Mix & Match! Buy 5 Products, Get 1 Free! Use code B5G1. Get Started!

Treatment Solution: Surgical Periodontal Treatment

CLINICAL CASE


THE OUTCOME
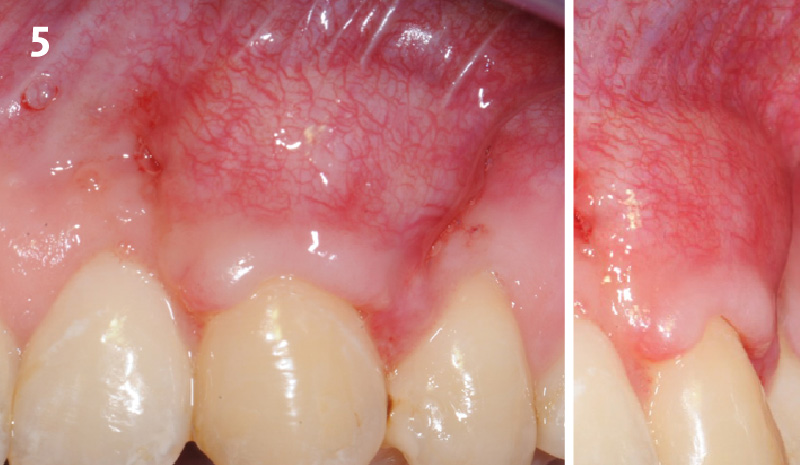
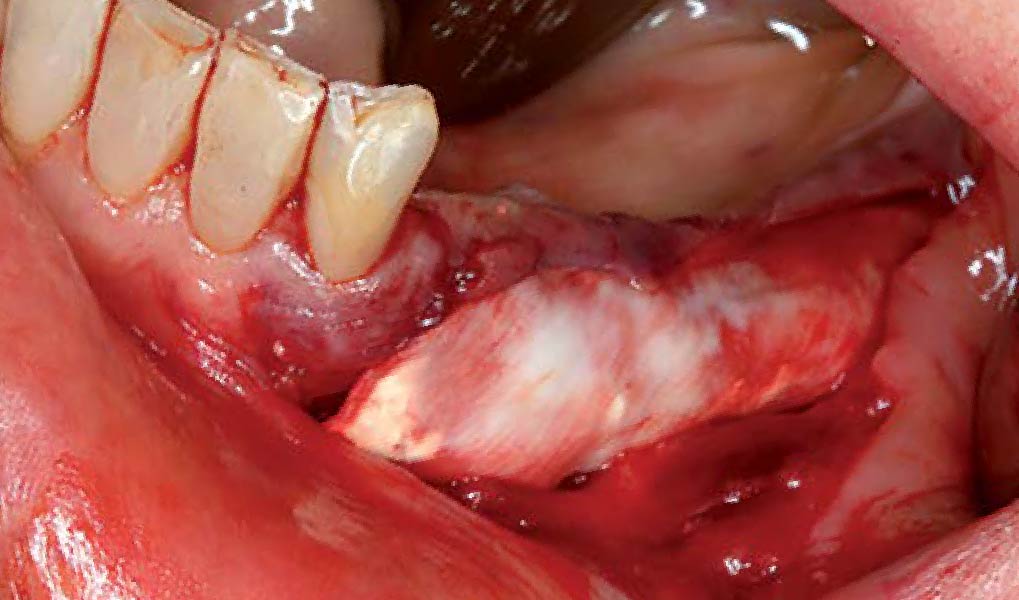
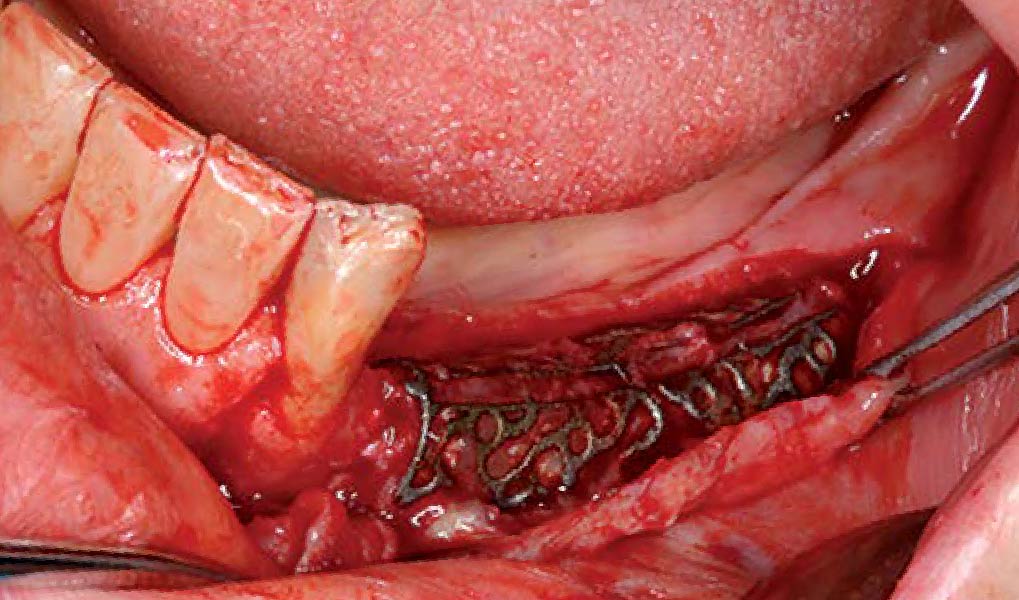
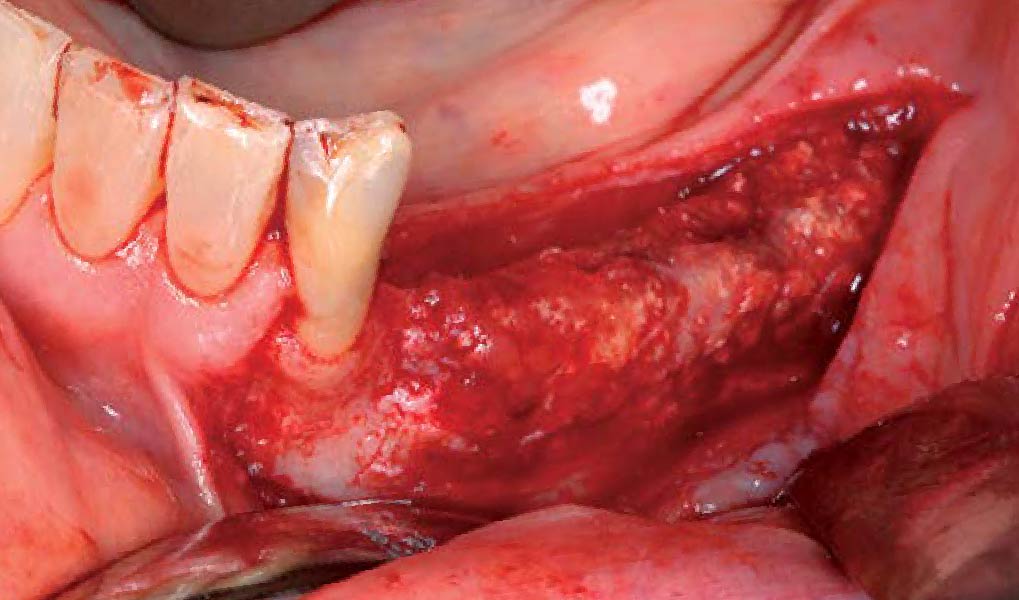
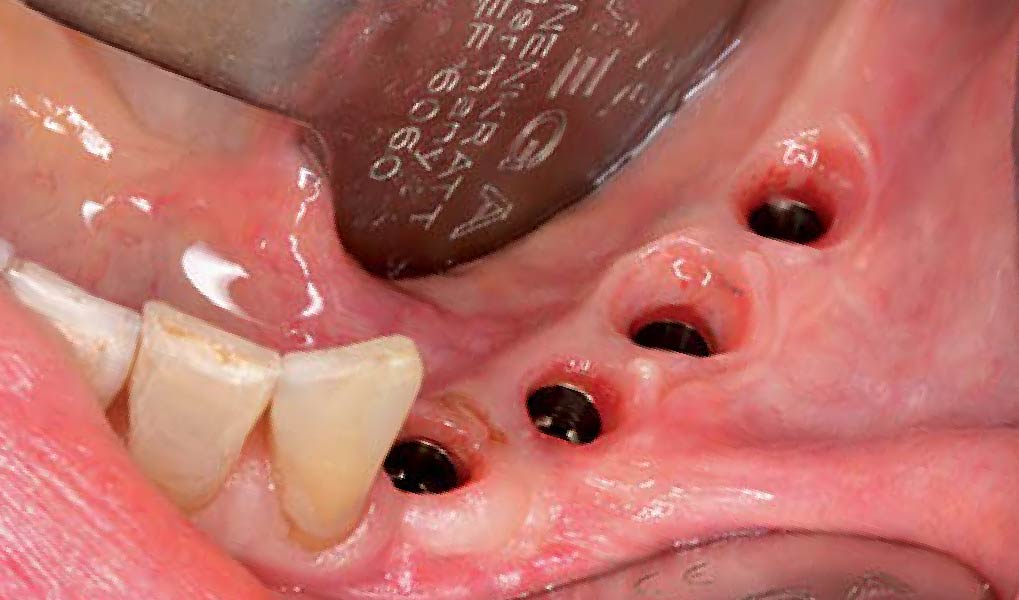
At 6 months, healing was complete with a bone fill of 10x10x6.5 mm. Tooth #7, affected by the combined defect, was fully regenerated. The adjacent ridge defect was also restored, enabling the placement of a regular-sized implant without the need for additional grafting.
Disclaimer: These results are not guaranteed; individual outcomes may vary depending on patient circumstances. This information is for informational purposes only and may not reflect Geistlich’s official position, opinion, or recommendation. Treatment decisions are made at the physician’s discretion, based on the unique needs of each patient.
GEM 21S® has not been approved by FDA for use in ridge augmentation in the US and the safety and effectiveness of GEM 21S® for this use has not been established by FDA.
CLINICAL CASE





THE APPROACH
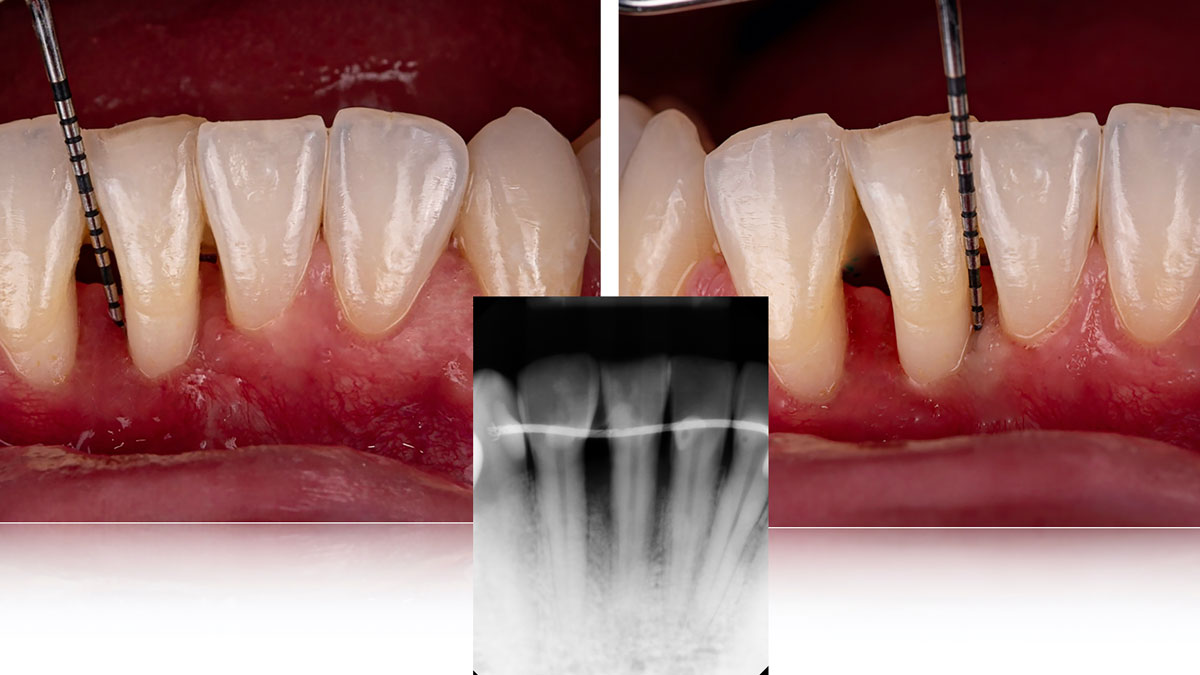
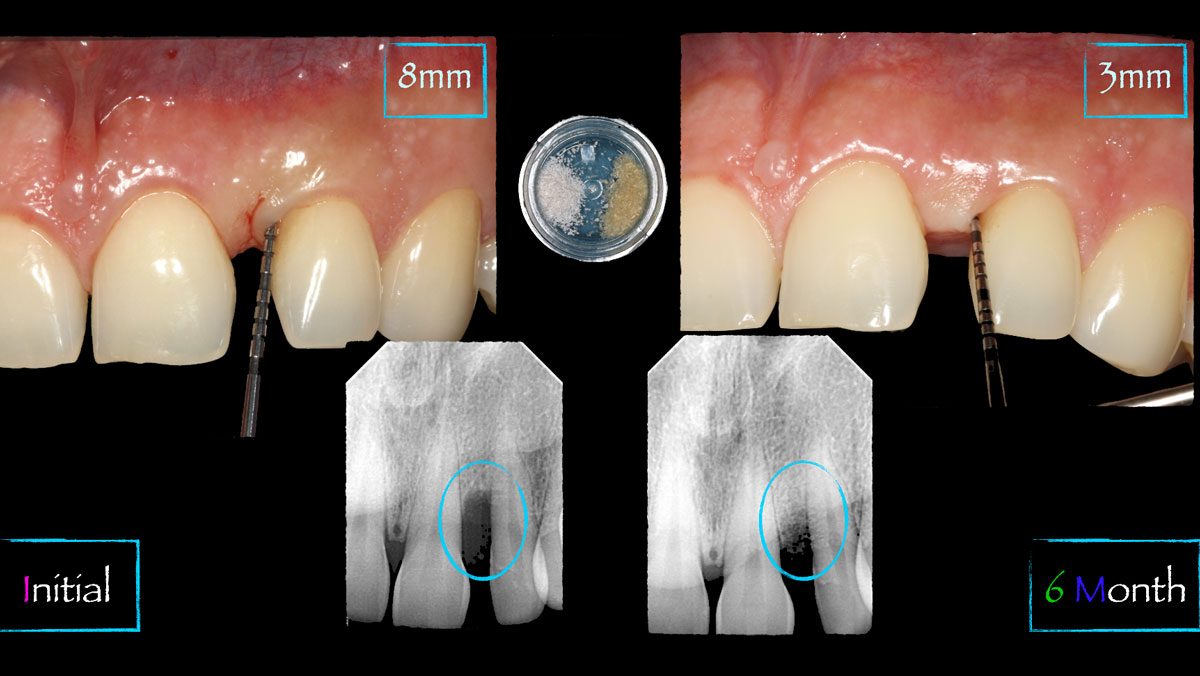
Considering the patient’s age, condition, and good compliance, a regenerative approach was chosen to preserve all teeth. Due to the extent and severity of the defect, a bone graft, biologics, and a membrane were utilized. The goal was to restore lost attachment and stabilize the teeth through splinted therapy.
THE OUTCOME
At the 7-month follow-up, probing depths decreased from 7 mm (MB, DB) to 3 mm, with radiographic bone fill indicating a 90% success. Attachment gain of 3 mm was achieved, improving from 7 mm to 4 mm. The patient reported satisfactory outcomes, and splinting effectively maintained tooth stability with no mobility.
Disclaimer: These results are not guaranteed; individual outcomes may vary depending on patient circumstances. This information is for informational purposes only and may not reflect Geistlich’s official position, opinion, or recommendation. Treatment decisions are made at the physician’s discretion, based on the unique needs of each patient.
CLINICAL CASE




