







BIOBRIEF
Vertical and Horizontal Maxillary Ridge Reconstruction with Advanced Grafting

THE SITUATION
A 26-year-old edentulous female presented for implant-supported maxillary rehabilitation. She was systemically healthy and classified as ASA I. Clinical and radiographic evaluation revealed a Seibert Class III maxillary ridge defect with combined horizontal and vertical deficiencies. The patient exhibited a medium smile line and reported a highly active lifestyle with regular physical activity, indicating the need for a stable, durable, and esthetically driven implant rehabilitation capable of meeting long-term functional demands.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system Non-smoker | Light smoker | Impaired immune system |
| Patient’s esthetic requirements | Low | Medium | High |
| Height of the smile line | Low | Medium | High |
| Gingival biotype | Thick – “low scalloped” | Medium – “medium scalloped” | Thin – “high scalloped” |
| Infection at implant sight | None | Chronic | Acute |
| Bone height at adjacent tooth | ≤ 5 mm from contact point | 5.5 – 6.5 mm from contact point | ≥ 7 mm from contact point |
| Soft-tissue anatomy | Intact | Compromised | |
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
THE APPROACH
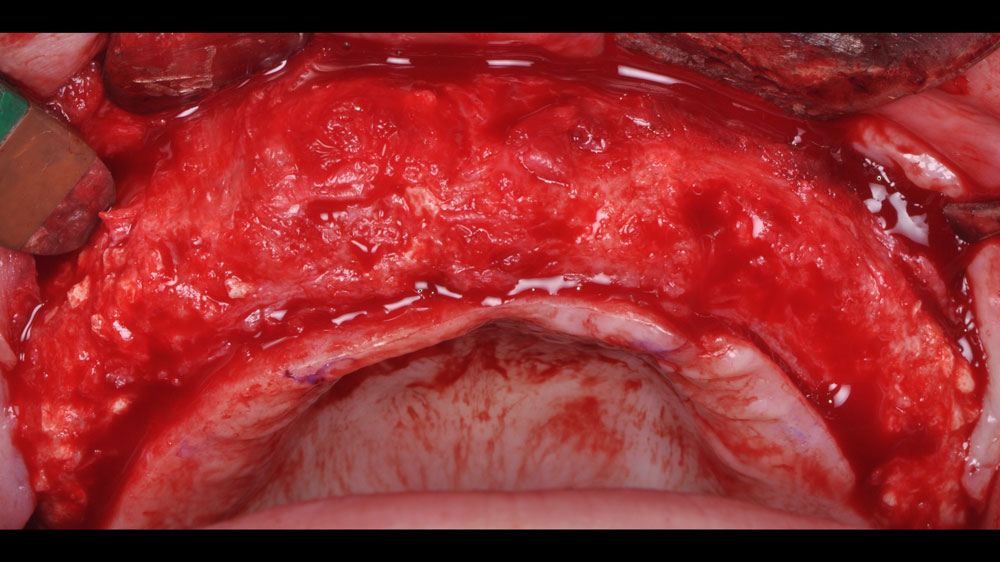
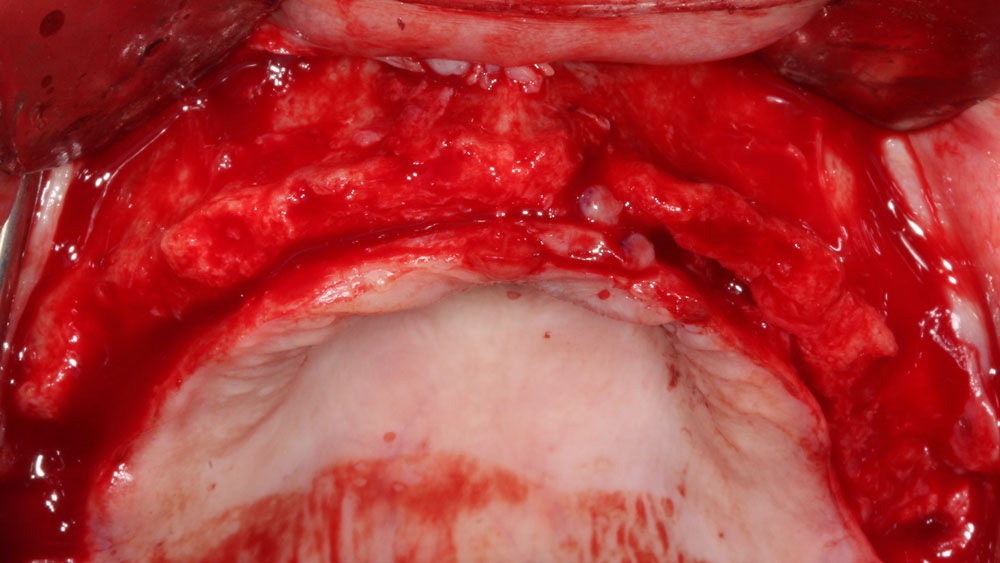
Horizontal and vertical ridge augmentation was performed using a full-thickness maxillary flap with two distal vertical releasing incisions. Extensive buccal periosteal release and cortical perforations were carried out. A composite graft of large-particle vallos® allograft (demineralized cortical granules) and large-particle Geistlich Bio-Oss® xenograft, combined with rhPDGF-BB, a component of GEM 21S®, was placed and stabilized under a high-density PTFE membrane, which was secured with four horizontal mattress and multiple simple interrupted 4-0 PTFE sutures.



