dr. Robert A. Levine
Robert A. Levine DDS is a board-certified periodontist at the Pennsylvania Center for Dental Implants and Periodontics in Philadelphia. He is a Fellow of the International Team for Dental Implantology (ITI), College of Physicians in Philadelphia, International Society of Periodontal Plastic Surgeons and the Academy of Osseointegration. He has post-graduate periodontology and implantology teaching appointments at Temple University in Philadelphia, UNC in Chapel Hill and UIC in Chicago and has over 80 scientific publications.