THE APPROACH
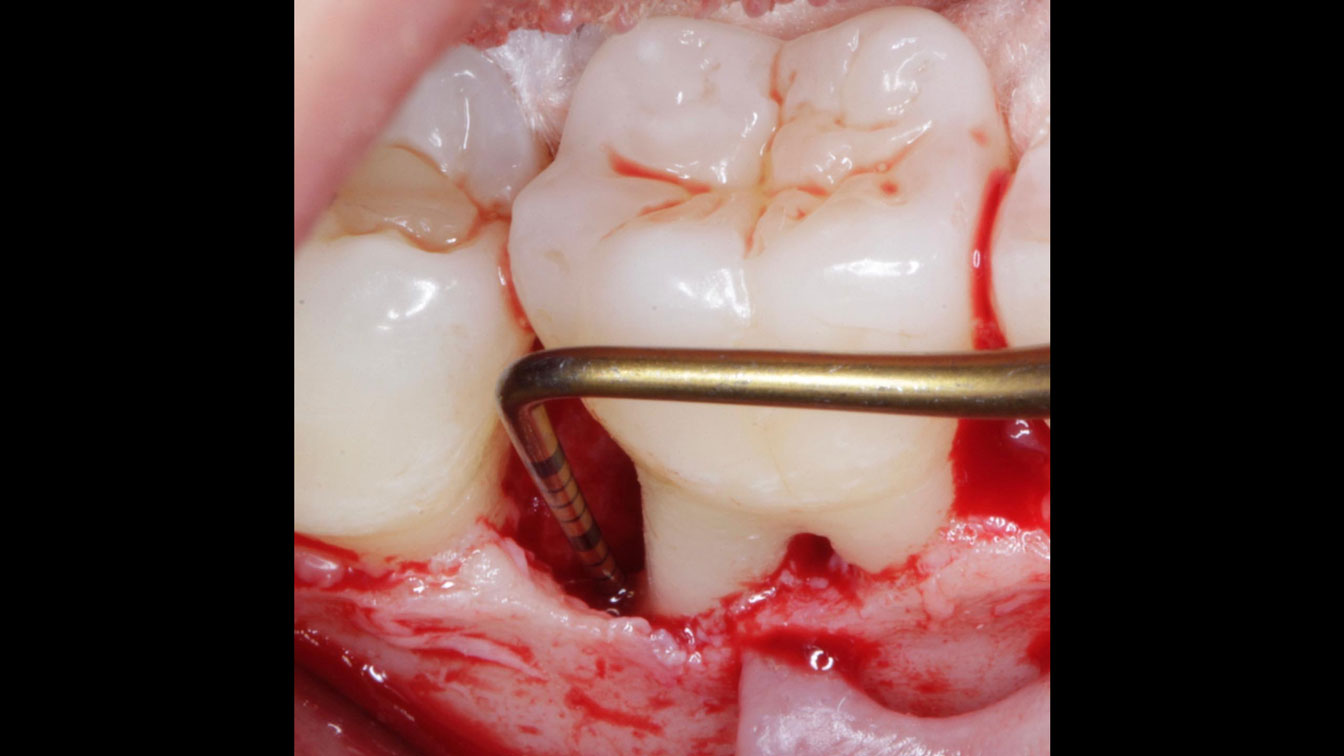
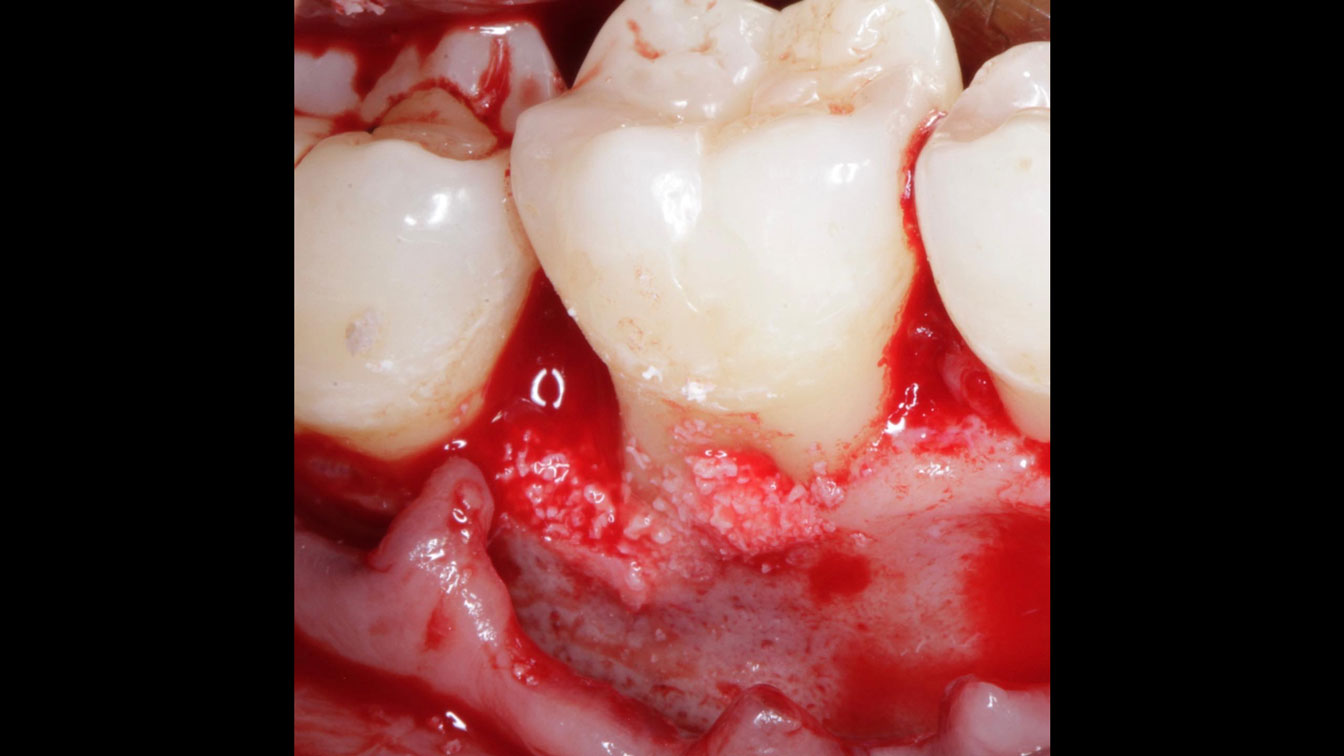
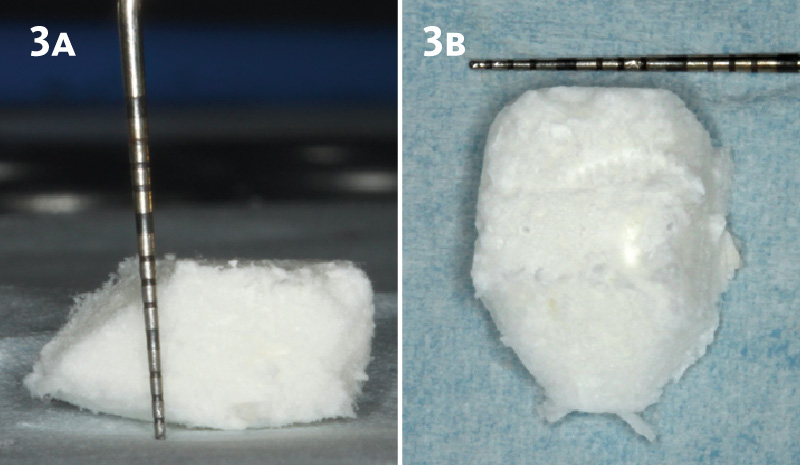
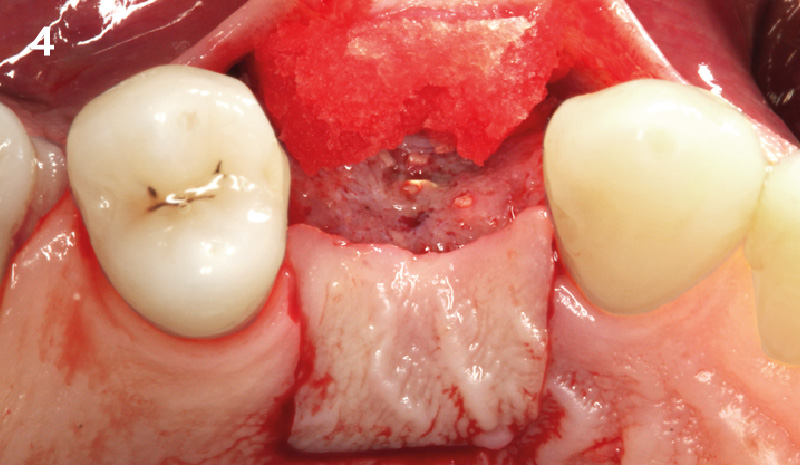
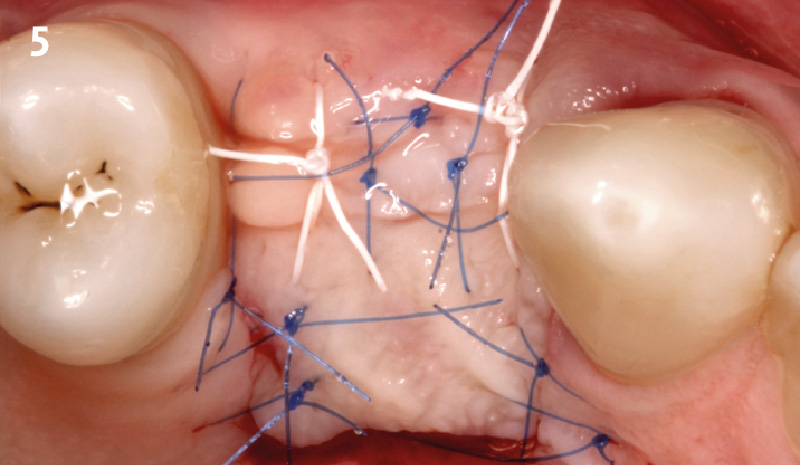
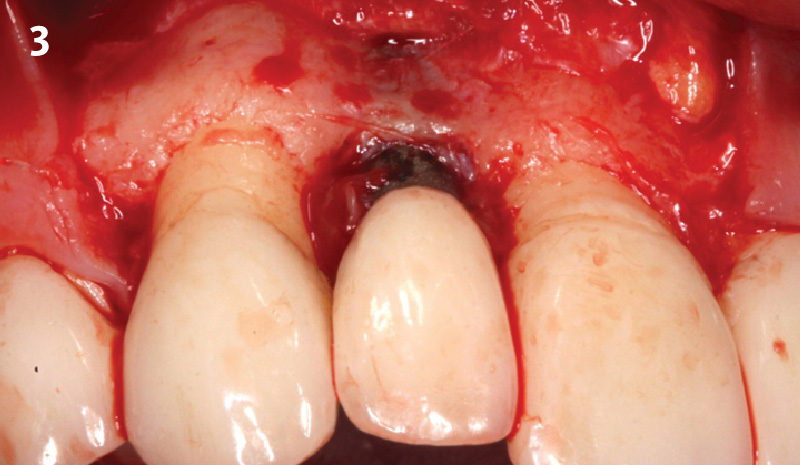
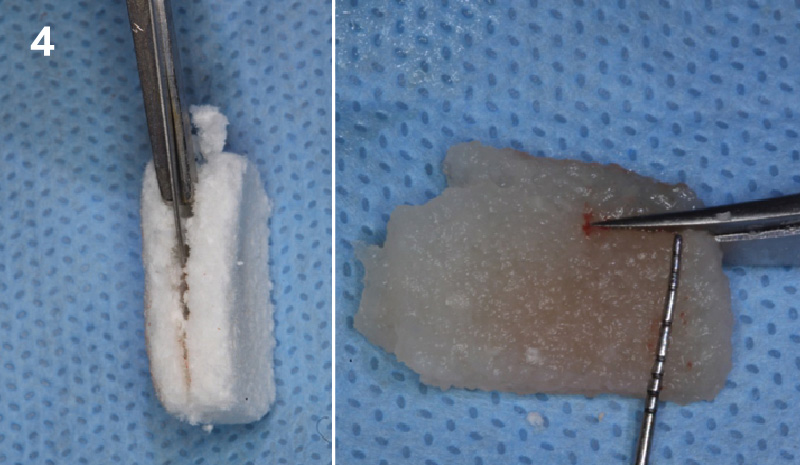
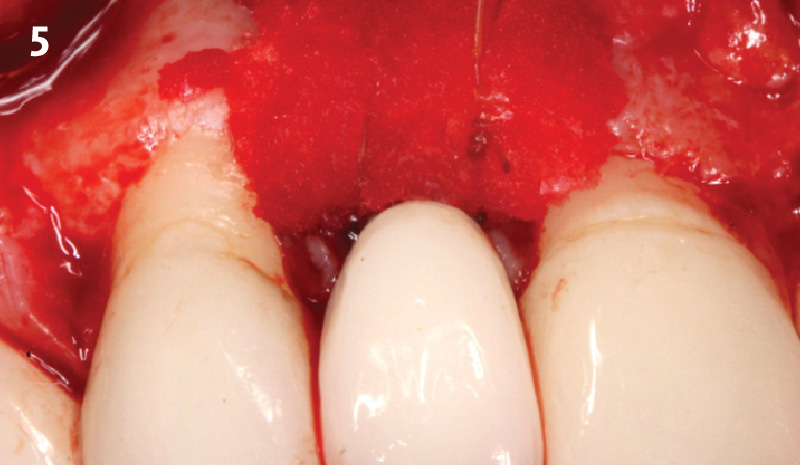
Following flap elevation and thorough defect debridement, a xenograft bone substitute mixed with PDGF (GEM 21S®) was used to fill the defect. The graft was left uncovered without a membrane.
THE OUTCOME
The 1-year follow-up radiograph demonstrated near-complete bone fill in a previously deep defect. Clinically, shallow probing depths and healthy tissue were also observed at the 1-year follow-up.
Disclaimer: These results are not guaranteed; individual outcomes may vary depending on patient circumstances. This information is for informational purposes only and may not reflect Geistlich’s official position, opinion, or recommendation. Treatment decisions are made at the physician’s discretion, based on the unique needs of each patient.
CLINICAL CASE





THE APPROACH
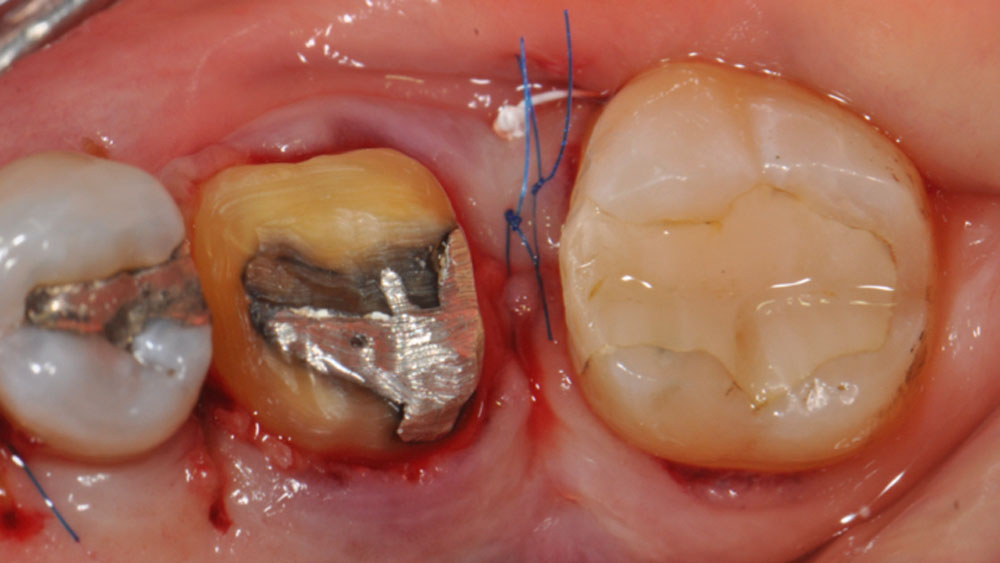
The crown was biologically shaped, and the root surface was detoxified using Ellman burs. Following flap elevation and thorough defect debridement, an allograft mixed with GEM 21S® was used to fill the defect. The graft was then covered with Geistlich Bio-Gide®.
THE OUTCOME
At the 10-month follow-up, radiographs revealed evidence of bone fill, and clinically, the interdental tissue showed signs of maturation. At the 9-year follow-up, clinical photos demonstrated long-term stability, with maintained bone levels, minimal interproximal recession, and lack of facial recession. Radiographic analysis further confirmed the sustained stability of the bone.
Disclaimer: These results are not guaranteed; individual outcomes may vary depending on patient circumstances. This information is for informational purposes only and may not reflect Geistlich’s official position, opinion, or recommendation. Treatment decisions are made at the physician’s discretion, based on the unique needs of each patient.

WEBINAR
Sorry, you do not have permission to view this content.