“The patient’s young age and
— Nikolaos Soldatos, DDS, PhD, MSD
excellent systemic health are favorable prognostic factors, but achieving optimal outcomes requires meticulous surgical execution, careful soft tissue management, and strict adherence to post-operative instructions to minimize complications and ensure long-term success.”
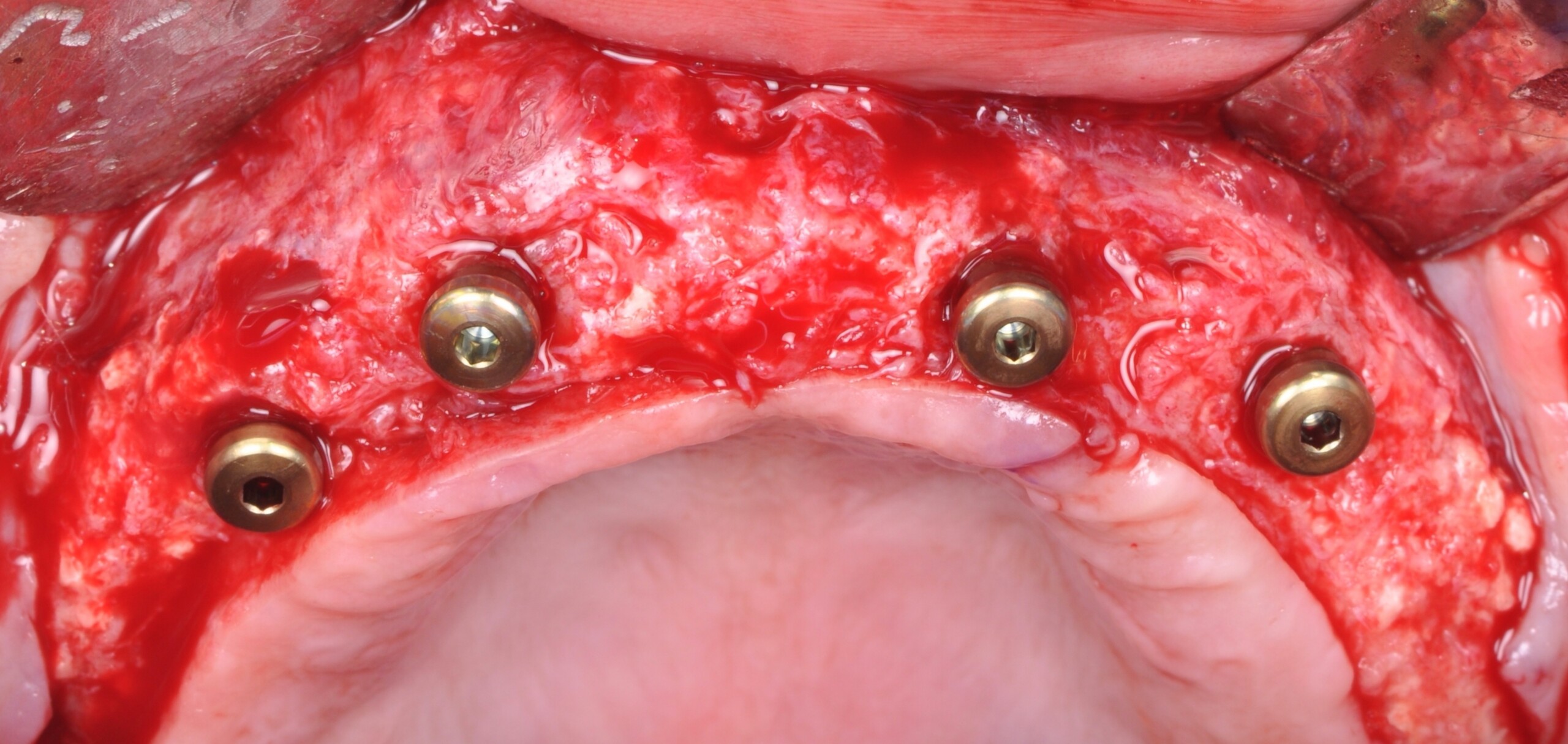
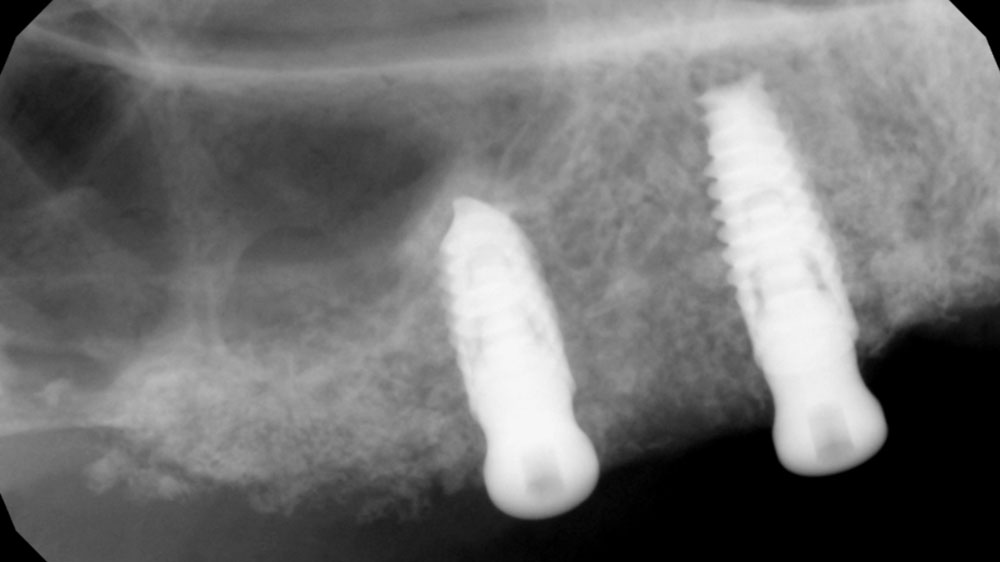
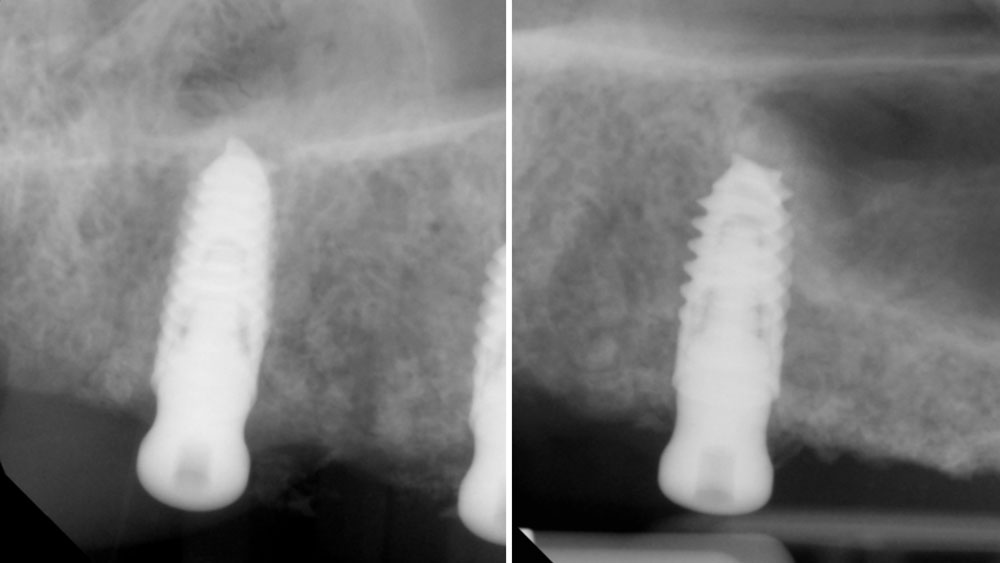
THE OUTCOME
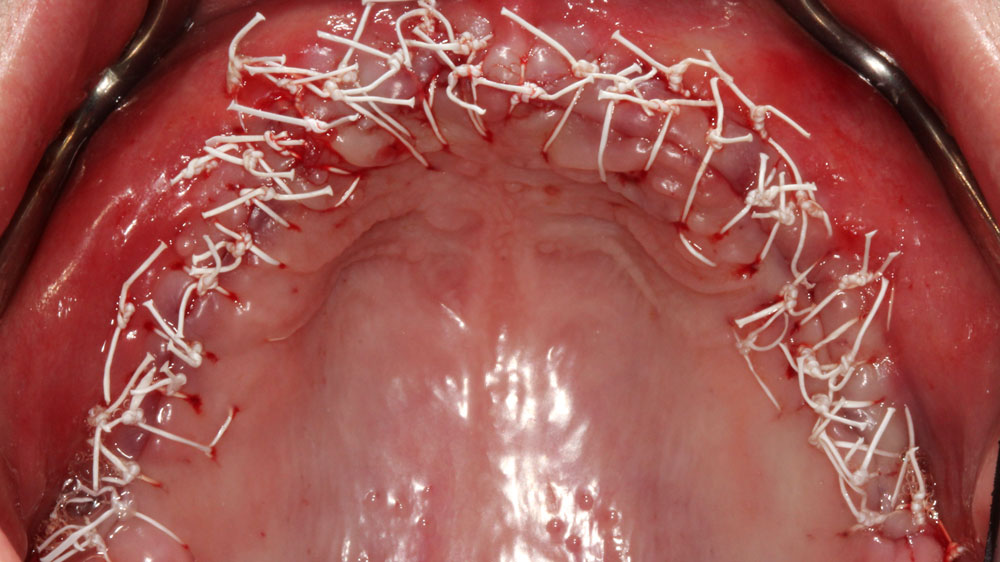
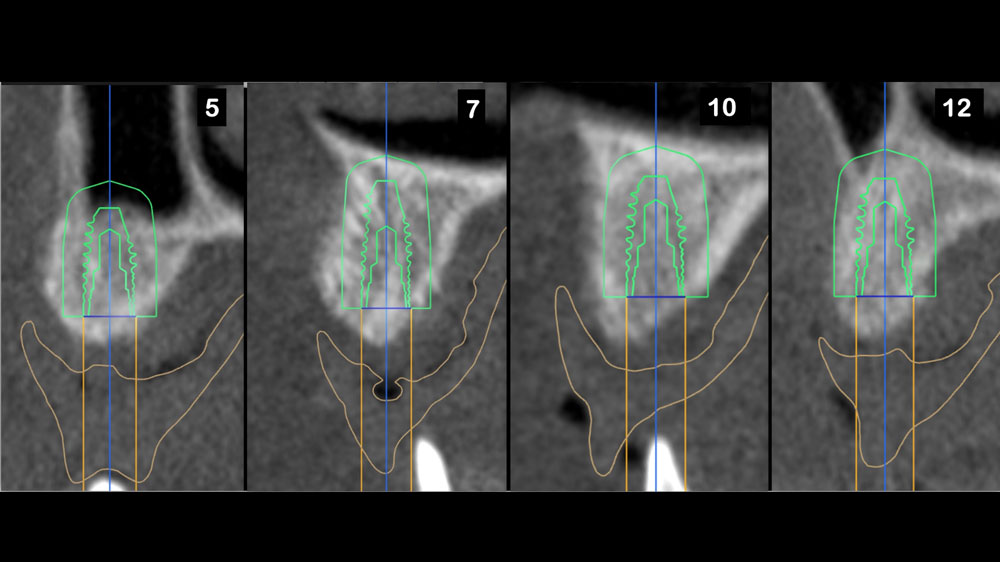
Horizontal (5–7 mm) and vertical (3–4 mm) ridge augmentation were successfully obtained, with stablewound management achieved through precise suturing techniques. The osteoinductive properties of the large vallos®, demineralized granules combined with rhPDGF-BB, a component of GEM21S® promoted high-quality bone regeneration, whereas the large Geistlich Bio‑Oss®, xenograft particles contributed to volume preservation by moderating resorption. As a result, four 4.3 mm implants were placed with high primary stability, each exceeding 35 N·cm of insertion torque, providing a strong foundation for a predictable esthetic and functional restoration.
Nikolaos Soldatos, DDS, PhD, MSD
Dr. Soldatos is a tenure-track Associate Professor and Clinical Director of the Postgraduate Advanced Program in Periodontics at Oregon Health & Science University. He is a Board-Certified Periodontist and Implant Surgeon, he holds a DDS, PhD, and MSD, and has completed advanced periodontal and implant training in both the U.S. and Europe. Dr. Soldatos’ research focuses on translational implant biology and bone regeneration. He is also a Fellow of the Academy of Osseointegration.