BIOBRIEF
The Buccal Pedicle Flap for Peri-Implant Soft Tissue Volume


THE SITUATION
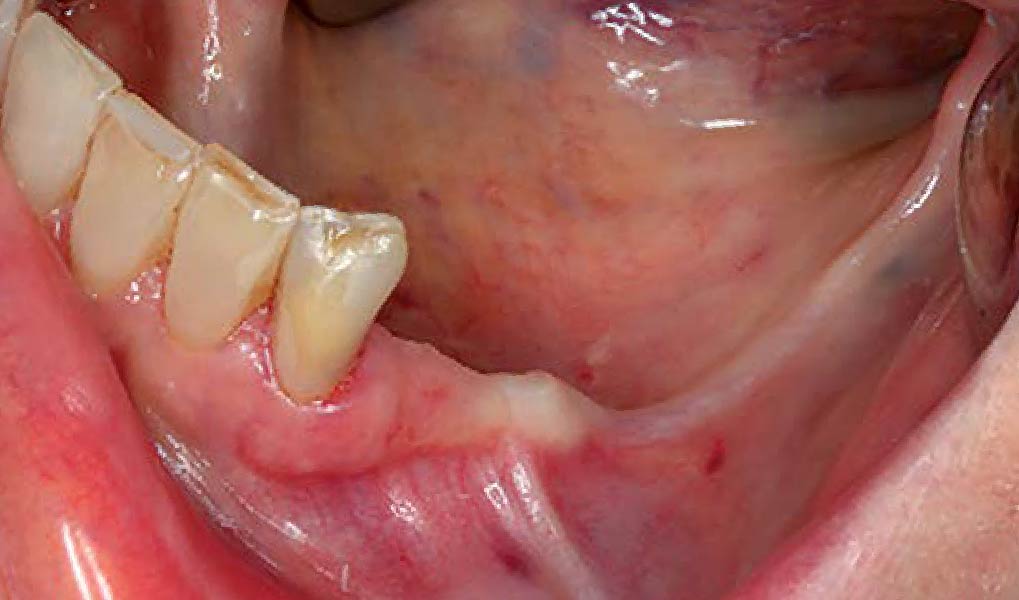
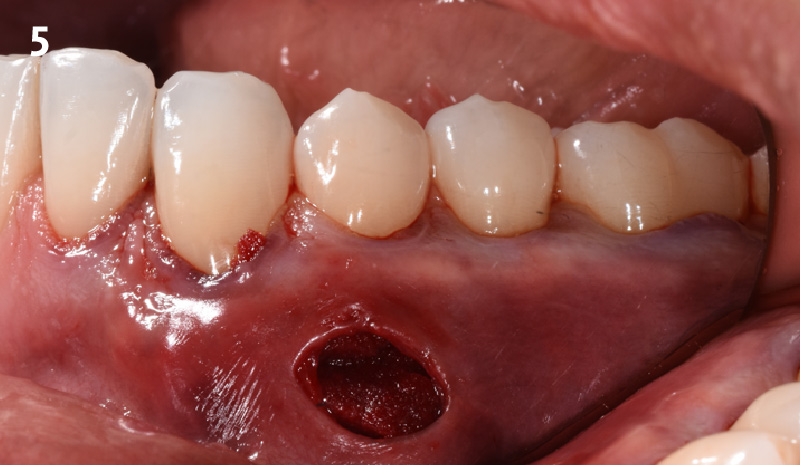
Patient presented with a fistula buccal on tooth #9 associated with a chronic peri-apical lesion and external root resorption. Also tooth #8 showed a chronic peri-apical lesion. Her chief complaint was the misalignment of her teeth. The clinical situation revealed the presence of bleeding upon probing and generalized moderate periodontal disease (Stage II, Grade I) as well as multiple endodontic failures.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system | Light smoker | Impaired immune system |
| Patient’s esthetic requirements | Low | Medium | High |
| Height of smile line | Low | Medium | High |
| Gingival biotype | Thick – “low scalloped” | Medium – “medium scalloped” | Thin – “high scalloped” |
| Shape of dental crowns | Rectangular | Triangular | |
| Infection at implant sight | None | Chronic | Acute |
| Bone height at adjacent tooth site | ≤ 5 mm from contact point | 5.5 – 6.5 mm from contact point | ≥ 7 mm from contact point |
| Restorative status of adjacent tooth | Intact | Restored | |
| Width of tooth gap | 1 tooth (≥ 7 mm) | 1 tooth (≤ 7 mm) | 2 teeth or more |
| Soft-tissue anatomy | Intact | Compromised | |
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
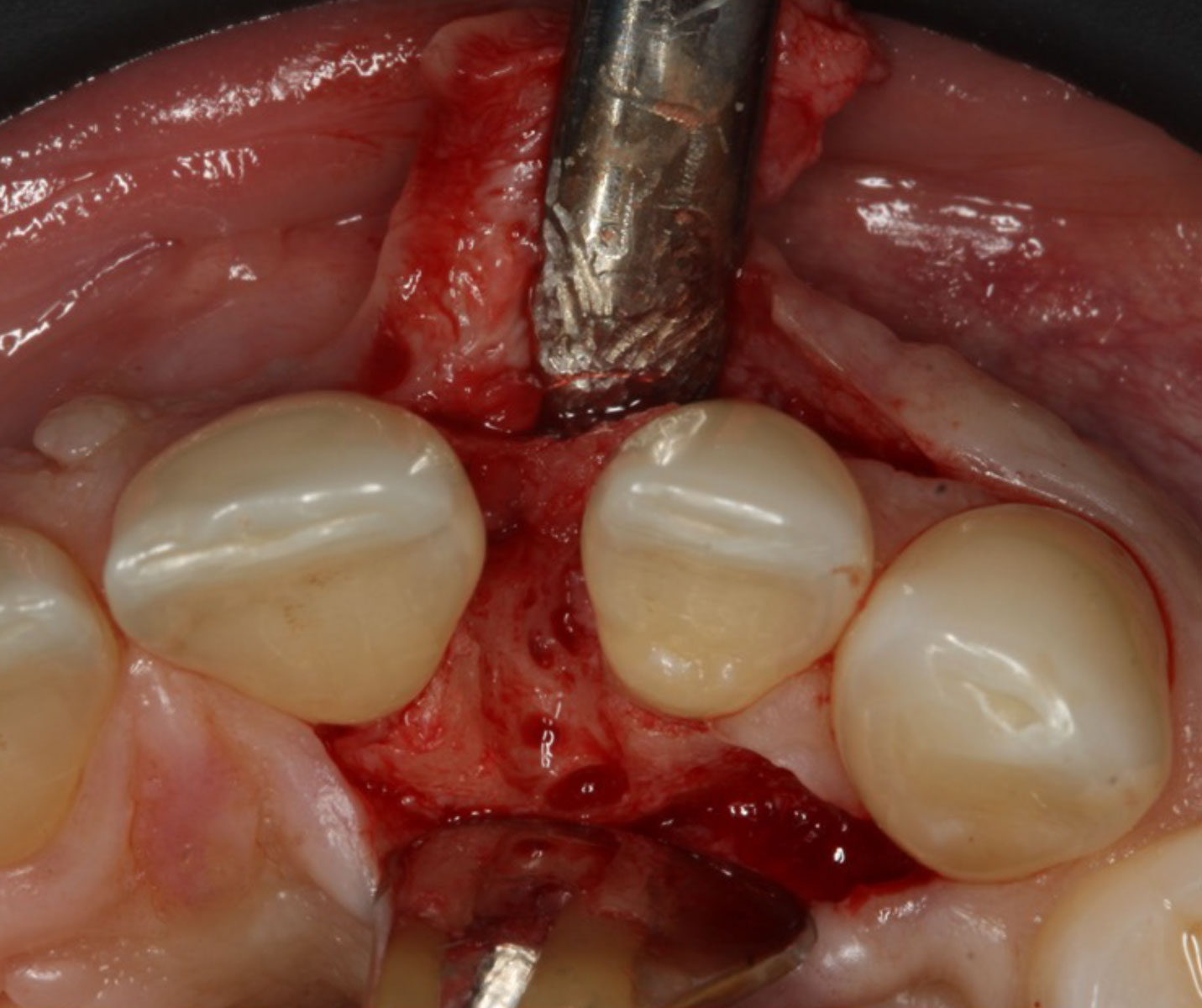
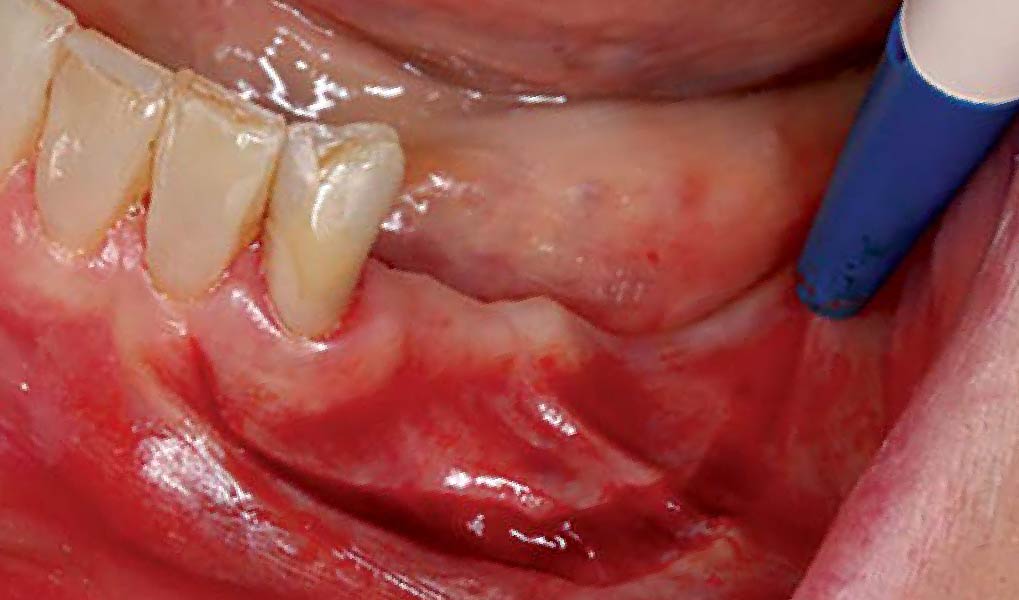
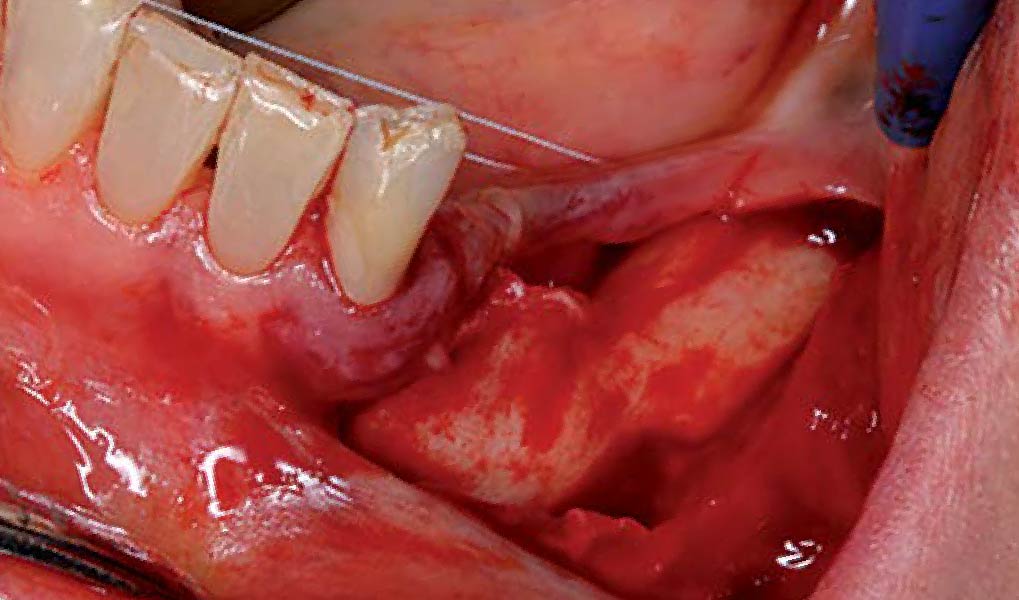
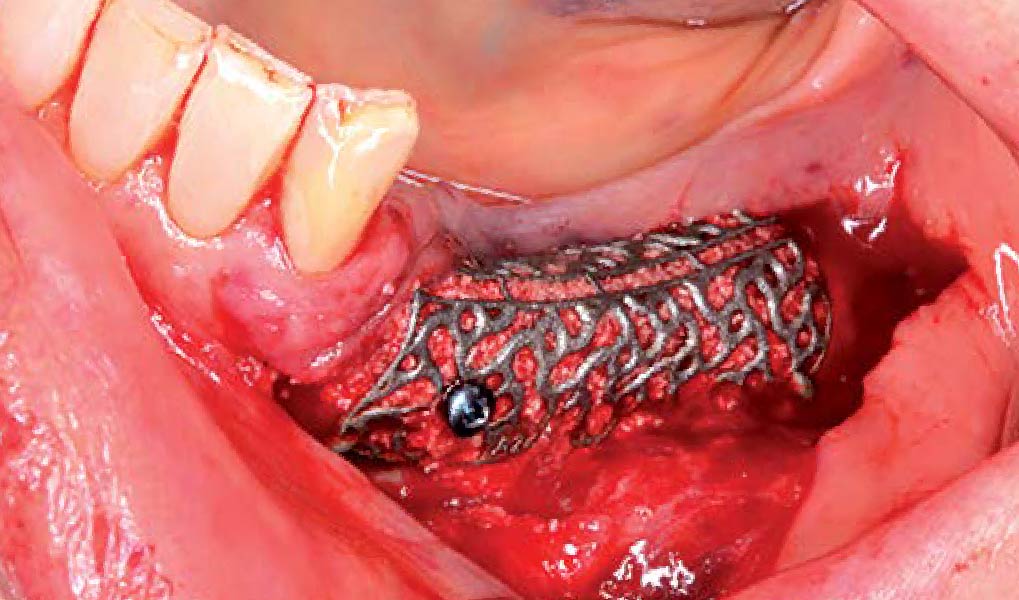
THE APPROACH
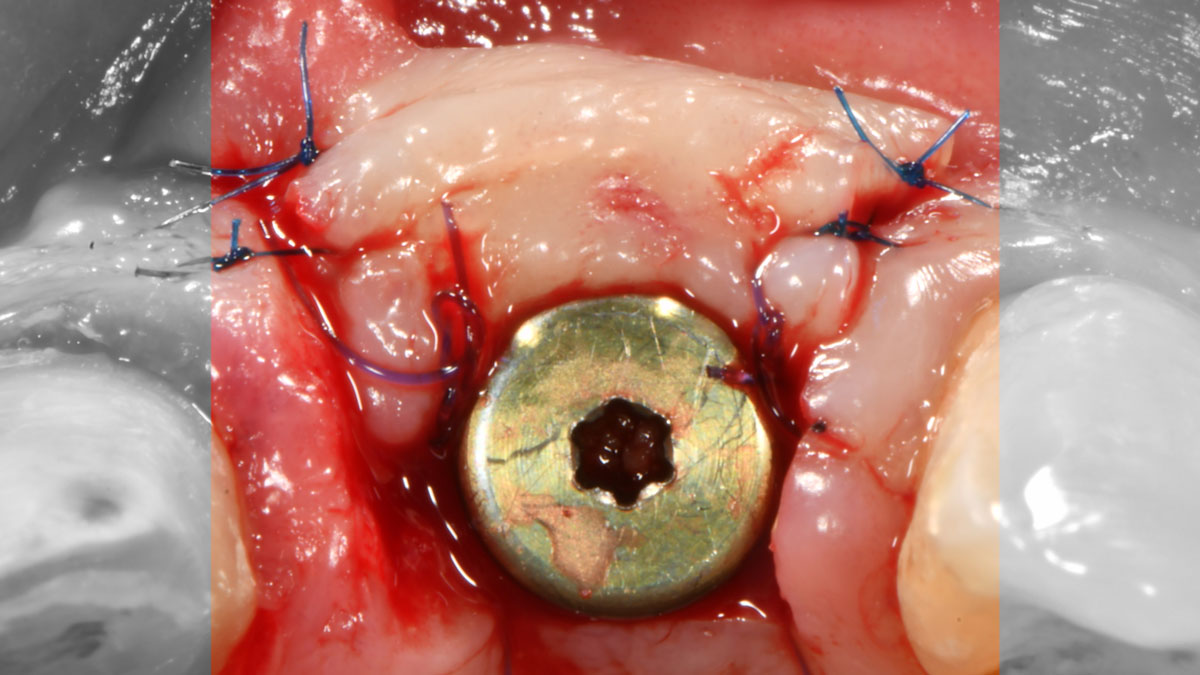
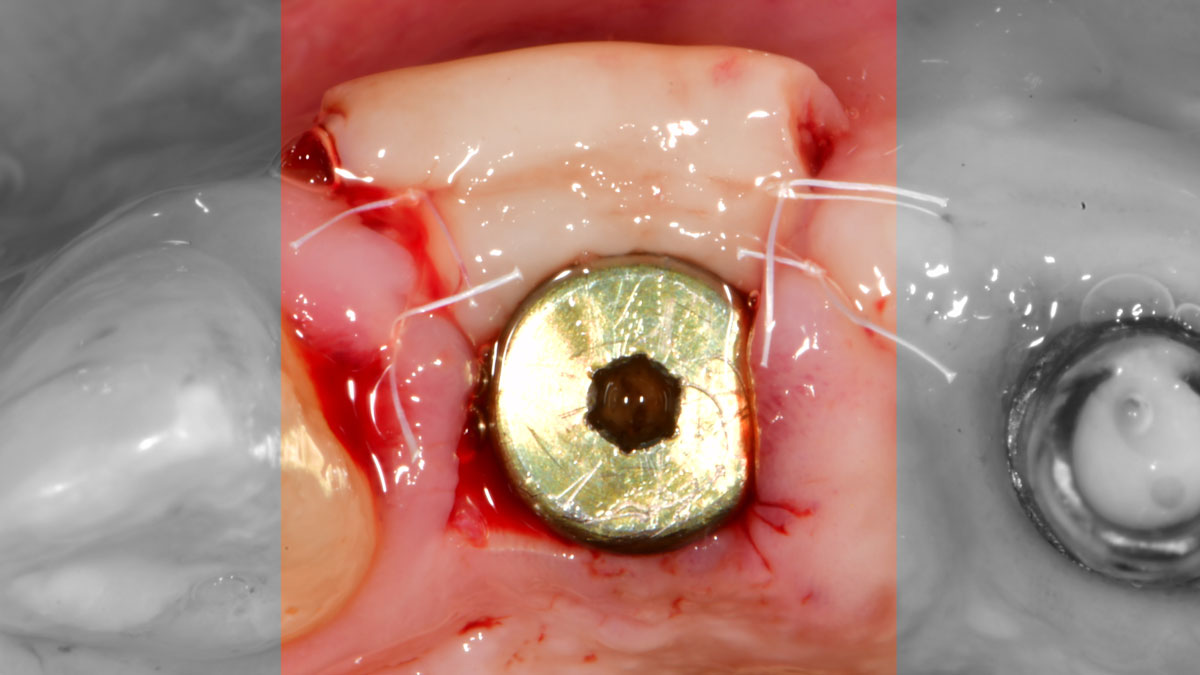
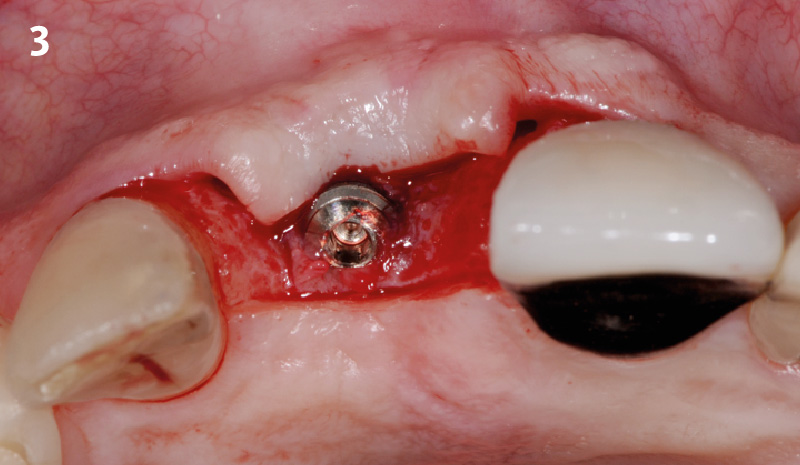
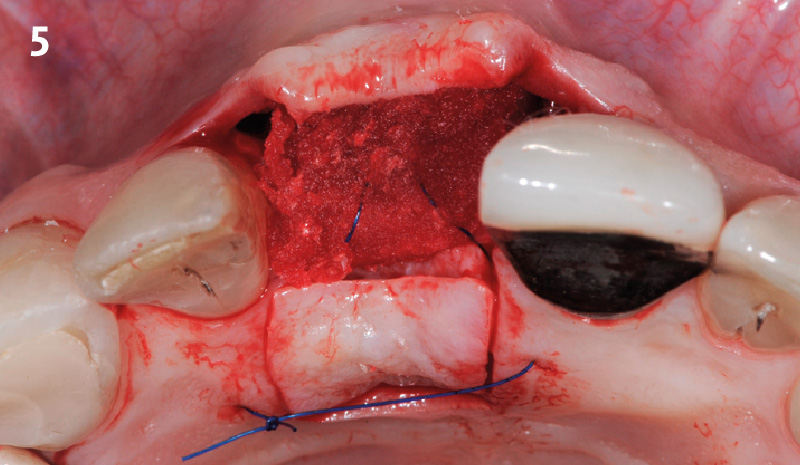
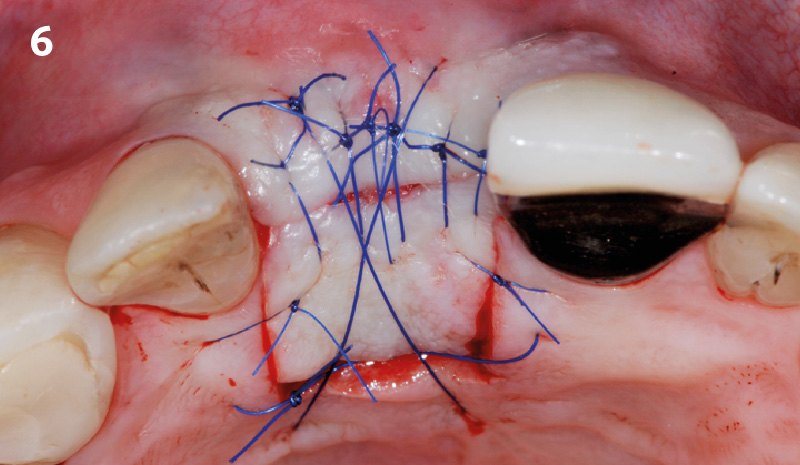
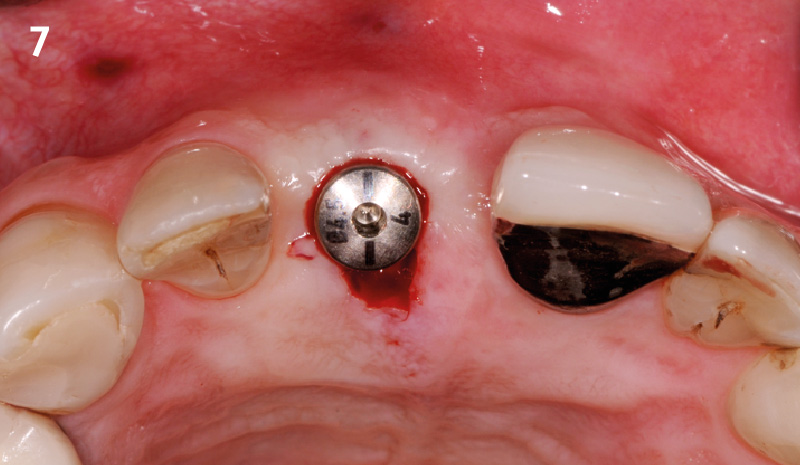
The aim of the treatment is to eradicate periodontal disease and restore esthetics and function. Treatment planning: non-surgical and surgical periodontal treatment, orthodontic alignment, extraction of both central incisors, immediate implant placement and Guided Bone Regeneration with Geistlich Bio-Oss®, peri-implant soft tissue boosting with a buccal pedicle flap and full ceramic CAD-CAM restorations.





“Orthodontic treatment must be postponed because of the presence of periodontal disease. A thin biotype and a high smile line needs to be taken into consideration.”
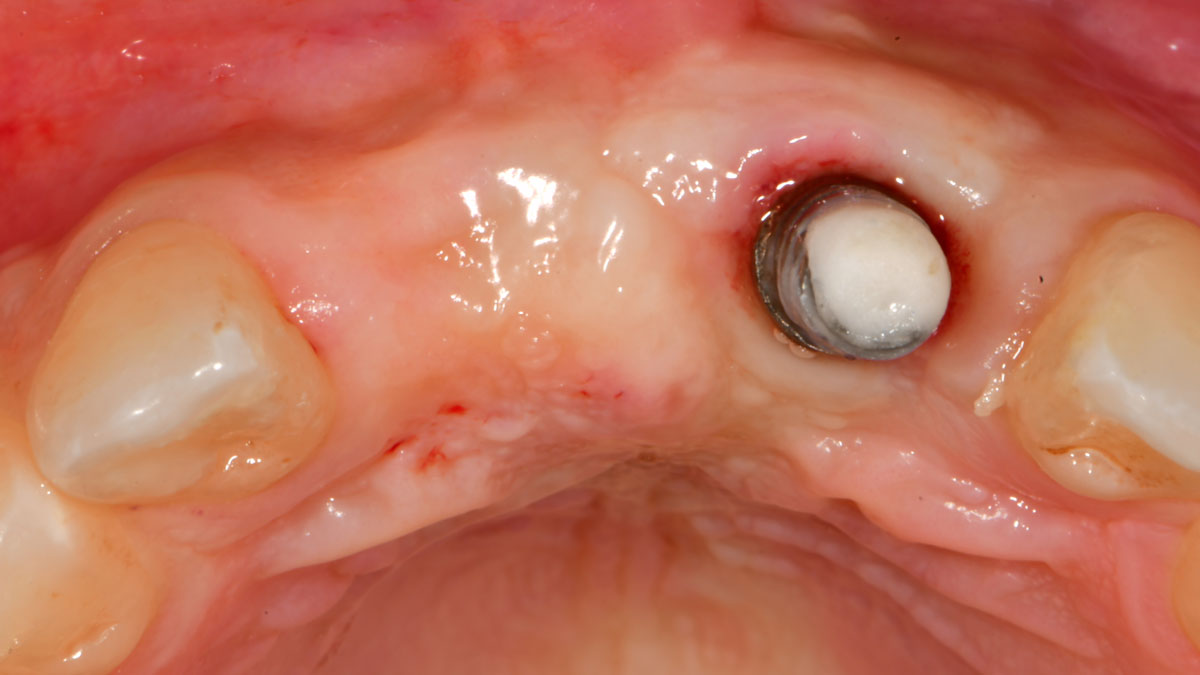
THE OUTCOME
The final outcome at 8 weeks is showing pink esthetics as well as biomimetics and function. The use of the buccal pedicle flap allowed the increased volume of the peri-implant mucosa with a minimally invasive approach. The combination of Geistlich Fibro-Gide® and a buccal pedicle flap had the main advantage of reducing the morbidity generally associated with CT harvesting.
Dr. Giorgio Tabanella
Dr. Tabanella is a Diplomate of the American Board of Periodontology, an Active Member of the Italian Academy of Esthetic Dentistry and author of the book “Retreatment of Failures in Dental Medicine”. He graduated from the University of Southern California, Los Angeles, USA where he obtained his Certificate in Periodontics as well as a Master of Science in Craniofacial Biology. He is Director of O.R.E.C. – Oral Reconstruction and Education Center (www.tabanellaorec.com), reviewer and author of original articles.
BIOBRIEF
Use of Geistlich Fibro-Gide® for Correction of Maxillary Anterior Soft Tissue Peri-implant Ridge Deficiencies


THE SITUATION
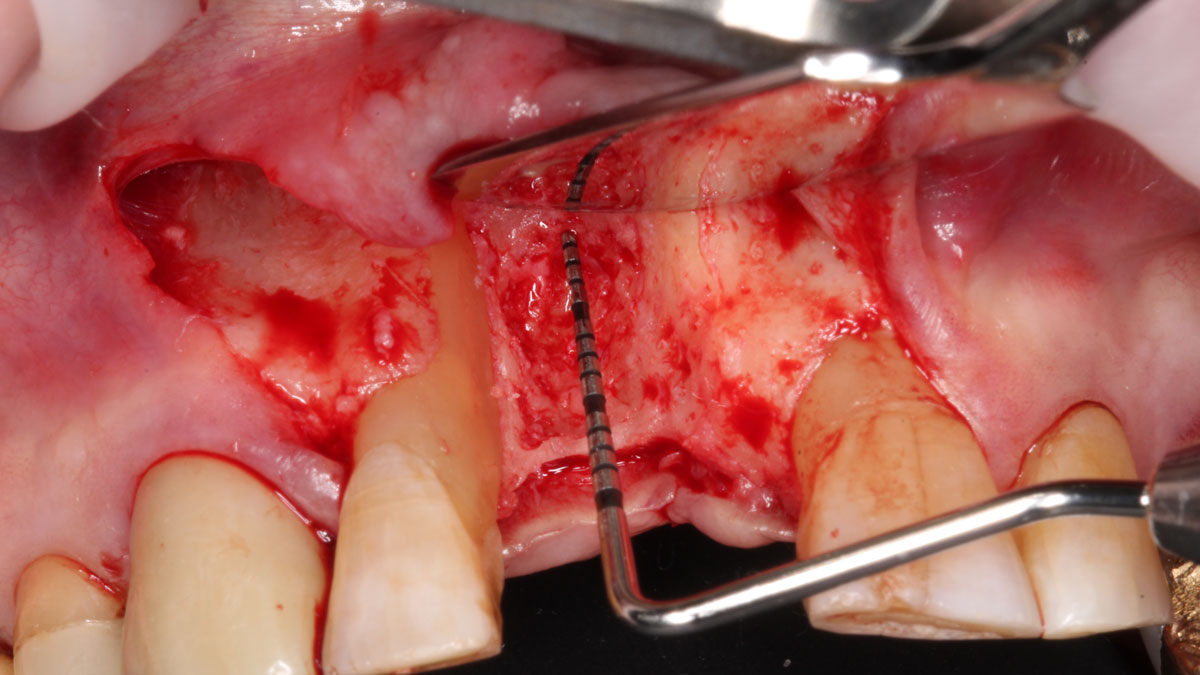
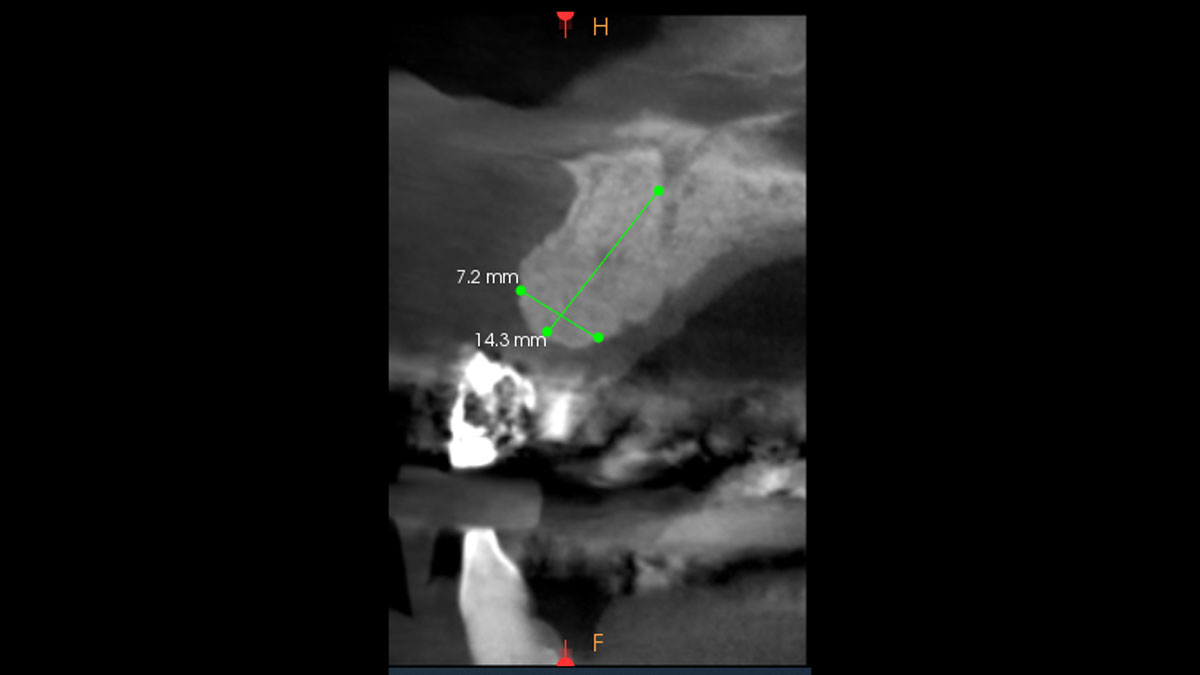
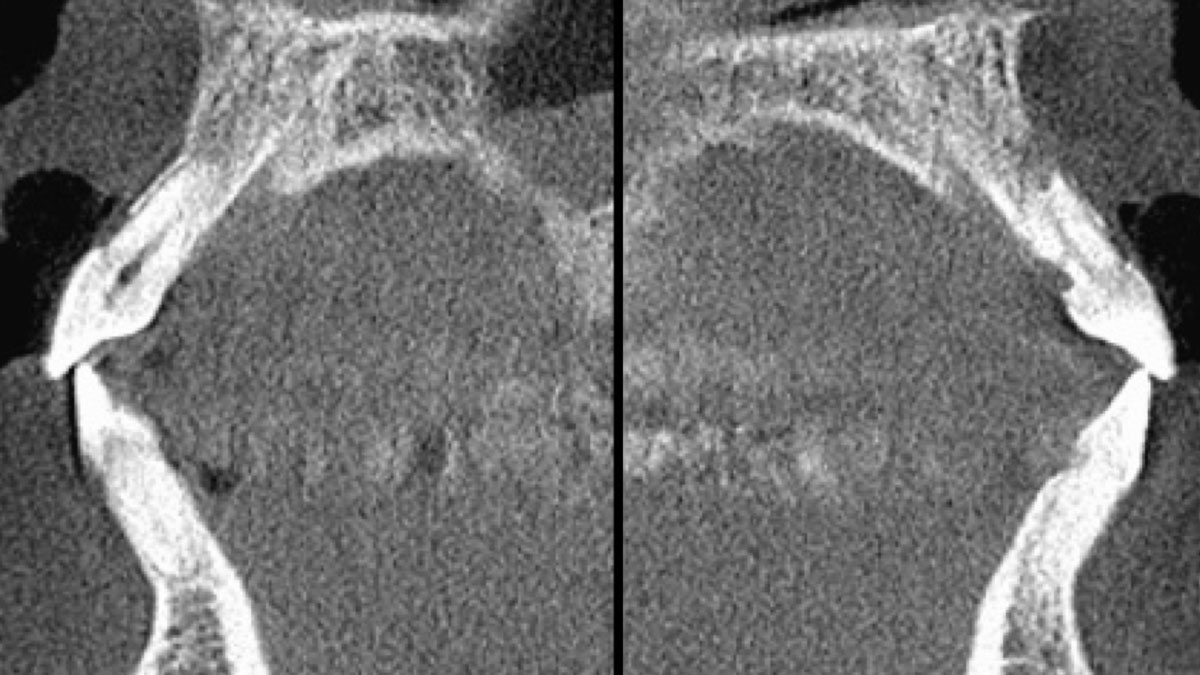
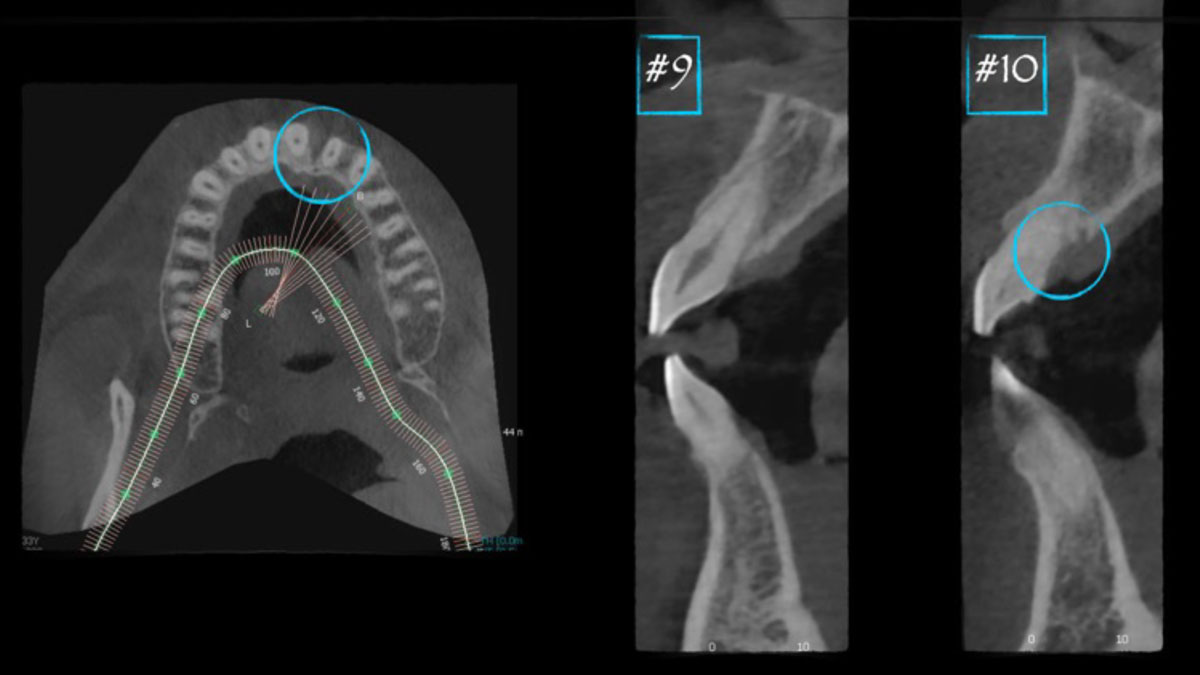
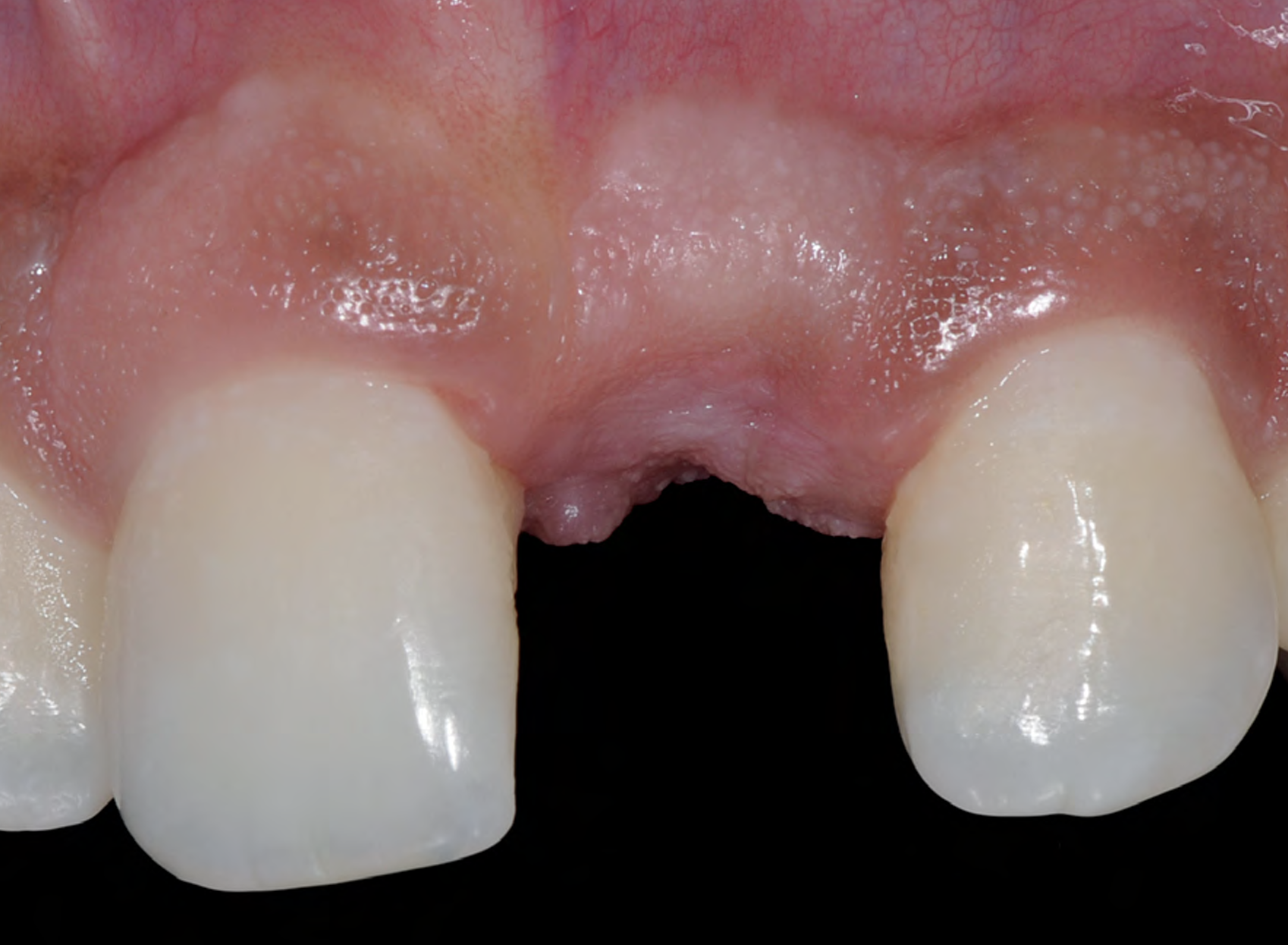
A 27-year-old female with congenitally missing maxillary lateral incisors was referred for implant placement. Following completion of orthodontics, a plan was developed to place dental implants at the #7 and #10 positions. Based on CBCT evaluation, alveolar ridge height and width was deemed sufficient for implant placement. Despite sufficient bone volume, facial ridge volume deficiencies were noted at both edentulous sites, requiring augmentation to allow for optimal esthetics.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system | Light smoker | Impaired immune system |
| Patient’s esthetic requirements | Low | Medium | High |
| Height of smile line | Low | Medium | High |
| Gingival biotype | Thick – “low scalloped” | Medium – “medium scalloped” | Thin – “high scalloped” |
| Shape of dental crowns | Rectangular | Triangular | |
| Infection at implant sight | None | Chronic | Acute |
| Bone height at adjacent tooth site | ≤ 5 mm from contact point | 5.5 – 6.5 mm from contact point | ≥ 7 mm from contact point |
| Restorative status of adjacent tooth | Intact | Restored | |
| Width of tooth gap | 1 tooth (≥ 7 mm) | 1 tooth (≤ 7 mm) | 2 teeth or more |
| Soft-tissue anatomy | Intact | Compromised | |
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
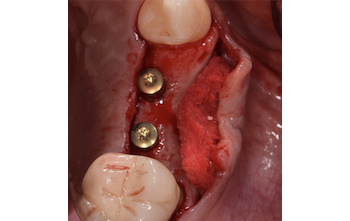
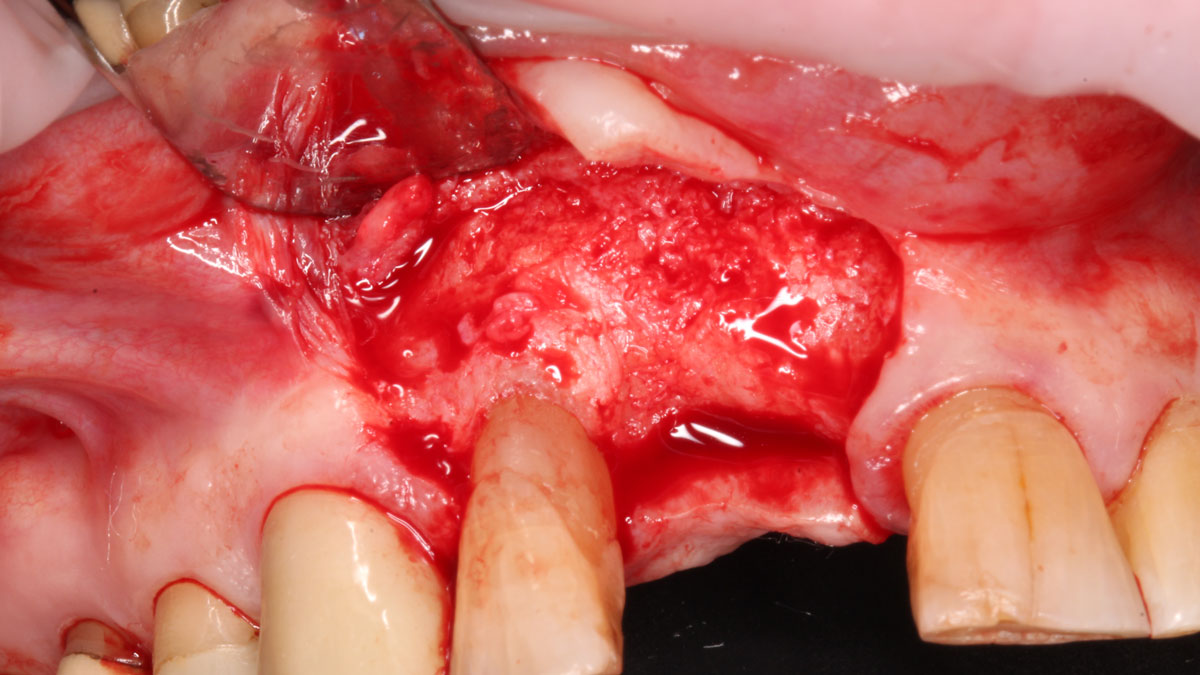
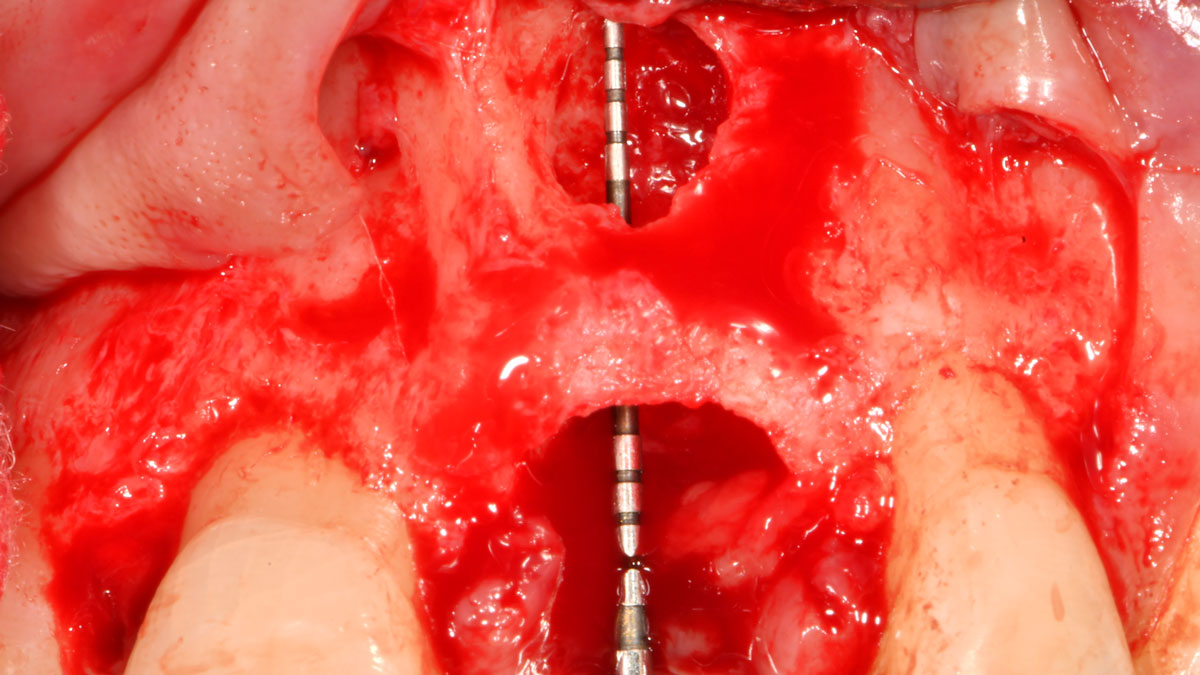
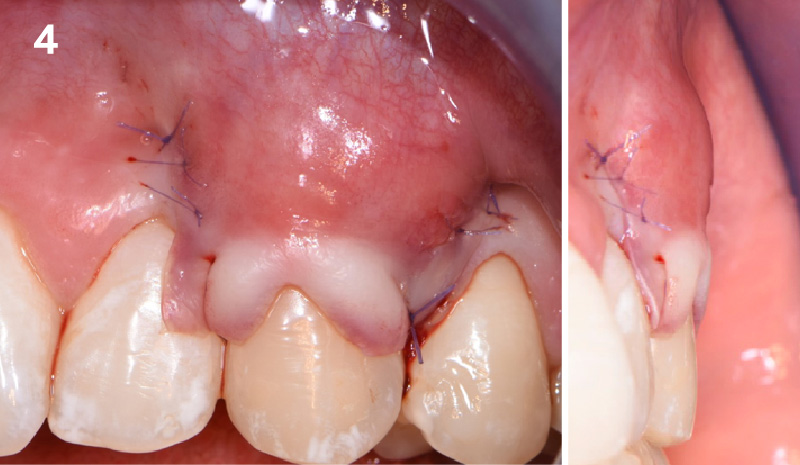
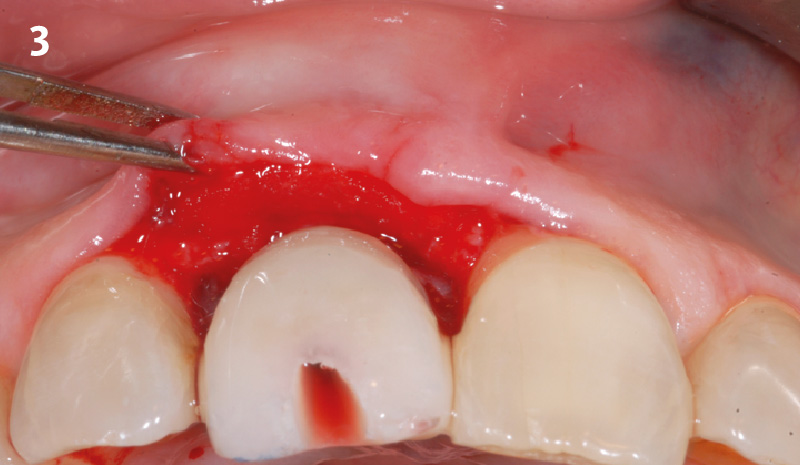
THE APPROACH
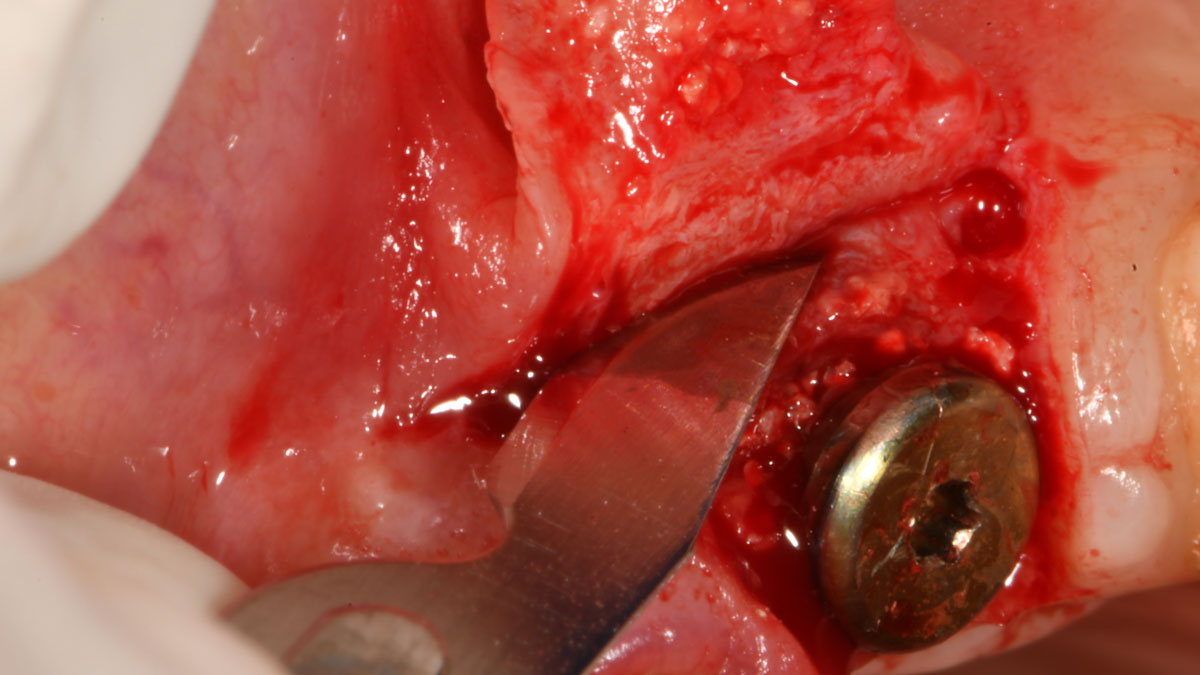
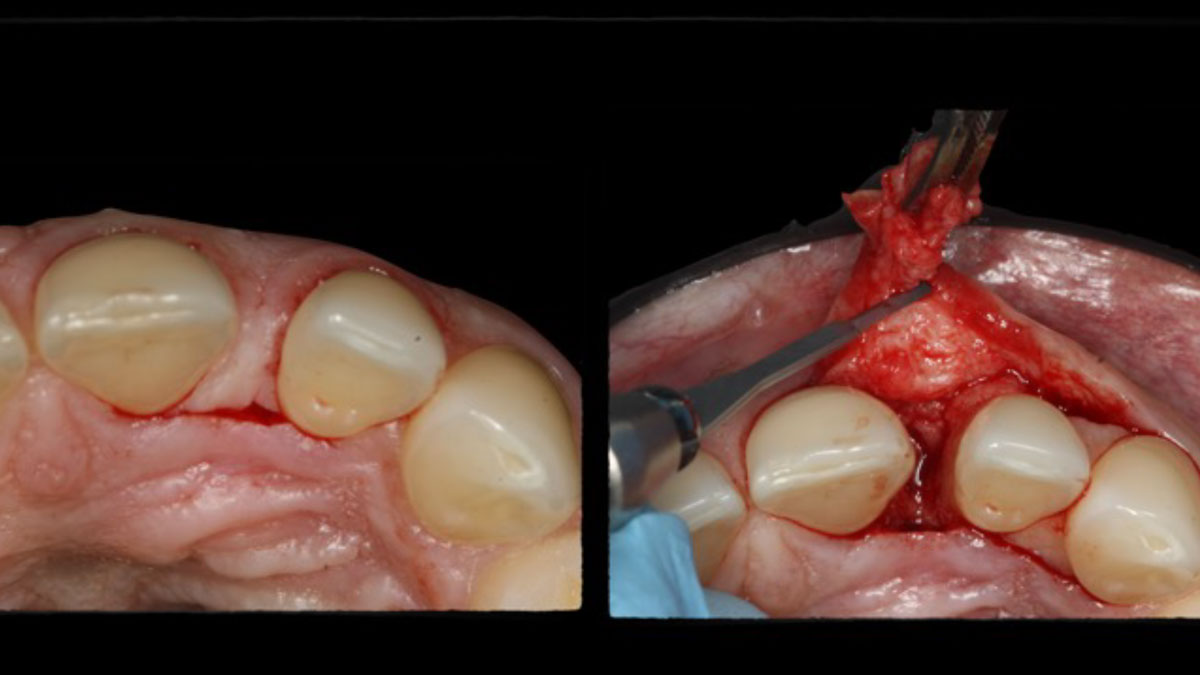
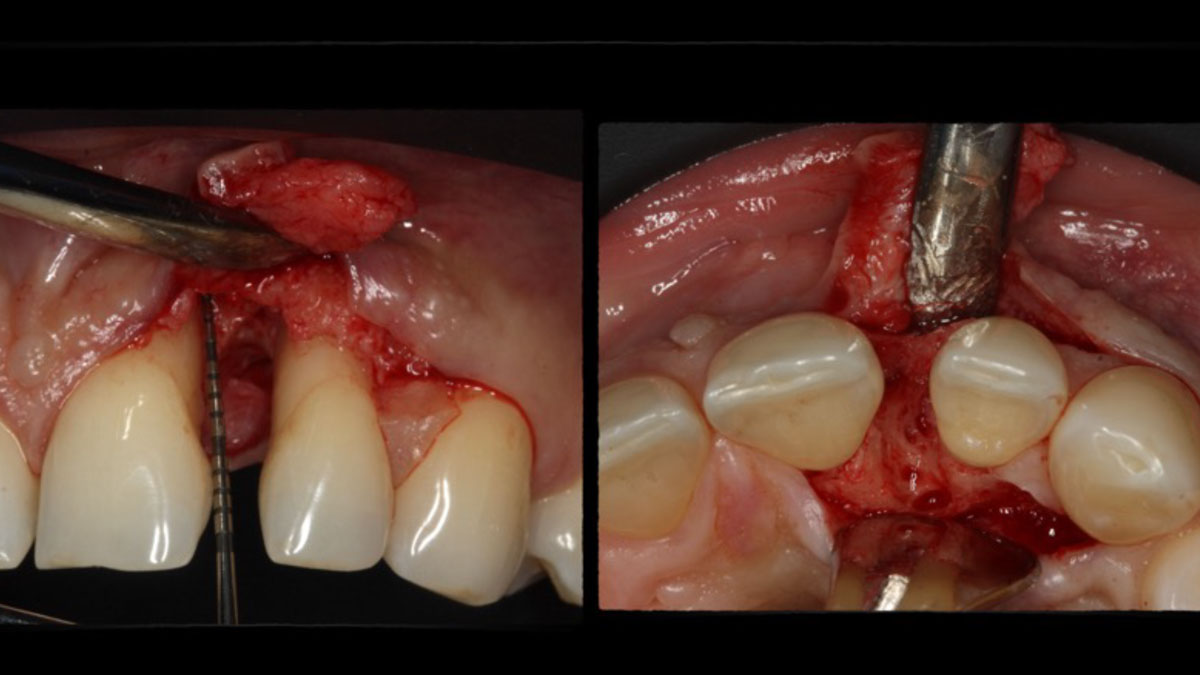
The goal of treatment was to replace missing maxillary lateral incisors with dental implants, while providing an esthetic result with predictable and minimally invasive techniques. Employing a surgical guide for implant placement, implants were placed in precise 3-dimentional positions. The use of xenograft biomaterials (Geistlich Fibro-Gide®) allowed for the augmentation of gingival biotype and elimination of the buccal ridge deficiencies while avoiding the harvesting of autogenous tissue.








“A buccal ridge deficiency with congenitally missing lateral incisors in a high-scallop, high-smile young female patient.”
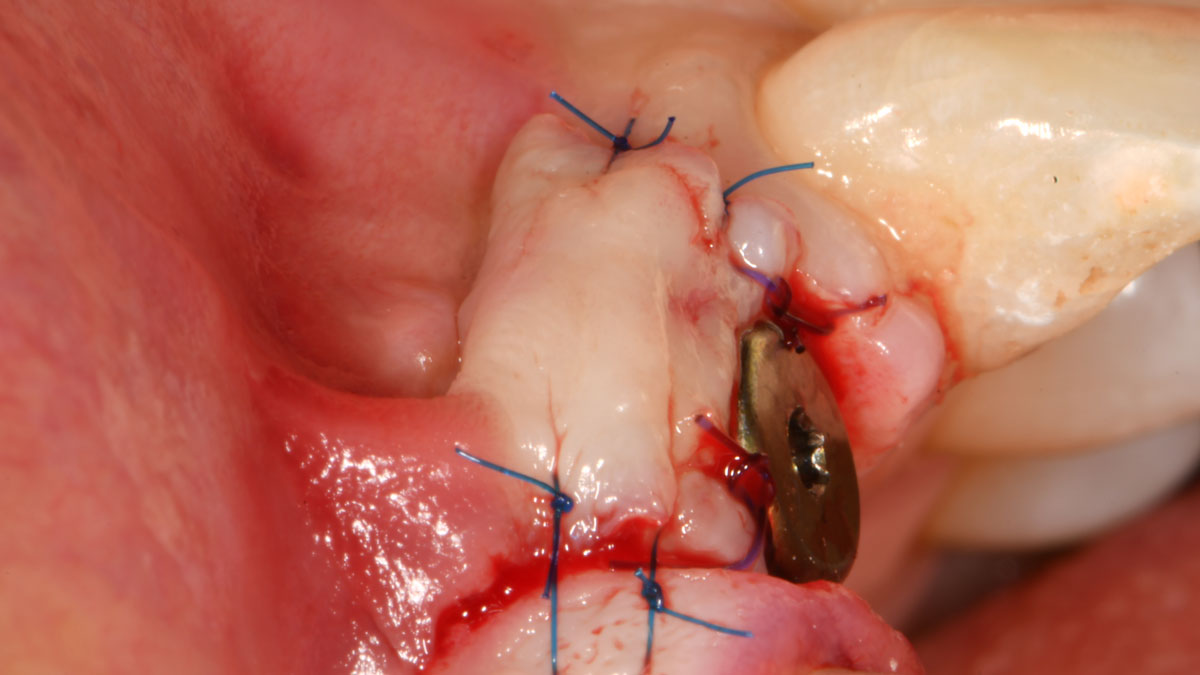
THE OUTCOME
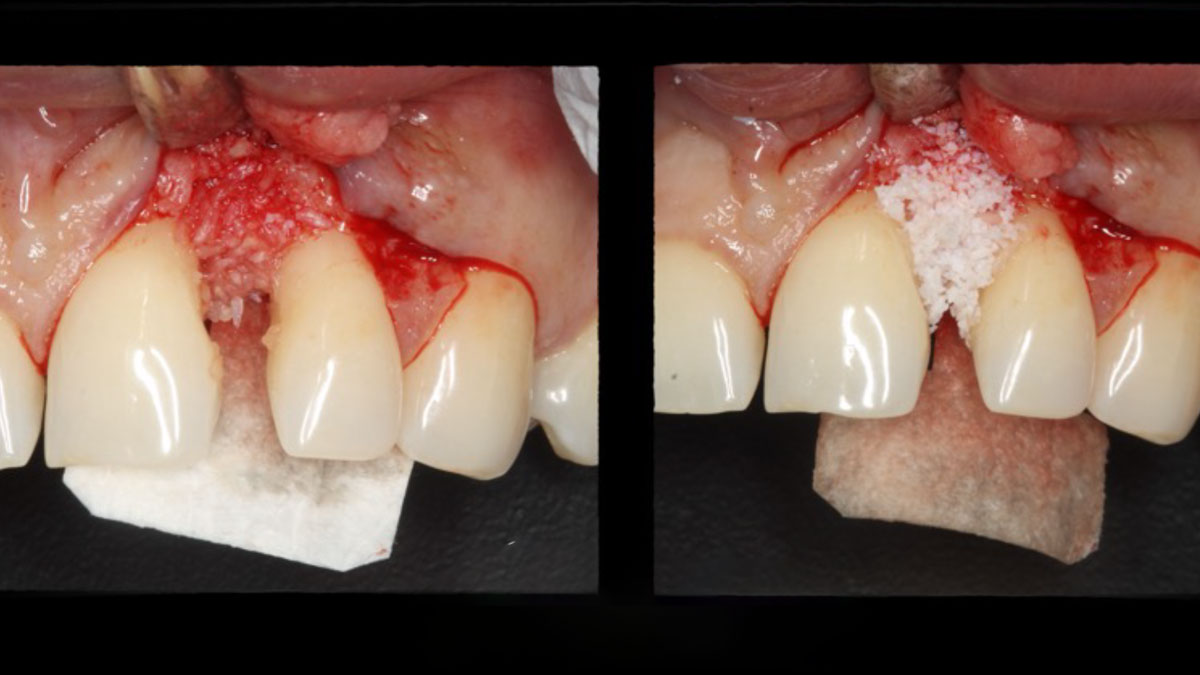
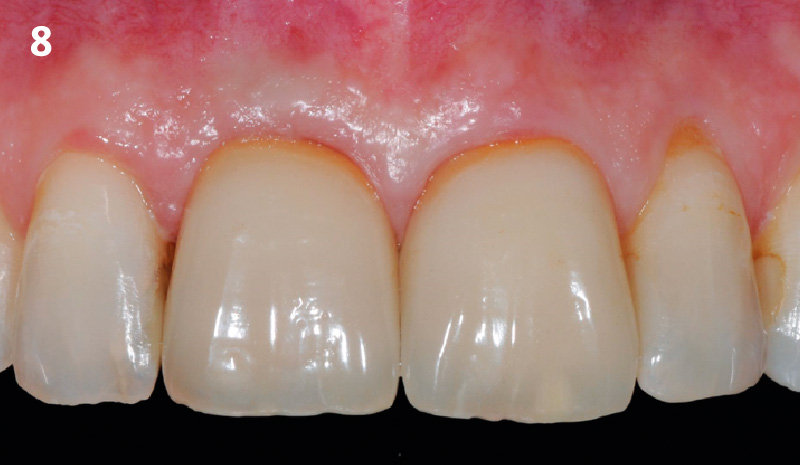
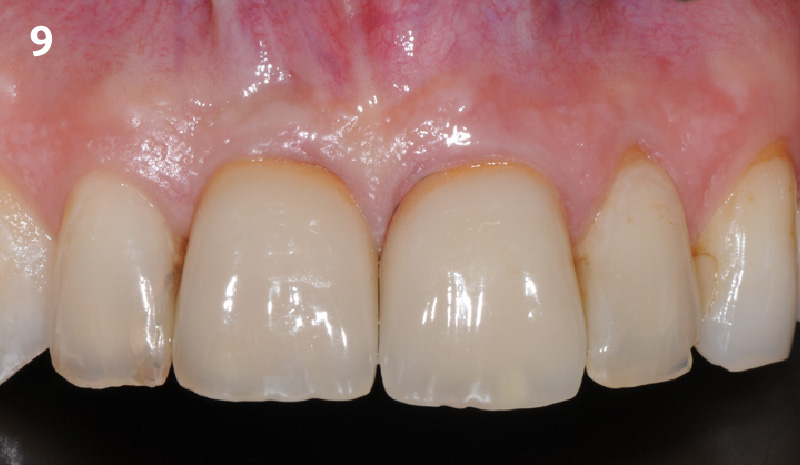
The presented case involves a female patient with congenitally missing maxillary lateral incisors and soft tissue ridge deficiencies. Implants were placed and a volume-stable collagen matrix Geistlich Fibro-Gide® was placed to provide labial soft tissue volume. The tissue emergence was then developed with the use of provisional restorations, one placed at the time of surgery, the other following implant integration. The implants were restored with gingival tissue transformed to mimic convex root emergence.
Dr. Israel Puterman
Dr. Puterman, originally from Montreal Canada, received his DMD from Boston University in 2002 and dual graduate certificates in Implant Dentistry and in Periodontics from Loma Linda University in 2008. He is a published author in various journals including the Journal of Prosthetic Dentistry and the Journal of Prosthodontics. He practices in the Washington, DC area.
BIOBRIEF
Guided Tissue Regeneration in the Esthetic Zone of a 34-Year-Old Male

THE SITUATION
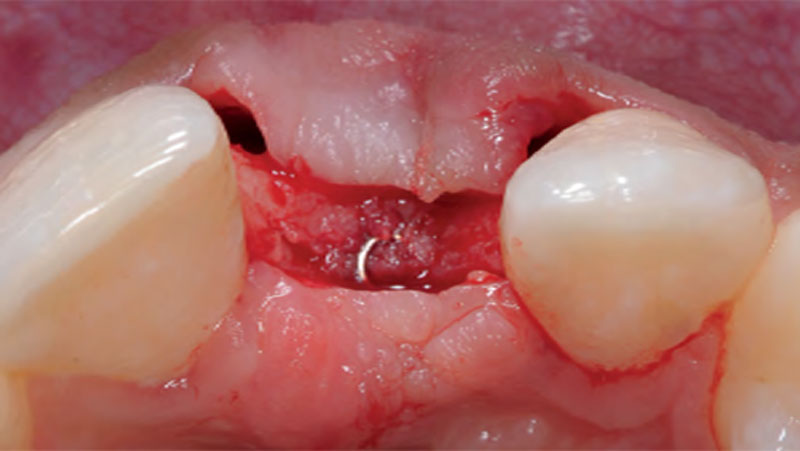
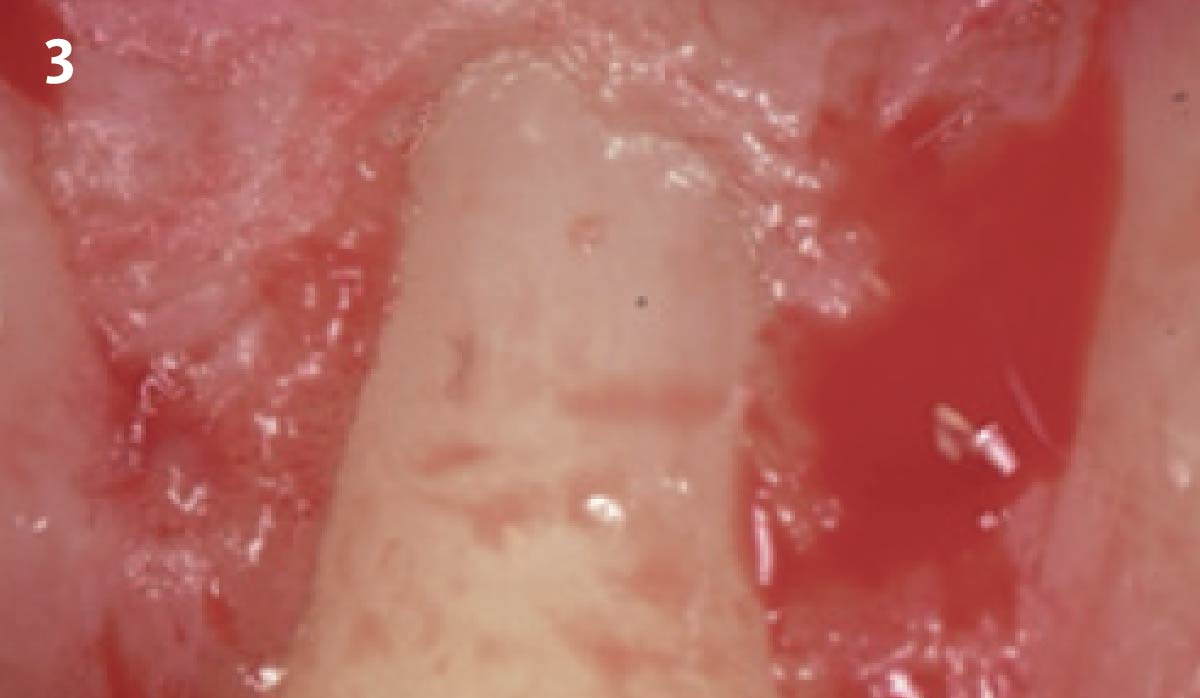
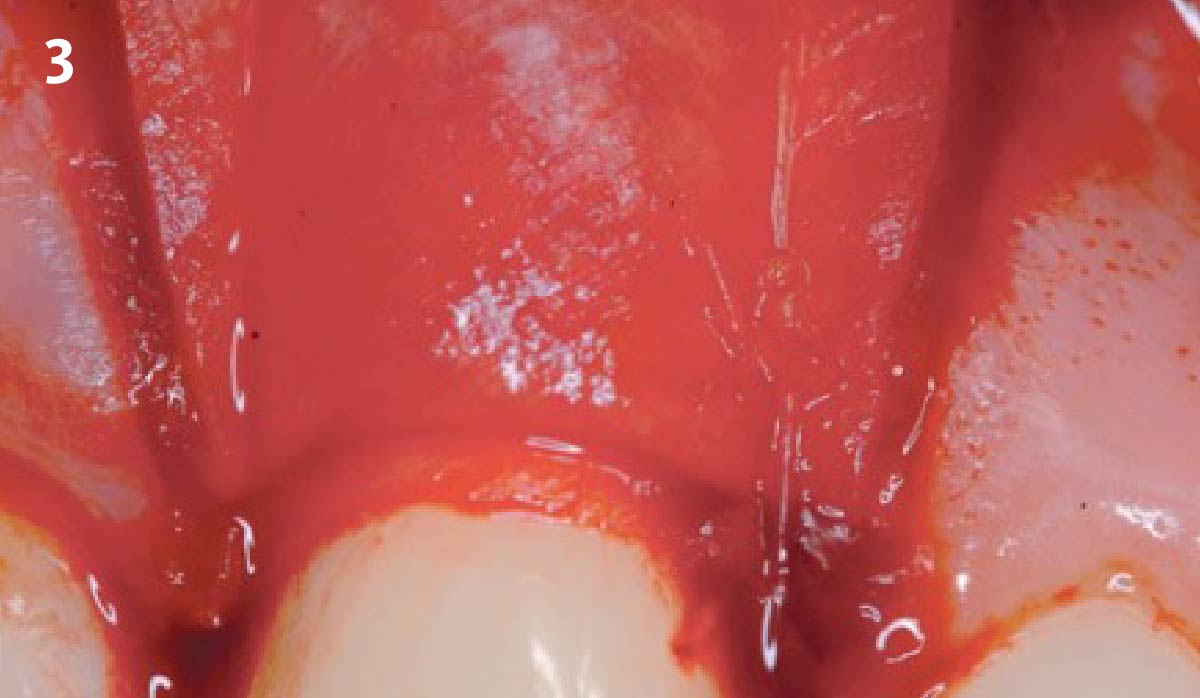
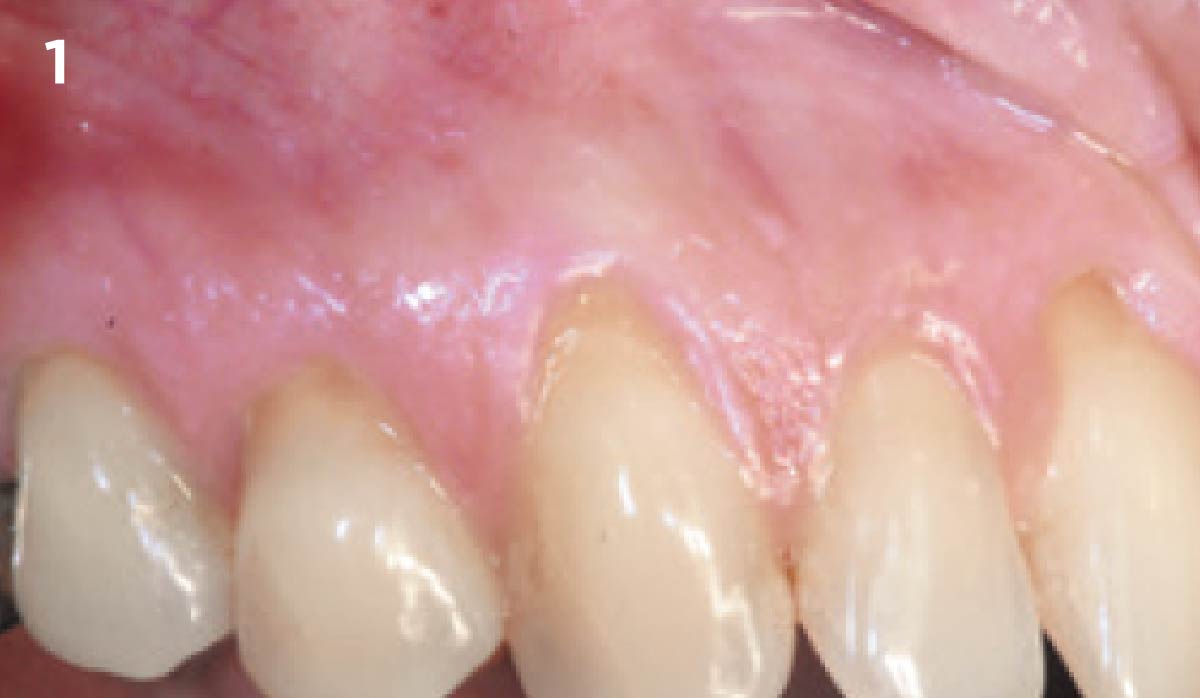
A 34-year-old healthy male presented with increased spacing between maxillary left central and lateral incisors. Clinical examination showed deep probing depths between #9-10 area. Cone-beam computed tomography (CBCT) showed vertical bone loss #9-10 wrapping around the palatal surfaces. Treatment recommendation included guided tissue regeneration (GTR) to stabilize the periodontium.
Area #9-10 was debrided and showed a wide 1-2 wall defect measuring ~7mm vertical bone loss. GTR procedure using Geistlich vallomix™ bone graft (allograft + xenograft) and a collagen membrane were employed and primary closure obtained. Healing at 2 and 4 weeks and 6 months showed proper bone fill with stable periodontium.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system | Light smoker | Impaired immune system |
| Patient’s esthetic requirements | Low | Medium | High |
| Height of smile line | Low | Medium | High |
| Gingival biotype | Thick – “low scalloped” | Medium – “medium scalloped” | Thin – “high scalloped” |
| Shape of dental crowns | Rectangular | Triangular | |
| Infection at implant sight | None | Chronic | Acute |
| Bone height at adjacent tooth site | ≤ 5 mm from contact point | 5.5 – 6.5 mm from contact point | ≥ 7 mm from contact point |
| Restorative status of adjacent tooth | Intact | Restored | |
| Width of tooth gap | 1 tooth (≥ 7 mm) | 1 tooth (≤ 7 mm) | 2 teeth or more |
| Soft-tissue anatomy | Intact | Compromised | |
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
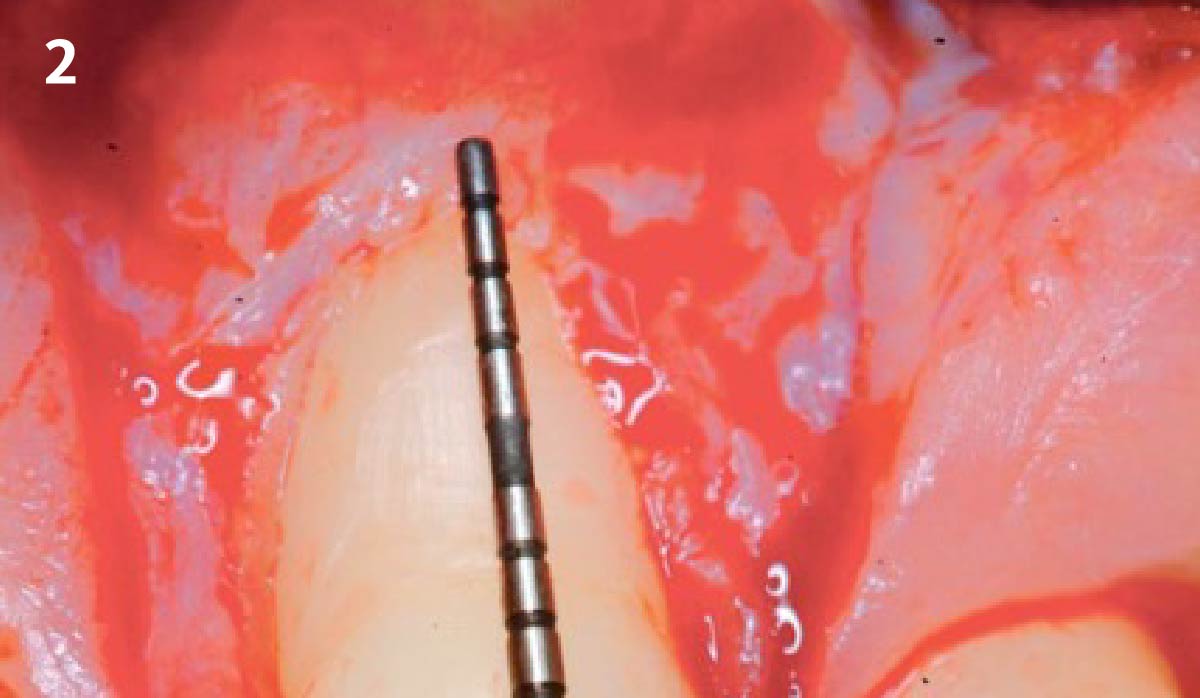
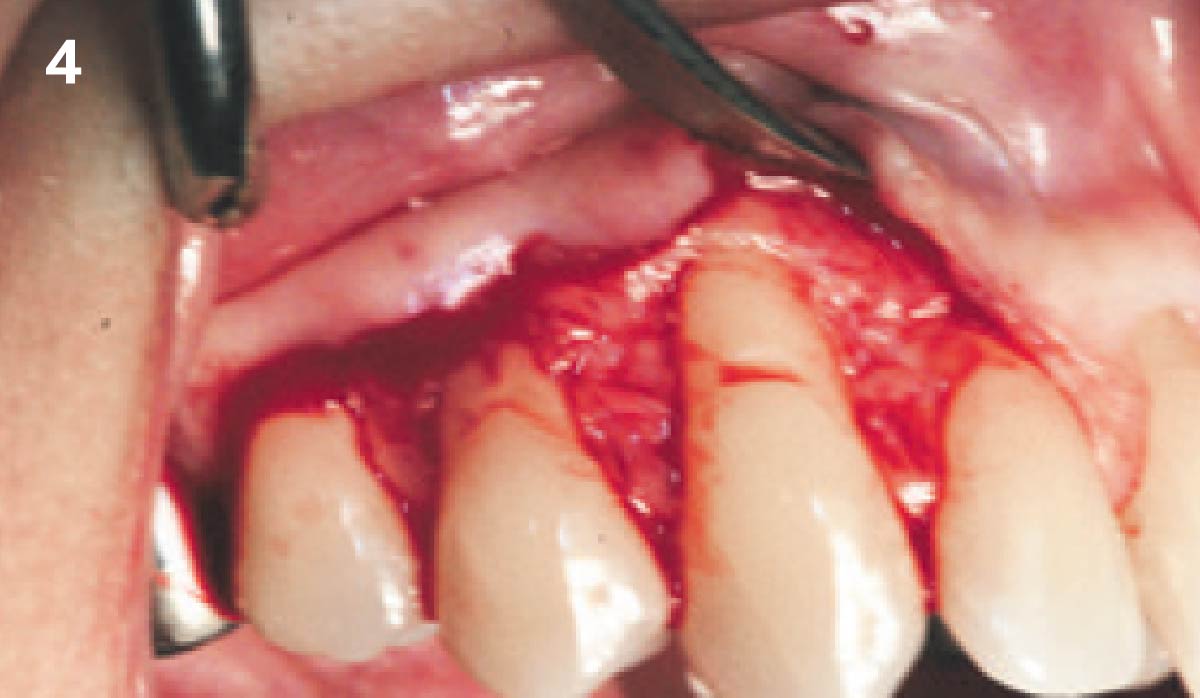
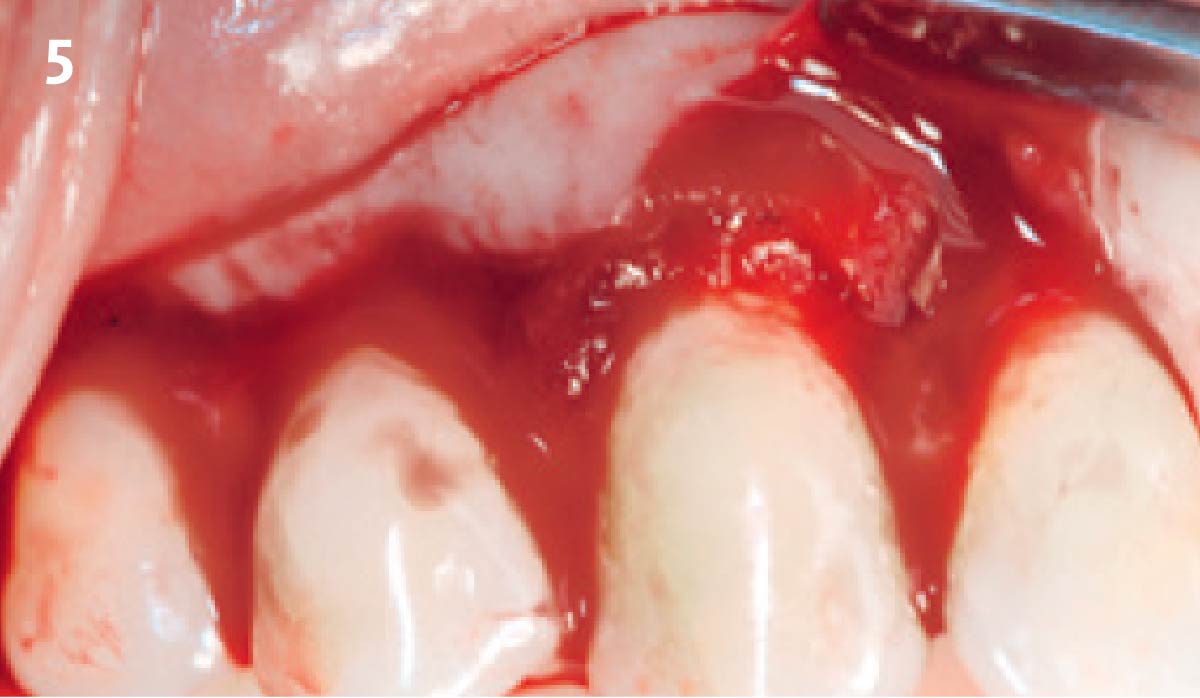
THE APPROACH
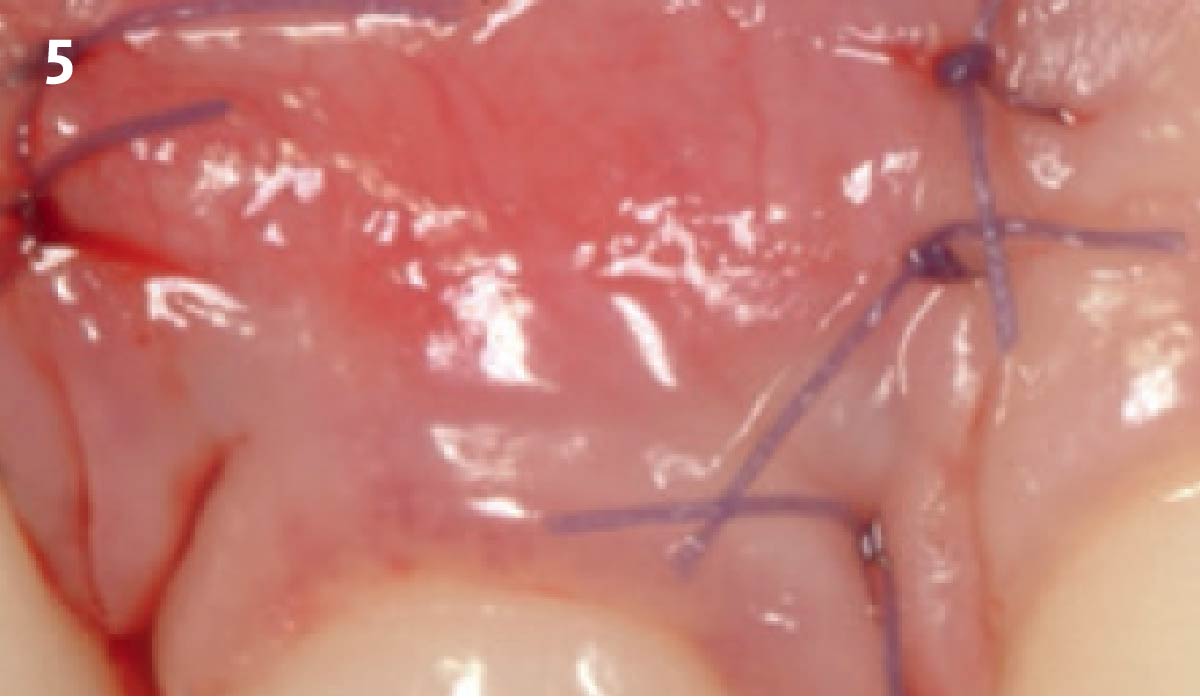
Correct the vertical bone loss around #9-10 and save the dentition. Sulcular incisions with a paracrestal incision around #9-10 were performed. The area was debrided showing a wide 1-2 bony wall defect (measuring ~7mm vertical bone loss). Primary closure was obtained using 6-0 prolene sutures.




“Guided tissue regeneration is indicated to correct the vertical bone loss around the #9-10 area and stabilize the periodontium.”
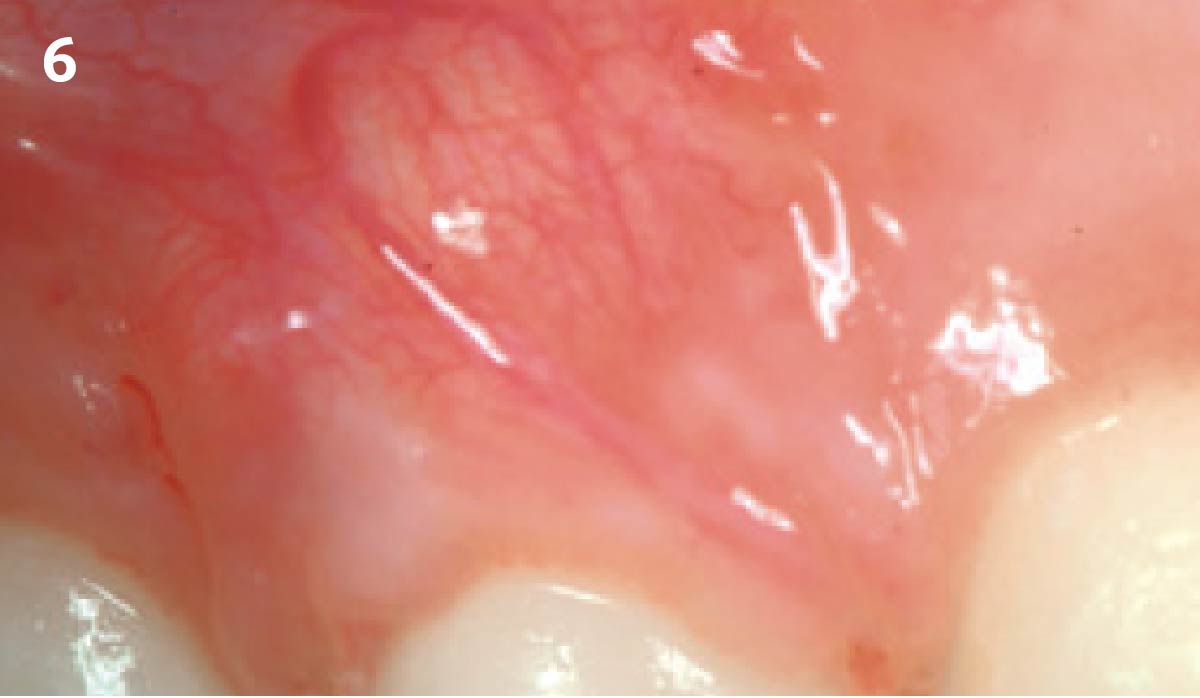
THE OUTCOME
The use of a minimally invasive surgical GTR approach showed excellent radiographic bone fill and reduction in probing depths from 8mm to 3mm at 6 months follow-up. Treatment outcome revealed stable periodontium and the patient was happy with the healthy stable teeth.

Bassam Kinaia, DDS, MS, DICOI
Dr. Kinaia is the Associate Director of the Graduate Periodontology Program at the University of Detroit Mercy (UDM). He is also the former Director of the Periodontology Program at UDM in Michigan and Boston University Institute for Dental Research and Education in Dubai. He is a Diplomate of the American Acade- my of Periodontology (AAP) and International Congress of Oral Implantology (ICOI). He received a certificate of Excellence from the AAP in recognition of teaching-research fellowship.
BIOBRIEF
Soft-Tissue Augmentation in the Esthetic Zone

THE SITUATION
A young male patient was referred to the clinic with a missing central incisor, #9 following trauma. An implant was placed and the patient was referred for an implant-born reconstruction. The patient does not smoke and drinks occasionally. Upon a clinical examination, extensive horizontal and vertical contour deficiencies are present prior to abutment connection.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system | Light smoker | Impaired immune system |
| Patient’s esthetic requirements | Low | Medium | High |
| Height of smile line | Low | Medium | High |
| Gingival biotype | Thick – “low scalloped” | Medium – “medium scalloped” | Thin – “high scalloped” |
| Shape of dental crowns | Rectangular | Triangular | |
| Infection at implant sight | None | Chronic | Acute |
| Bone height at adjacent tooth site | ≤ 5 mm from contact point | 5.5 – 6.5 mm from contact point | ≥ 7 mm from contact point |
| Restorative status of adjacent tooth | Intact | Restored | |
| Width of tooth gap | 1 tooth (≥ 7 mm) | 1 tooth (≤ 7 mm) | 2 teeth or more |
| Soft-tissue anatomy | Intact | Compromised | |
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
THE APPROACH
The compromized situation with a horizontal and vertical hard and soft-tissue deficit required a soft-tissue volume grafting procedure. A buccal split-thickness flap was prepared and Geistlich Fibro-Gide® shaped and placed. Primary wound closure was obtained. Abutment connection was performed after 8 weeks and the emergence profile created with a provisional reconstruction. The final reconstruction was placed at 3 months.






“The patient presented with severe horizontal and vertical hard and soft-tissue defects. I needed a solution that could increase the soft-tissue anatomy around the implant and prosthesis.”
THE OUTCOME
The outcome of the case was very pleasing having fulfilled the patient’s expectations in terms of esthetics and function. The tissues are healthy and volume was obtained through the grafting procedure to match the contour of the neighboring natural tooth.
Prof. Dr. Daniel S. Thoma
Prof. Dr. Daniel Thoma is the head of Reconstructive dentistry and Vice-chairman at the Clinic for Fixed and Removable Prosthodontics and Dental Material Sciences, University of Zurich, Switzerland. He graduated in 2000 at the University of Basel, Switzerland and was trained in implant dentistry and prosthodontics at the clinic for Fixed and Removable Prosthodontics and dental Material Sciences, University of Zurich, Switzerland.
BIOBRIEF
Root Coverage for Multiple Adjacent Teeth in the Maxilla with Geistlich Fibro-Gide® 1.5-Year Follow-Up


THE SITUATION
The patient is a healthy, 60-year-old female who presented to our clinic with a chief complaint of progressive gum recession which had led to compromised esthetics and sensitivity involving the maxillary left lateral incisor (#10), canine (#11), and first bicuspid (#12) teeth. The teeth in question had 3-4 mm of gingival recession on the buccal surface with a sufficient zone of keratinized gingiva. These teeth also had obvious cervical abrasion.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system | Light smoker | Impaired immune system |
| Patient’s esthetic requirements | Low | Medium | High |
| Height of smile line | Low | Medium | High |
| Gingival biotype | Thick – “low scalloped” | Medium – “medium scalloped” | Thin – “high scalloped” |
| Shape of dental crowns | Rectangular | Triangular | |
| Infection at implant sight | None | Chronic | Acute |
| Bone height at adjacent tooth site | ≤ 5 mm from contact point | 5.5 – 6.5 mm from contact point | ≥ 7 mm from contact point |
| Restorative status of adjacent tooth | Intact | Restored | |
| Width of tooth gap | 1 tooth (≥ 7 mm) | 1 tooth (≤ 7 mm) | 2 teeth or more |
| Soft-tissue anatomy | Intact | Compromised | |
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
Severity of recession – mild to moderate
Amount of keratinized gingiva – 2 mm or greater for all teeth involved
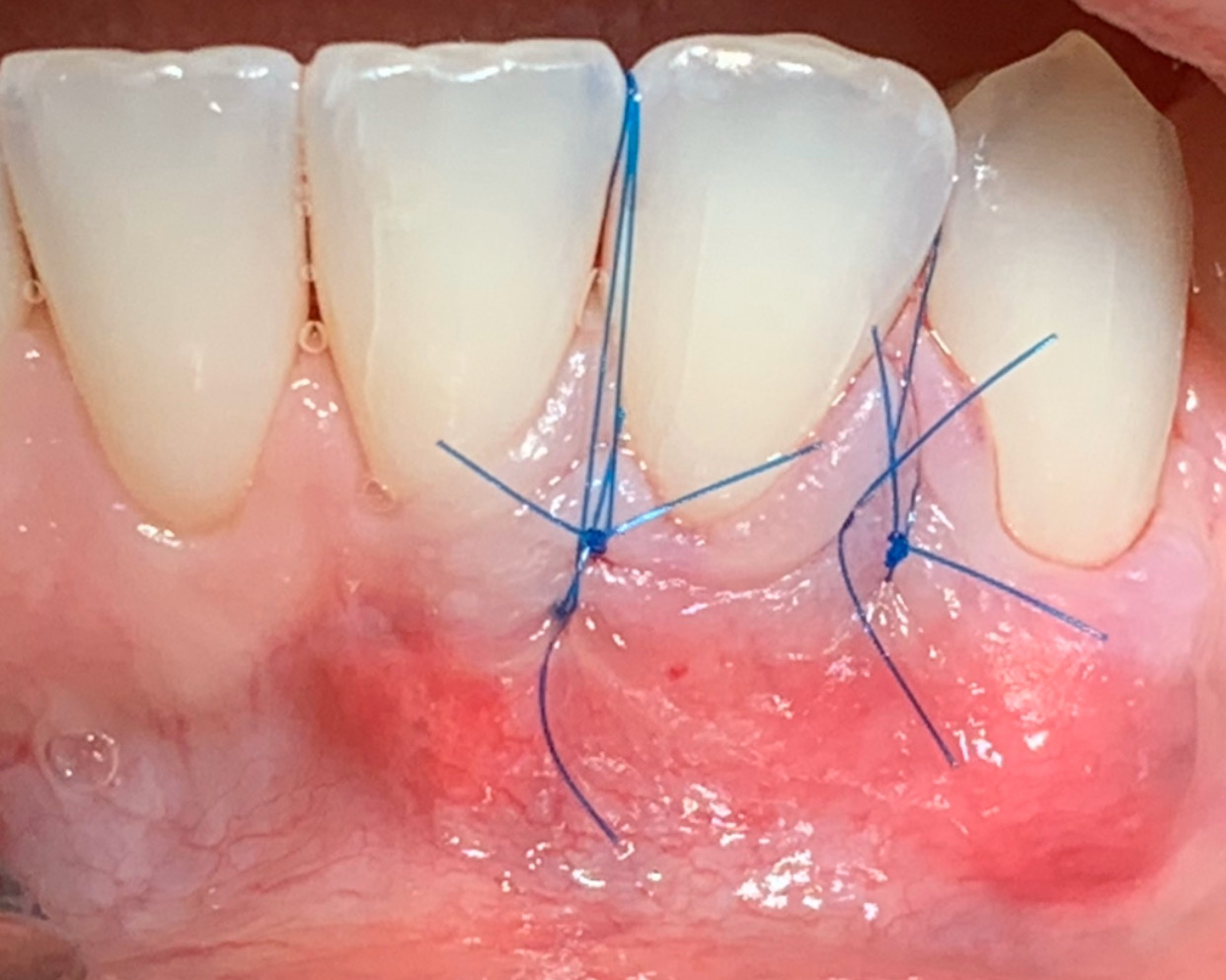
THE APPROACH
Treatment goals for this case were to obtain complete root coverage, increase soft tissue thickness, and reduce/eliminate cervical sensitivity. A split-thickness envelope flap approach was used. Geistlich Fibro-Gide® was then trimmed, hydrated with saline, and placed over the exposed root surfaces. The flap was coronally advanced in a tension-free manner to completely cover the biomaterial and exposed root surfaces.








“The patient’s main priorities were to improve esthetics and reduce/eliminate root sensitivity. Soft tissue grafting was done with autologous connective tissue in other areas of her mouth many years ago and she was hesitant to undergo surgery again if it involved harvesting tissue from her palate due to the post-operative pain she experienced after these previous procedures.”
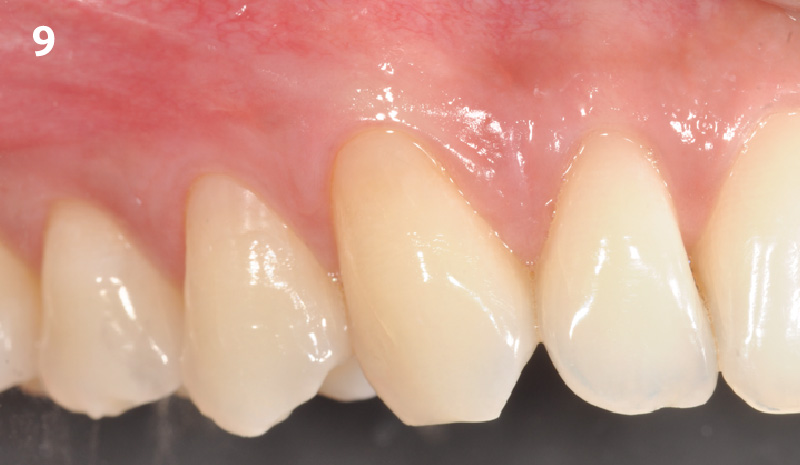
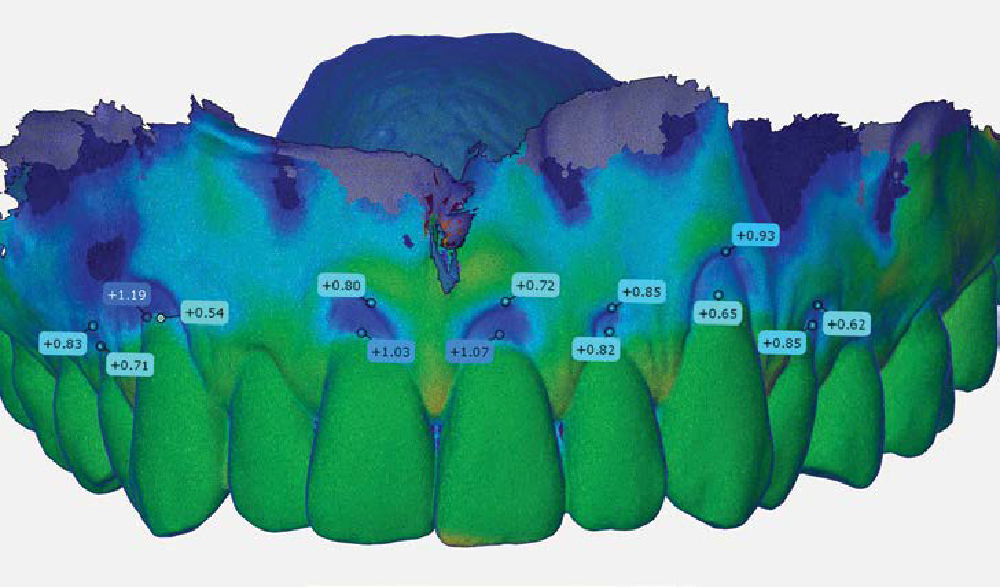
THE OUTCOME
This case nicely shows that the result following root coverage surgery to treat multiple adjacent teeth using a volume-stable collagen matrix is comparable to that seen with autologous connective tissue. At 1.5 years, there is continued stability of the treated site. The tissue appears healthy and firm. The patient‘s chief complaints of esthetics and sensitivity have been addressed and the patient is maintaining excellent oral hygiene and home care.
Dr. Vinay Bhide
Dr. Vinay Bhide is a board certified Periodontist with a special interest in periodontal plastics and reconstructive surgical procedures. Dr. Bhide did his dental and specialty training at the university of Toronto. In addition to private practice, Dr. Bhide is a clinical instructor in the Department of Periodontics at the university of Toronto. He is also a staff periodontist in the Center for Advanced Dental Care and Research at Mount Sinai Hospital, Toronto.
BIOBRIEF
Enhance Periodontal Phenotype with Geistlich Mucograft® for Soft Tissue Augmentation


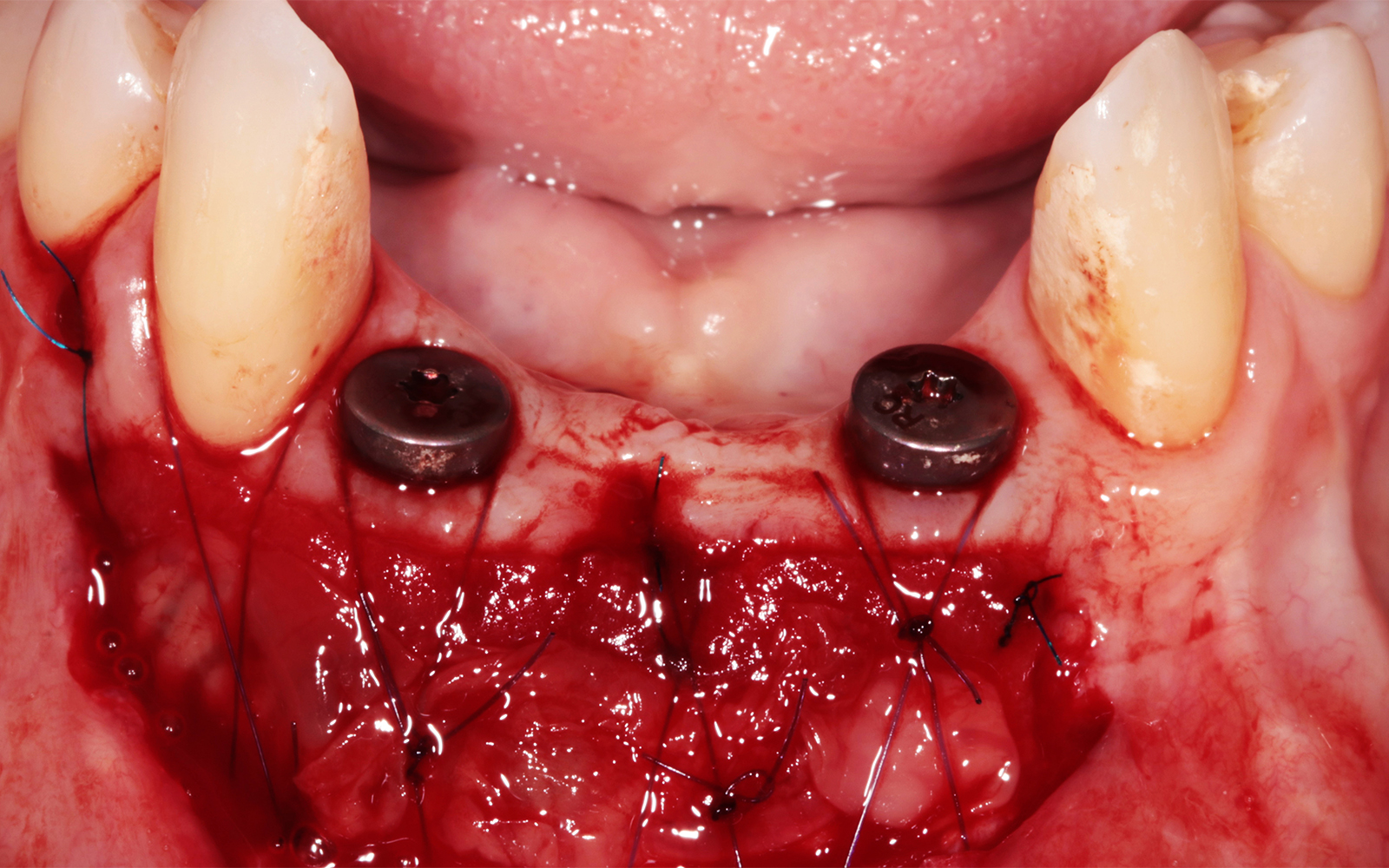
THE SITUATION
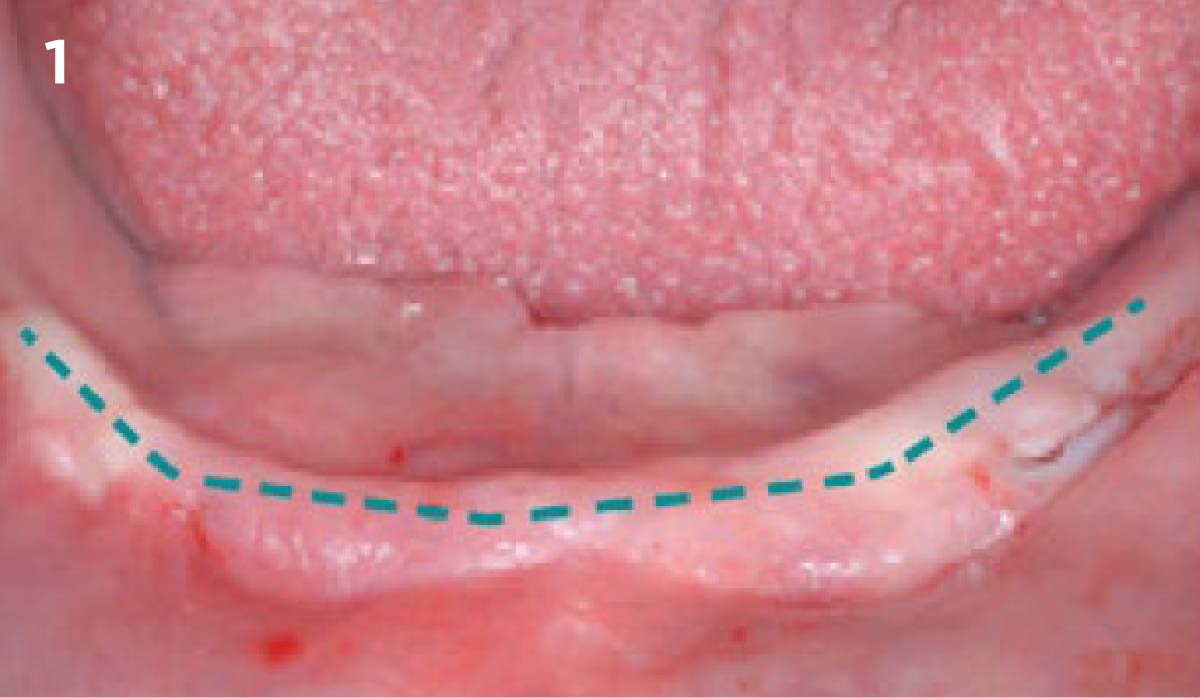
A healthy, non-smoking, 37- year-old female presented for second stage surgery at implant sites #23 and #26. Limited keratinized tissue width and gingival thickness can be appreciated in the edentulous ridge, and the patient can be classified as having a thin periodontal phenotype. Additionally, the patient states she experiences sensitivity, and the tissue feels “tender” when brushing. The patient hopes to address her needs in a minimally invasive manner.
THE RISK PROFILE
| Low Risk | Medium Risk | High Risk | |
|---|---|---|---|
| Patient’s health | Intact immune system Non-smoker | Light smoker | Impaired immune system Heavy smoker |
| Patient’s esthetic requirements | Low | Medium | High |
| Height of smile line | Low | Medium | High |
| Gingival biotype | Thick – “low scalloped” | Medium – “medium scalloped” | Thin – “high scalloped” |
| Shape of dental crowns | Rectangular | Triangular | |
| Infection at implant sight | None | Chronic | Acute |
| Bone height at adjacent tooth site | ≤ 5 mm from contact point | 5.5 – 6.5 mm from contact point | ≥ 7 mm from contact point |
| Restorative status of adjacent tooth | Intact | Restored | |
| Width of tooth gap | 1 tooth (≥ 7 mm) | 1 tooth (≤ 7 mm) | 2 teeth or more |
| Soft-tissue anatomy | Intact | Compromised | |
| Bone anatomy of the alveolar ridge | No defect | Horizontal defect | Vertical defect |
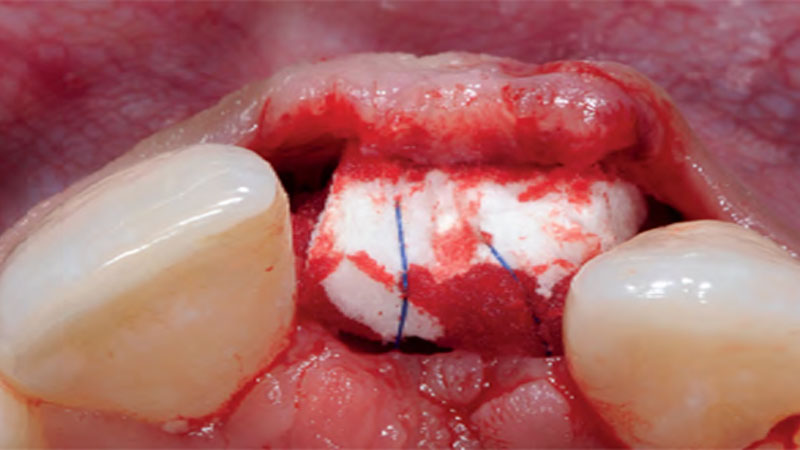
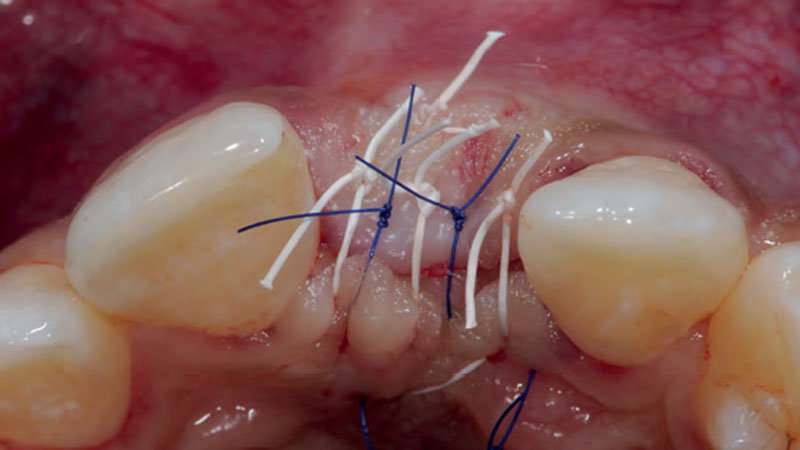
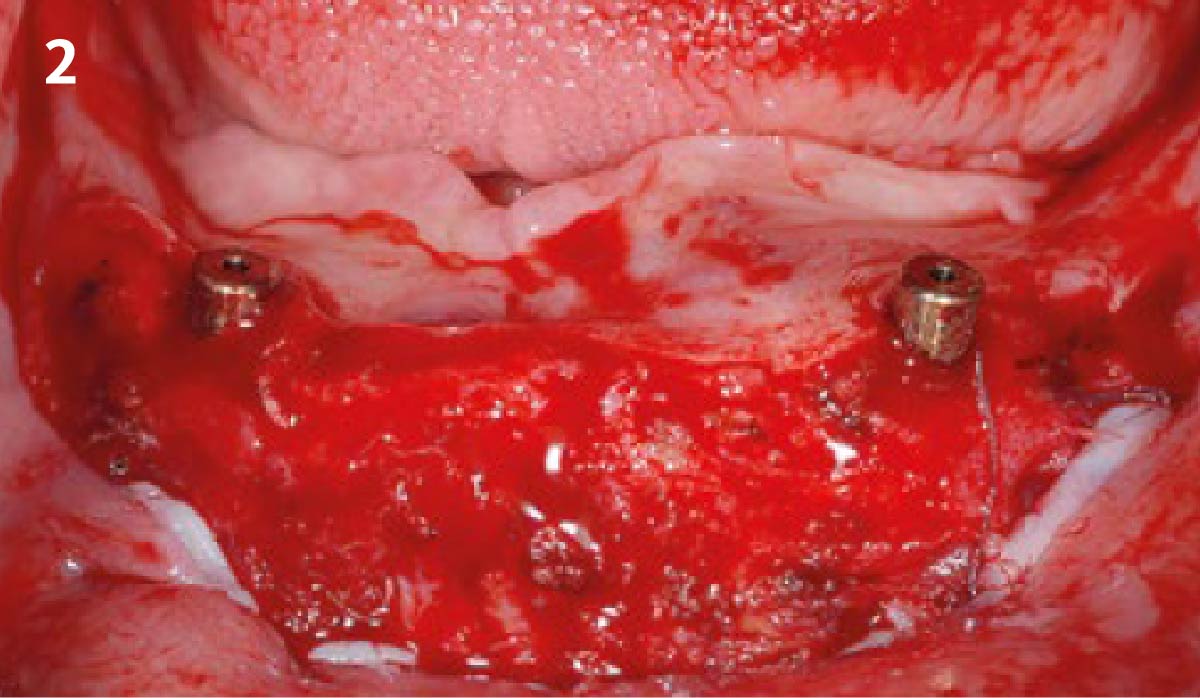
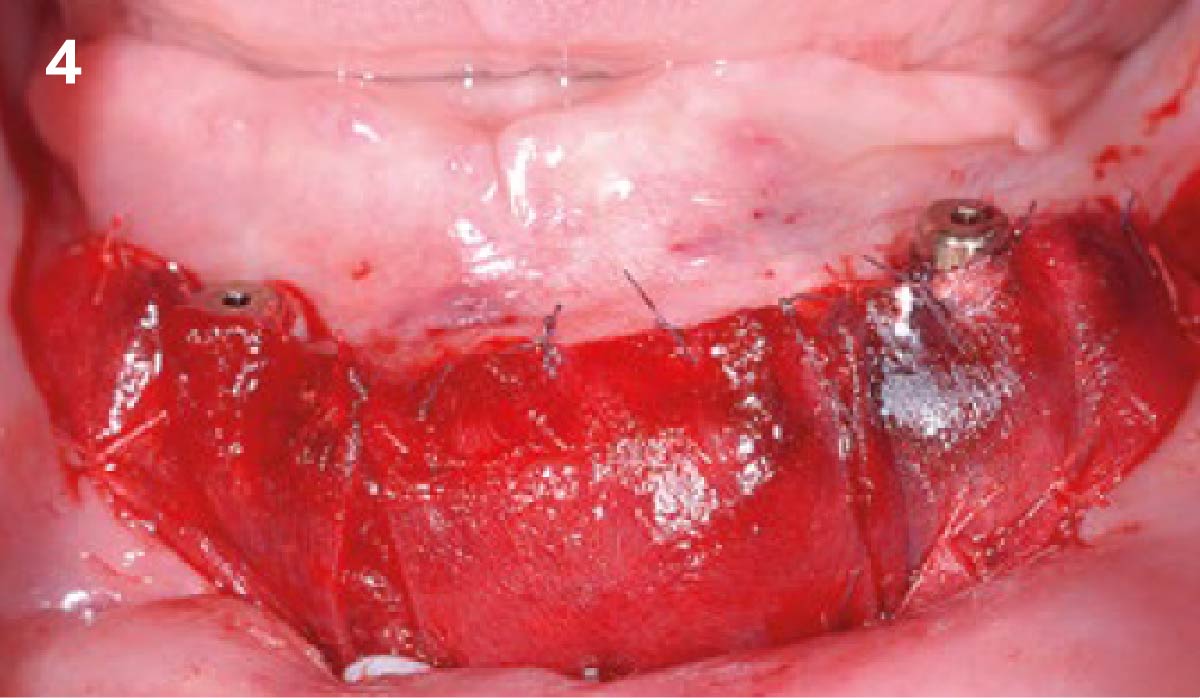
THE APPROACH
The aim of treatment was to enhance the existing periodontal phenotype from that of one which is thin, with limited keratinized tissue, to one that is thick and maintains an adequate band of attached keratinized tissue. Geistlich Mucograft® was used in conjunction with a PRF membrane, in order to provide optimal wound healing, due to its chemotactic and angiogenic properties.




A viable option that allows for reduced patient morbidity, adequate functional necessity, and ideal esthetics.
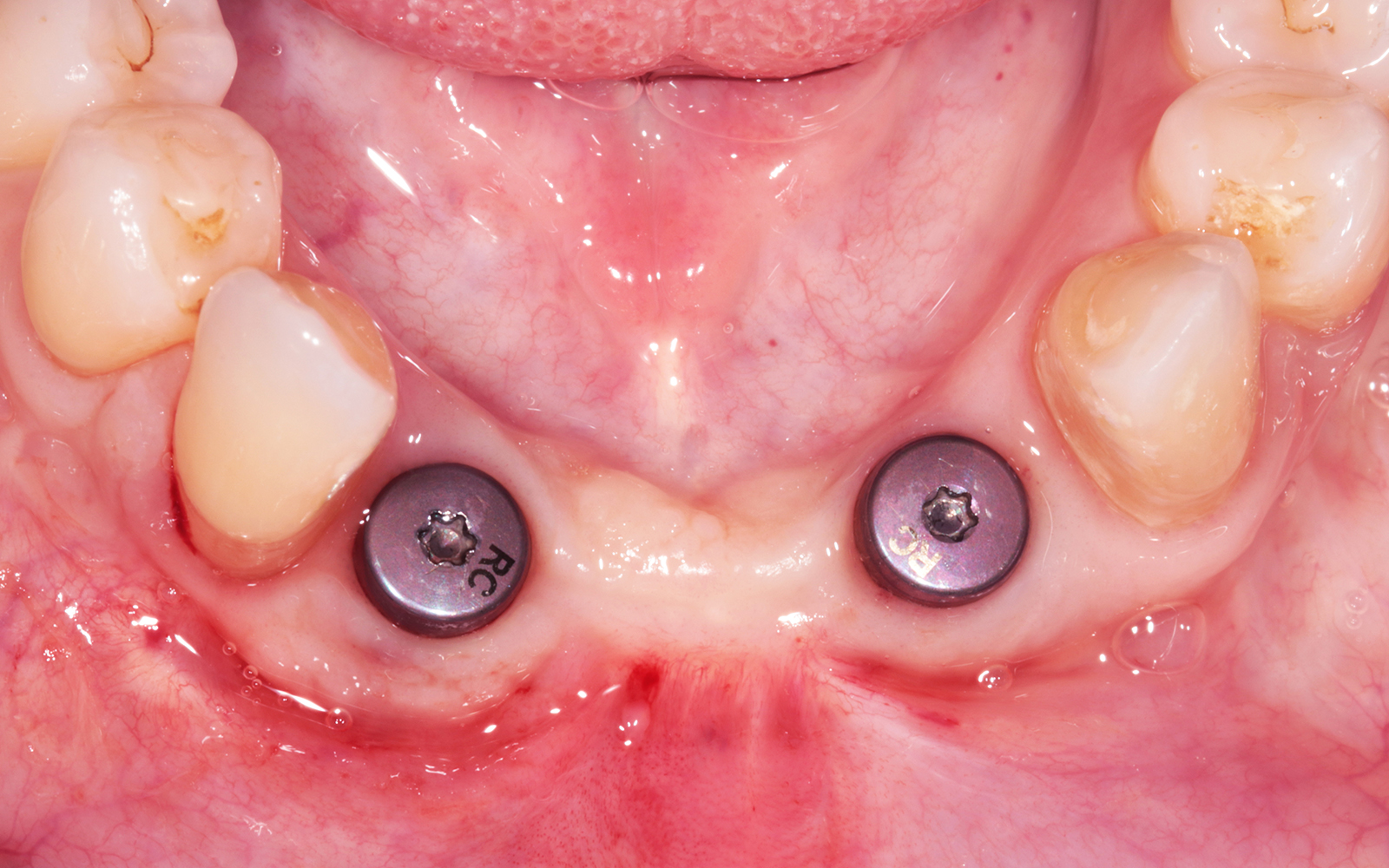
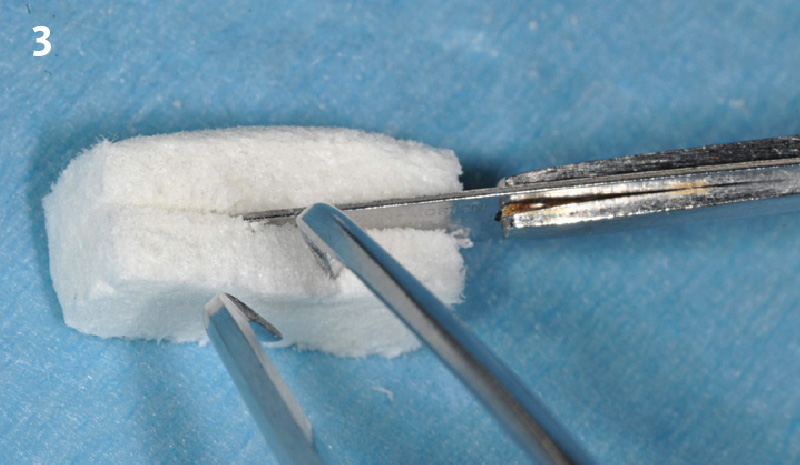
THE OUTCOME
Dual application of platelet-rich fibrin (PRF) and a xenogenic collagen matrix, Geistlich Mucograft®, led to successful augmentation of the edentulous ridge. At one-year, the tissues appear healthy, and an increased keratinized tissue width and gingival thickness can be appreciated. By using this soft tissue alternative, the patient was able to avoid post-operative morbidity from a second surgical site, and the chief complaint was addressed.
Allison Rascon, D.D.S., M.S.
Dr. Allison Rascon was born and raised in Miami, Florida. She received her Bachelor of Science in Biomedical and Health Sciences from the University of Central Florida. She received her DDS from New York University, where she graduated with honors in Periodontics and was inducted into the Omicron Kappa Upsilon National Dental Honor Society in 2020. She then went on to receive a Certificate in Periodontics and Master of Science in Oral Biology from the University of Pennsylvania. Currently, she is board-eligible by the American Academy of Periodontology. She is an active member of the AAP, AO, OF, and ADA. Aside from her active participation in organized dentistry, she is also passionate about her research in periodontal and peri-implant regeneration. Dr. Rascon was a recipient of the George J. Coslet Memorial Scholarship in 2021 and 2022. During her residency, she was awarded the Best Oral Clinical Presentation Award at the Academy of Osseointegration Annual Meeting in 2022 and was the recipient of the Northeastern Society of Periodontists Tannenbaum/ Schoor Resident School Competition Award for 2023. Currently, Dr. Rascon works in private practice in Manhattan, NY.
WEBINAR

WEBINAR
CLINICAL CASE






CLINICAL CASE







CLINICAL CASE






CLINICAL CASE









CLINICAL CASE






CLINICAL CASE









CLINICAL CASE







CLINICAL CASE








CLINICAL CASE


CLINICAL CASE







CLINICAL CASE






CLINICAL CASE




CLINICAL CASE

CLINICAL CASE








CLINICAL CASE



CLINICAL CASE








CLINICAL CASE






CLINICAL CASE